MedPath- Renal Lab 1
1/49
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
50 Terms
What is occurring in the glomerulus during nephritic syndrome?
-inflammation--> inflammatory response with cytokine release
-glomerular basement membrane disruption which enables red blood cells and proteins to leak out
-antibodies and antigens form immune complexes
-neutrophils
How does nephritic syndrome present clinically?
-hematuria--> blood in urine
-proteinuria
-hypertension
mixed nephritic-nephrotic syndrome clinical presentation
-hematuria
-nephrotic-range proteinuria
What is occurring in the glomerulus during nephrotic syndrome?
-podocyte damage, fusion, and loss
-loss of negative charge of GBM
-edema
-leakage of large molecules/ serum proteins
How does nephrotic syndrome present clinically?
-heavy proteinuria
-hypoalbuminemia--> edema
-hyperlipidemia--? lipiduria (fatty casts)
What are the mechanisms of glomerular injury?
-most immunologic in origin
-immune complex deposition--> deposition of circulating antigen-antibody complexes in glomerular capillary walls
-in situ immune complex formation--> antigen and antibody bind to each other directly in glomeruli
How are immunoglobulin deposition or complement seen in glomeruli?
-immunofluorescence or EM
What is the concern with immune complexes in glomeruli?
-may activate complement system
Why are antigen-antibody complexes formed in circulation prone to depositing in glomeruli?
-high vascular pressure that drives filtration of plasma to form urine
