Tissue integrity
1/77
Earn XP
Description and Tags
Concepts: Perfusion, Gas Exchange, Nutrition, Motion, Tactile Sensory Perception, Elimination, and Pain
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
78 Terms
Functions of the skin
Protects the body, helps retain fluids and electrolytes, enables sensation, thermoregulates, synthesizes vitamin D, and excretes sweat, urea, lactic acid, expresses emotions, and replaces dead cells.
Epidermis
Avascular w/melanocytes and active cells generated in the stratum germinativum that fill the stratum corneum with 30 of these layers
Keratinization
A process in which Keratin (protein) flattens, hardens, and makes newly generated cells waterproof. 30 of these layers make up the Basale layer.
Melanocytes
Produced in the basal cell layers, it secretes melanin to give pigment to skin and hair and protects from UV lights
Dermis
Highly vascular (supplies epidermis) w/ connective tissue (contract w/body movement). Controls dilation and constriction of blood vessels, and uses sensory nerve fibers to detect pain, touch, and temperature.
Hypodermins (Subcutaneous)
Anchor to upper layers. Has loose connective tissue and is filled with subcutaneous fat that helps retain heat, cushions, and provide calories.
Eccrine sweat glands
Controlled by the nervous system, these glands allow regulation of body temperature by secreting water through the surface of the skin
Aprocrine sweat glands
Only in axillae, nipples, areolae, anogenital area, eyelids, and external ear. Begin at puberty and secrete odorless fluid filled w/protein, carbs, and others. Its decomposition is associated w/body odor.
Sebaceous glands
A lipid-rich substance called sebum keeps hair and skin lubricated. Stimulated by sex hormone activity, accelerates during puberty
Which of the following is a risk factor for skin cancer?
A. Personal history of skin cancer
B. Family history of skin cancer
C. Older age
D. Exposure to UV light (lifetime sun exposure, sunburn, or indoor tanning)
E. Light skin (blonde or red hair)
F. Blue/green eyes
G. Moles
All of the above
Skin cancer primary preventions
Protect skin (wear hats, tight woven clothes, sunglasses, and SPF sunscreen +15)
Seek the shade
Avoid sunbathing + indoor tanning
What is an additional primary prevention from the U.S. service task force
Avoid UV light exposure from ages 6m-24yrs
Skin cancer secondary prevention
Examine new or unusual lesions immediately and use ABCDE melanoma mnemonics
what does ABCDE stand for in melanoma mnemonics
Asymmetrical
Border poorly defined/irregular
Color uneven/variegated
Diameter larger than 6mm
Evolving, changes shape, size, color
Pruritis, Red/purpleish rash, and dry skin
History of chronic illness from present health status
Current medications from present health status
allergic reactions/hives, thinning of skin/acne
Past health history of present health status
Hx of skin/nails disease serve as clue to current skin lesions
Family history from present health status
Family hx of skin cancers manifesting w/rash and alopecia
Personal and psychosocial history from present health status
Health care use of preventive measures, or exposure to chemicals due to work like cosmetology, health care, etc.
Cyanosis, pallor, jaundice, hypopigmentation, and hyperpigmentation
Unexpected findings when inspecting the generalized color for skin
Hypopigmentation
albinism or the absence of pigmentation
Hyperpigmentation
Increased melanin may indicate an endocrine disorder like Addison’s disease or liver disease
Melanoma, vitiligo, maceration, discoloration, rashes and localized hyperpigmentation
Unexpected finding when inspecting localized color of the skin
Pigmented nevi (moles), freckles, patches, and striae that is white or pink
Expected findings when inspecting localized color of the skin

Maceration
Too much moisture on skin. Unexpected finding of localized skin color w/discoloration and rashes.

Melanoma
Moles below the waist, on scalp, or breast are not normal, may have abnormal characteristics. Unexpected in localized skin color

Vitiligo
Development of unpigmented patch or patches, more common in dark-skinned people w/autoimmune disorder. Unexpected in localized skin color

Pigmented Nevi
Moles, common on chest, back, arms, legs, and face or sun-exposed areas. Normal finding in localized inspection of skin color

