Hypernatremia
1/60
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
61 Terms
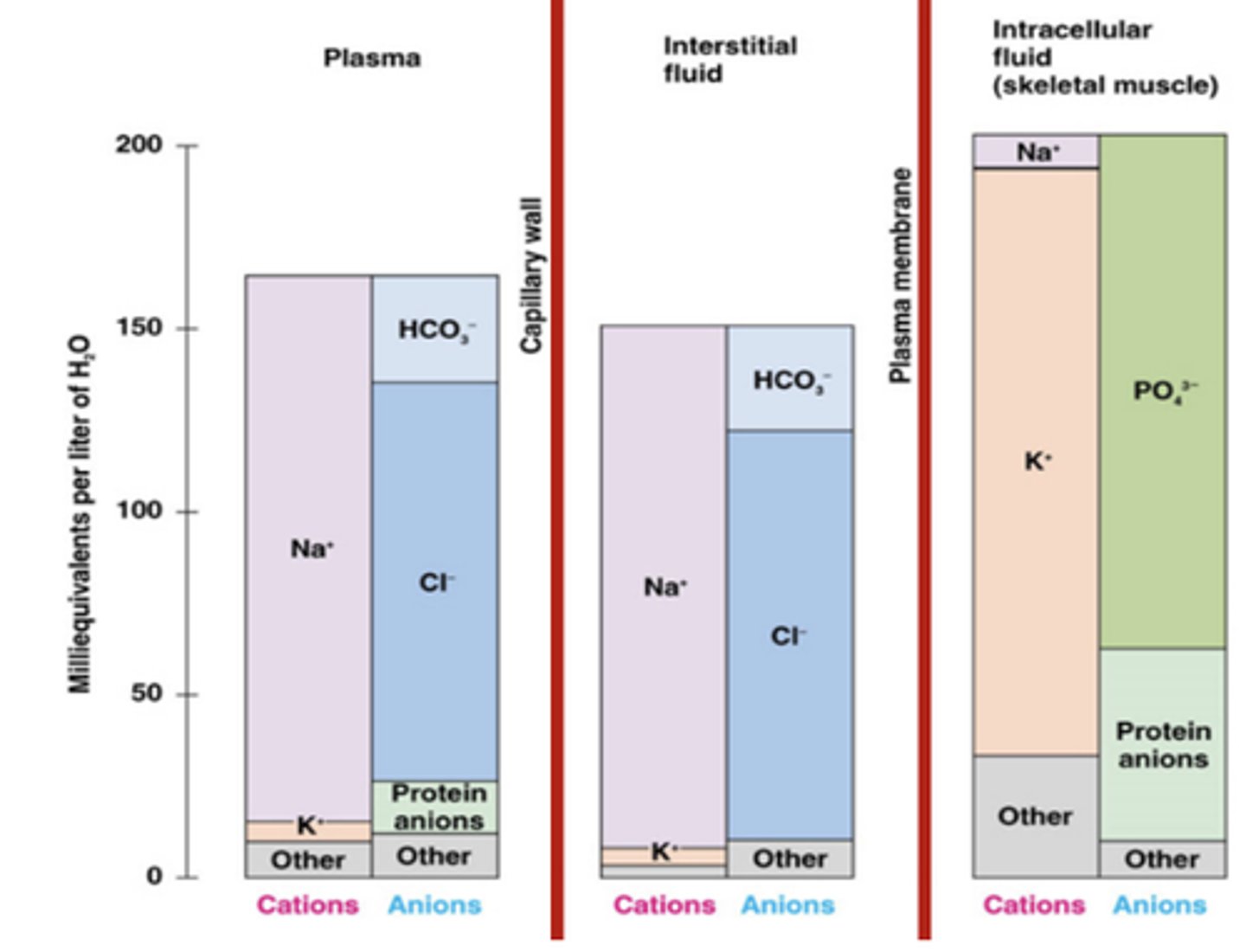
Solute Distribution
Extracellular vs Intracellular
Na is the primary extracellular solute
K is the primary intracellular
distribution is maintained by NaK ATPase
Normal Serum Sodium
135-145 mEq/L
Why is serum sodium so important?
sodium is the major determinant of plasma osmolarity
What controls the serum sodium concentration?
Serum sodium concentrations are controlled by water balance (not necessarily indicative of the total body sodium)
Sodium Intake
~150 mEq/day
Sodium Loss
Renal and Extrarenal
Renal
~150 mEq day
Extrarenal
Stool ~10 mEq/day
Insensible ~10 mEq/day
1 g of NaCl is how many mEq?
