4 SCL+Material+Properties-ACC
1/74
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
75 Terms
What is a polymer and what are its key structural characteristics?
Polymers = repeating monomer units forming long chains.
Characteristics: long chains, high molecular weight, covalent (not ionic) bonds.
What distinguishes a homopolymer vs a copolymer?
Homopolymer: same monomer repeated, typically linear (e.g., PMMA)
Copolymer: ≥2 different monomers in one polymer (common in modern materials)
What is cross-linking in polymers and how does it affect properties?
Cross-linking = covalent bonds between polymer chains.
Effect: ↑ durability/strength, ↓ flexibility (decreased “DK”/mobility)
How does increasing cross-linking affect polymer behavior clinically/material-wise?
More cross-linking → more rigid, durable material with less permeability/flexibility.
Compare PMMA vs pHEMA in terms of structure and material properties.
PMMA: hydrophobic, rigid, low water content
pHEMA: hydrophilic (–OH groups), absorbs water → soft, flexible hydrogel
What are the two physical states of soft contact lens (SCL) materials and what defines them?
Xerogel: dry state
Hydrogel: wet state with water imbibition
What is imbibition in hydrogel lenses and how does it affect oxygen transport?
Imbibition = water uptake into lens
Effect: ↑ water content → ↑ dissolved O₂ transport through contact lens
What is the typical water content range of hydrogel contact lenses and its significance?
~38–74% water → higher water content → more oxygen delivery but softer material
What is ionicity in contact lens materials and why does it matter?
Ionicity = surface charge of the material
Determines interaction with tear film → affects deposit formation
Compare ionic vs non-ionic contact lenses (mechanism + deposits).
Ionic: negative surface charge → attracts positively charged proteins/lipids → ↑ deposits
Non-ionic: neutral surface → repels charged molecules → ↓ deposits
What are the key properties and limitations of PolyHEMA (first soft lens material)?
Type: hydrogel (HEMA-based)
Advantages: cheap, machinable, durable, dimensionally stable
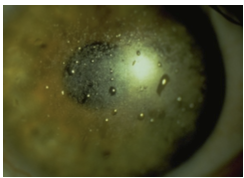
Major disadvantage: low Dk → poor oxygen transmission → edema, vascularization
Why is low Dk clinically important in hydrogel lenses?
Low Dk → ↓ O₂ transmission → hypoxia → corneal edema, neovascularization, complications
What are standard hydrogel (non-silicone) lenses used for and how are they made?
First soft lens materials
Manufactured via lathe cutting or molding
Used commonly for daily lenses + myopia control
Less expensive than silicone hydrogels
How do water content, ionicity, and deposits relate in hydrogel lenses?
High water + ionic → highest protein deposits
Low water + non-ionic → most deposit resistant
What are the key material advantages of silicone hydrogel (SiHy) lenses?
↑ Dk (oxygen permeability) via siloxane
↓ hypoxic complications (↓ edema, neovascularization)
↓ dehydration vs traditional hydrogels
What are the main disadvantages of silicone hydrogel lenses?
Hydrophobic → not inherently wettable (needs surface treatment/wetting agents)
↑ mechanical complications (stiffer modulus)
Still prone to deposition
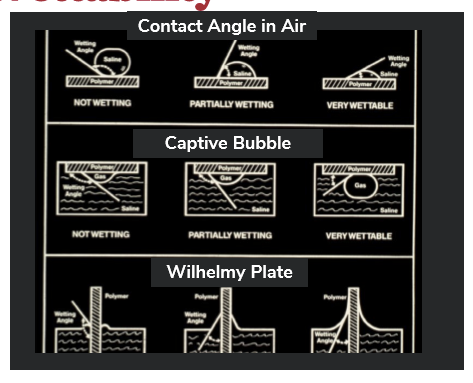
What determines surface wettability in contact lens materials?
