Glass Ionomer: Bases and Liners
1/94
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
95 Terms
why is deep dentin clinically significant
deep dentin is:
- porous
- susceptible to desiccation
- poor bonding substrate
what does deep dentin fail to protect against
- heat from rotary instruments
- toxic restorative materials
- thermal changes
- mechanical forces
- galvanic shock
- bacteria/toxins
- poor bonding conditions
deep dentin = biologically _____ + _____ weak
vulnerable, structurally
goals of liners/bases
- cover deep dentin
- reduce tubular fluid flow
provide:
- thermal barrier
- physical barrier
- improve bonding env.
protect pulp from:
- bacteria
- toxins
dental liner is defined by _____ of material
thickness
*most important consideration for pulpal protection... thickness of remaining dentin when choosing liners and/or base*

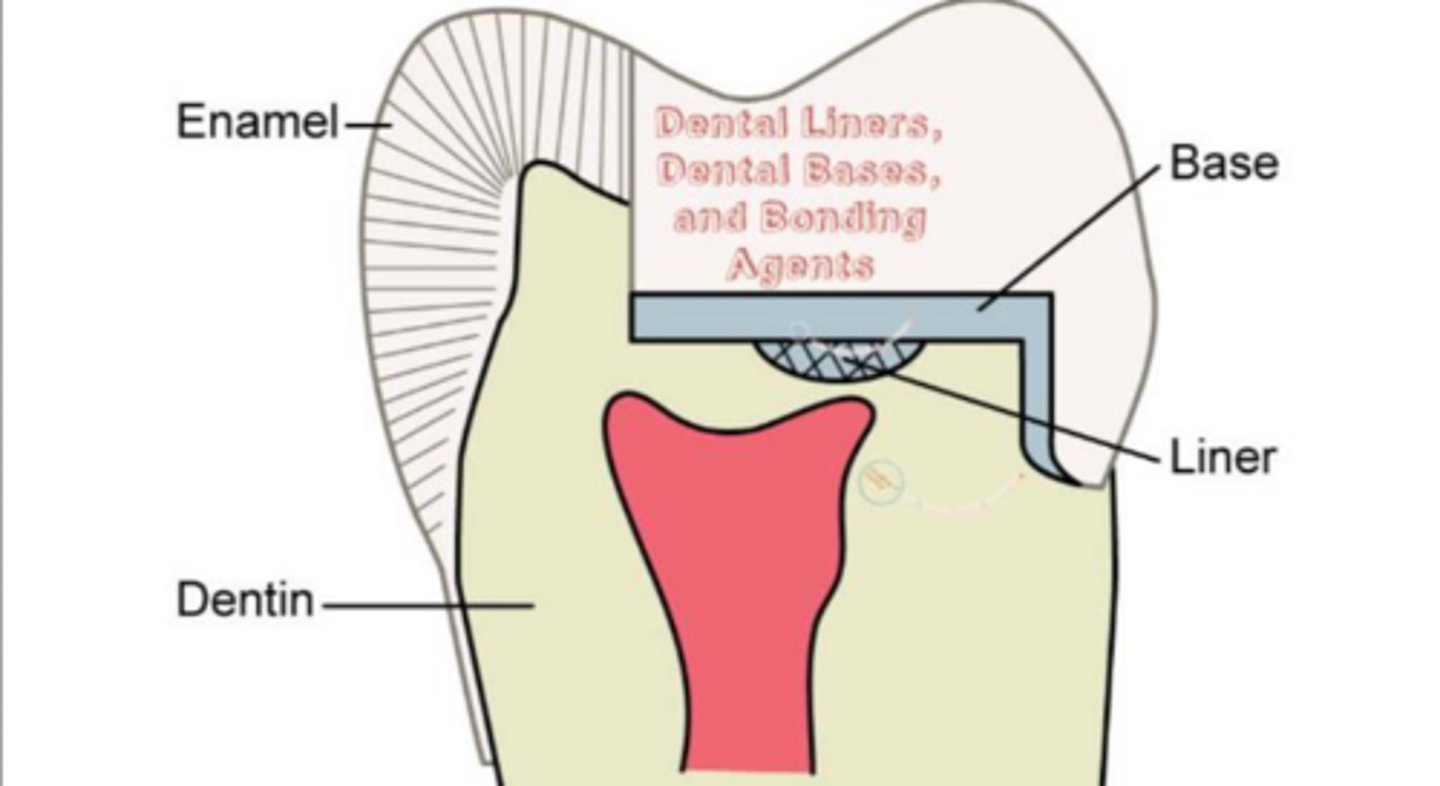
what is a liner
thin film or coating/layer (< 0.5 mm)
applied to exposed dentin
protects pulp from chemical and bacterial insult
where is a liner placed
ONLY deepest areas of cavity prep:
- pulpal floor
- axial wall
when is a liner indicated
when prep is ~0.5 mm from pulp
most important factor for pulpal protection
remaining dentin thickness (RDT)
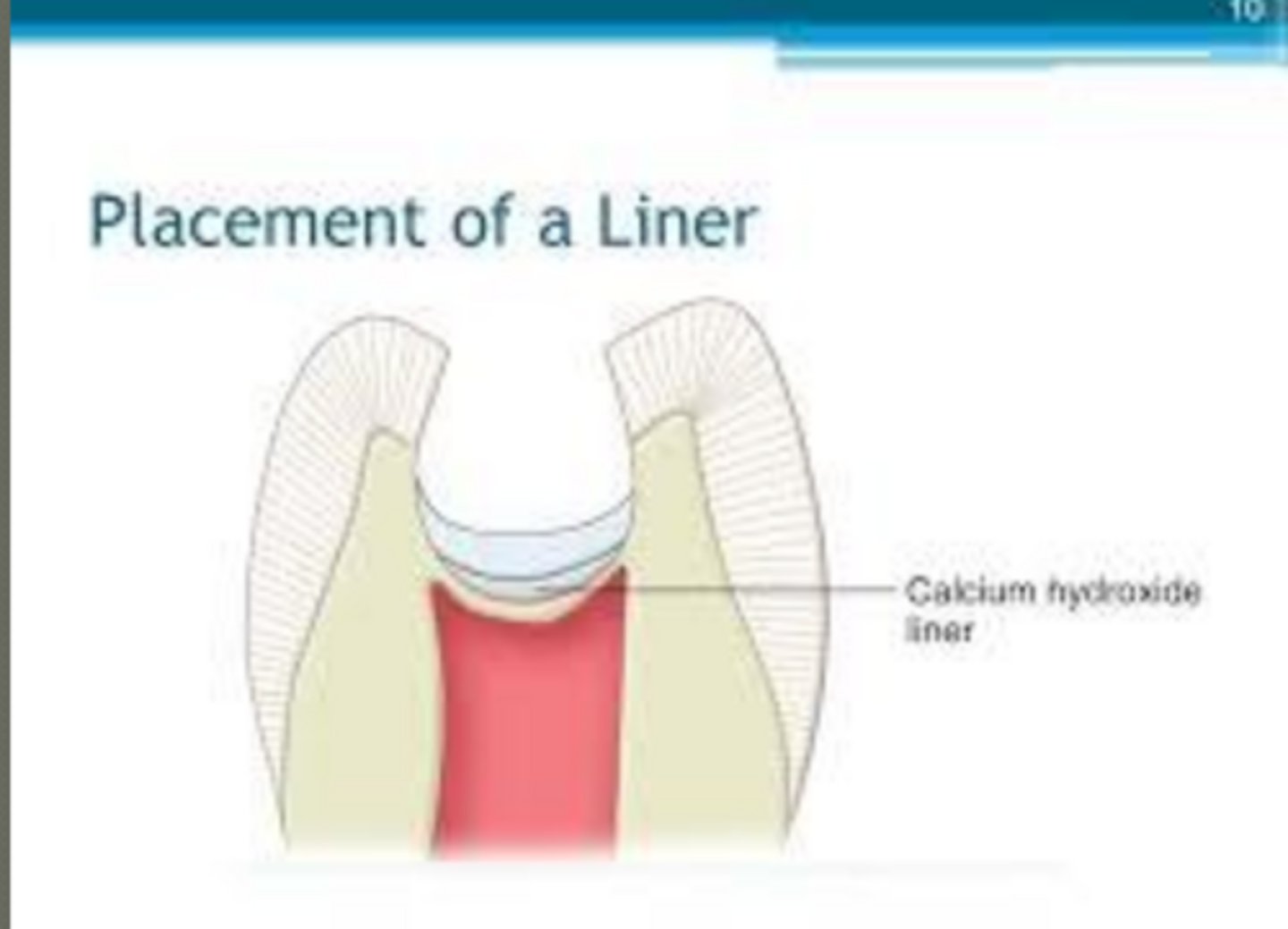
ex. of liners
calcium hydroxide
mineral trioxide aggregate (MTA-endo use, direct pulp cap)
glass ionomer
function of a dentin bonding agent (DBA)
seals dentinal tubules
prevents bacterial invasion

how is DBA used under composite
MANDATORY
acts as a bonding agent
how is DBA used under amalgam
optional
no etch
functions like a liner → reduces sensitivity
is etch required with dentin bonding agent
may require total etch, selective etch, or no etch technique when use as a bonding agent
what are the functions of calcium hydroxide (Dycal)
chemical barrier
antimicrobial (direct & indirect pulp capping)
stimulates reparative tertiary dentin (atubular)

what type of dentin does CaOH form
reparative (atubular) dentin
NOT reactionary
when is CaOH use indicated
deep cavities near pulp
must mix base and catalyst prior to placement
major disadvantage of CaOH
low compressive strength
material is brittle, weak under pressure, and unable to withstand the heavy forces of condensation when placing permanent restorations like amalgam
acts as a "low-strength base," requiring a stronger base (such as glass ionomer) to be placed over it to support the restoration
why must CaOH be covered
dissolves easily
cannot withstand forces
what covers CaOH
base (Not secondary liner for amalgam)
- thermal protection
base or secondary liner for composite
- done prior to etching and bonding
what is a base
thicker layer ( >0.5 to ~3 mm)
applied to exposed dentin
what is the only difference between liner and base
thickness
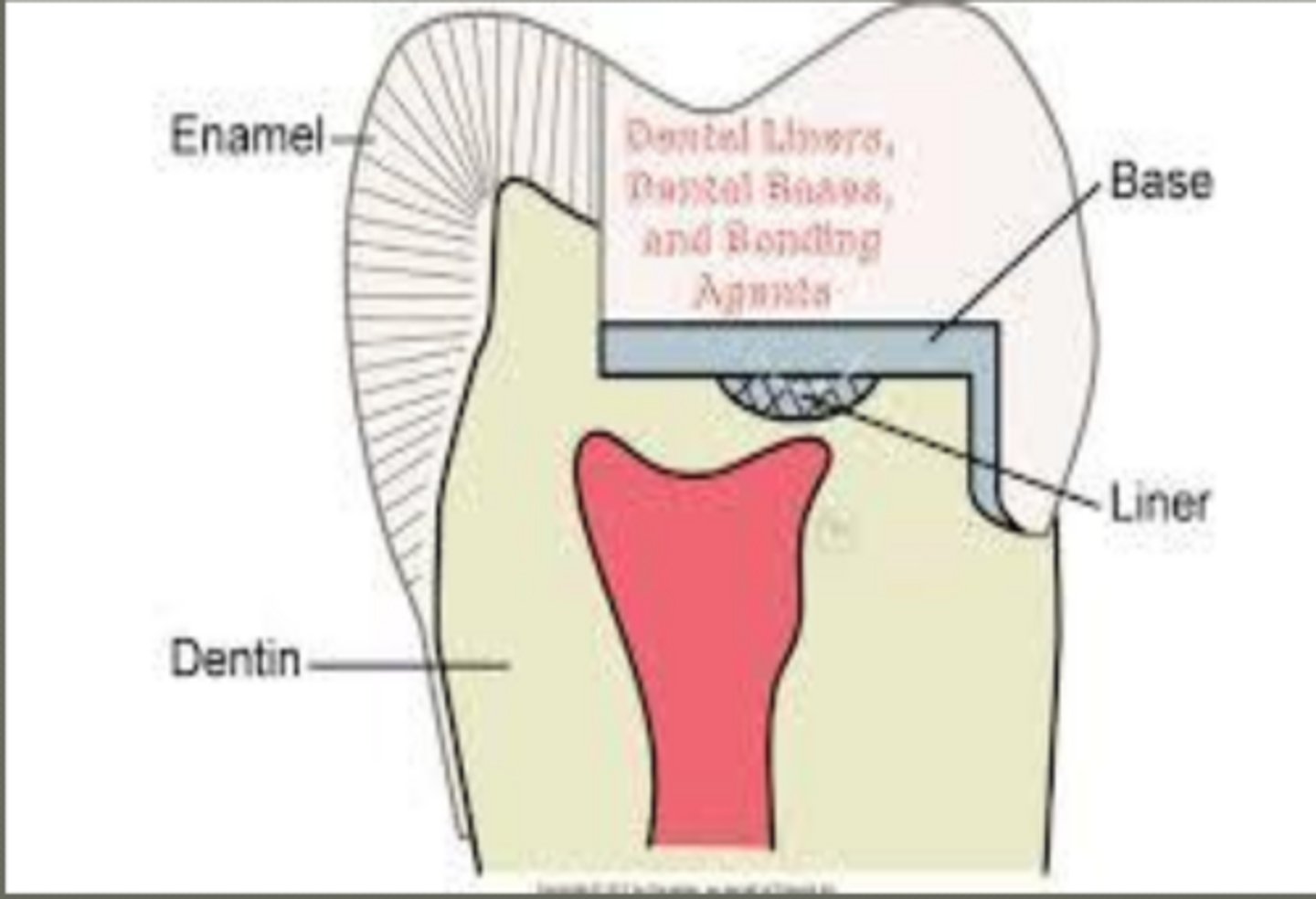
base
protects pulp from thermal insult in deep cavity preps
protects CaOH from dissolution
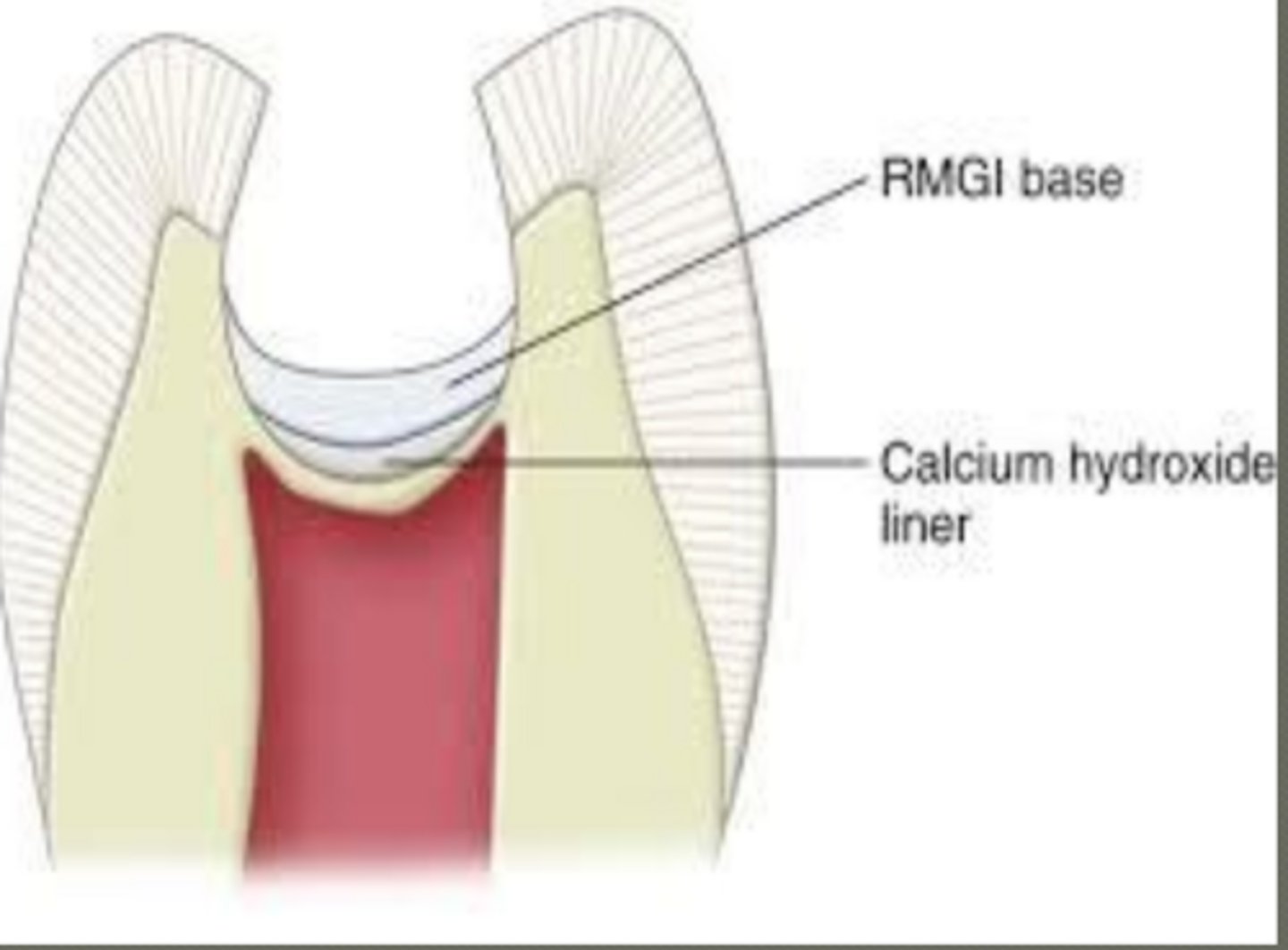
prep is 0.5 - 1.5 mm from pulp... what is done when RDT = 0.5-1.5 mm?
