Vulvar Disease and STIs
1/152
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
153 Terms
What is the 'Youth Disparity' in STI statistics?
People aged 15-24 represent ~25% of the sexually active population but account for 45.5% of all new infections.
What is the most common preventable cause of infertility?
Sexually Transmitted Infections (STIs).
What is the '60-Day Rule' in STI management?
All sex partners from the previous 60 days should be evaluated and treated.
What is the Expedited Partner Therapy management?
Providers are allowed to provide treatment for the patient's partner, without the partner having to be tested.
Why is retesting recommended 3 months after STI treatment?
Due to high re-infection rates
Which STIs are legally required to be reported to the health department?
Gonorrhea, Chlamydia, Syphilis, HIV, Acute Hepatitis B and C, and chancroid.
What is the USPSTF recommendation regarding HBV screening?
Screen all pregnant patients.
What is the recommended screening frequency for HIV for adults aged 15-65?
Universal one-time screening.
What are the preferred cervical cancer screening options for women aged 30-65?
Primary HPV testing every 5 years, cytology alone every 3 years, or co-testing (Pap + HPV) every 5 years.
What is the recommended screening for Chlamydia and Gonorrhea in sexually active women ≤24 years?
Universal annual screening.
What is the recommended screening for Chlamydia and Gonorrhea in sexually active women <25 years?
Screen only if at increased risk.
At what age should cervical cancer screening be discontinued?
Age 65, provided previous screening has been adequate and negative.
What is the gold standard for diagnosing Gonorrhea and Chlamydia in women?
NAAT (Nucleic Acid Amplification Test) via vaginal/cervical swab or first-catch urine.
What is the first-line treatment for Gonorrhea?
Ceftriaxone 500mg IM single dose (1g if ≥150 kg).
What is the first-line treatment for Chlamydia?
Doxycycline 100 mg BID for 7 days.