17 mEq Na+
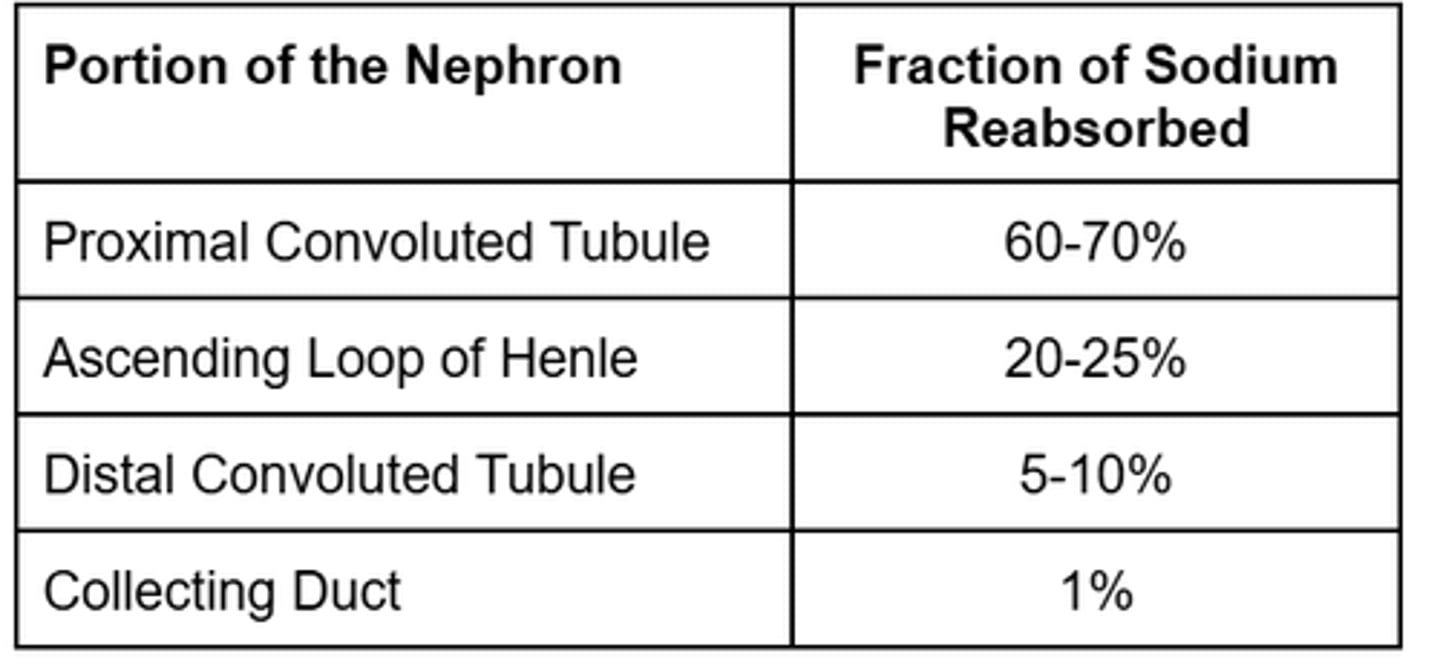
Sodium Reabsorption in the Nephron
PCT, Loop, DCT, Collecting Duct
Hypernatremia Serum Sodium
>145 mEq/dL
Hypernatremia is always a ________osmolar state.
HYPERosmolar
sodium is the primary determinant of serum osmolarity....
What total body water imbalance causes HYPERnatremia?
total body water DEFICIT
Moderate Hypernatremia
Serum Sodium, Symptoms
150-160 mEq/L
Muscle weakness
Restlessness
N/V
Severe Hypernatremia
Serum sodium, symptoms
>160 mEq/L
Confusion
Irritability
Lethargy
Stupor
Coma
3 Etiologies/Categories of Hypernatremia
Hypovolemic Hypernatremia
Euvolemic Hypernatremia
Hypervolemic Hypernatremia
Hypervolemic Hypernatremia
TBW, TBNa
TBNa ↑, TBW ↑↑↑
Sodium gain > water gain
Hypervolemic Hypernatremia Causes
Iatrogenic (most common)
hyperaldosteronism
cushing's syndrome
Iatrogenic Causes
Sodium overload (3% NaCl)
Excessive sodium ingestion
Antibiotic containing Na
Hypertonic dialysis
Hypervolemic Hypernatremia Treatment
1. D/c offending agent.
2. Diuretics to eliminate excessive sodium and water. (hemodialysis if renal failure)
--> Furosemide, 20 to 40 mg given orally or intravenously every 6 hours
3. Replace free water deficit.
Euvolemic Hypernatremia
TBW, TBNa
TBNa no change, TBW ↓
slight water loss
Euvolemic Hypernatremia
Renal Causes
Diabetes Insipidus
Signs and Symptoms of Diabetes Insipidus
polyuria, polydipsia, urine specific gravity < 1.005 (ref 1.010)
Why are DI patients typically euvolemic?