usually:
- base (RGMI)
- no CaOH unless very deep
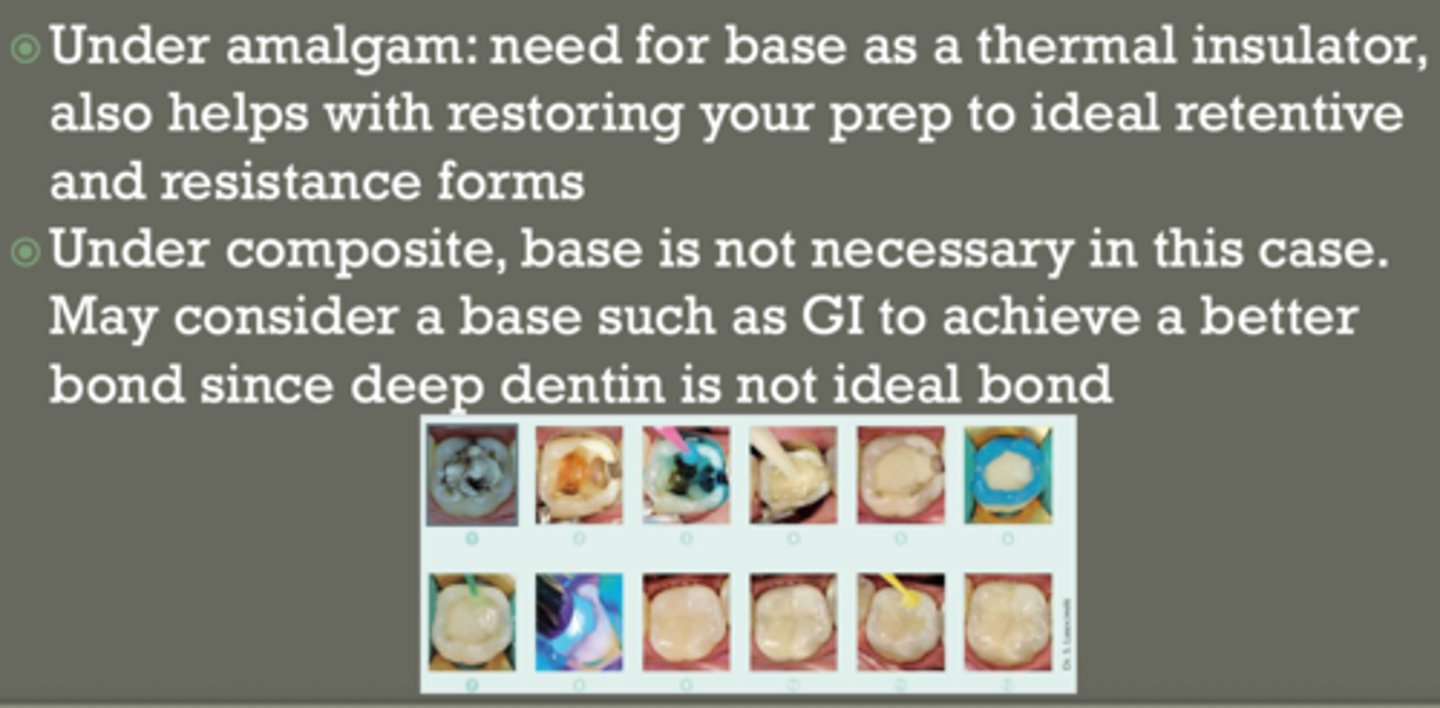
amalgam:
- base as thermal insulator
- helps with retentive and resistance forms
composite:
- base is not necessary
*RGMI helps achieve better bond since deep dentin is not ideal bond*
functions of a base
- thermal protection
- protect CaOH
- mechanical support
- restore ideal prep form
- resist compressive forces (of mastication)
- block out undercuts for indirect restorations
ex. of bases
glass ionomer
compomers
zinc phosphate cement
carboxylate cement
zinc oxide eugenol
what are compomers
polyacid-modified composite resin
key properties of compomer
properties of both composite and glass ionomer
- require DBA
- high strenght
- low fluoride ( < 10% of GI)
- light cured (polymerization reaction)
- less soluble than GI
- less esthetic than composite
why are compomers not commonly used
poor physical properties
less esthetic than composite
key features of Zinc Oxide/ Eugenol (IRM)
low strength
sedative effect of eugenol = advantage
Zinc Oxide/ Eugenol used...
under amalgam (low stress areas)
ex. axial walls
issues with Zinc Oxide Eugenol
interferes with composite polymerization reactions of bonded restoration (ex. composite)
glass ionomers can be used as ____ or secondary liner (thin amount placed over primary liner; ex. over _______ and under composite
base, CaOH
what are glass ionomers used for
base
secondary liner
sometimes final restoration
key properties of glass ionomer
chemical bond to tooth (predictable bonds to enamel & dentin)
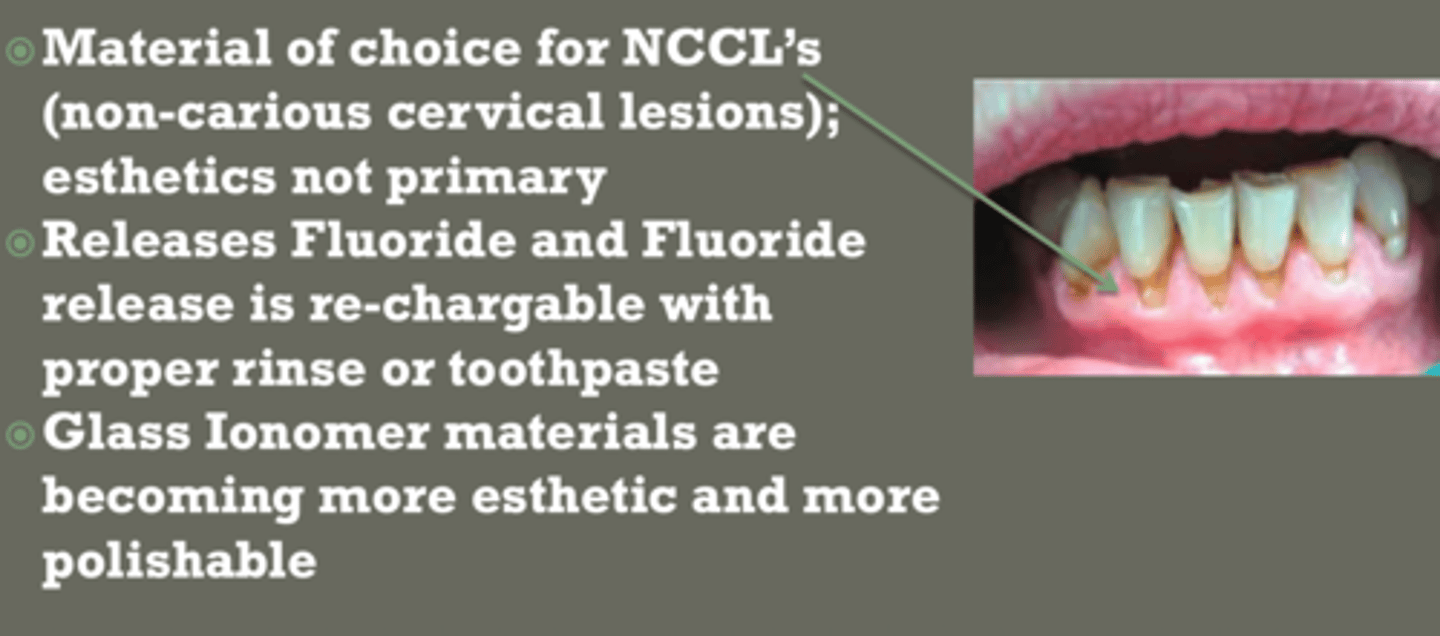
fluoride release + recharge
less esthetic & polishable than composite (exception EQUIA Forte)