-negative charge and permeability characteristics of basement membrane (promotes stable attachment of antibodies)
What are the 3 major functions of the complement system?
-inflammation
-opsonization (coating put on microbe to them more easily recognized and ingested by macrophages) and phagocytosis
-cell lysis
What do all pathways of the complement system lead to?
-formation of an active C3 convertase
What are the different locations immune complex deposition can occur in glomeruli?
-subendothelial deposits--> between epndothelial cells and basement membrane
-subepithelial deposits--> between basement membrane and podocytes
-membranous deposits--> within membrane
-mesangial deposits--> between mesangial cells and extracellular matrix
What is the most common cause of nephrotic syndrome in children?
-minimal change disease
What is the morphology of minimal change disease?
-no notable pathologies by light microcope--> no inflammation and no deposits of antibodies or immune complexes visible in glomerulus
-EM: diffuse effacement of podocyte foot processes
pathogenesis of minimal change disease
leakiness of basement membrane to albumin (low molecular weight proteins, selective loss)
treatment of minimal change disease
-corticosterioid therapy
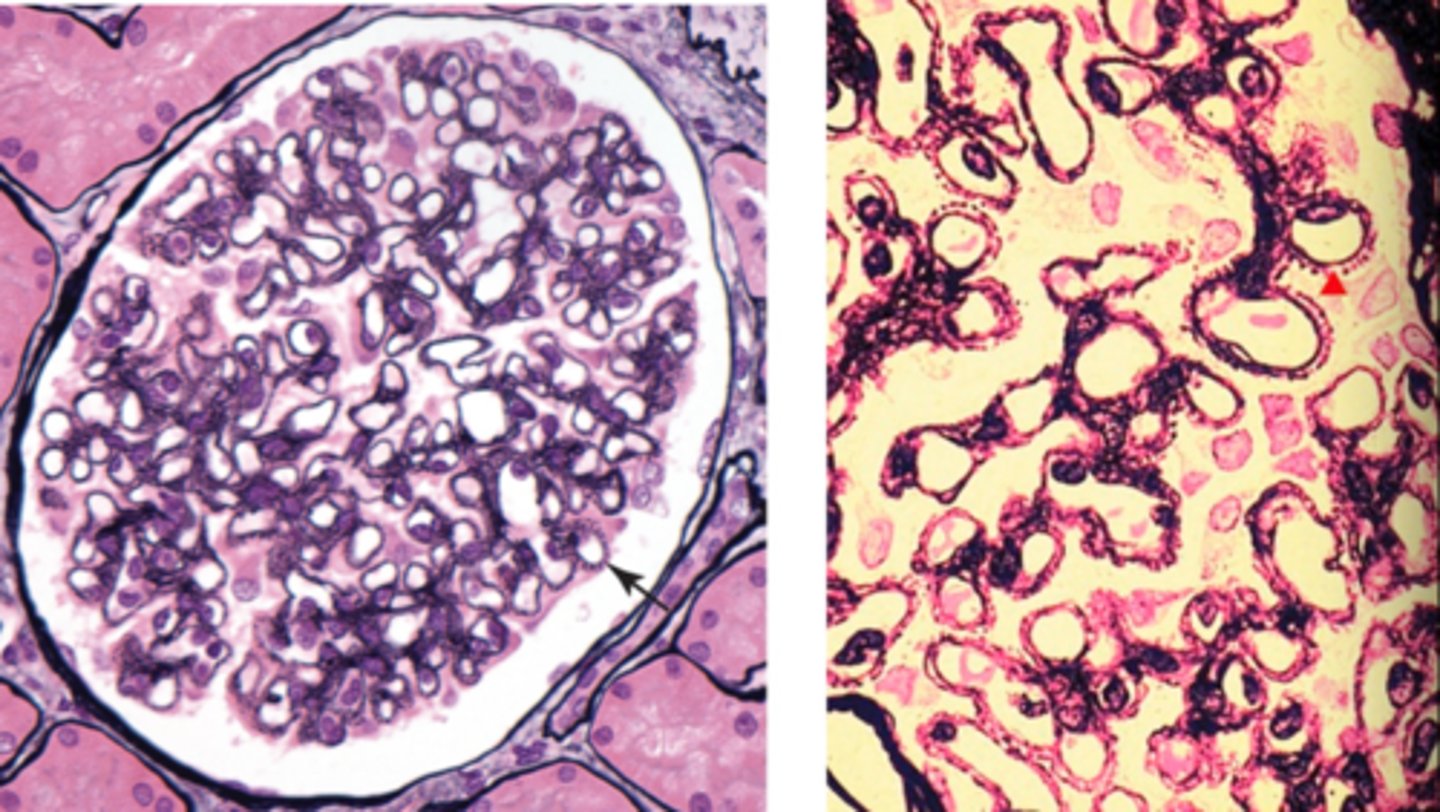
What is silver stain used for in nephorlogy?
-visualize the basement membrane--> better visualization of renal architecture and glomeruli
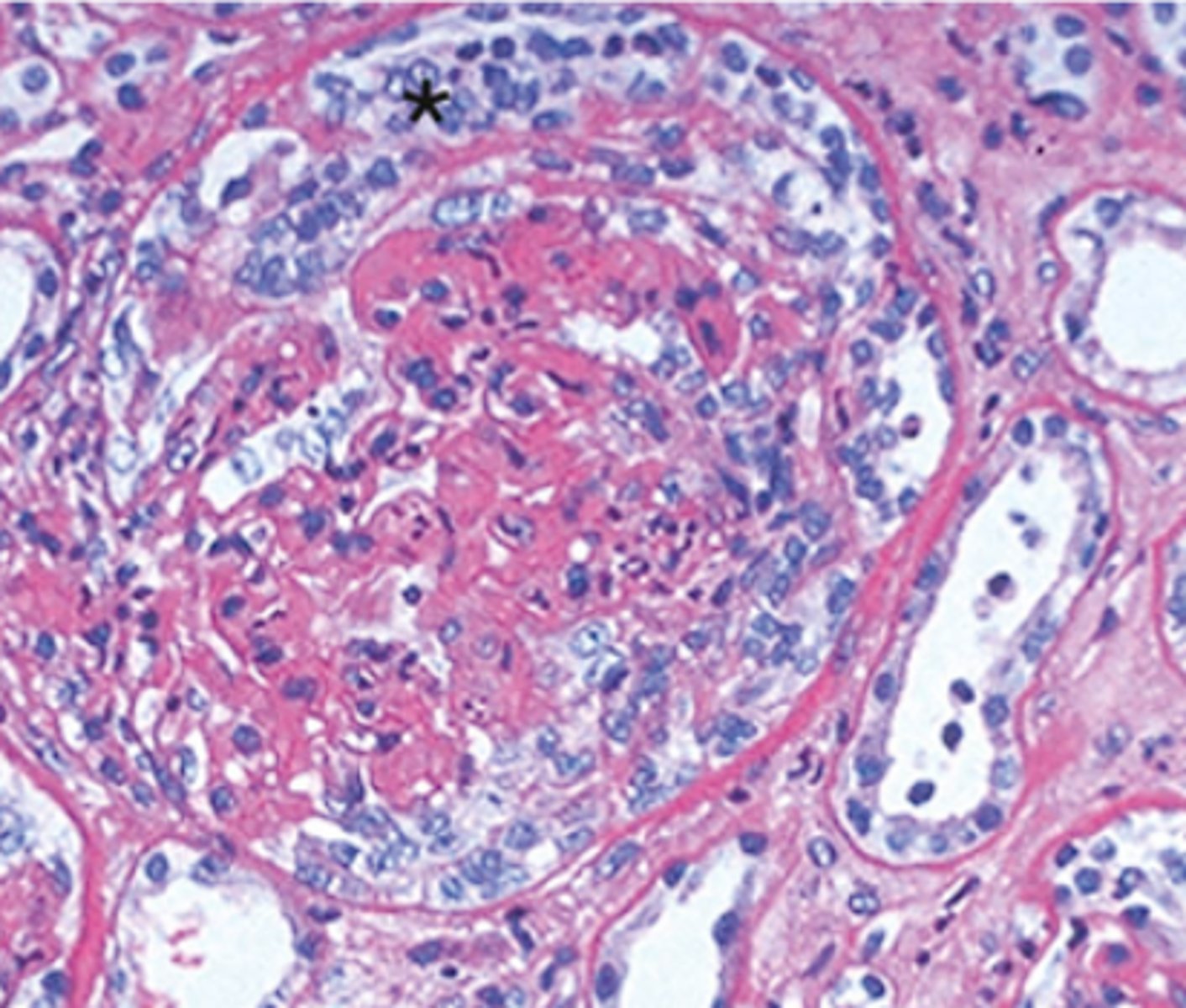
In membranous nephropathy, what does the silver stain show?