Patients with untreated AVP disorder excrete large volumes (320 L/day) of dilute urine, resulting in hypernatremia.
Renal water loss is compensated for by intense thirst (mild overall TBW loss).
Types of Diabetes Insipidus
Central DI: decreased AVP secretion leads to water loss.
Nephrogenic DI: resistance to AVP.
Central DI Causes
Caused by TBI, pituitary surgery, stroke.
Nephrogenic DI Causes
Caused by kidney disease.
Caused by medications: Lithium, Foscarnet, Clozapine
Euvolemic Hypernatremia
Non-Renal Causes
fever
hyperventilation
Euvolemic Hypernatremia Treatment
1. Replace free water deficit (PO if possible, IV if not)
2. If applicable, treat diabetes insipidus.
Central Diabetes Insipidus
Pharmacologic Treatment Options
Aqueous Vasopressin
Desmopressin
Aqueous Vasopressin
Place in Therapy
Only used for initial treatment due to short duration of action.
Aqueous Vasopressin
Route of Admin
IM or SC
Aqueous Vasopressin
SEs
Fluid overload with excessive dosing
Smooth muscle contractions
- Abdominal pain
- HTN
- Angina
- Uterine contractions
Aqueous vasopressin should be avoided in patients with hypersensitivity to what?
bovine or porcine agents
Desmopressin
Place in Therapy
Has increased potency, longer duration, and less smooth muscle effects
preferred agent
Desmopressin
Routes of Administration
nasal spray
rhinal tube
IV
oral
Desmopressin
Converting between dosage forms
10 mcg nasal spray = 1 mcg IV/SC = 0.05-0.1 mg tablet
Desmopressin
SEs
HA
HTN
Angina
Abd pain
conjunctivitis (nasal spray only)
oral tablet typically well -tolerated
Nephrogenic Diabetes Insipidus
Pharmacologic Treatment Options
hydrochlorothiazide, amiloride, indomethacin
HCTZ MOA
Has a paradoxical effect that results in enhanced proximal tubular Na/H2O reabsorption.
must be combined w sodium restriction
HCTZ Dosing
25 mg QD or BID
HCTZ SEs
Hypokalemia
Hypomagnesmia
Hypercalcema
Gout
Amiloride MOA
Inhibits Lithium reabsorption (Li inhibits ADV effect).
Amiloride Dosing
5-10 mg QD
Amiloride SEs
Mild hyperkalemia
HA
Weakness
Indomethacin MOA
Blocks prostaglandin (prostaglandins antagonize AVP effect)
Indomethacin
Dosing, Place in Therapy
Used as adjunctive therapy
100-150 mg/day (2-3 divided doses)
Indomethacin SEs
GI ulcer
AKI
Hypovolemic Hypernatremia
TBW, TBNa
TBNa ↓, TBW ↓↓↓
Water loss > sodium loss
Hypovolemic Hypernatremia
Renal Causes
Osmotic diuresis
Diuretic use
Acute/chronic kidney disease
Hypovolemic Hypernatremia
Non-Renal Causes
Diarrhea
Vomiting
Fistulas
Excessive sweating
Burns
Hypovolemic Hyponatremia
Treatment
1. If in hypovolemic shock, ALWAYS RESUCITATE FIRST.
250-1000 mL NS over 30-60minutes
2. Then replace free water deficit (see below)
Dehydration vs. Hypovolemia vs. Shock
Dehydration refers to a loss of TBW producing hypertonicity
Hypovolemia (volume depletion) is a symptomatic ECF volume deficit.
Shock hypotension + tachycardia.