can be pure or ______ glass ionomer (Ketac-Fil, EQUIA Fil) or resin ____ _____ ____ (RMGI) (Photac-Fil, Vitrebond)
conventional, modified glass inomer
pure or conventional glass ionmer
- acid/base reaciton
- aluminosilicate glass + polyacrylic acid ( w small ammounts of itaconic and tartaric acids)
- highest fluoride release
- lowest wear resistance & lowest strength
*new generations show marked improvement in strength and resistance ex. EquiaForte*
resin modified glass ionomer (RMGI)
- acid/base + polymerization (light activated) reaciton
- resin particles incorporated with glass ionomer
- less technique sensitive
- improved handling
- better physical properties
glass ionomer powder
SiO2 = 29.0%
Al2O3 = 16.6%
CaF2 = 34.3%
Na3AlF6 = 5%
AlF3 = 5.3%
AlPO4 = 9.8%
Calcium fluoroaluminosilicate glass
glass ionomer liquid
polymer acids:
- polyacrylic acid
- itaconic acid
- tartaric acid
glass ionomer setting reactoin
acid- base reaction between liquid (l) and powder (p)
polyacrylic acid (l) + aluminosilicate glass (p)

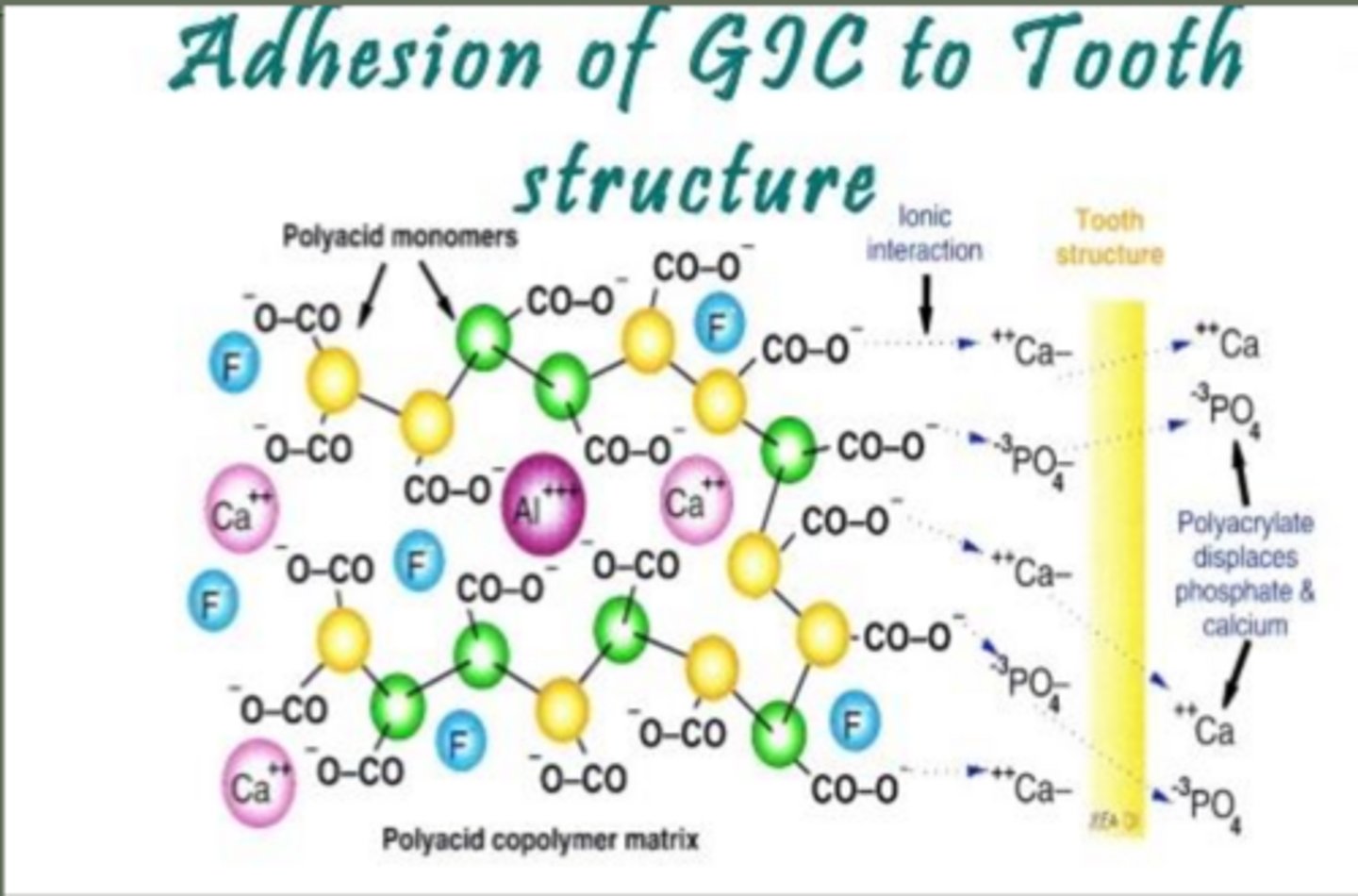
how do glass ionomers bond to tooth
chelation (chemically) to enamel and dentin
chelation reaction between carboxyl groups of polyacrylic acid and calcoum of hydroxyapatite crystals
carboxyl groups bind Ca2+ in hydroxyapatite
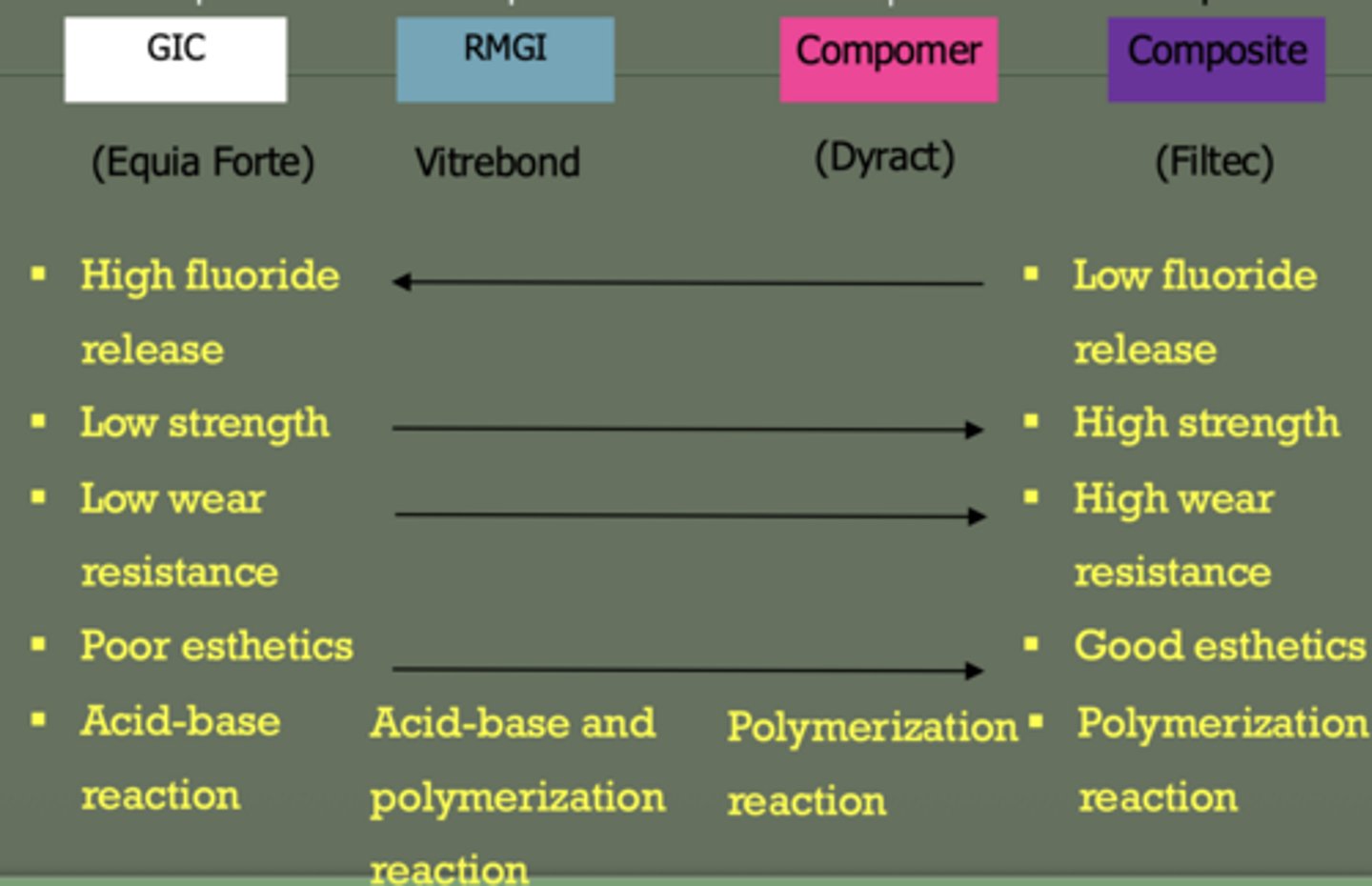
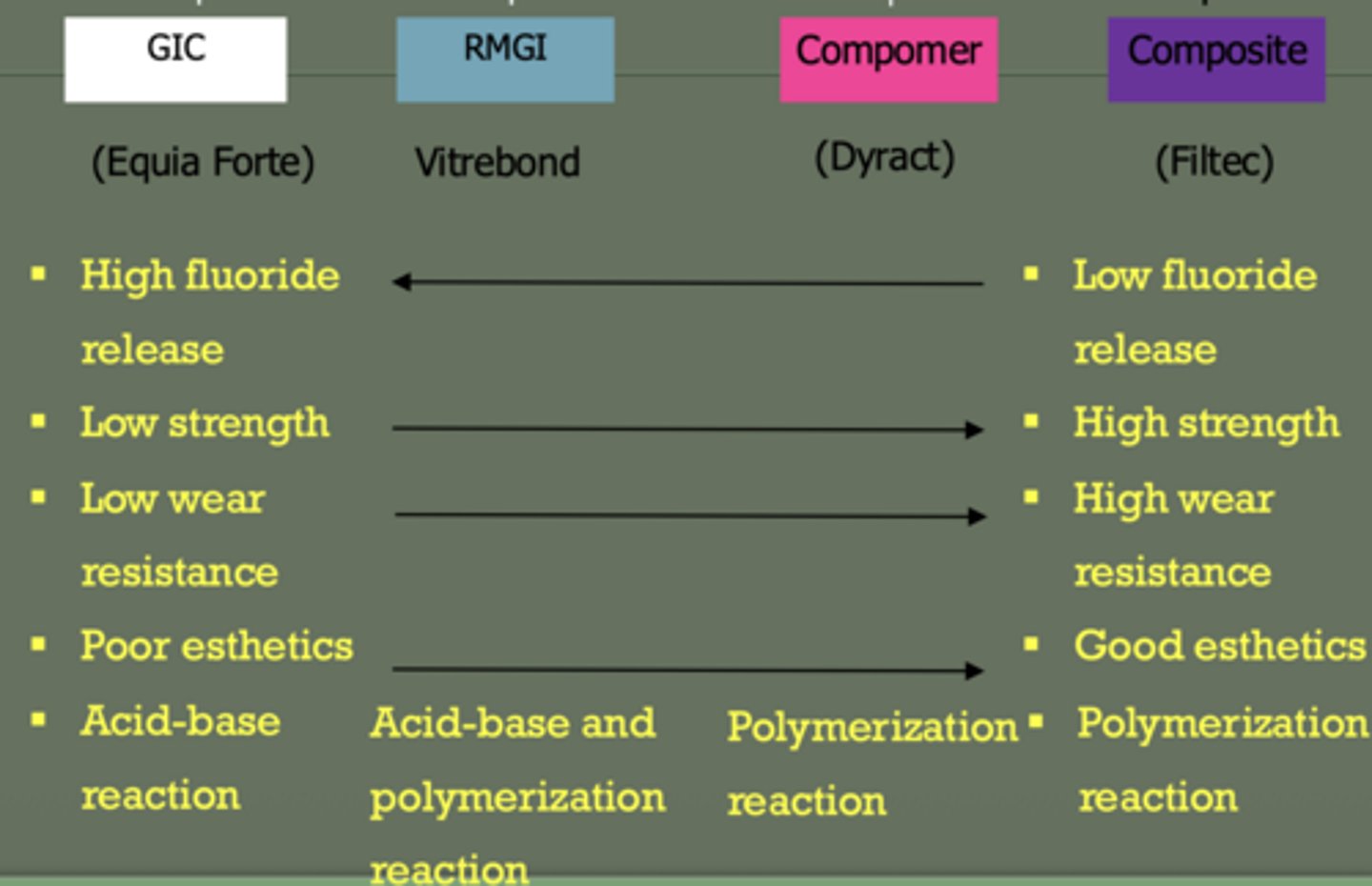
glass ionomer
reaction: acid- base
low strength
high fluoride
poor esthetics
low wear resistance
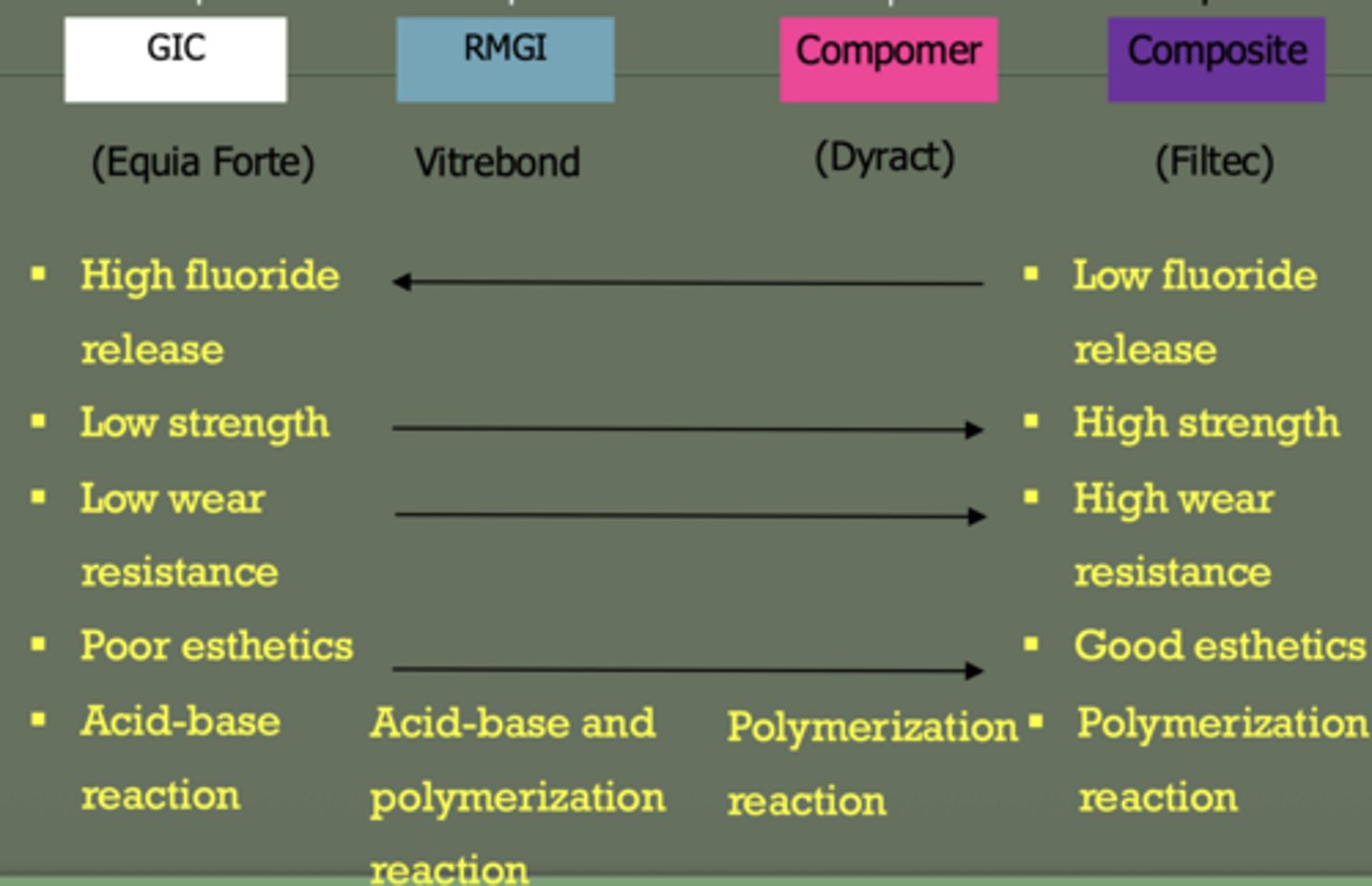
RMGI
reaction: acid-base + polymerization
moderate strength
moderate fluoride
better esthetics than GI
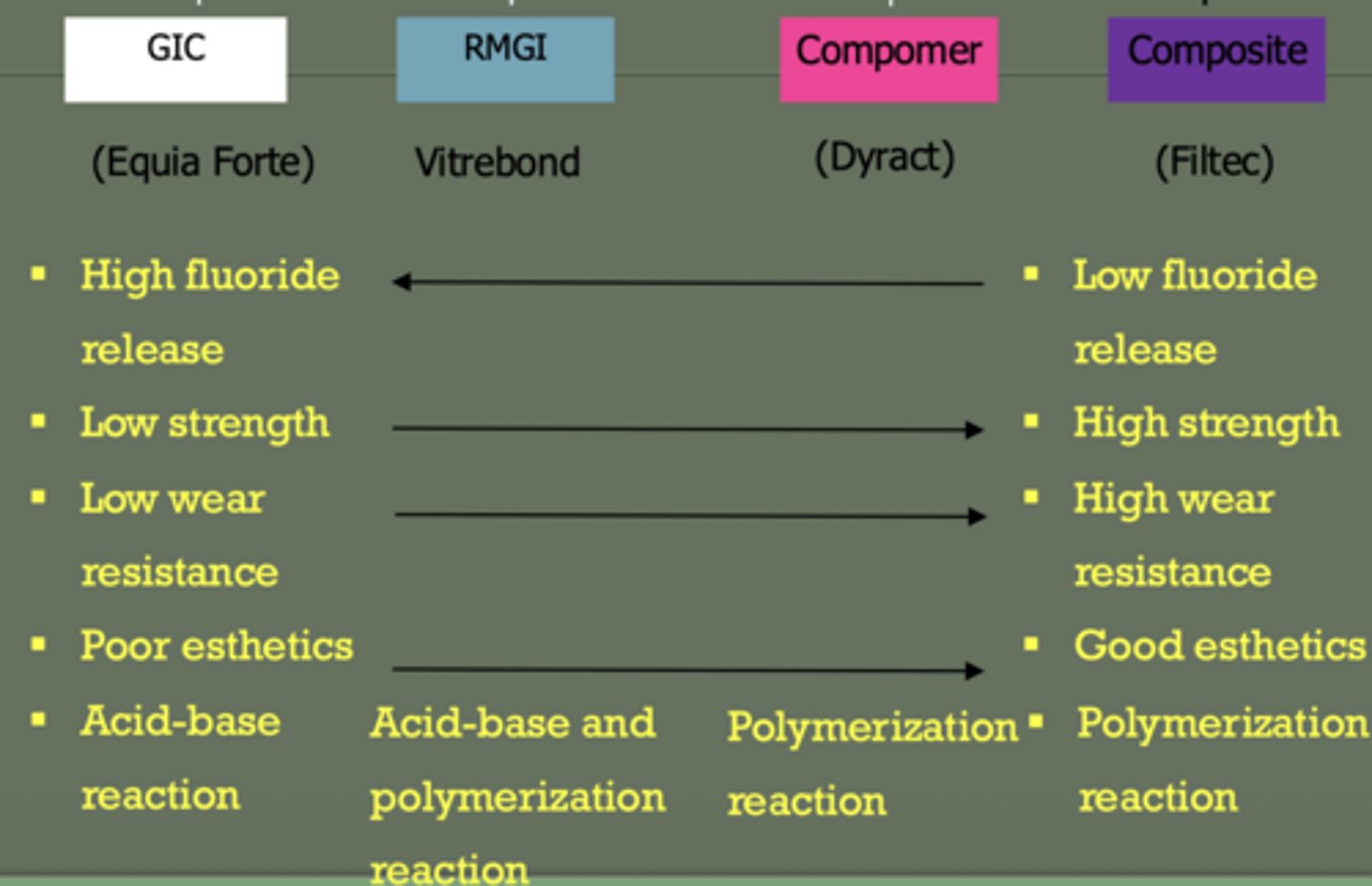
composite
reaction: polymerization (same with compomer)
high strength
no fluoride
best esthetics
high wear resistance