What is the classic triad of symptoms seen in disseminated gonococcal infection (DGI)?
Tenosynovitis, dermatitis (pustular lesions), and polyarthralgia.
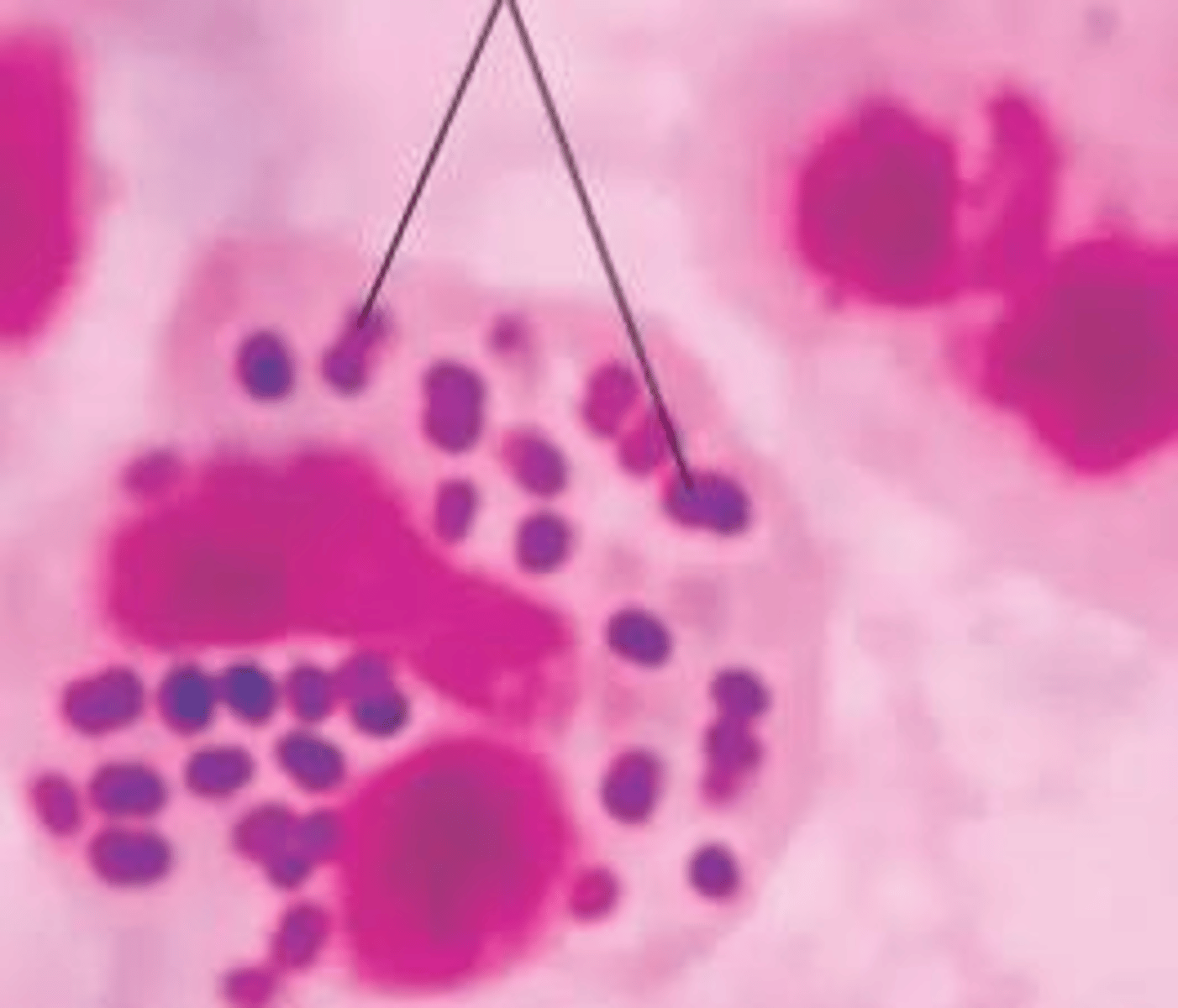
What is the etiology of Gonorrhea?
Neisseria gonorrhoeae, a gram-negative diplococcus.
What is the etiology of Chlamydia?
Chlamydia trachomatis, most common bacterial STI.
What percentage of women are asymptomatic with a Gonorrhea infection?
Up to 50%.
What percentage of women are asymptomatic with a Chlamydia infection?
70-80%.
What is the recommended management for a patient's partner after a Gonorrhea diagnosis?
Partner treatment is required, and the patient should abstain from sexual activity for 7 days after treatment.
What are the potential sequelae of Salpingitis?
Tubo-ovarian abscess, ectopic pregnancy, and infertility.
What is the recommended screening for Trichomoniasis in asymptomatic, low-risk women?
No routine screening is recommended.
What are the common complications associated with untreated Chlamydia infections?
PID, infertility, ectopic pregnancies, increased risk of other STIs, reactive arthritis, LGV, and neonatal complications like pneumonia and conjunctivitis.
Which Chlamydia serotypes cause Lymphogranuloma Venereum (LGV)?
Serotypes L1, L2, and L3.
What is the classic presentation of the primary stage of LGV?
Small, painless genital ulcer or papule at site of inoculation.
What is the classic presentation of the secondary stage of LGV?
The 'bubo stage,' characterized by painful, fluctuant inguinal lymphadenopathy occurring 2-6 weeks after the primary ulcer.
What is the recommended treatment for Lymphogranuloma Venereum?
Prolonged doxycycline (21 days), with or without incision and drainage (I&D).
What is the most common non-viral STI worldwide?
Trichomonas vaginalis.
What physical exam finding is pathognomonic for Trichomonas vaginalis?
A 'strawberry cervix' (petechial hemorrhages on the vaginal mucosa or cervix) and frothy, yellowish-green malodorous discharge.
