Anatomy + Kinesiology Exam 3
1/173
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
174 Terms
Good Posture
The proper alignment in all positions must be considered for its effect on the body.
*supports function by avoiding excessive stress
Kinetic Chain
- When the body moves, each segment affects the next, creating a chain reaction
- This is because the force generated by one segment is transferred to the next, building on the previous motion
Postural deviation (skeletal malalignment)
Misalignment of body segments. This causes other joints in the kinetic chain to compensate
joint stability
Integrity of a joint when it is placed under a functional load
optimal length-tension relationship
ideal position is where muscle can generate the most tension with the least effort (think door and door hinge)
insufficent length-tension relationship
can lead to muscle imbalance and nerve pathology, pain, joint effusion, poor posture, and repetitive activity of one muscle group
Postural Muscles
- support body against gravity
- usually deep muscles
- become overactivated and tightened or shortened
- prone to trigger points
trigger points
Pathological condition characterized by a small, hypersensitive area located within a muscle
Phasic muscles
- Provide movement to extremities
- Superficial muscles
- High percentage of fast-twitch (Type II) fibers
- Become inhibited and weakened
- Prone to tears and inflammation
Spinal Curves
primary curves develop before birth (anterior curve), and secondary curves after birth
Kyphotic Curve
- Anteriorly concave curves
- Thoracic and sacral spines
Lordotic
- Anteriorly convex curves
- Cervical and lumbar spines
Compensatory Curves
A change in curve in one portion of spinal column may result in compensation in other portions.
Common Types of Compensatory Curves
- Sway back -> increased lumbar lordosis
- Flat back -> decreased lumbar curve
How is the Pelvis the key to spinal curvature?
The neutral pelvis is when the iliac crests are level and the Anterior Superior Iliac Spines (ASISs) are level
Abnormal pelvis rotation
- Neutral pelvis = normal lordotic curve
- Anterior (forward) tilted pelvis = sway back occurs
- Posterior tilted pelvis = flat back occurs
Ways Compensatory Curves Can Develop:
- Working at a computer: increased thoracic kyphosis and cervical lordosis
- Texting: Increased thoracic kyphosis
- Scoliosis: Lateral curve of vertebral column
Scoliosis
- Primary curve: first curve to develop
- Secondary curve: compensatory curve; opposite primary curve
*Curve may be:
a. Functional curve: not a permanent curve
b. Fixed curve: permanent curve
Methods for observing posture
Objective tools:
1. Radiographs
2. Photographs
3. Computer analysis
Clinical tools:
1. Goniometers
2. Flexible rulers
3. Inclinometers
4. Plumb lines
Plumb lines
A string with a weight on the end suspended from above representing a "true" vertical landmark
Common Postural Deviations: Hips
Coxa Vara: Hip deformity, the angle of the femur and shaft are < 120 degrees
Coxa Valga: Hip deformity, the angle of the femur and its shaft are increased > 135 degrees
Common Postural Deviations: Knee
Genu Recurvatum: knee joint bends backward (Hyper-extension)
Genu Valgum: knees bend inward (Knock-kneed)
Genu Varum: knees bend outward (Bow-legged)
Common Postural Deviations: Feet
Pes Planus: flat arch
Pes Cavus: high arch
Leg-Length Discrepancy
- Structural (true)
Actual different in bone length between limbs (Measure ASIS to medial malleolus)
- Functional (apparent)
Attributed to something other than bone length discrepancies (Measure navel to medial malleolus)
Swayback Posture
- Increased lumbar lordosis
- Anterior pelvic tilt
- Hip assuming a slightly flexed position
(Potential causes: tight or shortened hip flexors/back extensors, weak or elongated extensors/abdominals)
Flat Back Posture
Decreased lumbar lordosis and lower thoracic kyphosis
(Potential causes: Shortened or tightened hip extensors, abdominal musculature, weakened/elongated hip flexors, back extensors, Decreased general muscle strength, Poor postural position sense)
Kypholordotic Posture
- Anterior pelvic tilt
- Flexed hip joint
- Increased lumbar lordosis
- Increased thoracic kyphosis