does composite or GI have higher wear resistance
composite
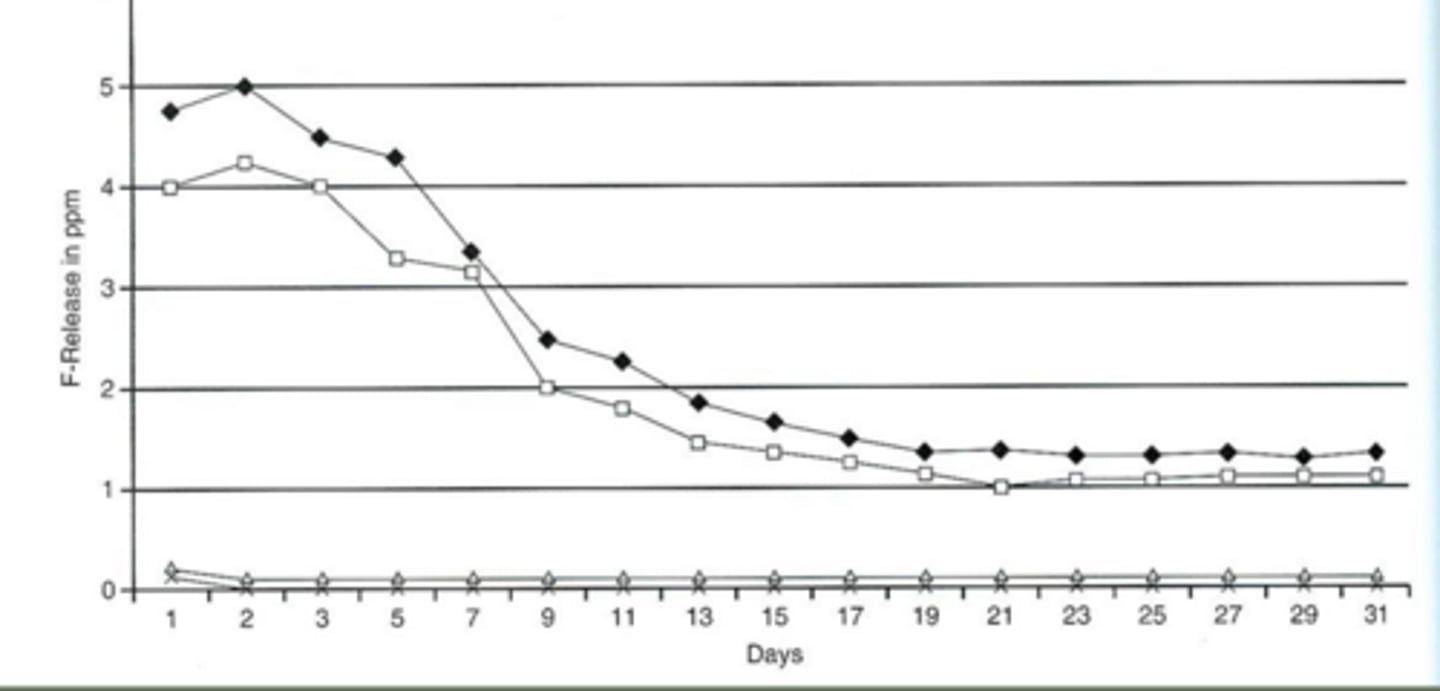
which material has best fluoride? highest strenght?
fluoride = glass ionomer
strength = composite > RMGI > GI
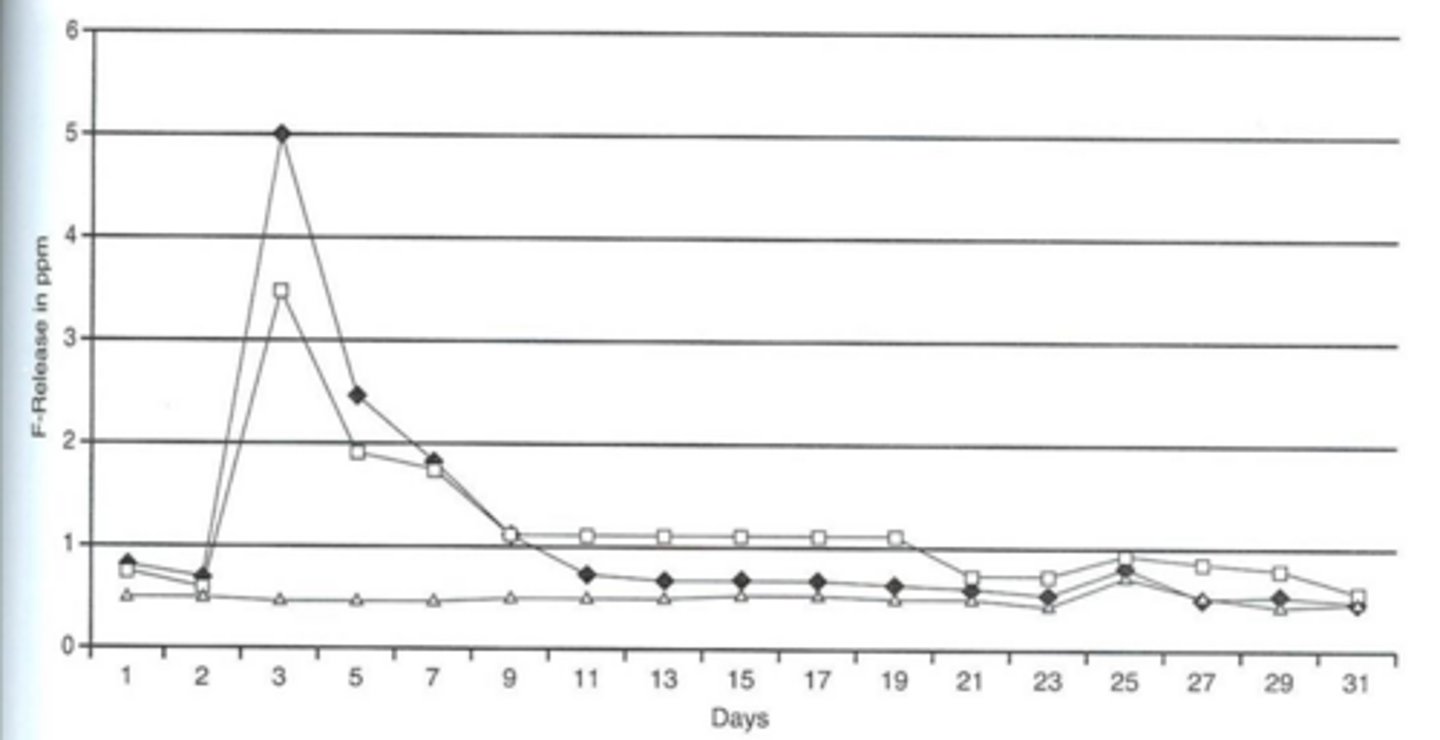
visual of fluoride releasing
fluoride recharging
process where dental materials absorb fluoride from external sources—such as toothpaste, mouthwash, or professional gels—and subsequently release it over time
tooth surface pre-treatment
- apply conditioner (polyacrylic acid) for 10 sec.
- rinse with water
- air dry
- avoid overdrying and any contamination
why use polyacrylic acid conditioner
removes smear layer without opening dentinal tubules & removing smear plugs
base and liners....
extend ideal prep to remove decay
prep is ready to receive liner & base

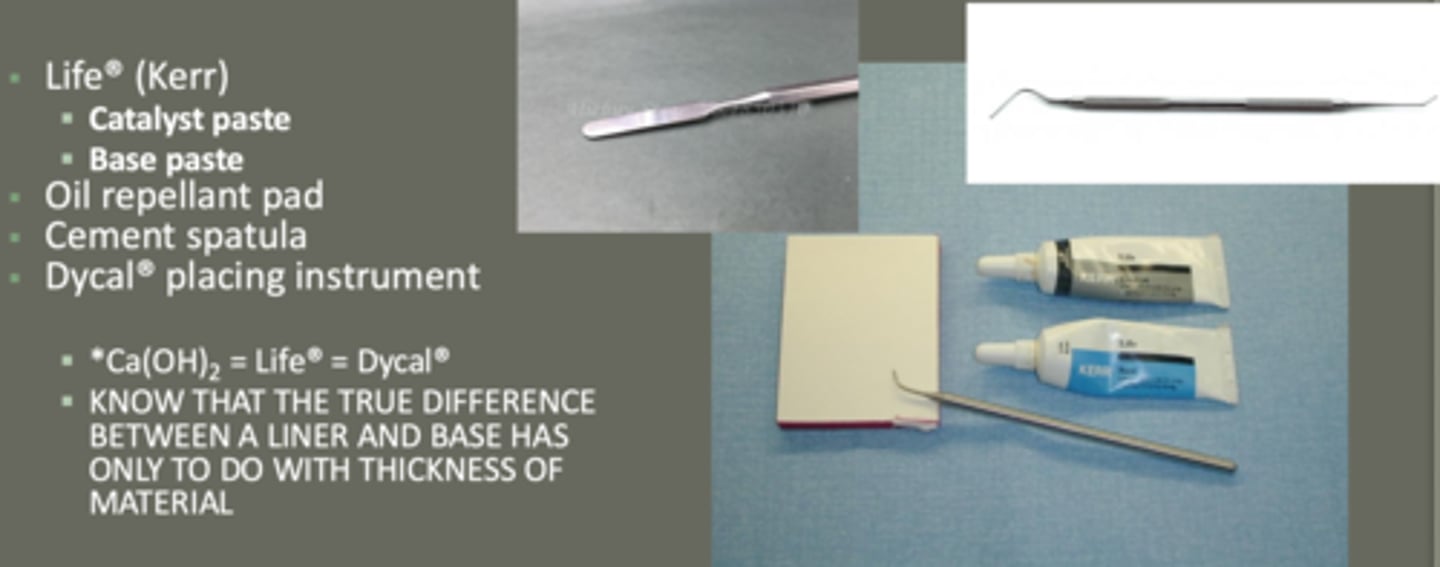
CaOH placement clinical steps--- mixing CaOH
equal parts base + catalyst
use cement spatula
DO NOT mix with placement instrument
* CaOH2 = Life = Dycal... true diff. between liners and base is only thickness*
place small, equal amounts of both pasts (____ and ____) on the oil repellant pad
catalyst, base
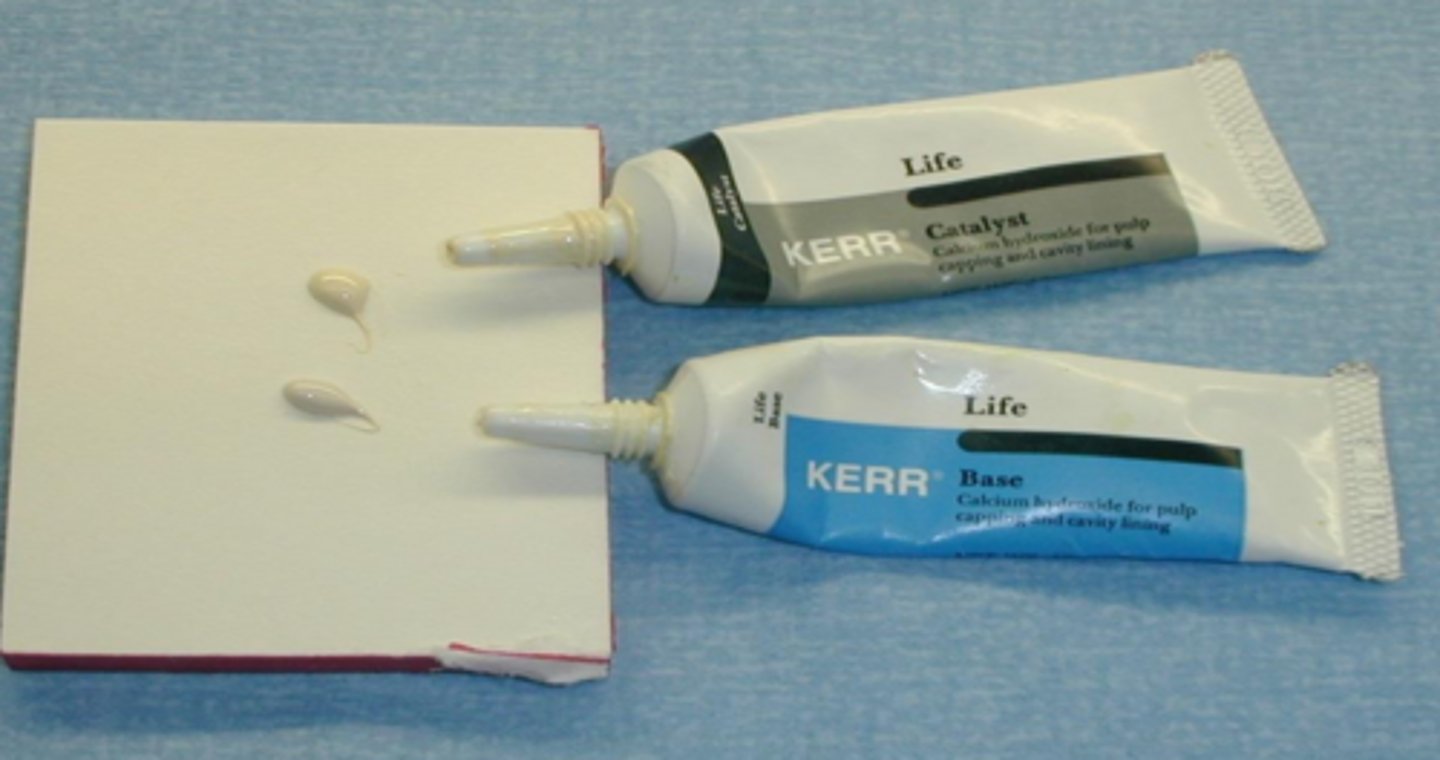
mix the two spates with a ____ ____, do not mix with the placement instrument
cement spatula
mix until a smooth, ____ colored mixture is obtained
uniformly

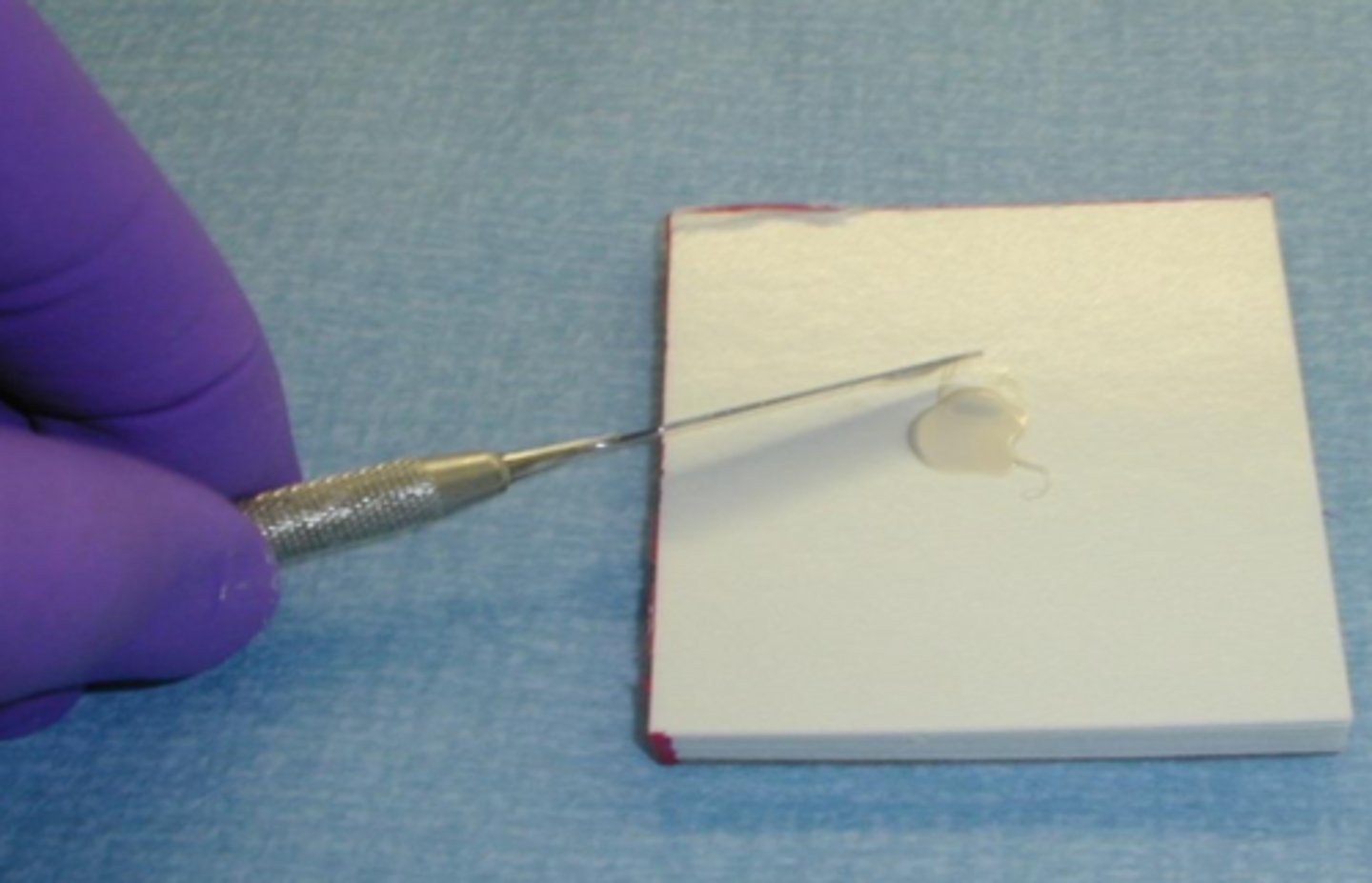
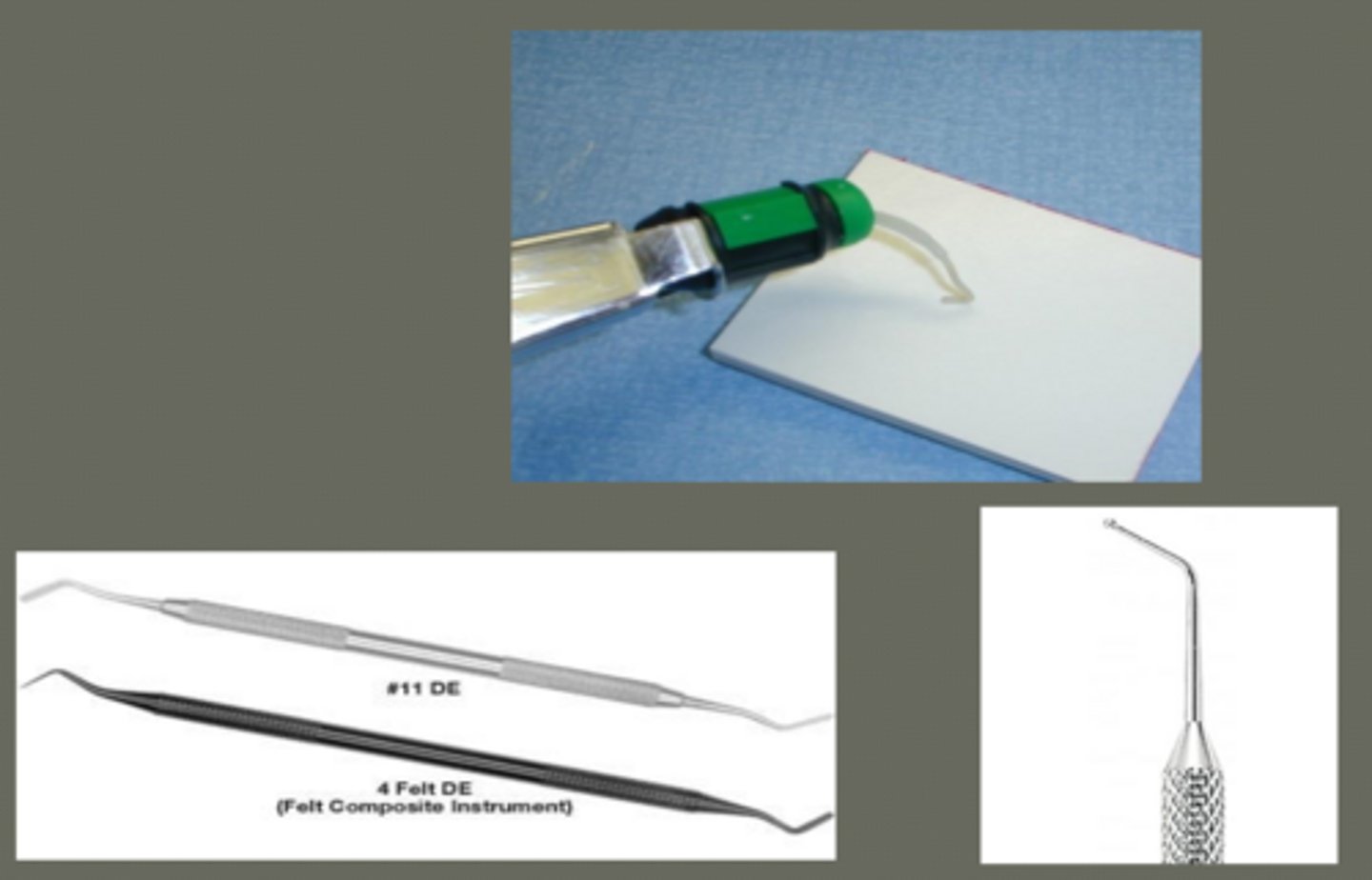
liner placement technique
small amount of mixed past on the ball tip of placing instrument
place only in deep portion of cavity prep.:
- pulpal floor
- axial wall
thin layer (on dentin closest to pulp)
wipe of the instrument before adding each ____ so that the material doesn't stick to the instrument
increment