-thickening of capillary walls but without increase in cellularity
-thickening basement membrane will have the appearance of spikes b/c basement membrane is stretching around deposits
pathogenesis of membranous nephropathy
-immune complexes are formed in situ by autoantibodies binding endogenous podocyte antigens (phospholipase A2 receptor) or planted antigens (autoimmune)
Is membranous nephropathy primary or secondary a majority of the time? What types of things is it secondarily associated with?
-primary (majority)
-secondary--> infections or tumors
-can also be seen in lupus
morphology of membranous nephropathy
-diffuse thickening of basement membrane (immune complex deposits), formation of "spikes" of the basement membrane material around deposits
-podocyte foot processes diffusely effaced
-no inflammation or increase cellularity
clinical features of membranous nephropathy
-usually present in adults
-nephrotic syndrome with non-selective proteinuria (includes large proteins leaking into urine)
treatment of membranous nephropathy
-does not respond well to corticosteriods (other immunosuppressive drugs are used
focal vs diffuse
segmental vs global
-focal: present in some but not all glomeruli
-diffuse: in all glomeruli
-segmental: in each affected glomerulus, but only a portion of the glomerulus is affected
-global: the full glomerulus is affected
Pathogenesis of focal segmental glomerulosclerosis (FSGS). Is it considered primary or secondary a majority of the time? What secondary things is it associated with?