(Tightened or shortened hip flexors or back extensors, weakened or elongated hip extensors or trunk flexors, poor postural position sense)
Forward Shoulder Posture
- Humeral head anterior to line bisecting the body in the frontal plane
- Internal GH rotation
(Potential Causes: Shortened or overdeveloped anterior shoulder girdle muscles, Weakened or elongated scapular stabilizing muscles, Abnormal cervical and thoracic spine alignments, Postural muscle fatigue, Large breast development, Repetitive occupational and sporting positions)
Forward Head Posture
- Flexed lower cervical spine
- Flattening or flexion of mid-cervical spine
- Extended upper cervical spine
(Potential Causes: Wearing of bifocals, poor eyesight and need for classes, Muscle fatigue and weakness, Compensatory mechanism for other postural deviations)
Scapular Winging
- Medial border projects posteriorly
(Potential Causes: Weakness of serratus anterior and middle and posterior trapezius muscles, Secondary trauma to the long thoracic nerve
Long thoracic nerve
innervates serratus anterior
Ambulation
Activity of moving from place to place regardless of method (crawling, wheelchair)
Walking
Upright bipedal ambulation
Gait
Clinical term used when referring to walking
Limb/Leg
Entire lower extremity
Gait Cycle
One complete sequence of movements of one leg during walking
Stride or Stride Length
Interval between the time one foot touches the ground and the same foot touches the ground again
Step Width
Side to side distance when walking
Step or Step Length
Interval between the time one foot touches the floor and the other foot touches the floor.
Cadence
- Number of steps per minute
(Adults average about 107 steps per minute)
Velocity
Distance per unit of time
(adults average 2.5-4 mph)
Stance Leg
Weight-bearing limb during gait cycle
Swing Leg
Non-weight-bearing limb during gait cycle
Foot Angle
Angle of foot relative to line of progression
(Imaginary line from heel to 2nd toe)
Ground Reaction Force (GRF)
- Contact of the foot with the ground creates force yielding:
a. Vertical
b. Anteroposterior (A/P)
c. Mediolateral (M/L) components
Center of Pressure (CoP)
Shows the path of the pressure point under the foot during gait
2 Phases of Gait Cycle
1. Weight-bearing (WB) stance phase (60% of cycle)
2. Non-weight-bearing (NWB) swing phase (40% of cycle)
Weight-bearing (WB) stance phase
Begins on initial contact with the surface and ends when contact is broken. Kinetic energy is absorbed from the ground and transferred up the kinetic chain allowing body to move forward
Consists of:
- Initial Contact
- Loading Response
- Midstance
- Terminal Stance
- Preswing
What part of the foot should the Weight-bearing (WB) stance phase occur on?
i. On the lateral aspect of the heel
ii. Then move forward toward the lateral edge of foot
iii. Finally, toward the undersurface of the great toe
Non-weight-bearing (NWB) swing phase
Begins at the instant the foot leaves the surface and ends just before initial contact. This is the low energy phase
Consists of:
- Initial Swing
- Midswing
- Terminal Swing
Normal gait should consist of
i. Efficient gait
- Minimal side-to-side motion and maximal forward motion
ii. Center of gravity (COG)
- Also called "Center of mass"
- Observed as horizontal and vertical movement of the pelvis
(Path should be a sinusoidal curve)
iii. Comfortable Walking Speed
- Average adult = 1.2 to 1.4 m/s (Roughly around 3 mph) This decreases with age due to decreased strength
6 Determinants of Gait:
1. Lateral Pelvic Shift: pelvis moves side to side to maintain COG
2. Lateral Pelvic Tilt: unsupported side of pelvis falls lower than supported side
3. Pelvic Rotation: one side moves forward at a time, they alternate
4. Knee Flexion: causes limb to shorten during mid swing so you don't trip
5. Interaction of Knee Flexion and Plantarflexion: Coordinated to maintain an appropriate vertical distance from floor to pelvis
Gait during Running
- As velocity increases and periods of stance decrease, right and left swing phases reach a point where they overlap
1. This results in periods when neither foot is in contact with the ground "Float Phase"
2. No period of double limb support
- COM is constrained even more due to horizontal and vertical displacement.