Wettability is evaluated by contact angle → smaller angle = better wettability
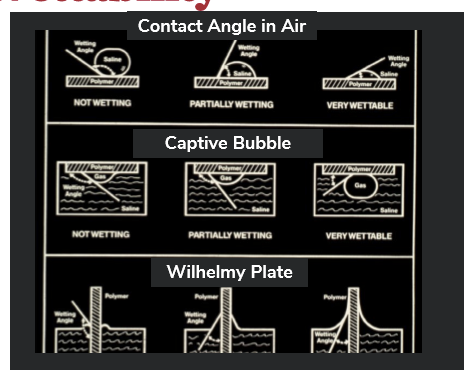
What are the three main laboratory tests for wettability?
Contact angle (in air)
Captive bubble
Wilhelmy plate
What is the role of surface treatments in silicone hydrogel lenses?
Improve wettability of hydrophobic silicone
Create hydrophilic surface layer (e.g., plasma treatment)
Enhance comfort and tear film stability
Why do silicone hydrogels require surface treatments?
Silicone = hydrophobic → poor wettability → surface modification needed to allow tear spreading
What are the main strategies used to improve silicone hydrogel wettability?
Plasma surface treatments → hydrophilic outer layer
Internal wetting agents (monomers in copolymer) → built-in hydrophilicity
Permanent water surface coatings → stable hydrophilic surface
How does plasma treatment improve wettability in silicone hydrogel lenses?
Cold plasma modifies the lens surface → creates hydrophilic layer → ↓ contact angle → ↑ wettability
What is plasma in the context of lens surface treatment?
Highly ionized gas (4th state of matter)
Contains free electrons
Used to chemically modify lens surface in a reaction chamber
Why are multiple wettability strategies needed in silicone hydrogels?
Silicone = hydrophobic → poor natural wettability → requires:
Surface modification (plasma) → modifies surface
Internal wetting monomers → hydrophilic monomers in polymer
Coatings → ensure stable tear film + comfort → hydrophilic outer layer
What are key monomers used as internal wetting agents?
Monomers: PVP (polyvinyl pyrrolidone), hyaluronic acid
How do permanent water surface coatings improve wettability?
Hydrophilic (non-silicone) outer layer over silicone core
Creates high water content at surface → excellent wettability
Why is water gradient technology clinically beneficial?Why is water gradient technology clinically beneficial?
Combines high oxygen permeability (SiHy core) + high surface wettability
↓ dryness, ↑ comfort (tear-like surface)
Mimics natural tear film better than standard SiHy
How does water gradient differ from other wettability strategies?
Not just surface treatment → true gradient from core → surface
Highest surface water content of all lens types
More advanced than plasma or internal wetting agents
How is % water content of a contact lens defined and measured?
% water = (wet weight − dry weight) / wet weight
Measured before and after oven drying
Can also estimate via refractometer (water = 100% − solid content)
How does water content relate to dehydration in hydrogel lenses?
Higher free water content → more dehydration
More water = more water loss to environment
How are the FDA soft contact lens material groups classified?
Based on:
Water content: low (<50%) vs high (>50%)
Ionicity: non-ionic vs ionic
What are the four FDA hydrogel groups (I–IV)?
Group 1: Low water, non-ionic
Group 2: High water, non-ionic
Group 3: Low water, ionic
Group 4: High water, ionic (MOST deposits)
What is FDA Group 5?
Silicone hydrogels (SiHy) → separate category due to silicone → ↑ Dk (oxygen)
Which FDA group has the highest protein/chemical deposition and why?
Group 4 (high water + ionic)
Ionic → attracts proteins
High water → absorbs molecules → MOST deposition
How does water content affect hydrogel lens properties (Groups 1–4)?
High water (>50%) → ↑ Dk, ↑ flexibility, ↑ thickness
BUT → ↑ dehydration, ↑ deposits, ↓ dimensional stability, harder careLow water (<50%) → ↓ Dk, ↑ rigidity, ↓ thickness
BUT → ↓ dehydration, ↓ deposits, ↑ stability, easier care
What is the tradeoff with high vs low water hydrogel lenses?