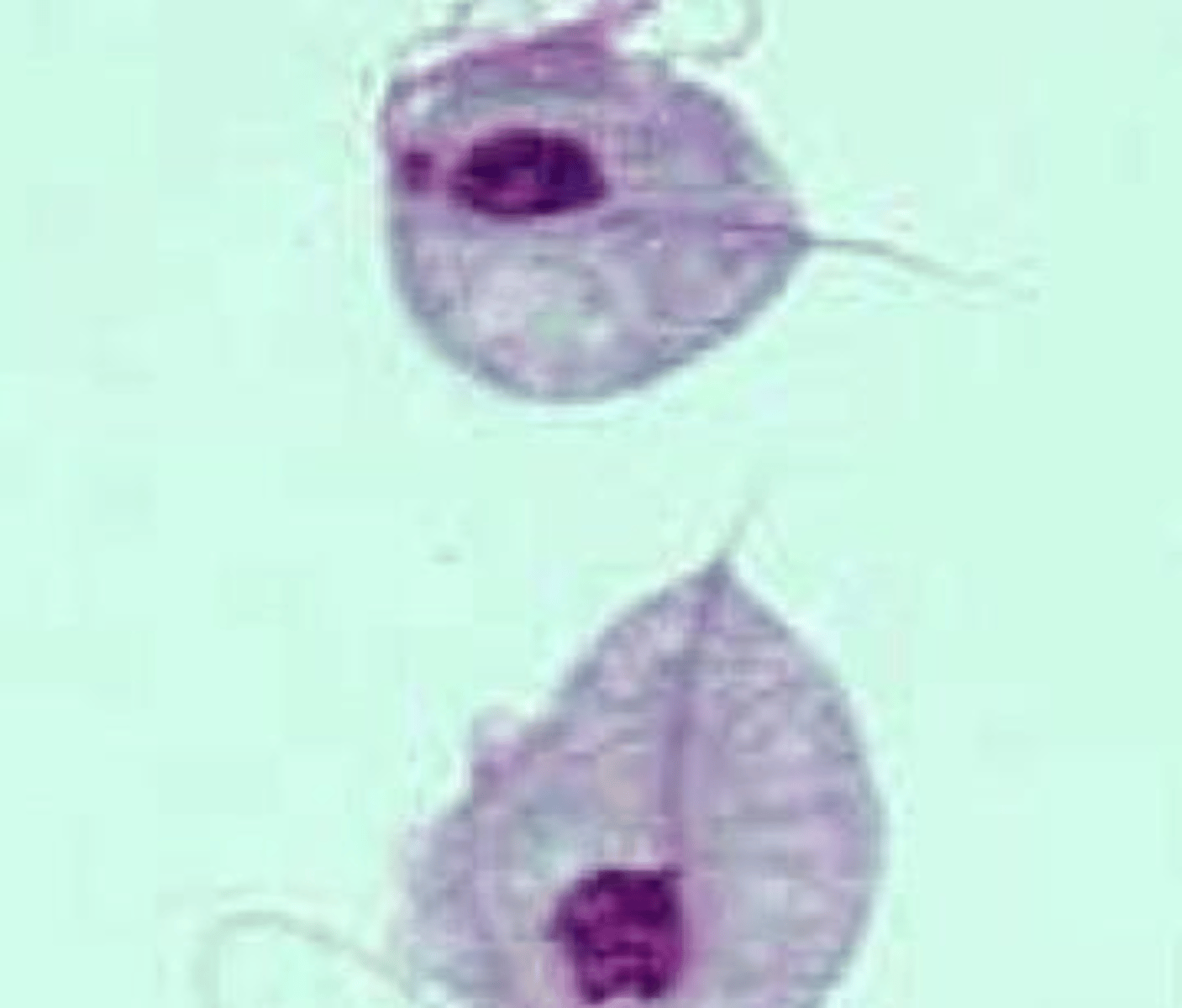
What are the diagnostic criteria for Trichomonas vaginalis via wet mount?
Presence of rapidly moving flagellated organisms described as 'pear with a tail'.
What is the preferred treatment for Trichomonas vaginalis?
Metronidazole 500mg BID for 7 days (for both pregnant and non-pregnant patients).
What is the two-stage treatment regimen for Mycoplasma genitalium?
Doxycycline 100mg BID for 7 days, followed by moxifloxacin 400mg once daily for 7 days.
What are the four clinical stages of syphilis?
Primary, secondary, latent (early/late), and tertiary.
What is the hallmark clinical feature of primary syphilis?
A painless chancre at the site of inoculation, appearing approximately 21 days after exposure.
What are the characteristic symptoms of secondary syphilis?
A diffuse, non-pruritic maculopapular rash involving the palms and soles, often accompanied by systemic symptoms like fever, malaise, and lymphadenopathy.