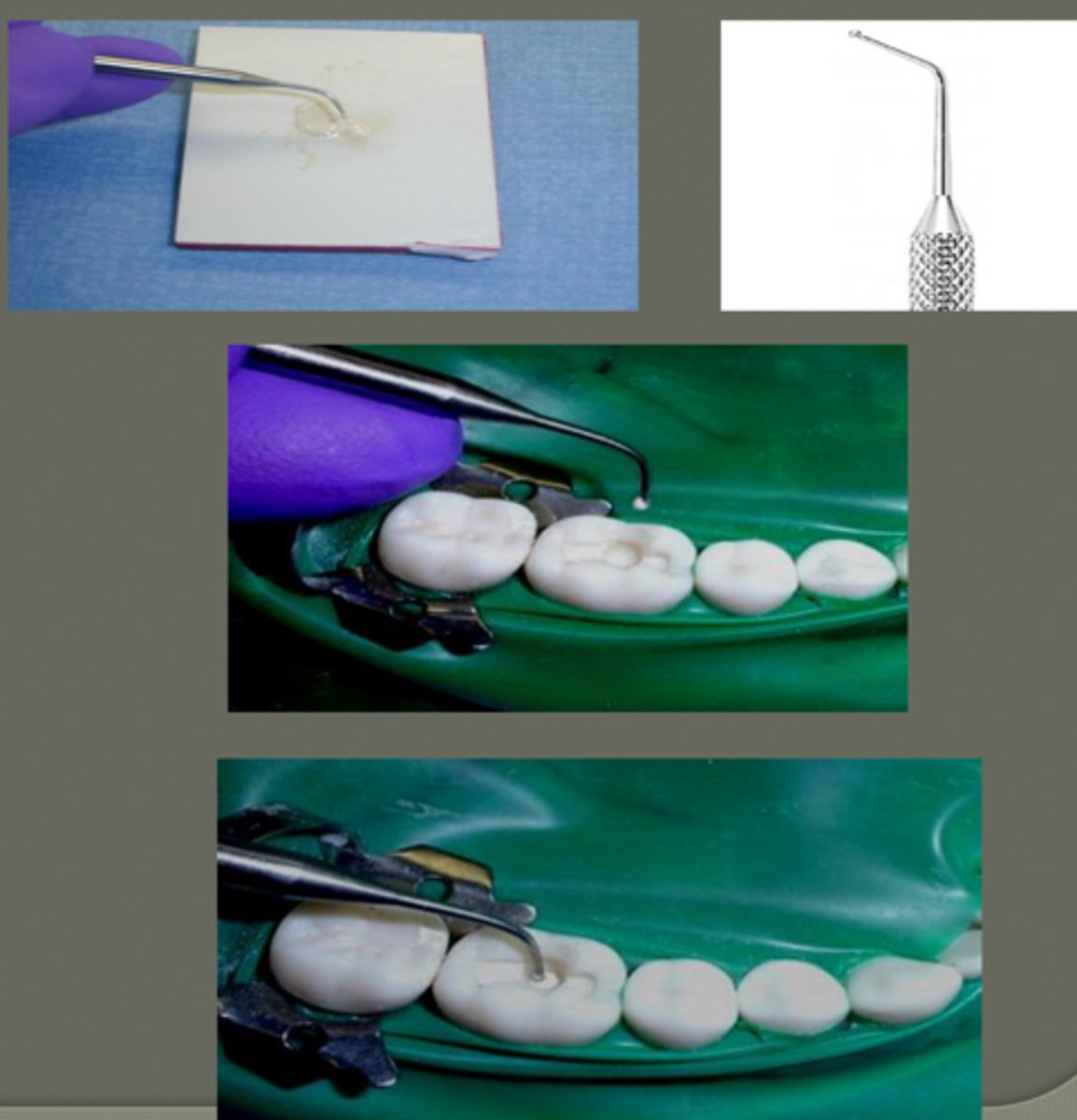
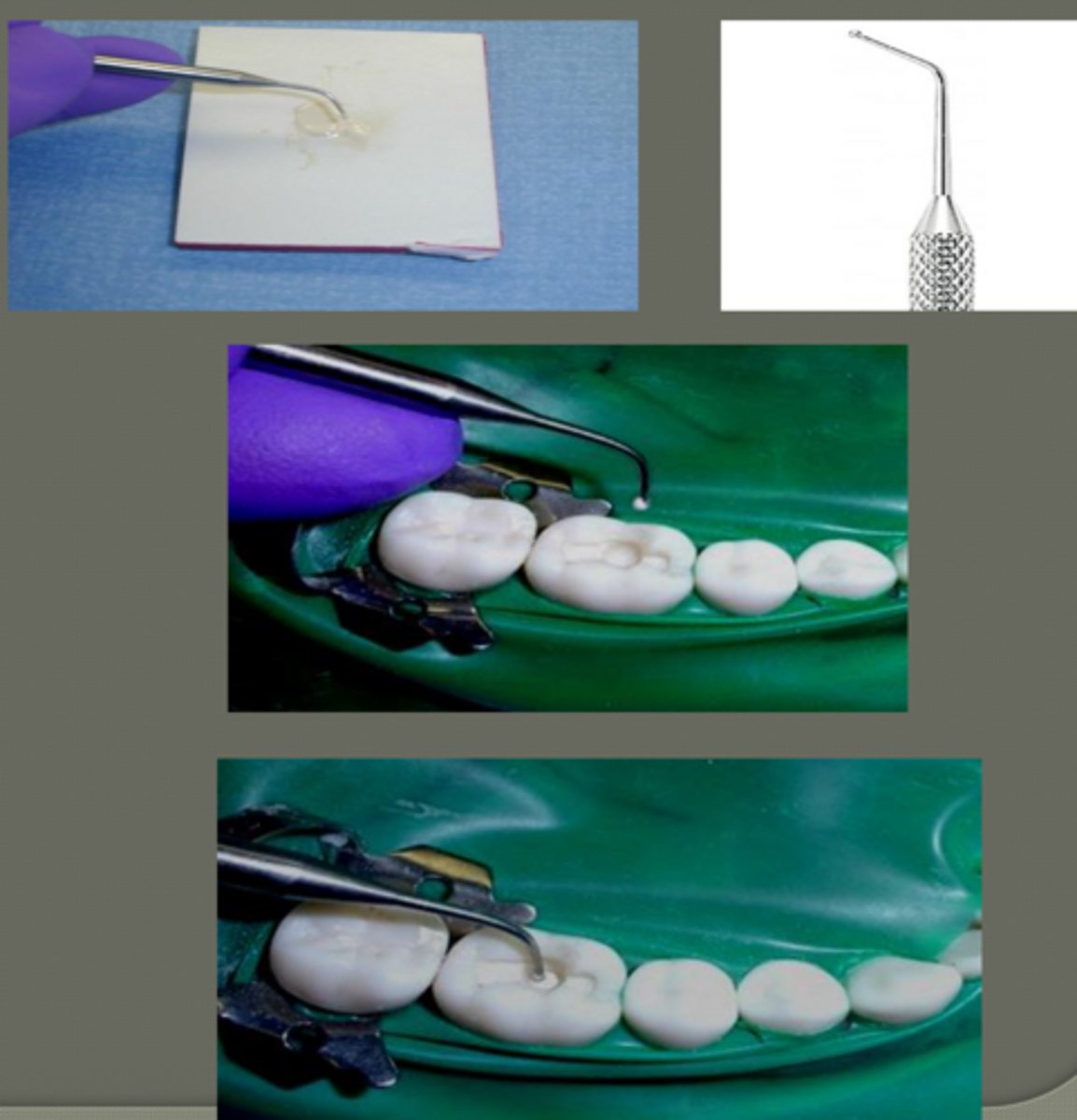
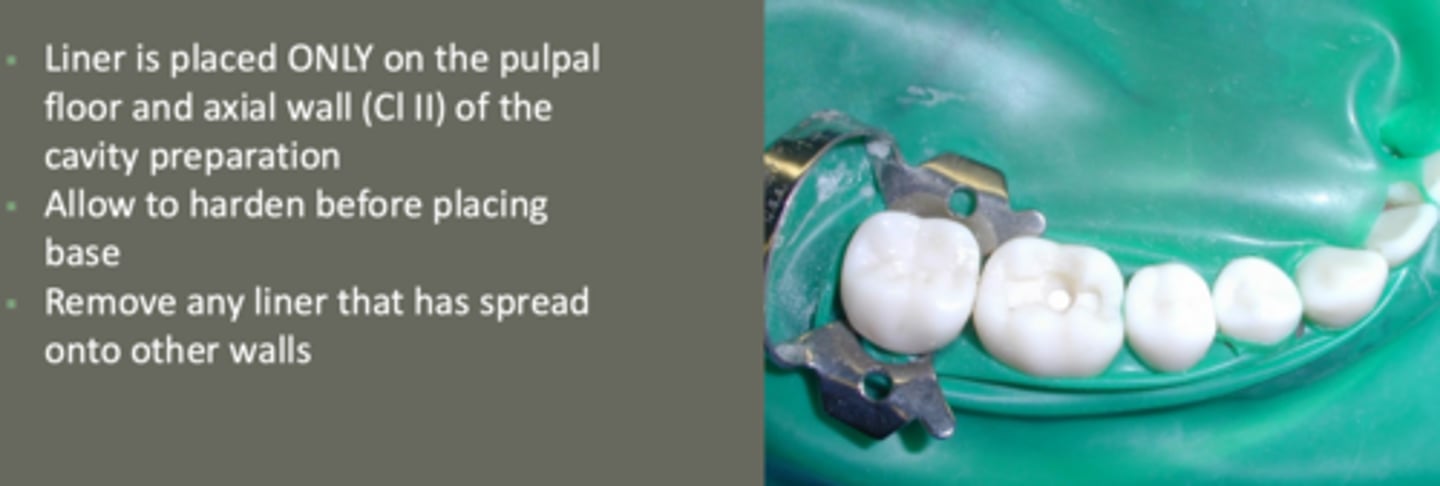
important rules of liner placement
- placed only on pulpal floor & axial wall (class II) of prep
- allow to harden before placing base
- remove any liner that has spread onto walls
bases/secondary liners
types of bases:
- EQUIA-Forte: self curing glass ionomer materia
- polyacrylic acid used before placement
ex. of secondary liner:
- Vitrebond: light curing resin modified glass ionomer material
- polyacrylic acid used before placement
where is conditioner placed (removal of dentin smear layer & improves GI bond strength)
around liner where GI will be placed... GI will bond to tooth structure
NOT on liner
steps:
- dispense form bottle onto a pad & apply with disposable applicator peripheral to liner
- rinse with water
- dry with 2-3 short bursts of air
- surface will appear matte
capsule activation steps of EQUIA Forte (base placement)
1. shake or tap capsule to loosen powder
2. activate by pushing plunger (hold for 2 secs)
- make sure it is flush with main body
- fully pressed to avoid incorrect mixing
3. set into amalgamator & mix for 10 secs

EQUIA-Forte mixing
mix in amalgamator
set at 10 seconds on rabbit speed
visual of activated capsule in the amalgamator/mixer
place _____ in syringe; extend the dispensing tube
capsule

placement of base
- extrude small amount of "test" material from capsule using syringe
- carry material to prep using a "plastic" instrument or Dycal
- condense once placed in prep.
EQUIA says to place directly due to its ___ ____ capabilities
bulk flow

base in prep ready for condensing visual

condensing base
- keep base away from walls
extent of base:
- amalgam: placed to block out undercuts & to keep amalgam 2 mm from pulp as thermal insulator
-composite: used as secondary liner btwn CaOH and composite
(protect CaOH from being washed away)

important notes for base placement
prep is ready for permanent restoration when:
- no excess material is on pulpal floor
- no base material is on walls of prep
maintain 2 mm from pulp (amalgam)
EQUIA will self cure in 2.5 mins
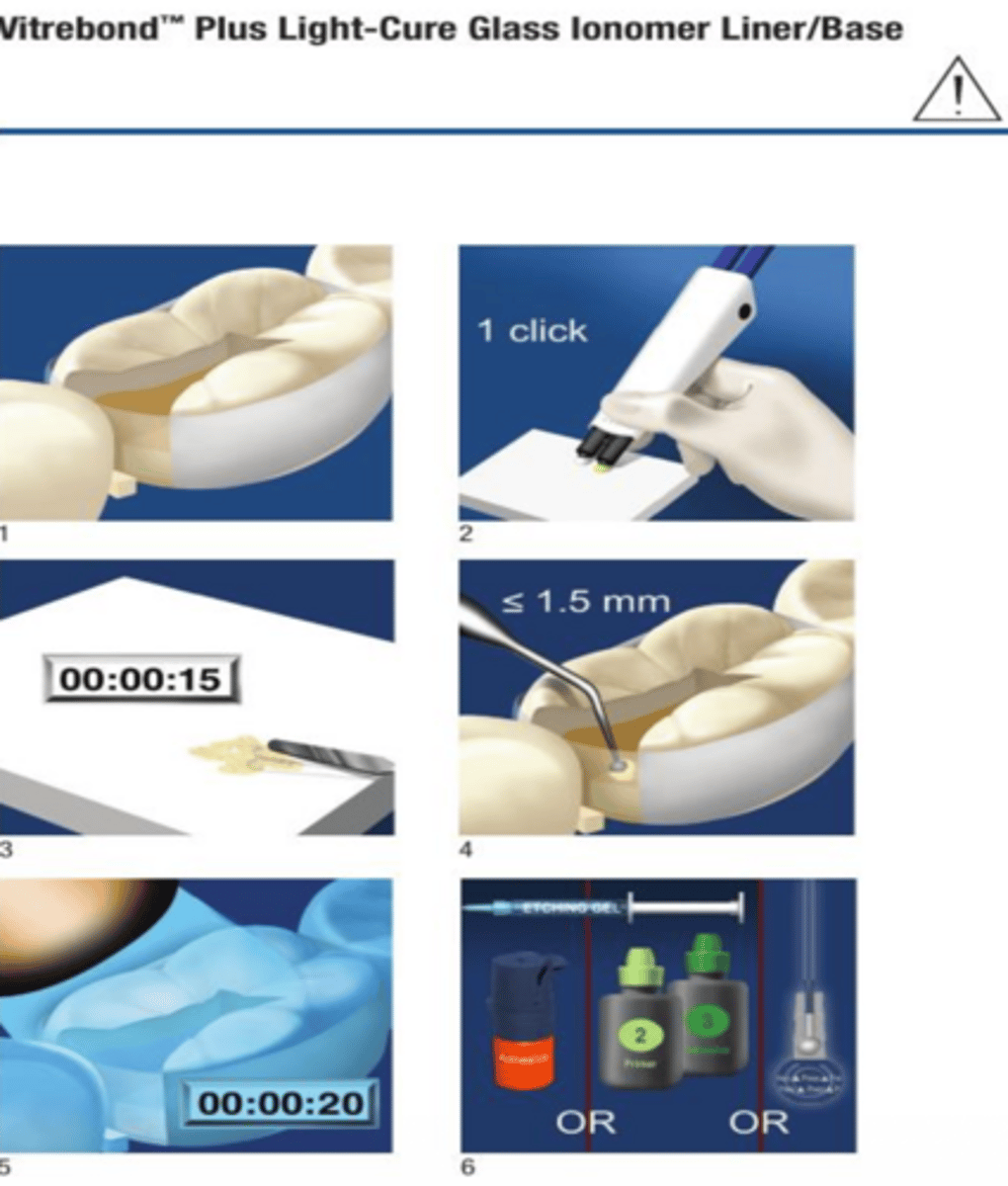
properties of RMGI Vitrebond
- reduces shrinkage
- strong dentin bond
- radioopaque
- light cure (20 secs)
- ease of dispense/placement similar to CaOH
use of RMGI Vitrebond
secondary liner/base
CAN'T be used as a final restorative material

Vitrebond Plus Light-Cure Glass Ionomer Liner/Base
visual

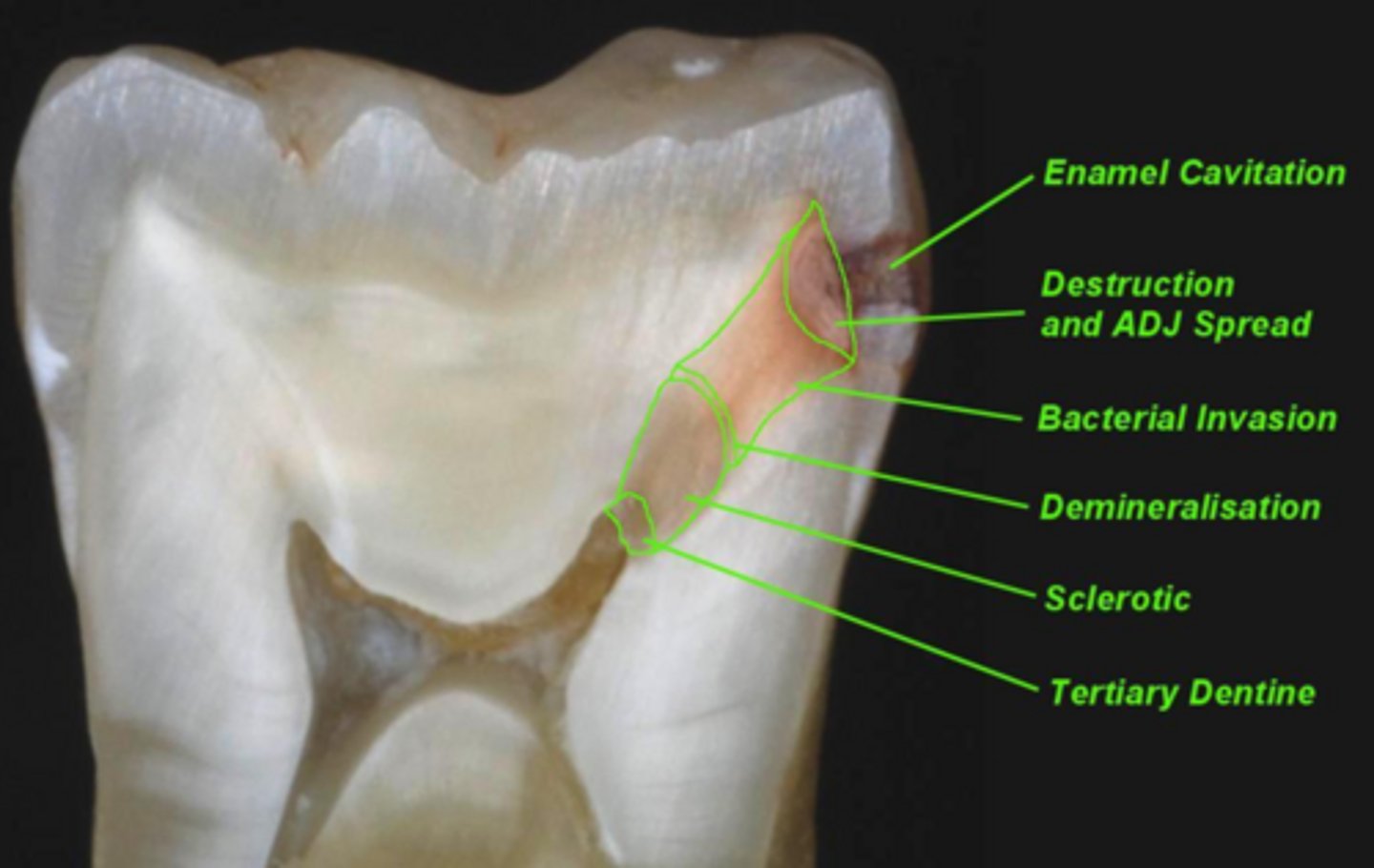
visual internal tooth tissues
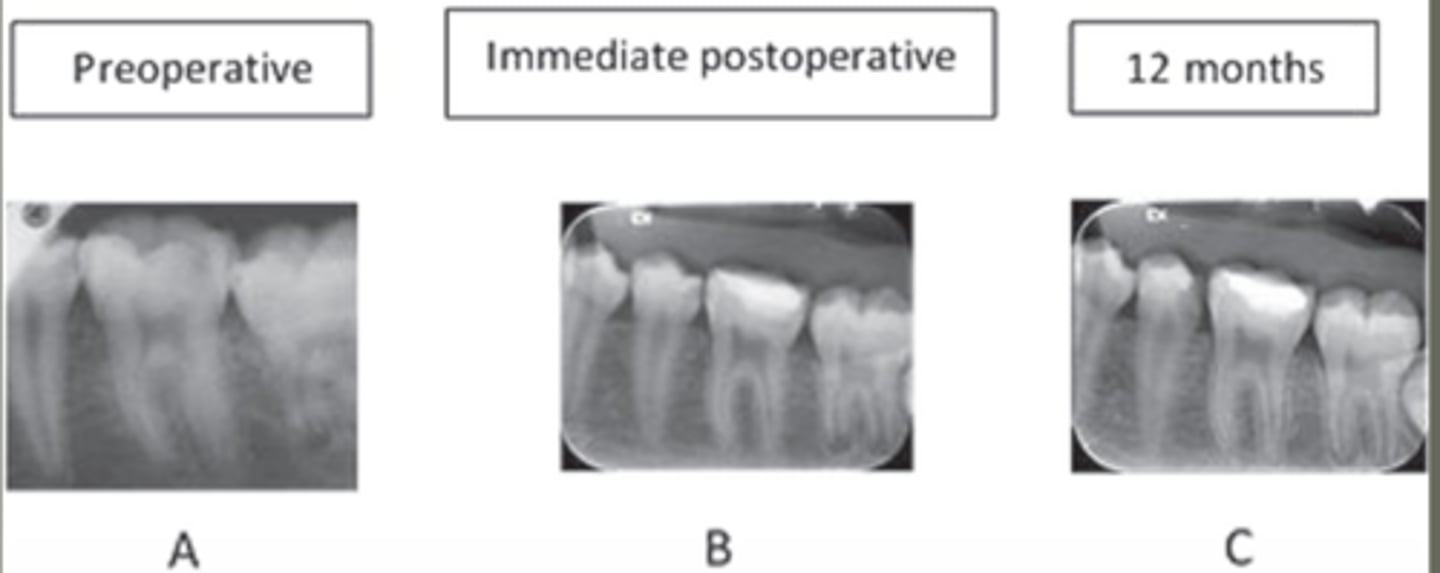
preoperative to 12 months post op progression
EQUIA Forte
glass hybrid with superior wear resistance and flexural strength
suitable for certain low compressive force areas
why is EQUIA Forte special ( new GI materials; advanced)
- high strength
- wear resistant
- resistant to acid erosion
- non sticky and packable
- no shrinkage
- high fluoride release & recharge capability
- better esthetics
- can be final restoration
available in 8 shades
clinical application of EQUIA Forte
- tooth prep
- pulp capping = CaOH beneath
- anatomical matrix system for class II
- rinse cavity prep w water
- blot dry with cotton pellet (do not desiccate... surface should appear moist)
restorative steps/tehcnique EQUIA Forte
- remove from mixer & load into GC capsule applier III
- 2 clicks to prime the capsule then syringe
- within 10 secs of mixing, extrude mixture directly into prep.