-initiating event is injury to podocytes through unclear mechanism (circulating factors may damage podocytes)
-primary (majority)
-secondary--> HIV infection (can cause severe glomerular insure), heroin use, other glomerular diseases, inherited defects in cytoskeletal or podocyte proteins
morphology of focal segmental glomerulosclerosis
-increased mesangial matrix protein obliterates capillaries + deposition of matrix material (hyaline) throughout the abnormal segment
-immunofluorescence: nonspecific trapping of antibodies but no immune complexes
-EM: diffuse foot processes effacement
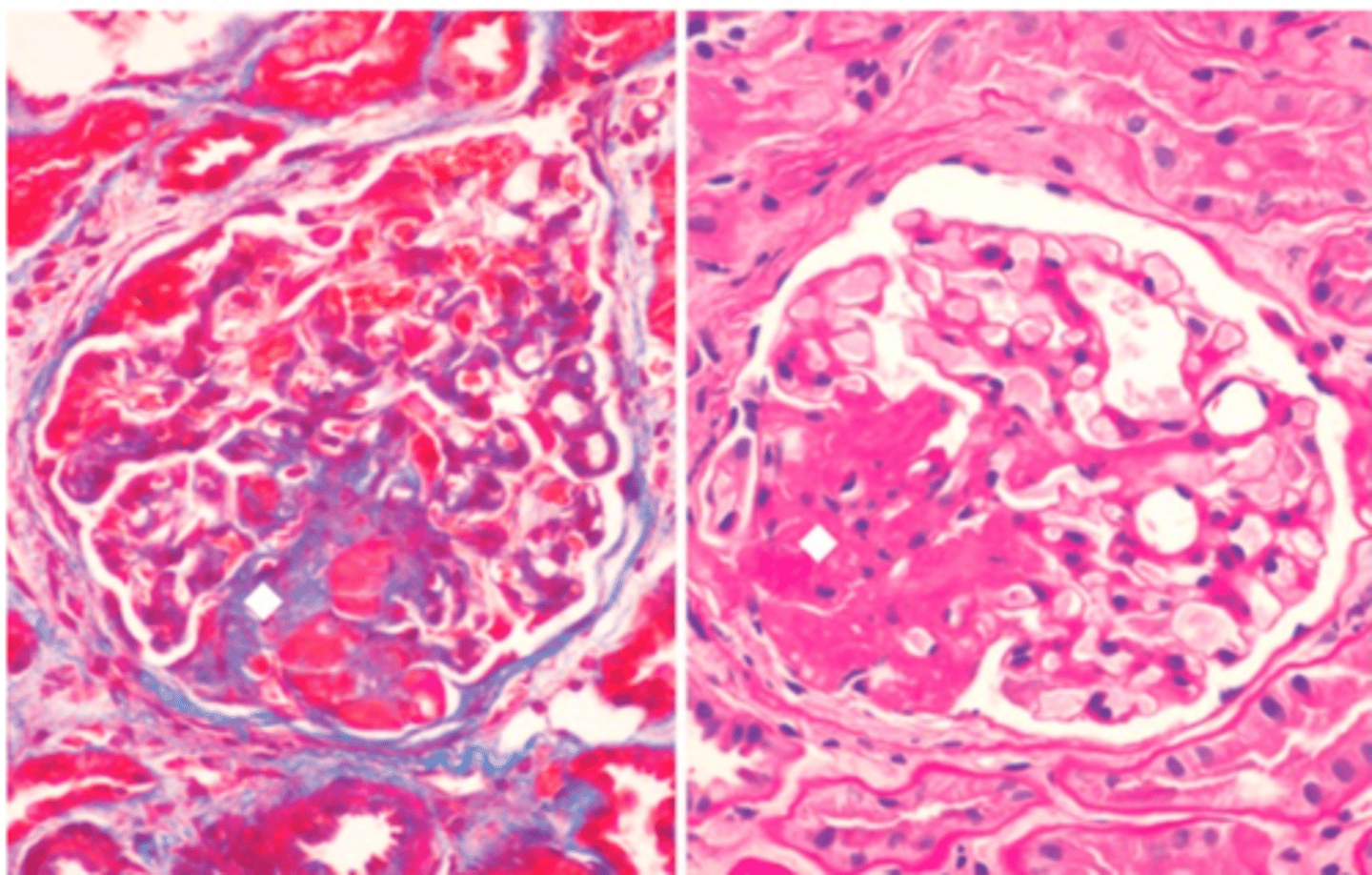
clinical presentation of focal segmental glomerulosclerosis and treatment
-nephrotic syndrome; can see microscoptic hematuria
-treatment: response to immunosupprissive drugs is poor; half of patients develop end stage renal disease
What occurs in membranoproliferative glomerulonephritis?