Striae
Stretch marks that are silver or pink, secondary to weight gain or pregnancy. Normal finding when inspecting the localized color of skin
Coining
Common practice by many, particularly Southern Asian’s that uses coins or spoon and rubs over bony prominences of rib cage on back and chest.
Cupping
Practiced by Russians and Latin Americans, a form of alternative medicine for arthritis, stomach aches bruises, and paralysis. Uses heated glass cups to create negative pressure to adhere to skin, leaving red marks
Palpate the skin for: Texture
Expected: Must be smooth, soft, and intact (calluses may be present)
Unexpected: Dry, flaking, crackling, or scaling skin (nutritional deficiency)
Palpate the skin for: Temperature
Use back of hand to find the unexpected:
Generalized cool skin → Hypothermia or poor peripheral perfusion
Generalized hot skin → Hyperthermia, increased BMR, hyperthyroidism, inflammation, infection, sunburn, or traumatic injury
Palpate the skin for: Moisture
Unexpected: Diaphoresis or excessive sweating in the absence of physical activity.
Indicates hyperthermia, anxiety, pain, or shock. Excess moisture can be due to hyperthyroidism
Palpate the skin for: Mobility and Turgor
Unexpected:
Scleroderma→ connective tissue disorder decreasing skin mobility
Tenting → Slow return of skin to original condition (indicates weight loss or dehydration)
Turgor positive
Slow receding of the skin back to its original place (tenting)
Palpate the skin for: Thickness
Unexpected: thick and thin skin caused by
Diabetes mellitus → Due to collagen resulting in hyperglycemia.
Excessively thin skin looks shiny and is due to hyperthyroidism, arterial insufficiency, and aging
Inspect and palpate the scalp and hair for surface characteristics, hair distribution, texture, quantity, and color
Unexpected:
Parasitic infections (lice)
Alopecia (hair loss) → autoimmune disorders, anemic conditions, treatment w/radiation, or antineoplastic agents.
Dull, coarse, and brittle hair → malnutrition.
Alopecia
Hair loss different from balding (doesn’t happen gradually, symmetrically, by high androgen, and genetic disposition like balding)
Inspect facial and body hair for distribution, quantity, and texture
Unexpected:
Hirsutism → Deviation from normal hair growth pattern (triangle for men, inverted triangle for women)
Thinning of the eyebrows (hypothyroidism)
Hirsutism
Hair growth in women with an increase of hair on the face, body, and pubic area
Inspect the nails for shape, contour, and color; palpate for thickness and firmness
Unexpected:
Excessive length or damage to edges, grooves, depressions, pitting, and ridges.
Pitting→ Psoriasis caused (minor pitting may also be normal)
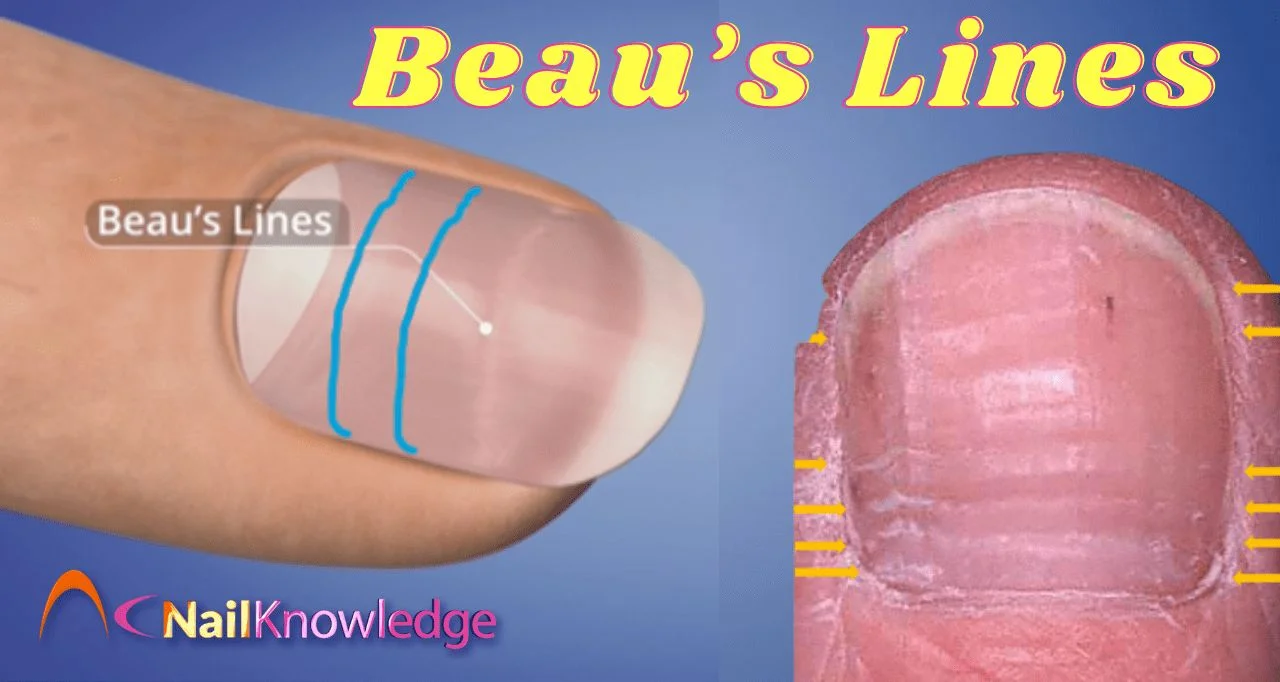
Beau’s lines
Grooves or transverse depression running across the nails. Grooves move from cuticle to top of nail. Caused by stressors like trauma.