How is 'early latent' syphilis defined?
Infection acquired within the previous year; it is still potentially infectious.
When can neurosyphilis occur?
At any stage, not just in tertiary syphilis
What are the three main manifestations of tertiary syphilis?
Gummatous lesions, cardiovascular syphilis, and late neurosyphilis.
What are the clinical signs of Tabes dorsalis in late neurosyphilis?
Sensory ataxia, lancinating pains, bladder dysfunction, and Argyll Robertson pupils.
What is the screening vs. confirmatory testing protocol for syphilis?
Screening is done via non-treponemal tests (RPR or VDRL); confirmation is done via treponemal tests (FTA-ABS or TP-PA).
What is the treatment for primary and secondary syphilis?
Penicillin G Benzathine 2.4 million units IM in a single dose.
What is the treatment for neurosyphilis?
IV Aqueous penicillin G (3-4 million units every 3-4 hours) for 10-14 days, or Penicillin G procaine IM daily plus probenecid for 10-14 days.
What bacteria causes Chancroid?
Haemophilus ducreyi.
How are the ulcers of Chancroid clinically described?
Painful genital ulcers with 'shaggy and undermined borders' and painful, unilateral inguinal lymphadenopathy.
What is the primary mode of transmission for Genital Herpes?
Direct skin-to-skin contact, most commonly via asymptomatic shedding.
What are the characteristic physical exam findings of Genital Herpes?
Painful, grouped, fluid-filled vesicles on an erythematous base that eventually rupture into tender, shallow ulcers.
What is the preferred diagnostic test for Genital Herpes?
PCR of the lesion.
What is the purpose of suppressive therapy in Genital Herpes management?