alterations in glomerular basement membrane and proliferation of glomerular cells
morphology of membranoproliferative glomerulonephritis
-subendothelial electron dense deposits
-duplication of basement membrane
-accentuated lobular architecture
-mesangial cell proliferation (increased cellularity)
-increased mesangial matrix
-BM thickening with splitting/ duplication (double contour, "tram tracking")
-influx of WBCs
pathogenesis of membranoproliferative glomerulonephritis
-immune complex deposition; unknown citing antigen
-less commonly a secondary disease (lupus, viral hepatitis, chronic infection); immune complex may be composed of antibodies bound to nucleoproteins or microbial antigens
What does immunofluorescence of membranoproliferative glomerulonephritis show?
-granular deposits of antibodies and complement proteins
clinical presentation of membranoproliferative glomerulonephritis
-nephrotic syndrome, some patients get nephritic syndrome; poor prognosis
What kind of disease is Goodpasture Syndrome and what does it affect?
autoimmune disease affecting the lung and kidney
What kind of kidney disease is Goodpasture Syndrome categorized as?
-rapidly progressive glomerulonephritis
pathogenesis of Goodpasture Syndrome
-pathogenic autoantibodies to non-collagenous domain of the a3 chain of type IV collagen
Why does Goodpasture syndrome affect both pulmonary alveoli and renal glomeruli?