- form preliminary contour
moist dentin (no dessication)
working time ~ 1:15 mins from start of mixing at 23
avoid moisture contamination first 2.5 min
*higher temps will shorten working time*

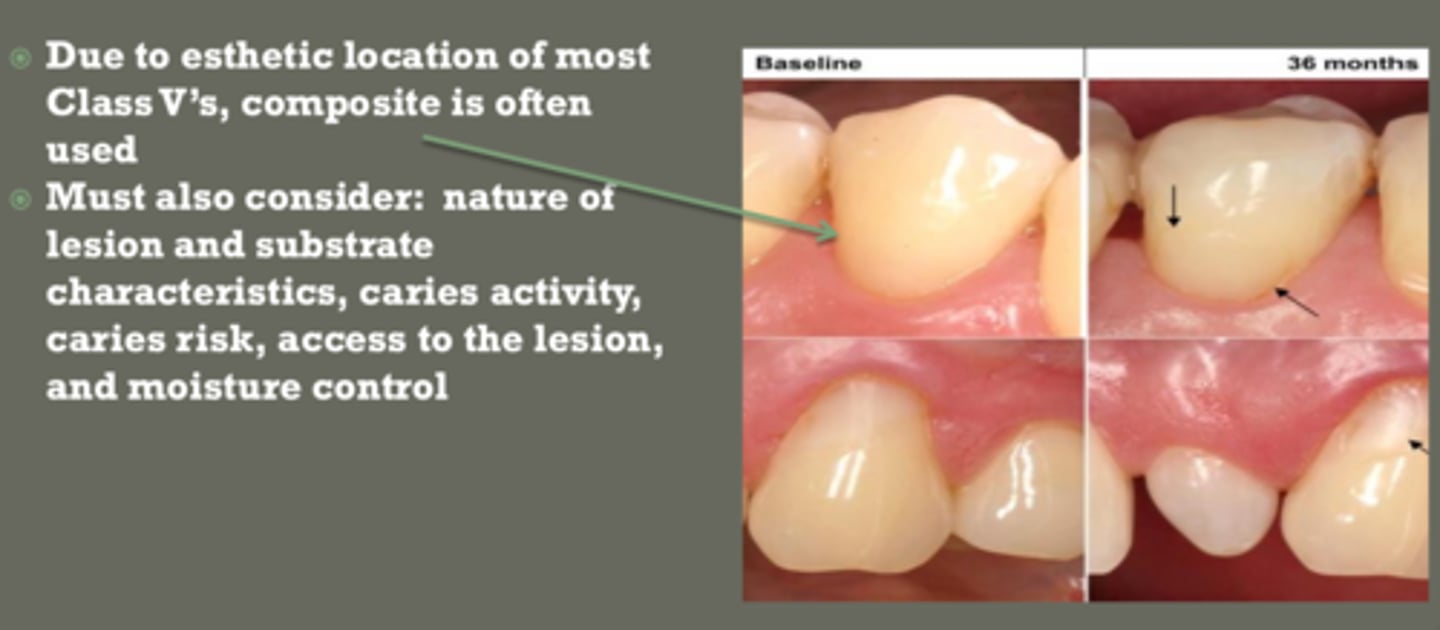
class V material selection
use composite in esthetic zones
use GI:
- poor isolation
- high caries risk
- NCCLs
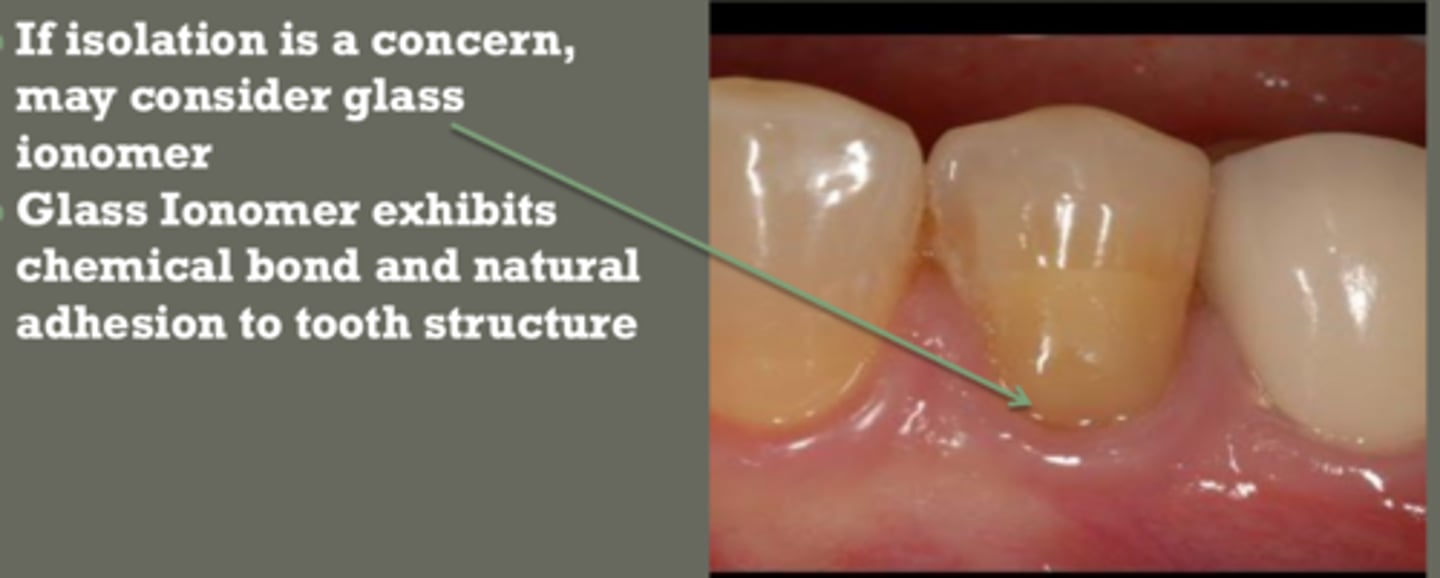
if isolation is a concern in class V restoration, probably use _______ ____ because significantly less sensitive to moisture than composite resin
glass ionomer
(GI exhibits chemical bond & natural adhesion to tooth structure)
material of choice for NCCL
esthetics not primary focus
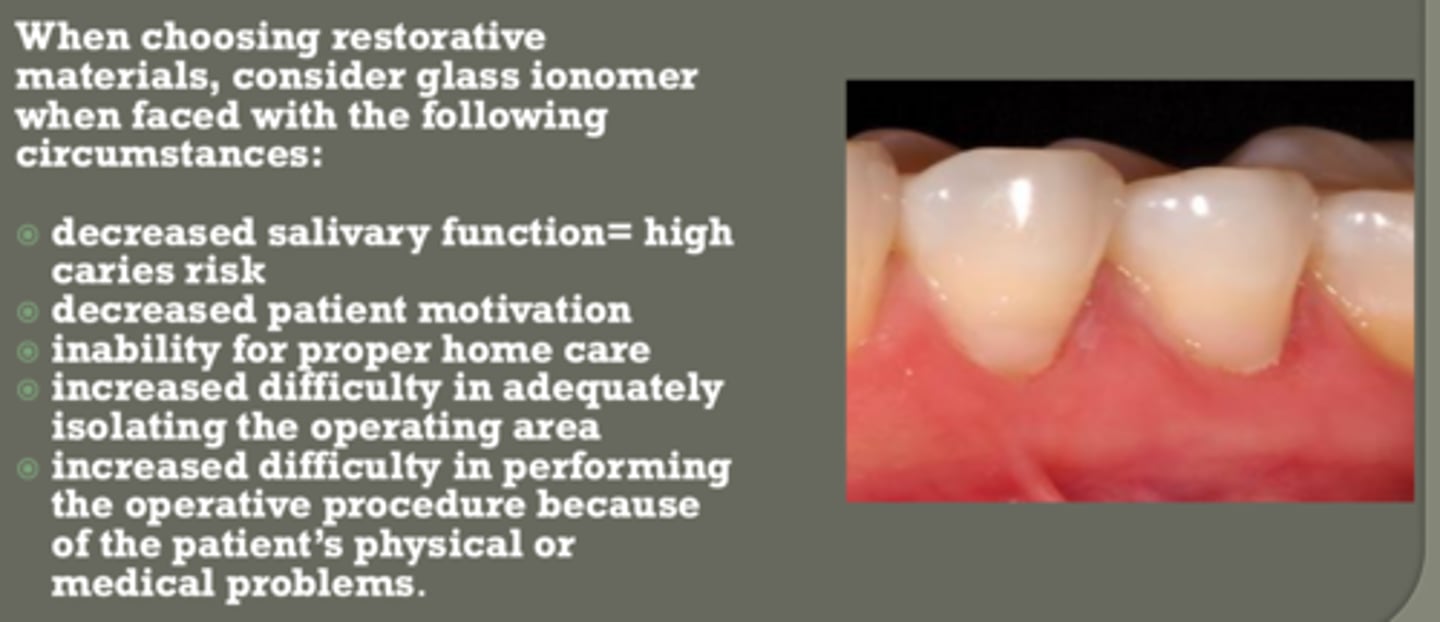
consider glass ionomer when faced with the following situations
- decrease salivary function = high caries risk
- decrease patient motivation
- inability for proper home care
- increased difficult in isolation
- increased difficult in performing op. procedure bc pt physical or medical problems
finishing and polish GI
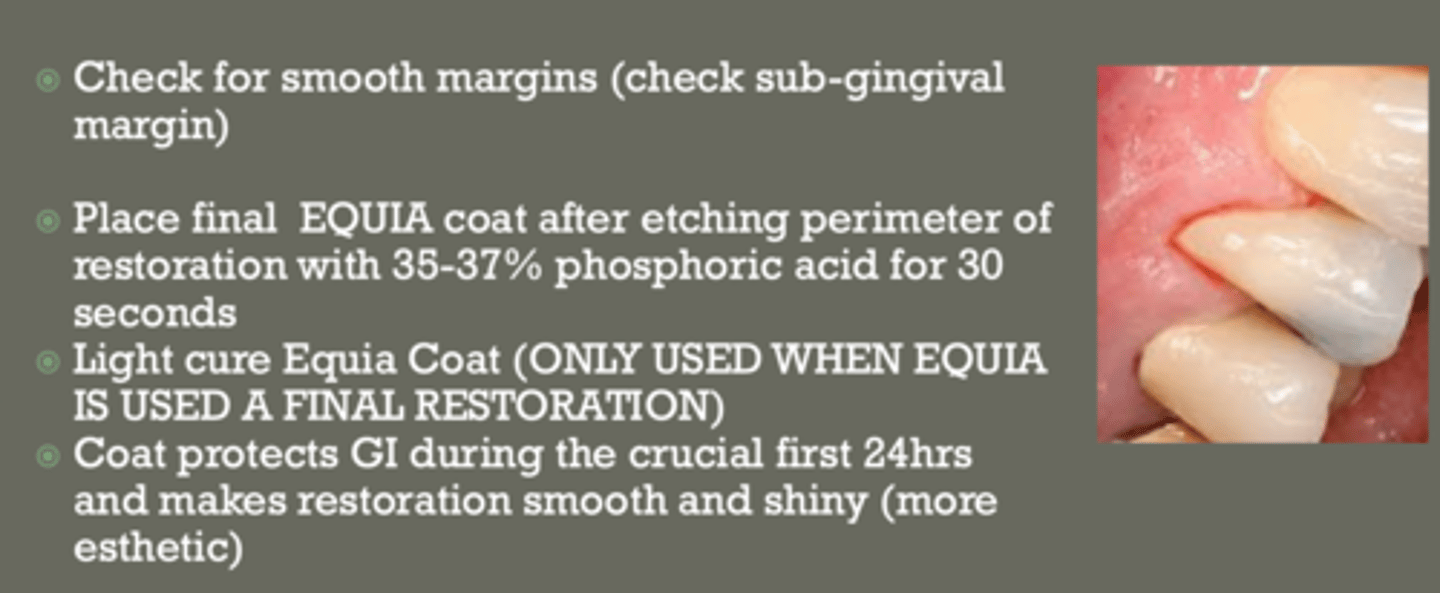
- check for smooth margins (sub gingival as well)
- place final EQUIA coat after etching perimeter of restoration w 35-37% phophoric acid for 30 secs
- light cure Equia coat = only when used as final restoration
- coat protects GI during the crucial first 24 hrs & makes restoration smooth and shiny (more esthetic)
when do you light cure EQUIA coat
only when it is used as a final restoration material
amalgam summary
moderate caries removal:
- base as thermal insulation
- no liner
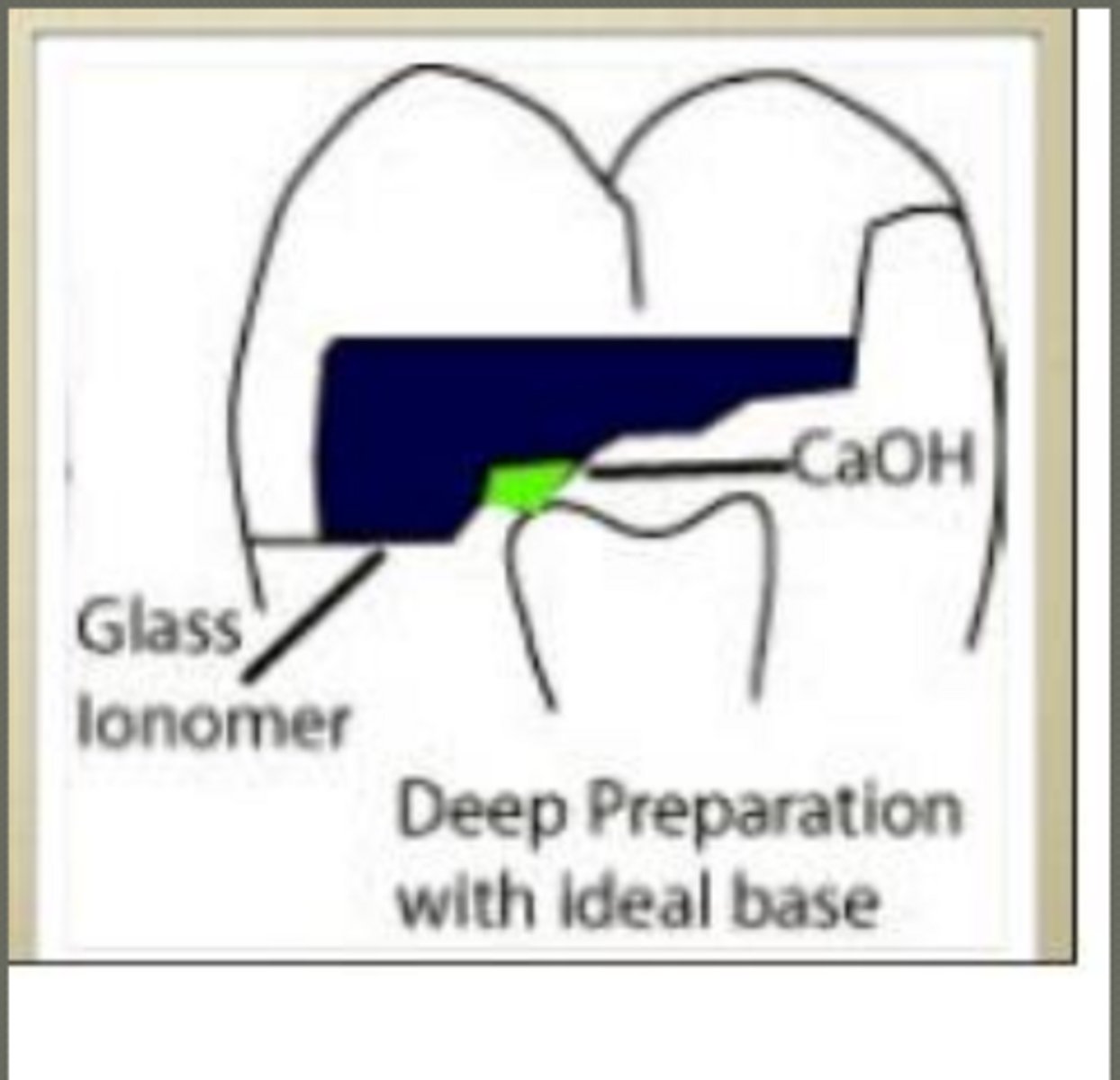
deep caries removal:
- CaOH liner
- base as thermal insulator
any depth prep... can use DBA to seal dentinal tubules
(not required, but would apply DBA right before amalgam)
liners and secondary liners composite summary
deep caries removal:
- CaOH as liner
- GI as secondary liner
what must be placed before composite
DBA (always)
follow guidelines for particular DBA technique (our clinic uses selective etch)
what is selective caries removal
leave soft dentin over pulp to avoid exposure
aka indirect pulp cap
must start with asymptomatic vital tooth
benefits of selective caries removal
- maintains vitality of pulp by preventing pulp exposure
- apply minimally invasive (MI) techniques
- decrease financial burden on pt.