- Vertical GRF increase 2-6 x's body weight
Walking vs. Running COM
When walking:
- Reduced vertical and horizontal displacement of the body's COM occurs
When running:
- Vertical and horizontal displacement of the body's COM is constrained even more
2 types of Gait Analysis
1. Qualitative Assessment
2. Quantitative Assessment
How to Observe (Andy's Rules)
1. Observe entire body
- Overall impression of cadence, balance, characteristics
2. View from all four sides
3. Observe one joint of one LE through entire cycle
- Usually start at foot/ankle
4. Observe trunk, UE, and head also
5. Observe with and without shoes
6. Using a water on person's sole to observe parts of gait cycle
- Or inspect shoe tread ware
Normal Arch Type
Neutral foot alignment
Shoe type: Stability
High Arch Type
Supinator
Shoe type: Cushioned
Flatfoot Type
Pronator
Shoe type: Motion control
Common Gait Deviations: Elderly
- Slower cadence
- Wider BOS
- Barely clear floor during swing
- Increased time in double stance
Common Gait Deviations: Temporary or permanent
- Orthopedic
- Neurological
- Acute or chronic
- Pain
Common Gait Deviations: Glutes
1. Gluteus maximus gait:
- Weak gluteus maximus
- Presents as a quick trunk extension movement at the time of initial contact to create hip extension
2. Gluteus medius gait:
- Also called "Trendelenburg gait"
- Weak gluteus medius
- Increased pelvic tilt to involved side
Common Gait Deviations: Abductor Twist gait
- Weak hip external rotators and abductors
- The foot abruptly abducts
Common Gait Deviations: Muscle Weakness
1. Quadriceps weakness:
- Decreased ability to extend knee or maintain knee extension
- Use of hand on thigh pushing posteriorly to keep knee extended
2. Dorsiflexor weakness:
Causes:
1. Foot slap: sound made at initial contact as forefoot hits ground
2. Steppage gait: greater hip and knee flexion (hip hike) to clear foot during swing
Drop foot
Common nerve pathology that prevents dorsiflexion
Common Gait Deviations: Calcaneal gait
During the stance phase, increased dorsiflexion and knee flexion occur on the affected side, resulting in a decreased step length
Common Gait Deviations: Waddling gait
Commonly observed in individuals with diffuse weakness such as that caused by muscular dystrophies
Common Gait Deviations: Vaulting gait