both have basement membranes containing type IV collagen which is targeted
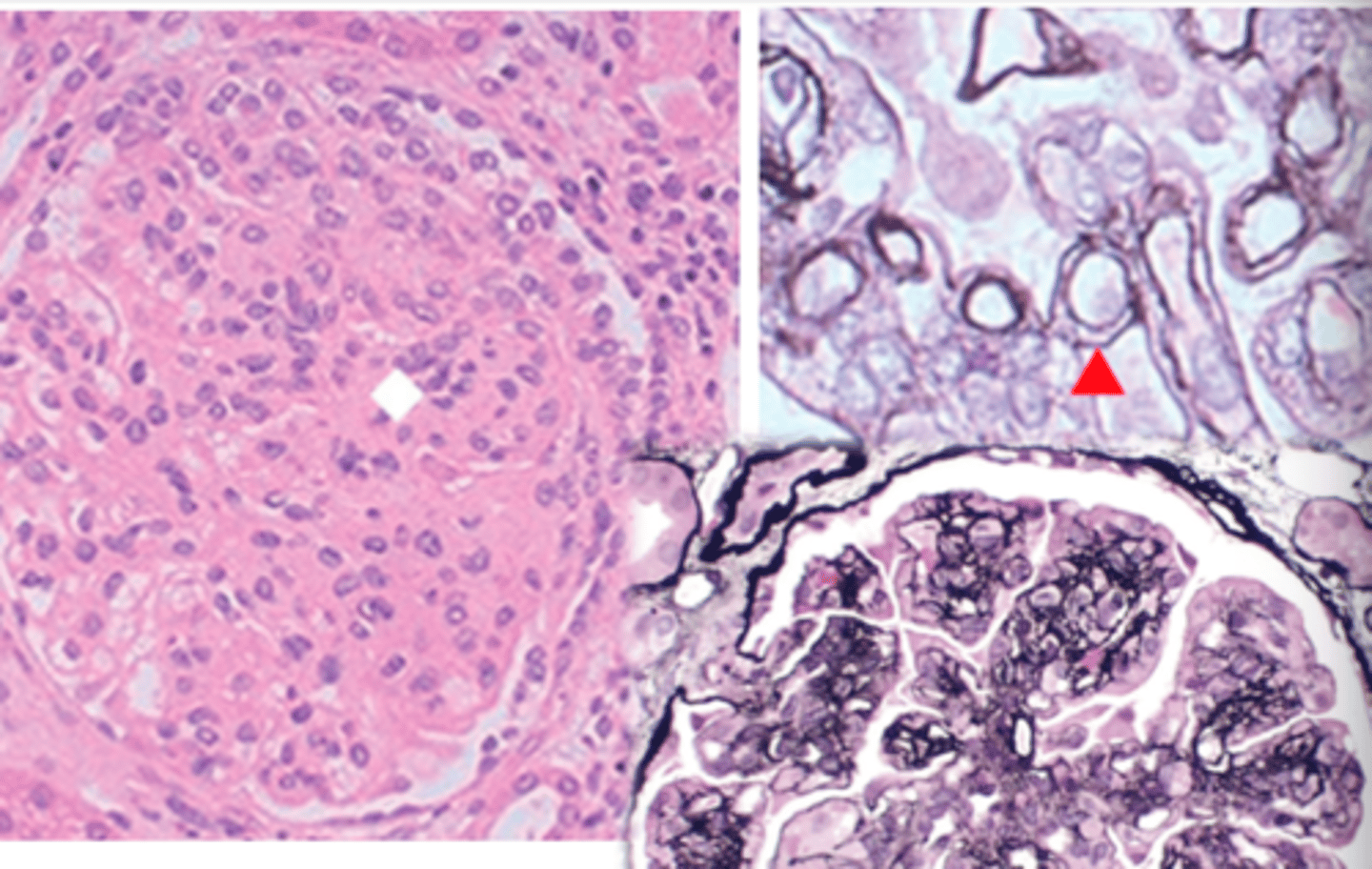
morphology of Goodpasture syndrome
-crescentic glomerulonephritis
-crescents composed of visceral epithelial cells (podocytes) cause by severe glomerular damage--> fibronogen to leak into bowman's space--> proliferation of podocytes
-diffuse linear IgG complex in glomeruli
-hemorrhagic lung
What does that autoantibody attack of the type IV collagen do to the lungs and kidney
causes necrotizing hemorrhagic interstitial pneumonitis and glomerulonephritis
How is Goodpasture Syndrome diagnosed?
immunofluorescent study of immunoglobulin deposition (usually IgG) in renal or pulmonary specimen
Who is usually diagnosed with Goodpasture syndrome?
-people in their teens or 20's, mostly smokers
What type of hypersensitivity reaction does Goodpasture syndrome represent? What does that mean?
-type II hypersensitivity
-IgG mediated cytotoxic hypersensitivity
-cells are destroyed by bound antibody, either by activation of complement or by cytotoxic T cell with Fc receptor for the antibody
What are the common characteristics of rapidly progressive glomerulonephritis?
-anti-GBM autoantibodies
-known immune complex disease manifestation (acute postinfectious GN or lupus)
-Pauci-immune crescentic GN: characteristic clinical lesion in the absence of detectable antibodies or immune compleses
What else is rapidly progressive glomerulonephritis called?