Koilonychia
Spoon nail, present as thin depressed with lateral edges turned upward (can be anemia or congenital problem)

Leukonychia
White spot-on nail plate, associated w/minor trauma or manipulation of the cuticle.
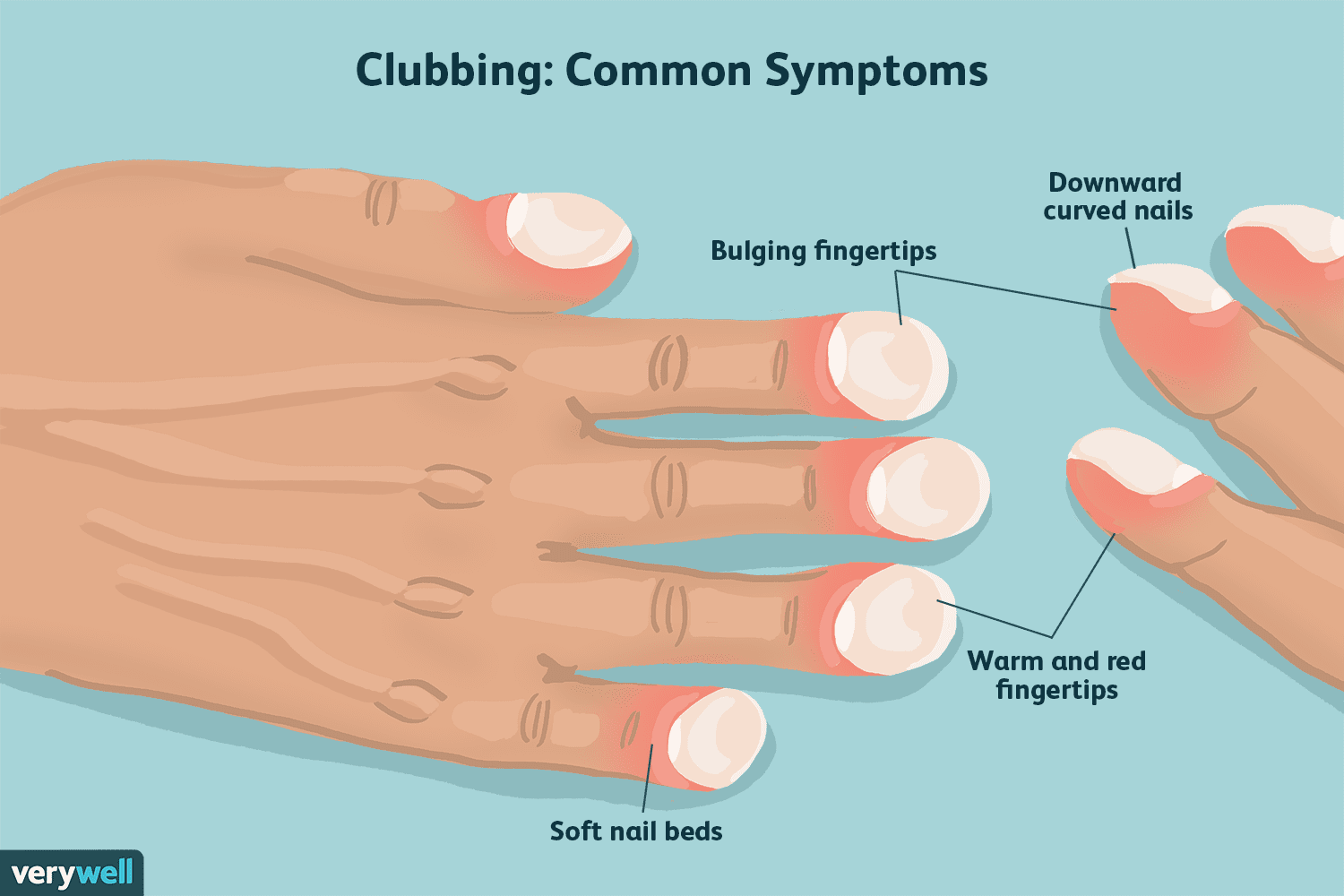
Clubbing
Angle of nail base exceeds 180. Common in COPD or cardiovascular disease, caused by proliferation of the connective tissue, enlarging distal fingers
Why inspect and palpate skin lesions?
When new lesions appear, changes occur, or pain is identified. Inspect primary, secondary, and vascular lesions
Primary lesions
Expected variations in the skin like freckles, moles (nevi), patches, comedones (acne). Use Wood’s lamp to identify infections
Secondary lesions
Expected variations like Scars
Vascular lesions
Common variations of the skin like Ecchymosis (bruising), Telangiectasis, and cherry angioma