Unequal leg lengths or unable to flex knee. To compensate, plantar flexion of stance leg so swing leg can clear ground
Common Gait Deviations: Circumduction gait
Unequal leg lengths, Knee unable to flex during swing, During swing LE is abducted and swings out and around
Range of Motion Limitations (Toe-In gait vs Toe-out gait)
Toe-In gait:
- Found in midstance or just after push-off
- Can be cause by: Increased tibial rotation and/or Increased hip rotation
- Puts stress on lateral soft tissues and peroneus longus muscle
Toe-out gait:
- Causes same as Toe-in
- Puts stress on medial and plantar soft tissues
Neurological Causes
Hemiplegia gait: loss of function of one side of the body due to brain injury
Ataxic gait: "Parkinson's gait" Lack of coordinated movement. Movements are jerky and uneven, affecting balance
Scissors gait: Caused by spasticity of hip adductor muscles
Pain Causes: Antalgic gait
a "limp", When gait deviations result from pain
Effect of pain on cycle varies depending on:
1. Cause
2. Location
3. Intensity of pain
Vertebral Column: 5 Regions
Cervical: 7 vertebrae
Thoracic: 12 vertebrae
Lumbar: 5 vertebrae
Sacral: 5 vertebrae
Coccyx: 3 fused vertebrae
(Think meal times)
Atlantooccipital (AO) joint
- C1 and occiput
- Main movement his head nodding ("yes")
Atlantoaxial (AA) joint
- C1-C2
- Main movement is rotation ("no")
Cervical Spine
- C2-C7
- Flexion, extension, rotation, side-bending
Thoracic Spine
- T1-T12
- Flexion, extension, rotation, side-bending
- Movement can be limited by rib cage
Lumbar Spine
- L1-L5
- Flexion, extension, slight side-bending
- No rotation
Vertebral Column: Motions
Movement at each intervertebral joint is small, but the sum of all joints produces significant movement
- Flexion
- Extension
- Rotation
- Lateral (side) bending
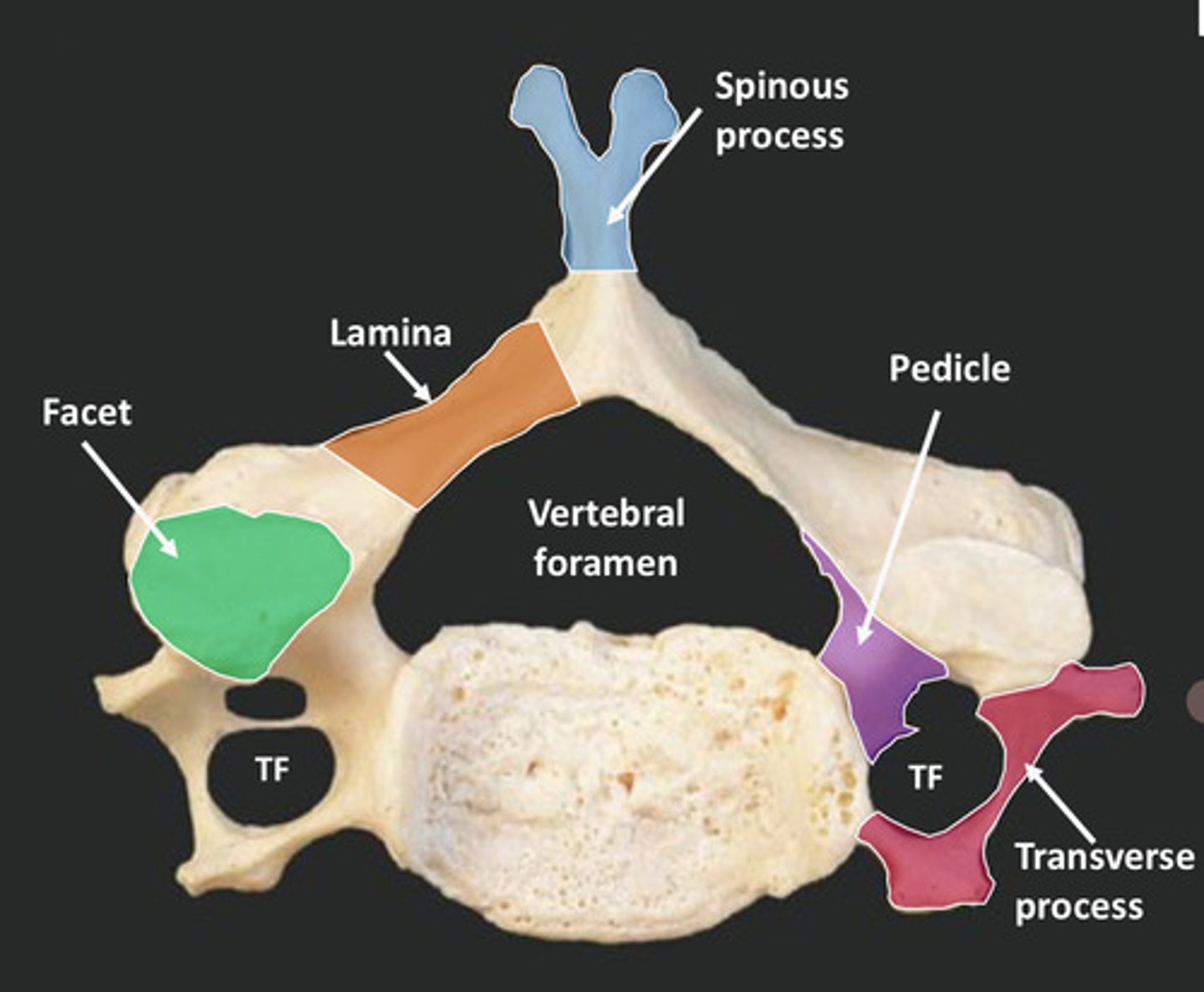
Vertebral Column: Bony Landmarks draw this one
know these
- Body
- Vertebral arch
- Vertebral foramen
- Pedicle
- Transverse process
- Spinous process
- Lamina
- Facet
- Intervertebral foramen
Intervertebral Discs
- 23 discs, beginning between C2 and C3
- Shock absorption during transmission of forces through spine
- Loss of water content contributes to loss of height with aging
Components of the Intervertebral Discs
Annulus Fibrosus:
- Outer portion
- Encircles and contains nucleus pulposus
Nucleus Pulposus:
- Gelatinous substance in the center
- High water content (70-80%)
Trunk (Soft Tissue Structures)
Linea Alba:
- Vertical fibrous band in anterior midline
- Extends from xiphoid process to pubic symphysis
Rectus Fascia:
- Sheet-like tendon
- Connects obliques and transverse abdominals muscles to Linea Alba
Sternocleidomastoid
- Bilaterally: head and neck flexion
- Unilaterally: lateral neck flexion to same side; rotation of head to opposite side
Scalenes
- Bilaterally: neck flexion
- Unilaterally: lateral neck flexion to same side
Splenius Capitis
- Bilaterally: head and neck extension
- Unilaterally: lateral flexion and rotation of head to same side
Splenius Cervicus
- Bilaterally: neck extension
- Unilaterally: lateral flexion to same side
External Intercostals
Elevate ribs during inspiration
Internal Intercostals
Depress ribs during expiration
Rectus Abdominis
Trunk flexion
External Oblique
- Bilaterally: trunk flexion
- Unilaterally: trunk lateral flexion and rotation to opposite side
Internal Oblique
- Bilaterally: trunk flexion
- Unilaterally: lateral trunk flexion and rotation to same side
Transverse Abdominis
Compression of abdomen
Accessory muscle of respiration
Erector Spinae Group
All perform either cervical and trunk extension
Thoracic Outlet Syndrome
- A disorder caused by compression of: Brachial plexus, Subclavian artery, Subclavian vein
- Results in various vascular, neurological, or muscular s/s
Compression caused by:
Tightness of Scalenes
Cervical rib & clavicle
Possibly an extra cervical rib
Pec minor and rib cage
Poor posture
Brachial Plexus Pathology
a "burner" or a "stinger"
- Caused by either traction or impingement of brachial plexus
- Pain on opposite side of lateral bending= tension
- Pain on side toward lateral bending = compression)
Erb's point
- 2-3 cm superior to the clavicle
- Represents most superficial passage of brachial plexus
- Pressure here can result in pain and paresthesia radiating into arm
Torticollis
- A condition where the neck muscle become tight
- Causes the head to tilt or turn to one side
- Can be:
1. Congenital -> present at birth
2. Acquired -> develops later in life
Rib Contusions
- Bruise to the ribs
- MOI - A blow to the ribs
Costochondral Separation
- Separation of the rib bone from costo cartilage
- MOI -Direct blow or a twisting + Compressive mechanism