crescentic GN
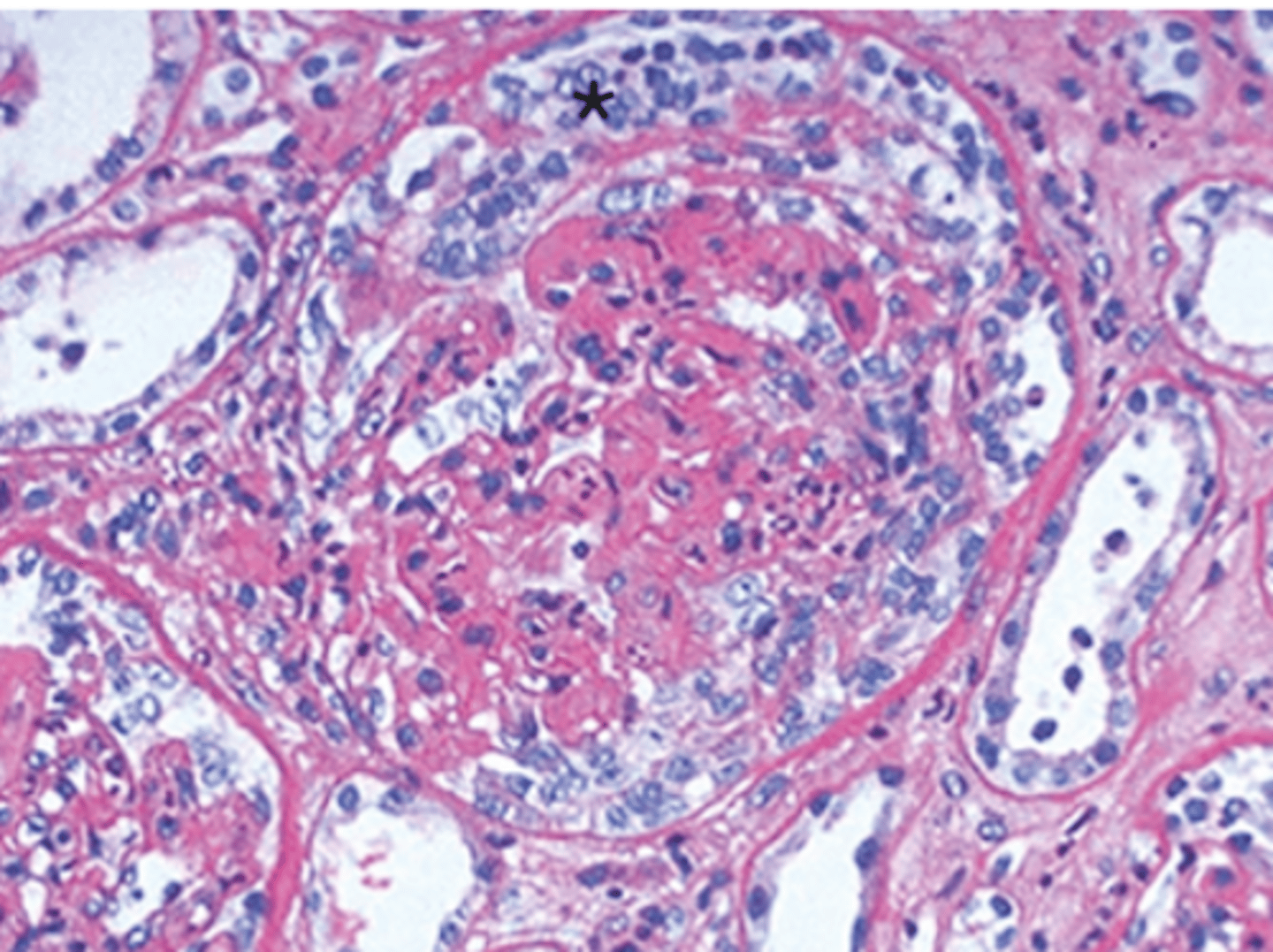
morphology of rapidly progressive glomerulonephritis
-main feature is the formation of crescents
-severe glomerular injury: segmental capillary necrosis, breaks in the basement membrane (visible on EM)
-deposition of fibrin in Bowman's space
How does rrapidly progressive glomerulonephritis appear on IF and EM?
-IF: linear or granular IG and C3 along the GBM (except in in pauci-immune type)
-EM: ruptures in the GM with or without immune deposits
pathogenesis of IgA nephropathy
-respiratory infection induces increased mucosal IgA production (which becomes abnormally glycosylated)
-abnormal IgA appears as foreign protein elicits antibody response--> complexes are deposited in the kidney, activate complement, causing glomerular injury
morphology of IgA nephropathy
normal or subtle inflammatory changes in glomeruli (mild increase in mesangial cellularity) with IgA deposits
What stain is used to highlight mesangial cellularity seen in IgA nephropathy?
PAS highlights the expansion of the mesangium
Clinical scenario of IgA nephropathy
-hematnuria following upper respiratory infection, resolves spontaneously but can recur
How is IgA nephropathy diagnosed?
IF with deposition of IgA in mesangium