Unit 4 Exam
1/31
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
32 Terms
Joslin/Allen (early 1900’s)
Diabetes (usually type 10 was fatal
glycosuria
hyrerphagia
extreme thirst
weight loss
ketoacidosis
their hypothesis: body cannot handle incoming nutrients, so we should reduce metabolic burden
caloric restriction
approach: intake vs. urine output
findings:
+intake → glycosuria, +ketonuria
fasting → -glycosuria, -ketonuria
→”starvation diet”
not a cure, nut did extend patient’s lives a few months
T1D is insulin deficiency
cells don’t uptake glucose
liver → gluconeogenesis and glycogenolysis
lipolysis → ketones
Banting/Best/MacLeod/Collip 1922:
pancreatic extracts (dogs, rabbits, etc) → T1D
first major endocrine discovery
1920’s-1930’s
no drugs
T2D poorly understood
caloric restriction the norm
early recommendations:
structured diets (caloric counting)
energy balance
known that weight loss improves glycemia
1930’s-1950’s
no drugs
amphetamine derivatives
central appetite suppressors
effective
side effectives:
addiction
CV problems
Psychiatric effects
Mason/Ito 1967
Roux-en-Y:
create a small stomach pouch
reroute small intestine
first patient 1966: lost 30% of her weight in 9 months
1970’s-1990’s
backlash against drugs/surgery
focus on behavior, exercise, diet
findings:
modest weight loss
high long-term regain
weight loss is possible, maintenance is not
Metabolic Syndrome
T2D rates rising
clinical studies identify cluster:
hyperinsulinemia
hypertension
dyslipidemia
findings:
IR central to T2D
introduction of metabolic syndrome
BMI problems not about willpower
metabolic dysfunction
Anti-Diabetics 1970’s-1990’s
modern diabetes drugs
sulfonylureas (increased insulin secretion)
stimulates b-cells (Ca2+)
metformin (increased insulin sensitivity)
reduces hepatic glucose output
increase hepatic insulin sensitivity
no effect on BMI
treating glucose not the same as treating obesity
Fen-Phen
1990’s: “Lost Decade”
Fen-Phen (fenfluramine + phentermine)
+serotonin (+satiety), + norepinephrine (+appetite suppression)
significant weight loss
widely prescribed (millions)
Fen-Phen Problems
Fen-Phen side affects:
heart valves
pulmonary hypertension
off-target effects: 5-HT receptors → valve thickening
lawsuits, public/regulatory backlash
drugs withdrawn
retrospectively:
it worked
correctly targeted brain regions
but not dafe: receptor specificity matters!
GLP1 Research
Two directions of GLP1 research occurring in the background:
inhibit DPP4, prolong endogenous GLP1
find deregulation-resistant GLP1 receptor agonists
1992: eventide discovered
approved by FDA in 2005
Pories 1995:
Context? Approach: long-term follow-up of gastric bypass patients
findings; high rates of diabetes remission
interpretation:
surgery has metabolic effects?
cut-endocrine regulation?
Safer T2D drugs
UKPDS 34 1998:
sulfonylureas work against T2D, but cause weight gain
insulin works but also causes weight gain
high BMI cohort;
randomized to:
conventional therapy
metformin
sulfonylureas, insulin
Metformin Wins
Findings:
all drugs lowered HbA1c
only metformin did not cause weight gain
reduction in:
diabetes-related endpoints
all-cause mortality
myocardial infarction
Knowler 2002:
contact:
T2D rising
risk factors known
hypothesis: progression to T2D can be prevented:
lifestyle?
metformin?