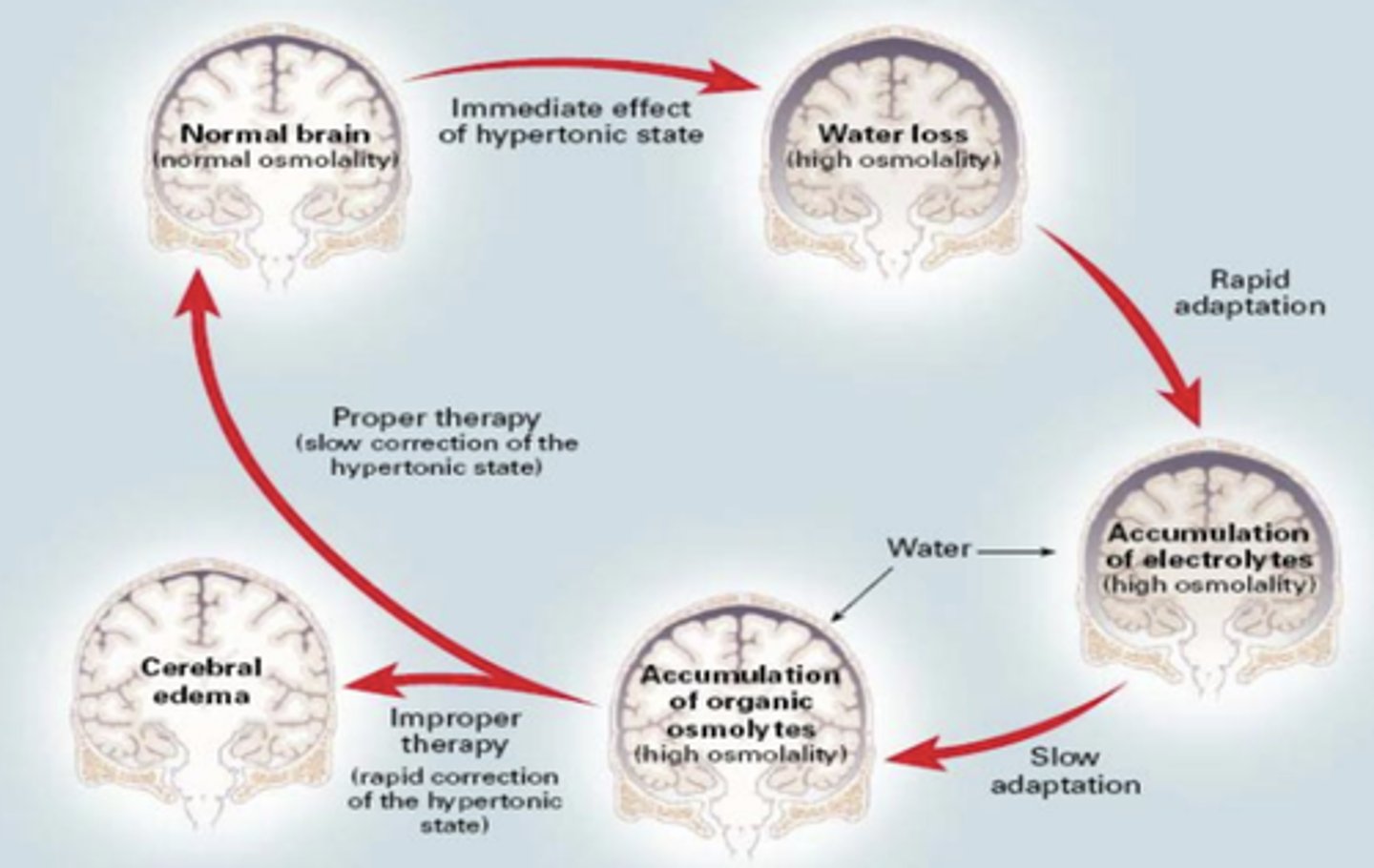
Why must sodium level correction rate be monitored?
rapid correction can cause cerebral edema
Brain Compensation in Hypernatremia
plasma hyperosmolarity --> brain generates organic solutes to prevent water loss --> rapid correction of plasma osmolarity --> brain swelling
Maximum Correction Rate
Acute Hypernatremia
< 48 hours
1 mEq/L/hr
Maximum Correction Rate
Chronic Hypernatremia
> 48 hours
0.5 mEq/L/hr
Maximal Daily Sodium Correction
10 mEq/L
What is the goal serum sodium?
To prevent overcorrection, goal serum sodium is 145-150 mEq/L.
Equation to Calculate an IV Fluid's Correction Rate

What fluids are used to correct hypernatremia?
D5W, 0 mEq/L
0.45% NaCl, 77 mEq/L
Free Water Deficit Equation
TBW Deficit = Normal TBW - Current TBW
Normal TBW = BW*(%water)
Current TBW = (140/serum sodium)*Normal TBW
How do you replace the free water deficit?
Replace ½ of the deficit in the first 24 hours THEN replace the remainder in the next 24-72 hours.
Always report fluid replacement calculations in L/hour!