pituitary disorders
1/47
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
48 Terms
what is acromegaly
•Condition of excessive production of growth hormone (GH)
•Most common cause is a pituitary adenoma (tumor)
Leads to soft tissue growth
what can acromegaly lead to
Can lead to multiple issues
Cardiovascular disease
Joint issues
Elevated glucose for some patients
acromegaly treatment
Most cases can be treated with surgery
In some cases, medications may be needed instead of or as adjuncts to surgery
acromegaly treatment goal
Treatment goal is to reduce GH and insulin-like growth factor (IGF-1)
IGF-1 is a key mediator of IGF-1
GH level goal below 1 mcg/L or lower depending on test sensitivity
IGF-1 goal is to be normal for age and gender
Can measure these following oral glucose tolerance test (OGTT)
See if therapy is effective (measure elevated glucose)
GH should drop when glucose is elevated
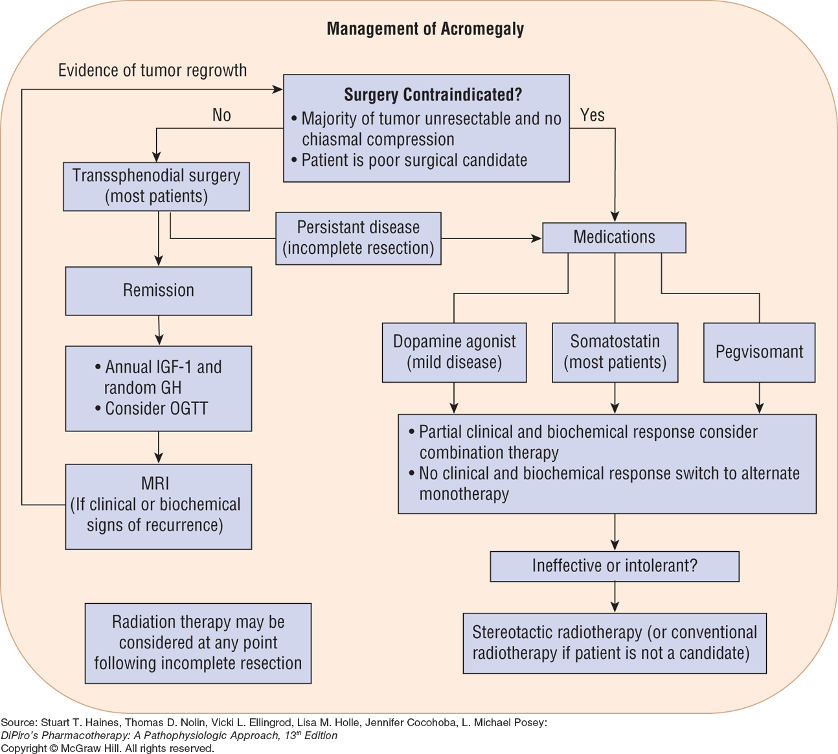
chart for acromegaly management
dopamine agonist drugs
Cabergoline or Bromocriptine
dopamine agonist
Dopamine normally stimulates release of growth hormone (GH)
Dopamine agonists (DAs) can have a paradoxical decrease of GH in acromegaly
Likely related to abnormal expression of dopamine 2 (D2) receptor on pituitary tumors
Different DAs than used for Parkinson’s
For GH, Das are ergot derivatives
DA for Parkinson’s are non-ergot and have differences in dopamine receptor binding
bromocriptine used less frequently
cabergoline used primarily due to greater efficacy over bromocriptine
DAs are least expensive options and have oral administration but less effective than others
dopamine agonist adverse reaction
Gastrointestinal effects
Nausea common
Remember: these do the opposite of dopamine antagonists that help with nausea
Taking with food may help
CNS effects
Dizziness
Impulse control: important to warn patients
Cardiovascular
Orthostatic drop
Peripheral edema: may be overlooked as a med cause
Potential for valvular heart disease with cabergoline
somatostatin analogs
•Mimic natural somatostatin
•Natural somatostatin inhibits growth hormone release
•Also decreases insulin release and affect multiple mediators in digestive tract
•octreotide and lanreotide considered similar efficacy
•pasireotide has affinity for more somatostatin receptor subtypes and may treat adenomas resistant to the other somatostatin analogs
somatostatin drugs
octreotide SUBQ: given 3 times daily
octreotide depot:
IM every 28 days
can use if benefit on SUBQ for at least 2 weeks
octreotide oral: twice daily
Indicated if has tolerated octreotide SUBQ or lanreotide
Very expensive and potentially not covered by insurance
lanreotide (Somatuline® depot): deep SUBQ every 28 days
pasireotide (Signifor®): monthly intramuscular injection
somatostatin analog considerations
Lower doses recommended for renal and hepatic impairment
Potential gastrointestinal effects, including gallstones
Glucose effect may vary
may be impacted by both medication and degree of acromegaly
pasireotide may cause more hyperglycemia
glucose monitoring important
Monitor for benefit and side effects and dose adjustment as needed
GH, IGF-1
Longer acting require multiple doses to evaluate
what to monitor for somatostatin
glucose
GH, IGF-1
pegvisomant (Somavert) MOA
Growth Hormone Receptor Antagonist
Blocks effect of growth hormone rather than affecting release
Most effective mechanism
pegvisomant (Somavert) monitor
•Daily subcutaneous injection
•More expensive than somatostatin analog injections
•GH will not decrease but monitor IGF-1
pegvisomant (Somavert) side effects
gastrointestinal effects and flu-like symptoms
elevation of hepatic aminotransferase, requiring liver function monitoring
acromegaly points
combination treatment with medications of different classes may be needed if insufficienty response to monotherapy
greater risk for adverse effects
growth hormone deficiency
May happen in children but not necessarily continue into adulthood
Growth Hormone may be used in adults who have a confirmed growth hormone deficiency
Growth hormone treatment not generally recommended in older adults
Beers Criteria indicates risk generally outweighs benefit
Exception is replacement for pituitary gland removal
growth hormone products
Multiple products are available
One not considered more effective than the other
2 products requiring once weekly dosing are available
others require daily injection
growth hormone product contraindication
history of malignancy
what to monitor for growth hormone product
may increase blood glucose, so glucose monitoring is required
growth hormone products rare effects
pseudotumor cerebri (idiopathic intracranial hypertension)
Headache, visual issues
Usually develops in first 8 to 12 weeks
Requires discontinuation
IGF-1 deficiency