Daily medication to reduce the frequency of outbreaks and decrease the risk of transmission to partners by approximately 50%.
What counseling must be provided to patients with Genital Herpes?
Antivirals reduce symptoms but do not cure the virus, and transmission can occur even when no lesions are visible.
What is the benefit of suppressive acyclovir treatment late in pregnancy for patients with recurrent genital herpes?
It reduces the frequency of cesarean delivery.
What type of virus is HPV and which tissue layer does it primarily infect?
It is a DNA virus that infects the basal layer of the stratified squamous epithelium.
What is the most common STD?
HPV
Which HPV types are most commonly associated with genital warts?
Types 6 and 11.
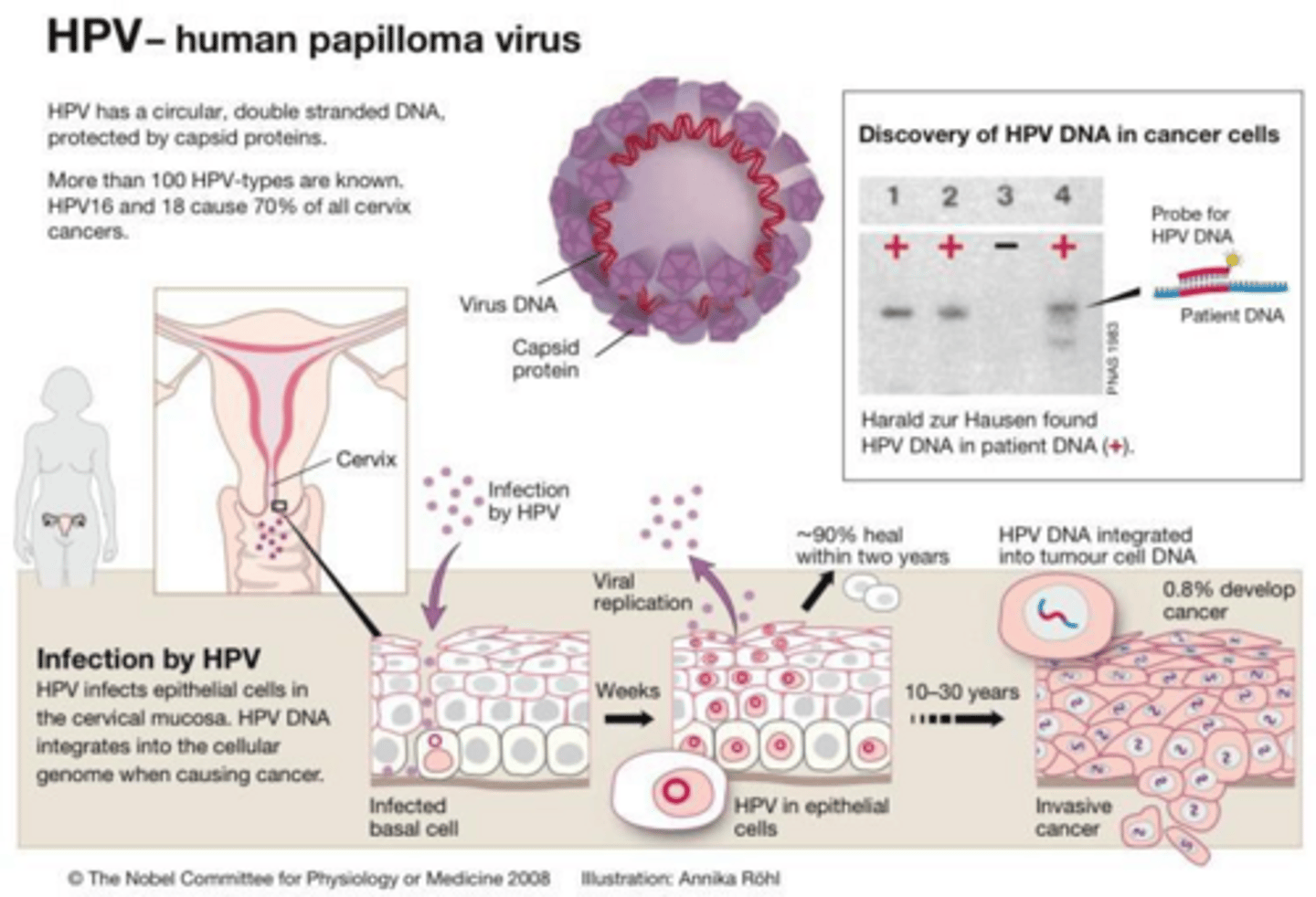
What are the 'high-risk' HPV types primarily associated with cervical cancer?
Types 16, 18, 31, 33, 45, and others.
What is the clinical appearance of condyloma acuminata?
Soft, skin-colored, fleshy, cauliflower-like lesions on the vulva, perineum, or perianal area.
How is the diagnosis of genital warts typically made?
Clinical diagnosis based on visual inspection; biopsy is only indicated if the diagnosis is uncertain.
What is the 'Gold Standard' for HPV prevention?
The Gardasil-9 vaccine.
What is the vaccination schedule for Gardasil-9 based on age?
2 doses if started before age 15; 3 doses if started between ages 15-45.
What is the primary target of the HIV retrovirus?
CD4+ T-lymphocytes.
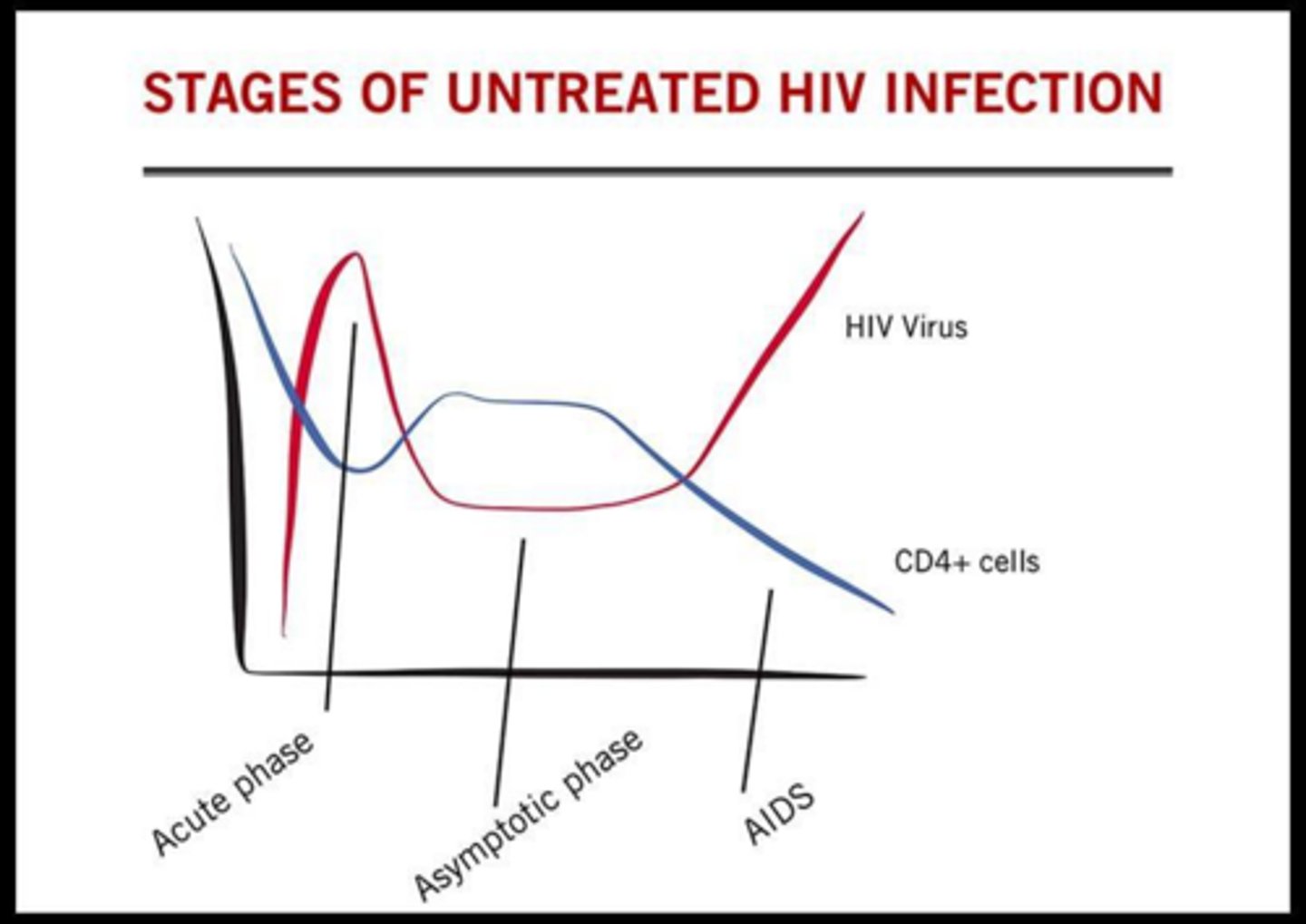
What are the clinical criteria for an AIDS diagnosis?
A CD4 count < 200 or the development of an AIDS-defining condition or illness.