Telangiectasis (vascular lesion)
Permanent dilation of preexisting small blood vessels (capillaries, arterioles, or venules) resulting in superficial, fine, irregular red lines within the skin
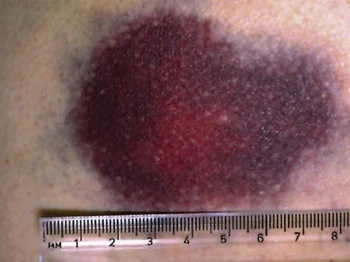
Ecchymosis (vascular lesion)
Flat, reddish-purple, nonblanchable bruising spot of variable size. Blue/purple in light skin; blue or black tone in dark skin.

Vascular spider (spider angioma) (vascular lesion)
Type of telangiectasia characterized by a small central red area with radiating spiderlike legs; this lesion blanches with pressure
Occur in absence of disease, with pregnancy, in liver disease, or with vitamin B deficiency.

angioma (e.g. cherry angioma) (vascular lesions)
Benign tumor consisting of a mass of small blood vessels; can vary in size from very small to large.

Capillary hemangioma (nervous flammeus) (vascular lesions)
Type of angioma that involves the capillaries within the skin producing an irregular patch that can vary from light red to dark red to purple in color.
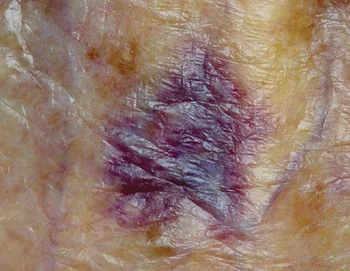
Purpura (vascular lesion)
Flat, reddish-purple, nonblanchable discoloration in the skin greater than 0.5 cm in diameter. Infection or bleeding disorders resulting in hemorrhage of blood into the skin.

Venous star
Type of telangiectasia characterized by a nonpalpable bluish, star-shaped lesion that may be linear or irregularly shaped. Unexpected vascular lesion, caused by increased pressure on superficial veins.

Petechiae
tiny red spots less than 5 cm big. Tiny hemorrhages within the dermal or submucosa—caused by intravascular defects and infection. Unexpected in vascular lesions.
Scale
Secondary skin lesions, heaped-up keratinized cells; flaky, irregular, thick or thin, dry or oily. Unexpected. Can follow drug reaction, eczema, seborrheic dermatitis, follows scarlet fever.

Lichenification
Secondary skin lesions, unexpected rough, thickened epidermis secondary to persistent rubbing, pruritus, or skin irritation in chronic dermatitis or psoriasis

Keloid
Secondary skin lesion. Irregular shaped elevated, enlarging scar. Follows after surgery. Unexpected
Scar
Secondary skin lesion. Surgical or healed wound, thin or thick fibrous tissue replacing normal skin. Unexpected.

Excoriation
Secondary skin lesion. Unexpected loss of epidermis, linear hollowed-out crusted area from abrasions or scratches, scabies.
Fissure
Secondary skin lesion unexpected linear crack or breaks from epidermis to the dermis found in athlete’s foot, cracked skin, chapped hand,

Crust
Secondary skin lesion unexpected, dried drainage or blood, slightly elevated with mix colors by scab on abrasion or eczema.

Erosion
Secondary skin lesion unexpected loss or part of the epidermis. Depressed, moist, glistening that may be due to varicella or following rupture of bulla

Ulcer
Secondary skin lesion expected loss of epidermis or dermis, concave by pressure ulcers, stasis ulcers, or syphilis chancre.

Macule
Primary lesion like freckles, nevi, petechiae, measles, or scarlet fever

papule
primary lesion unexpected wart or elevated mole, cherry angioma, or skin tag that is firm and less than 1 cm diameter

patch
primary lesion unexpected nonpalpable, irregular-shaped

plaque
primary lesion unexpected by psoriasis, elevated, firm, rough, with flat top surface greater than 1 cm

wheal
primary lesion unexpected caused by insect bites or allergic reactions and even urticaria

nodule
primary lesion, elevated, deeper than dermis, unexpected in dermatofibroma erythema.

Tumor
Primary lesion unexpected solid lesion, not clearly demarcated, neoplasm

Vesicle
Primary lesion unexpected caused by varicella filled w/serous fluid

Bulla
primary lesion unexpected vesicle greater than 1 cm, blister

Pustule
primary lesion unexpected in impetigo, acne, and folliculitis elevated and similar to a vesicle but filled with purulent fluid like acne

Cyst
Primary lesion unexpected and encapsulated lesion in dermis or subcutaneous layer.