- restore tooth health
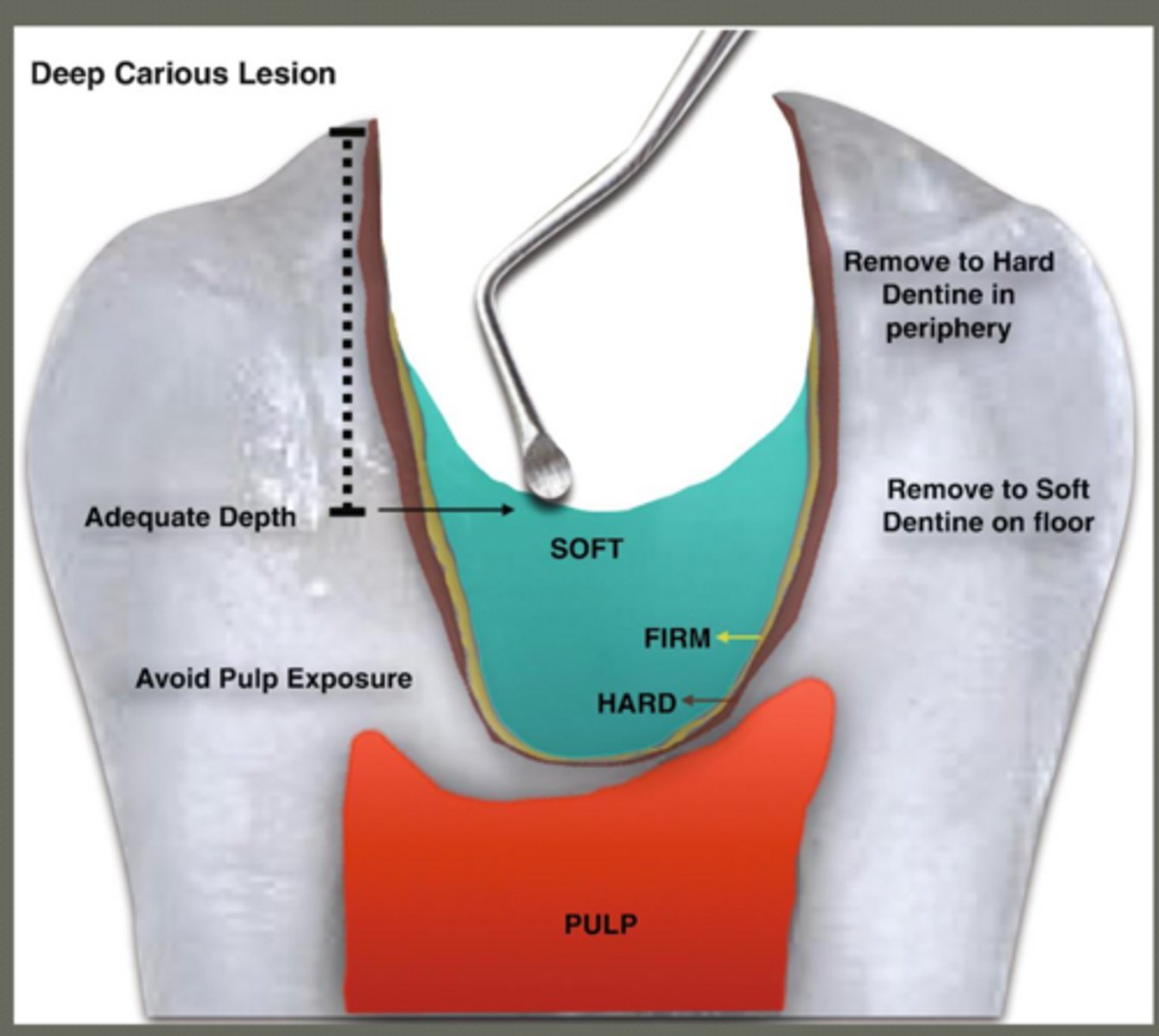
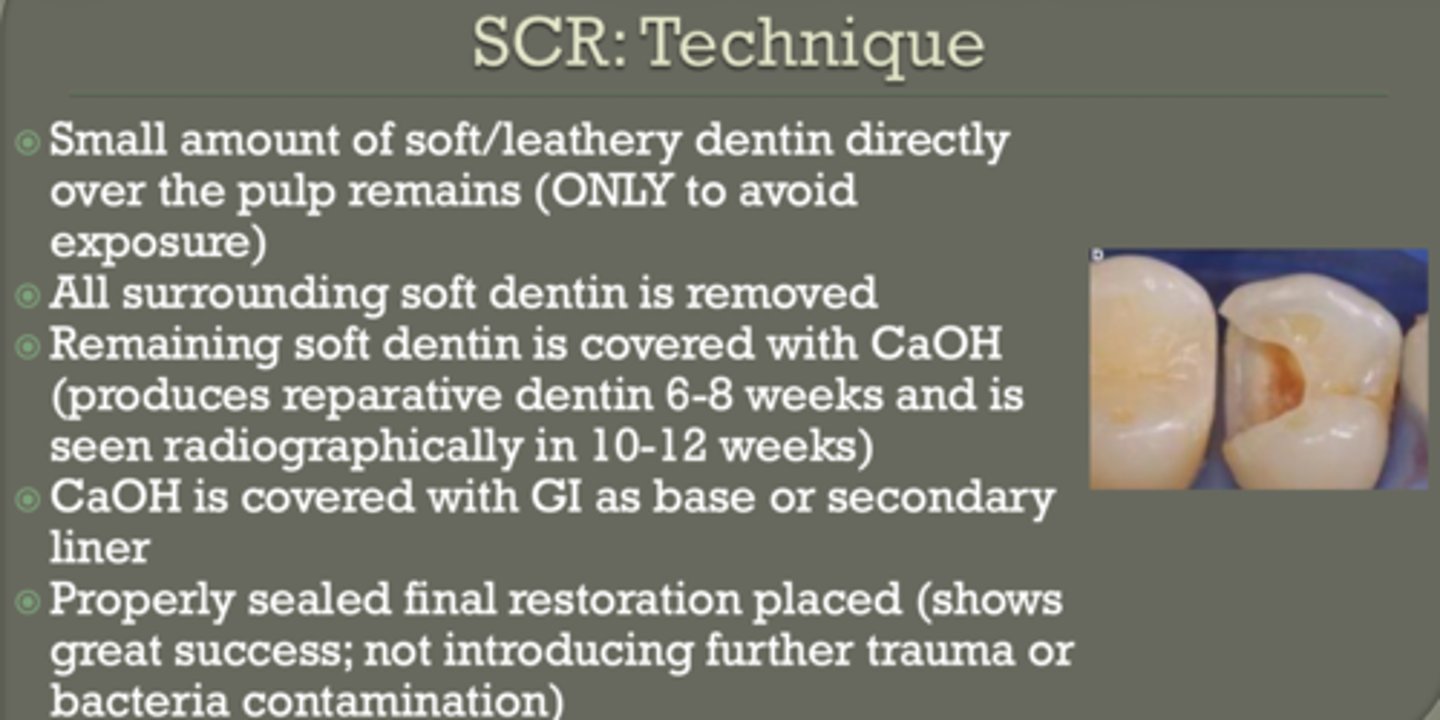
steps of SCR
- remove surrounding caries
- leave soft dentin at pulp (or leathery... only to avoid exposure)
- cover with CaOH
- cover with GI
- seal restoration ( no trauma or bacteria contamination)
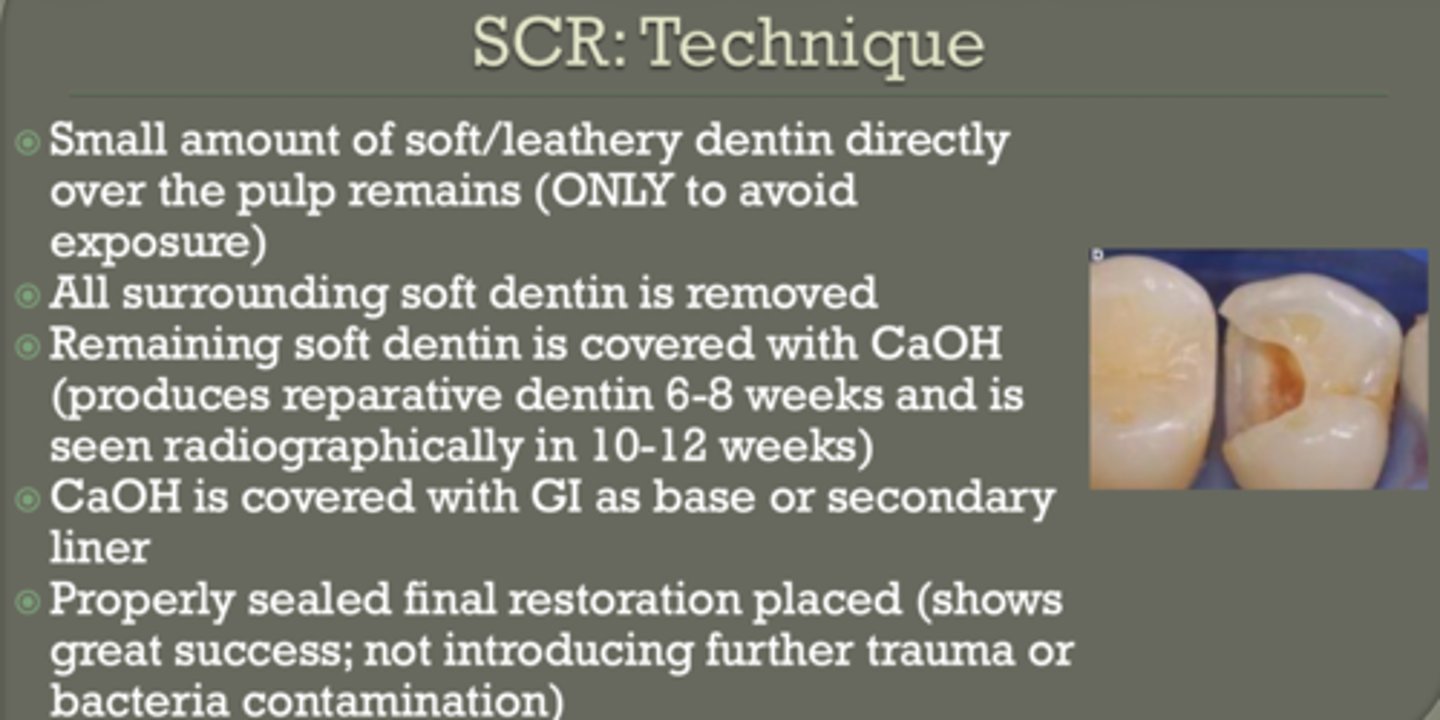
covering soft dentin with CaOH in SCR
produces reparative dentin 6-8 weeks
seen radiographically in 10-12 weeks
favorable prognosis conditions for direct pulp cap
- asymptomatic tooth
- small exposure (< 0.5 mm)
- controlled bleeding
- clean field (rubber dam)
- minimal trauma, little desiccation of tooth occurred, no aspiration of blood into dentin (dentin blushing)
treat exposure with CaOH to form reparative dentin
important concepts
Liner vs Base = THICKNESS ONLY
CaOH:
-stimulates reparative dentin
-MUST be covered
GI:
- chemical bond (chelation)
deep dentin:
-poor bonding → use RMGI
composite:
-ALWAYS needs DBA
amalgam:
-needs thermal insulation (base)