What is 'Acute Retroviral Syndrome' and when does it occur?
A flu-like viral syndrome occurring 2-6 weeks after HIV exposure; patients are highly infectious during this phase due to high viral load.
What is the screening test for HIV?
4th generation combination HIV-1/2 Antigen/Antibody Immunoassay.
What is the clinical goal of antiretroviral therapy (ART) in HIV management?
To reach undetectable status (viral load <200 copies/mL), which means the virus is untransmittable.
What is the 'Golden Window' for starting Post-exposure prophylaxis (PEP) after HIV exposure?
Within 72 hours of exposure.
What is the recommended follow-up for a patient on PrEP?
Every 3 months for HIV testing, STI screening, and pregnancy testing; every 6 months for renal function.
What are the eligibility requirements for starting PrEP?
Documented HIV-negative status within one week, no signs of acute HIV infection, and normal renal function.
How is liver damage caused in Hepatitis B infection?
The virus is not directly cytopathic; damage is caused by the host's immune response attacking infected hepatocytes.
What are the common clinical findings associated with Hepatitis B?
Jaundice, icteric sclera, clay-colored stools, darkened urine, and nausea/vomiting.
What does a positive HBsAg test indicate?
The virus is present; if positive for >6 months, the infection is chronic.
What does the presence of Anti-HBs indicate?
Immunity; the patient is 'protected'.
What does the presence of IgM Anti-HBc indicate?
Acute infection (detectable for 6 months).
What does the presence of HBeAg signify regarding Hepatitis B?