High water: better oxygen (Dk) but worse dehydration + deposits
Low water: better stability + comfort (less drying) but lower Dk
Why are silicone hydrogels their own FDA group?
Opposite relationship vs hydrogels
Hydrogels: ↑ water → ↑ Dk
SiHy: LOW water but HIGH Dk (oxygen through silicone, not water)
Compare Dk relationship in hydrogels vs silicone hydrogels.
Hydrogels: Dk ∝ water content
Silicone hydrogels: Dk independent of water (silicone provides O₂)
→ allows low water + high oxygen
What is the significance of water gradient lenses in classification?
May form separate category
Combine SiHy core (high Dk) + high-water surface (comfort)
→ best of both systems
What is Dk in contact lenses?
Dk = oxygen permeability of the material
D (diffusion) = ability of O₂ to move through material
K (solubility) = how much O₂ dissolves in material
What is oxygen transmissibility and how is it calculated?
Dk/t (or Dk/L)
Accounts for lens thickness (t)
Determines actual oxygen reaching cornea
How do high minus vs high plus lenses affect oxygen transmission?
High minus: thin center → ↑ central O₂
High plus: thick center → ↓ central O₂ → ↑ hypoxia risk
What Dk/t values are needed for daily wear and overnight wear?
Daily wear: ~25
Overnight/extended wear: ~85–135 (87)
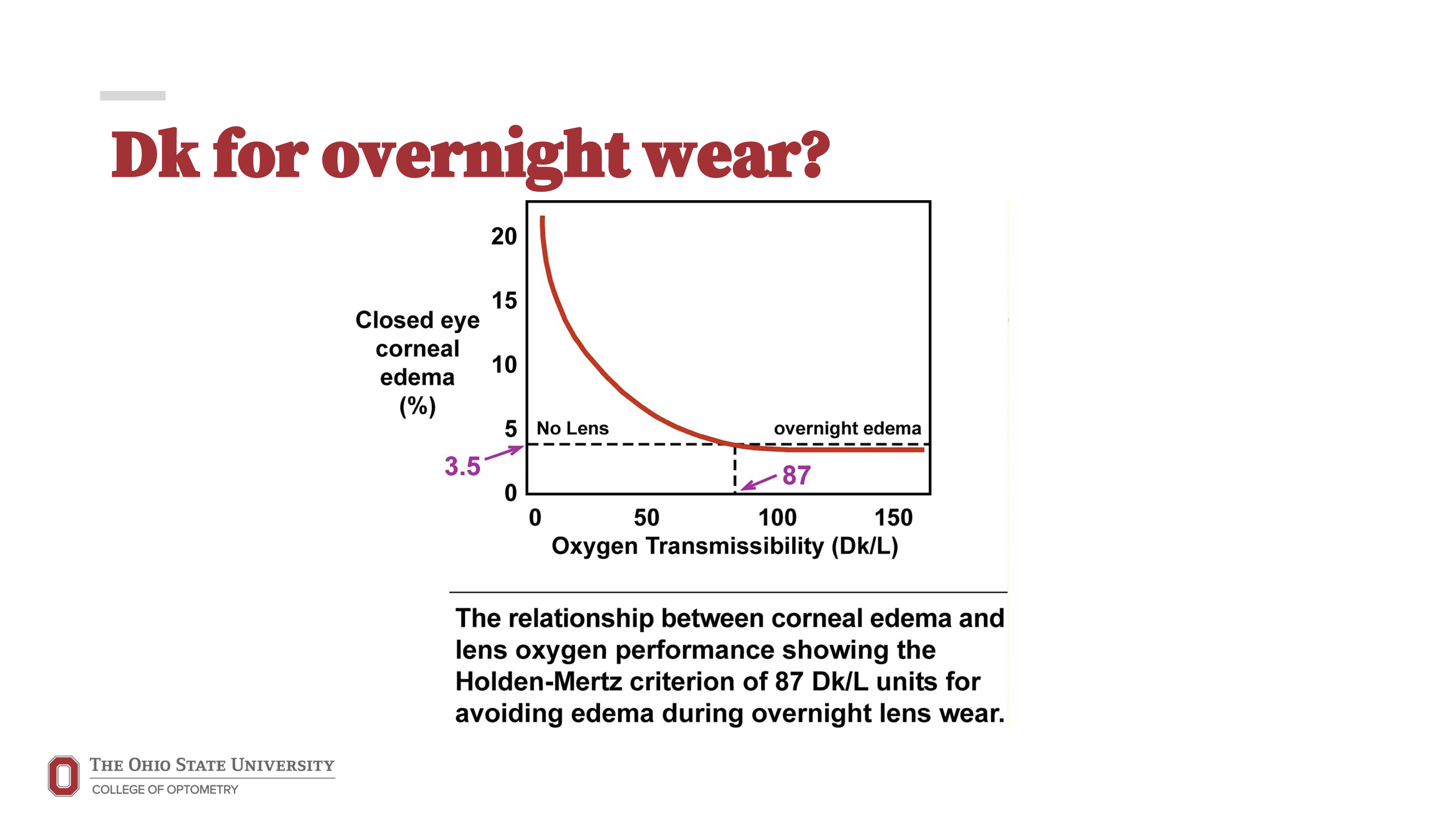
How much does the cornea swell overnight without contact lenses?
~4% swelling overnight (normal baseline)
How does tear exchange contribute to oxygen delivery and why are GP lenses better?
~25% tear volume turnover per blink
GP lenses allow tear exchange under lens → improves O₂ delivery
What is Equivalent Oxygen Percentage (EOP)?
Compares corneal O₂ uptake with lens vs no lens (open eye)
Measured with electrode
Reflects effective oxygen reaching cornea