approach:
3200 pre diabetic adults
high fasting glucose
poor glucose tolerance
= high risk for T2D
randomized into 3 groups:
lifestyle: diet/exercise/weight loss (150min/wk)
metformin: 850mg twice daily
control: placebo and standard advice
findings:
reduction in diabetes:
lifestyle: 58%
metformin: 31%
lifestyle 2X as effective at preventing diabetes
interpretation:
diabetes is preventable
lifestyle is a first-line therapy
pre diabetes is a clinical target
criticism:
lifestyle group was highly monitored and coached: not feasible broadly
2012; Stampeded trial
150 patients with T2D
range of BMIs
randomized to:
medical therapy
+gastric bypass
+sleeve gastrectomy
primary endpoint: HbA1C <6%
findings:
primary endpoint
therapy alone: -12%
gastric bypass: -42%
sleeve gastrectomy: -37%
weight
therapy: -5%
surgery: -25%
Early 2000’s
Roux-en-Y dramatically increases GLP1 production
+PYY
-ghrelin
faster nutrient delivery to distal intestine
+insulin
=+satiety
Exenatide (2005):
peptide from Gila monster
DPP-4-resistant
GLP1-RA
AMIGO trial
Reduced HbA1c, modest weight loss
Liraglutide (2010)
Manipulations of structure to make it longer-acting
→GLP1 + fatty acid
-CV events
HbA1c
-weight
GLP1-RAs with modest effects:
lixisenatide
albiglutide (dimer fused to albumin)
dulaglutide (fused to IgG Fc)
Semaglutide (2017):
injectable and oral formulations
highly potent,long-acting
GLP1 + fatty acid
many trials, all good
15% weight loss
strong CV benefit
-HBA1c
Tirzepatide (2022)
dual GIP + GLP1 agonist (“twincretin”)
20% weight loss, HbA1c -2.3%
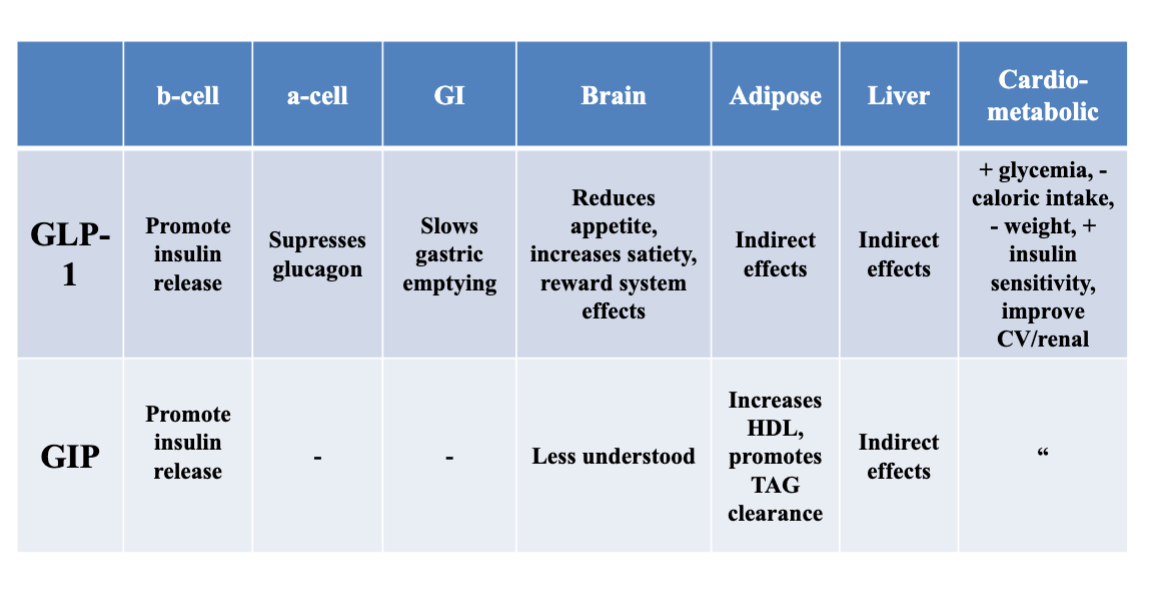
GLP Summary
GLP-1 and children
AAP 2023 guideline: offer weight-loss drugs to 12yo and older with obesity
GLP-1 and side effects
Common:
GI: nausea, vomitting, diarrhea, constipation, abdominal pain
pancreatitis, gallbladder disease, hypoglycemia, dehydration
thyroid tumors in mice
AHA 2024/2026
treat the BMI and glucose, it fixes everything else
no longer thought of as a willpower problem
BMI+T2D
GLP1-RA
SGLT2 inhibitor (renal glucose excretion)
T2D prevention:
lifestyle: 150 min/week physical activity
Diet/CVD:
behavioral counseling
mediterranean-style, low carb
The Problem
short-term success common
long-term maintenance hard, rare
Mann 2007 review:
diets produced modest weight loss (~5%)
Regained 3-5 years
Look AHEAD trial (2012)
can diet +exercise reduce CV events?
5k adults w/T2D → either:
ILI (intensive lifestyle intervention)
did lose more weight, had better HbA1c, BP, HDL, TAG
But did not significantly reduce CV events
early success, hard to maintain
Crtl: support/education, not intensive
Liebel 1995:
energy expenditure reduced after wight loss, hunger increases (promote return to original weight)
gain? energy expenditure does not increase enough to return to original weight (settling point)
Proietto 2011
50 participants, 8wk diet, 1 yr follow-up
weight regain
+ ghrelin
- PYY
-CCK
Food Industry
Whole/minimally-processed → ultra-processed (UPF)
shelf-stable products
hyper-palatability
food system works to maximize:
yield
predictable production
profit
U.S. Farm Bill:
subsidies, crop insurance, commodity pricing, SNAP
Big Four:
corn, soybeans, wheat, rice
subsidized → cheap for manufactures → profitable → UPF
UPF
industrial formulations
~69% of calories in U.S. diet
additives:
override satiety
drive repeat consumption
Fractionation + recombination
+ absorption (proximal intestine)
Matrix effect:
UPF refined, essentially pre-digested, rapid glucose absorption