High infectivity; the virus is actively replicating.
What is the management of HBV?
Prevention with Universal Vaccination (3 dose series at 0, 1 and 6 months)
What is the recommended Post-Exposure Prophylaxis (PEP) for an unvaccinated person exposed to HBV?
HBV vaccine + HBIG (Hepatitis B Immune Globulin).
Define Pelvic Inflammatory Disease (PID).
An ascending infection that moves from the vagina/cervix to the upper genital tract, including the Fallopian tubes, uterus, and/or ovaries.
What are the primary pathogens responsible for PID?
Neisseria gonorrhoeae and Chlamydia trachomatis.
What is the clinical triad used to identify Pelvic Inflammatory Disease (PID)?
Lower abdominal tenderness, adnexal tenderness, and Cervical Motion Tenderness (CMT) or 'Chandelier Sign'.
What is the minimum diagnostic criteria for a clinical diagnosis of PID?
Pelvic or lower abdominal pain plus either cervical motion tenderness or adnexal/uterine tenderness.
What is the standard outpatient treatment regimen for PID?
Ceftriaxone 500 mg IM (single dose) + Doxycycline 100 mg BID x 14 days + Metronidazole 500 mg BID x 14 days.
List three criteria that would necessitate inpatient treatment for PID.
Pregnancy, failure of outpatient medications, inability to tolerate oral medications, severe illness (nausea/vomiting), or suspected Tubo-Ovarian Abscess (TOA).
What is the consequence of failing to see improvement in PID symptoms 48-72 hours after treatment if an IUD is present?
The IUD must be removed.
What is a Tubo-Ovarian Abscess (TOA)?
An inflammatory mass involving the fallopian tube, ovary, and occasionally adjacent pelvic organs.
How do you treat TOA?
Requires hospitalization and IV antibiotics.
How does the risk of tubal factor infertility change with repeated episodes of PID?
The risk increases with each episode: 8% after one, 18% after two, and 38% after three episodes.
What is Fitz-Hugh-Curtis Syndrome?
Perihepatitis characterized by 'violin-string' adhesions between the liver capsule and the anterior abdominal wall, often presenting with RUQ or referred shoulder pain.
What is the normal physiologic discharge?
1-3mL of fluid per 24 hours, which is white or transparent and mostly odorless.