•Some children may have primary deficiency of IGF-1
•Alternatively, may have IGF-1 deficiency with a resistance to GH
IGF-1 deficiency treatment
Treatment is mecasermin (Increlex®) given by subcutaneous injection
recombinant IGF-1
can cause hypoglycemia
needs to be administered within 20 minutes of eating food to avoid hypoglycemia
not indicated for adults
mecasermin (Increlex) counseling
can cause hypoglycemia
administer within 20 min of eating food to avoid hypoglycemia
monitoring growth hormone deficiency
•Needs consistent monitoring to adjust doses
•Monitor height, weight growth and IGF-1 levels
•Dose adjustments needed as a child grows
•Glucose and thyroid monitoring important
•Measure bone age every 6 to 12 months
•For adults, continue to monitor IGF-1
hyperprolactinemia
Prolactin increases normally during pregnancy
Any other elevations abnormal
Premenopausal women have naturally higher levels than men and postmenopausal women
In women can cause menstrual irregularities
In both men and women can affect sex steroid synthesis and affect libido
Can cause galactorrhea in both men and women and gynecomastia in men
hyperprolactinemia cause
Primary causes are pituitary adenomas
More often affects women; primarily have microadenomas
Men more likely to have macroadenomas
medication that can cause hyperprolactinemia
dopamine antagonists most direct effect
dopamine has an inhibitory effect on prolactin release
SSRIs, SNRIs, TCAs
estrogen, progesterone
variety of other medications have been associated
hyperprolactinemia treatment
•Surgery may be indicated for some patients
•Pharmacologic: dopamine agonists
Cabergoline primary treatment
hyperprolactinemia primary treatment
•Cabergoline primary treatment
•Considered more effective and fewer side effects than bromocriptine
•Can actually shrink tumors over time
dopamine agonist monitoring for hyperprolactinemia treatment
•Monitoring every 6 to 12 months
•Can consider dose reduction or withdrawing treatment with improvement over time
•If a woman becomes pregnant, dopamine agonists not recommended during pregnancy (monitoring therapy) unless the adenoma becomes more severe
Syndrome of Inappropriate Anti-Diuretic Hormone
issue with not being able to suppress AVP
AVP responsibility and what it causes
AVP responsible for helping with retention of water
Results in fluid retention
Concentrates urine
Causes hyponatremia from dilution and urine loss
SIADH causes
different potential causes
tumors secreting AVP
CNS issues: (ex: stroke, trauma)
medications
medications that cause SIADH
chlorpropamide
carbamazepine/oxcarbazepine
SSRIs
various others
SIADH treatment
Treat underlying condition
If possible
Key for pharmacists is to help determine if medication can be the cause
Fluid restriction (<1L/day)
may be difficult to maintain
may not be appropriate for all situations depending on underlying issue(s)
Salt (sodium) supplements: depending on sodium level/severity
Diuresis: generally mild diuresis used
AVP receptor antagonist drug
•Tolvaptan (Samsca®): also called “vasopression antagonist”
AVP receptor antagonist when to use
•Reserved if other treatments not effective
tolvaptan concerns
Concern about overcorrection/correction too rapidly
Careful monitoring required and only recommended in hospital
Fluid restriction during initiation not recommended to avoid overcorrection
tolvaptan duration of treatment
not recommended beyond 30 days
tolvaptan warning
has a warning about liver harm (specifically for high dose to treat polycystic kidney disease)
other medications for SIADH
•Some data with SGLT-2 inhibitors
•Urea has been given but limited evidence
•Demeclocycline: nephrotoxicity concerns
•Lithuim: not common
arginine vasopressin deficiency (AVP-D) causes
•posterior pituitary being unable to produce AVP (neurogenic)
•kidneys do not respond well to AVP (nephrogenic)
what does AVP-D result in
•Polyuria
•Nocturia
•Increase in serum sodium and osmolality: from concentration due to water loss
•Polydipsia (increased thirst): response to increase water intake to balance
AVP-D primary treatment
For neurogenic, primary treatment is desmopressin (DDAVP®)
analog of AVP
replacing the key hormone
desmopressin dosage forms
•Oral tablet for those who can swallow
•Nasal spray
additional AVP-D treatment
May be helped by low sodium, lower protein diet (decreased solute diet)
Low-dose hydrochlorothiazide may help, especially for nephrogenic
NSAIDs, especially indomethacin have been used-for fluid retention
Others have been utilized but not common because of some AVP effects
chlorpropamide
carbamazepine
clofibrate
AVP-D monitoring
Sodium levels
Urine output
Continued need based on underlying issue
May be permanently needed for some patients
Others may improve with improvement in underlying condition