How does Dk relate to EOP?
Higher Dk → higher EOP → more oxygen available to cornea
How can Dk be increased in soft contact lenses?
Increase water content (hydrogels)
Increase silicone content (silicone hydrogels)
How does increasing water content affect Dk in standard hydrogel lenses?
↑ water content → ↑ Dk (oxygen carried through water)
First strategy used
Limited by ↑ dehydration + deposits
How does increasing silicone content affect Dk in silicone hydrogels?
↑ silicone → ↑ Dk (oxygen dissolves in silicone)
Works even with low water content
Requires wettability treatments (silicone is hydrophobic)
Why did silicone hydrogels replace high-water hydrogels for oxygen delivery?
Achieve high Dk WITHOUT high water
Avoid dehydration + deposit issues of high-water lenses
→ Better overall oxygen + comfort balance
How does water content affect Dk in standard hydrogel lenses?
Increasing water content → ↑ Dk
Oxygen is carried through water phase
How does Dk change with water content in hydrogels vs silicone hydrogels?
Hydrogels: ↑ water → ↑ Dk (direct relationship)
Silicone hydrogels: ↑ water → ↓ Dk (inverse relationship; silicone drives oxygen)
Why is increasing water content not ideal long-term for improving Dk?
Back:
Improves oxygen BUT → worsens comfort, deposits, stability
Led to shift toward silicone hydrogels
What material properties determine durability and dimensional stability in contact lenses?
Hardness (RGPs, sclerals)
Modulus (stiffness)
Toughness (resistance to fracture)
What is modulus in contact lens materials and why is it important?
Modulus = stiffness (slope of stress–strain curve, MPa)
Higher modulus → more rigid lens
Important for masking astigmatism
How does cross-linking affect lens stiffness and durability?