What is the typical pH range of a healthy vaginal environment?
4.0 to 4.5.
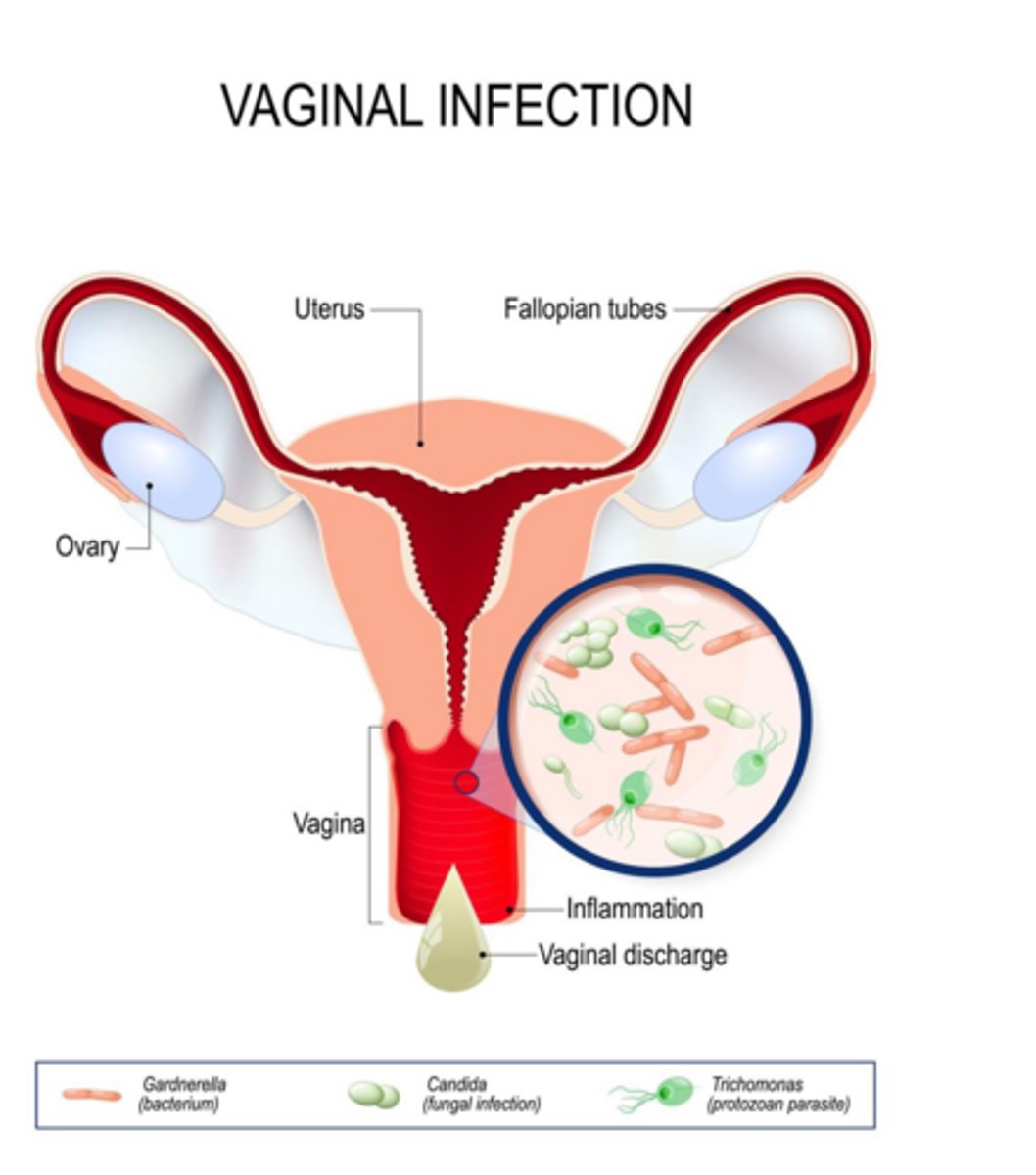
What is the most common cause of vaginitis?
Bacterial vaginosis
What is the purpose of the 'Whiff Test' in a wet mount preparation?
To detect an 'amine' or fishy odor when 10% KOH is added to vaginal discharge, which is positive in Bacterial Vaginosis and Trichomoniasis.
What are the four Amsel criteria used to diagnose Bacterial Vaginosis (BV)?
1. Vaginal pH > 4.5, 2. Homogeneous thin grayish-white discharge, 3. Positive whiff-amine test, 4. Presence of clue cells on microscopy.
What is the etiology of Bacterial Vaginosis?
A disturbance in normal vaginal microbiota characterized by a decrease in lactobacilli and an overgrowth of anaerobes like G. vaginalis, Prevotella, and Mobiluncus.
What is the clinical significance of 'clue cells' on a wet mount?
They are a diagnostic marker for Bacterial Vaginosis.
What is the purpose of using 10% KOH in a wet mount?
It facilitates the 'whiff test' and dissolves epithelial cells and bacteria to make yeast easier to visualize.
What are the common symptoms of vaginitis?
Itching, changes in discharge (amount, odor, color, consistency), vaginal soreness, swelling, dyspareunia, burning, erythema, and pelvic pain.
What is the primary function of lactic acid produced by lactobacilli in the vagina?
It maintains an acidic pH, which prevents the growth of pathogenic microorganisms.
Name three factors that can affect the vaginal ecosystem.
Hormonal changes, sexual activity (semen), contraceptive use, personal hygiene (douching), antibiotic use, and lifestyle factors.
What is the difference between the saline slide and the KOH slide in a wet mount?
The saline slide is used to identify motile trichomonas and clue cells, while the KOH slide is used for the whiff test and to visualize yeast.
What are clue cells on a saline wet mount?
Epithelial cells with bacilli clinging to their surface, indicative of Bacterial Vaginosis.
What is the first-line treatment for Bacterial Vaginosis?
Metronidazole 500mg orally twice daily for 7 days OR Metronidazole 0.75% vaginal gel daily for 5 days.