More cross-linking → ↑ stiffness (↑ modulus)
↑ durability / dimensional stability
BUT ↓ oxygen transmissibility (less permeability)
What is the tradeoff between stiffness and oxygen transmission in contact lenses?
↑ stiffness (more cross-linking)
→ ↑ durability, shape retention
→ ↓ O₂ transmission (↓ Dk/t)
Why can high-modulus lenses cause more mechanical complications?
Stiffer lenses interact more with ocular surface → ↑ risk of mechanical irritation (e.g., SEALs)
What is modulus in contact lenses?
Stiffness (MPa) = slope of stress–strain curve
Higher modulus = stiffer lens
Lower modulus = softer, more flexible lens
How does water content affect modulus in soft lenses?
More water → ↓ modulus → less stiff
What are the effects of lower modulus (less stiff) lenses?
Move less on eye
More difficult to handle
Often more comfortable
How do thickness and modulus affect lens handling?
↑ thickness → ↑ rigidity (dramatic: doubling thickness → ~8× stiffness)
Easier handling with:
Thicker lenses
Higher modulus (stiffer)
How does cross-linking affect modulus and oxygen transmission?
More cross-linking → ↑ modulus (stiffer)
↑ durability/stability
↓ O₂ transmission
How does increasing water content affect Dk and modulus in hydrogels vs silicone hydrogels?
Hydrogels (Groups 1–4):
↑ water → ↑ Dk
↑ water → ↓ modulus (less stiff)
Silicone hydrogels (Group 5):
↑ water → ↓ Dk
↑ water → ↓ modulus
Why does increasing water increase Dk in hydrogels but decrease Dk in silicone hydrogels?
Hydrogels: O₂ travels through water → more water = more O₂
SiHy: O₂ travels through silicone → adding water dilutes silicone → ↓ Dk
What is the consistent effect of increasing water content on modulus across all soft lenses?
↑ water → ↓ modulus → less stiff
Applies to both hydrogels and silicone hydrogels
Summarize the tradeoffs of increasing water content in soft contact lenses.
Hydrogels: ↑ Dk but ↑ dehydration + deposits + ↓ stiffness
SiHy: ↓ Dk and ↓ stiffness
Overall: softer lenses but potential oxygen + handling tradeoffs
How important is index of refraction in contact lenses and what are typical values?
Less important than in spectacles
Materials are very similar (~1.40–1.49)
Examples:
PMMA ≈ 1.49
PureVision ≈ 1.426
Biofinity ≈ 1.40
Acuvue Oasys ≈ 1.42
What are silicone elastomers and their key properties?
Own class (not GP or standard soft lens)
High MW cross-linked silicone polymer
Very high Dk (~340)
Used in pediatric aphakia (e.g., Silsoft)
What are the key advantages and disadvantages of silicone elastomers?
Advantages:
Extremely high oxygen permeability (Dk ~340)
Disadvantages:
Very hydrophobic → poor wettability
Lipophilic → deposits
Requires surface treatment (plasma/coating)
What are the main types of tints used in soft contact lenses and their purposes?
Handling tint: improves visibility of lens (no effect on vision)
Enhancing tint: boosts natural eye color (subtle change)
Opaque tint: fully changes eye color
Prosthetic (masking) tint: covers defects, therapeutic/cosmetic
Compare handling, enhancing, and opaque tints in function and effect.
Handling: faint color → visibility only
Enhancing: translucent → intensifies natural iris color
Opaque: solid pigment → completely changes iris color
What are prosthetic (masking) contact lens tints and their clinical uses?
Used to mask ocular abnormalities or for cosmetic rehab:
Iris defects: albinism, trauma, congenital issues
Corneal opacities
Color vision deficiency
Blind eye cosmesis
Occlusion/patching for diplopia
How do prosthetic tinted lenses improve patient outcomes?
Cosmetic masking of disfigured eye
Restore symmetry/appearance
Can provide functional benefit (light control, diplopia suppression)