Apex Mock Exams + Valley Pre-course Exam
1/99
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
100 Terms
"Can't ventilate, can't intubate" scenario. What is the best way to secure the airway?
Requires an emergent surgical airway
a) surgical cricothyrotomy
b) transtracheal jet ventilation
tracheostomy and retrograde intubation are not considered emergent airways
Convert Fahrenheit to Celsius
F= (C x 1.8) + 32
What are the best oxygen sources for transtracheal ventilation?
High pressure O2 sources (TTJV requires psi of at least 25)
1. jet ventilator attached to anesthesia machine
2. O2 tank with a pressure regulator set to 50 psi
3. O2 flush valve on the anesthesia machine
Low pressure O2 sources (self resuscitation bag or reservoir bag on the anesthesia machine) are not used for TTJV because they cannot fill the lungs with adequate O2 flow
LA ranked from shortest DOA to longest DOA
a) procaine
b) lidocaine
c) chloroprocaine
d) bupivacaine
e) mepivacaine
f) tetracaine
g) ropivacaine
shortest (lowest protein binding) : procaine, cholorprocaine (zero protein binding)
intermediate: lidocaine, mepivacine
longest (most protein binding): bupivacaine, ropivacaine, tetracaine
In a cirlce system, work of breathing is primarily determined by which component of the system?
Think about Pouiselle's Law...
Whatever answer choice gives you the smallest diameter--> decreased radius/diameter increases resistance
ETT is likely the answer since it has the narrowest diameter out of the Y piece, unidirectional valves and circuit tubing
In the 15 kg pediatric patient who experiences cardiac arrest, what is the first defibrillation shock set at? What about the second attempt?
first attempt: 2J/kg --> 30 J
second attempt if necessary: 4J/kg --> 60 J
Rank the following tests of neuromuscular function based on the % of receptors that can be occupied when the desired response is achieved
TOF 4/4
double burst stimulation without fade
TV 5mL/kg
biting on tongue blade for longer than 5 seconds
TV 5 mL/kg-- 80% of receptors still occupied by NMBD
TOF 4/4 -- 70% of receptors still occupied by NMBD
double burst stimulation without fade -- 60% of receptors still occupied by NMBD
biting on tongue blade > 5 seconds -- 50% of receptors still occupied by NMBD (this is the most sensitive test of reversal)
Surgery is needed within __ hours of spinal hematoma symptoms. If delayed for more than __ hours, recovery is unlikely.
8 hours
surgical decompression needs to happen within 8 hours of spinal hematoma symptoms or recovery is unlikely
2 causes of hypocalcemia in the operating room
1. administration of PRBCs (citrate binds calcium)
2. hyperventilation (causes decreased ionized calcium because H+ ions get displaced from plasma proteins and Ca takes its place)
Equation for therapeutic index (TI)
LD50/ED50
Post synaptic nicotinic receptors are found at each of the following sites EXCEPT:
a) NMJ
b) SA node
c) autonomic ganglia
d) adrenal medulla
B- muscarinic receptors and adrenergic (B1) receptors are at the SA node
Rank the following from most likely to least likely to cause a perioperative allergic reaction
muscle relaxants
antibiotics
latex
protamine/ blood products
most likely: 1. muscle relaxants (50-60%)
2. latex (15%)
3. antibiotics (10-15%)
4. protamine/ blood products (<2-3%)
What dose of epi causes beta effects?
low dose epi 0.01-0.03 mcg/kg/min --> beta effects (B1= increased HR and contractility, B2= decreased SVR)
intermediate dose epi 0.03-0.15 mcg/kg/min --> mixed alpha and beta
high dose epi >0.15 mcg/kg/min --> alpha effects (increased SVR--> increased BP)
What is the first step of the soda lime reaction?
What are the final products of the soda lime reaction?
First step:
CO2 + H2O --> H2CO3
(carbonic acid)
Final products:
CaCO3 + NaOH
(calcium carbonate and sodium hydroxide)
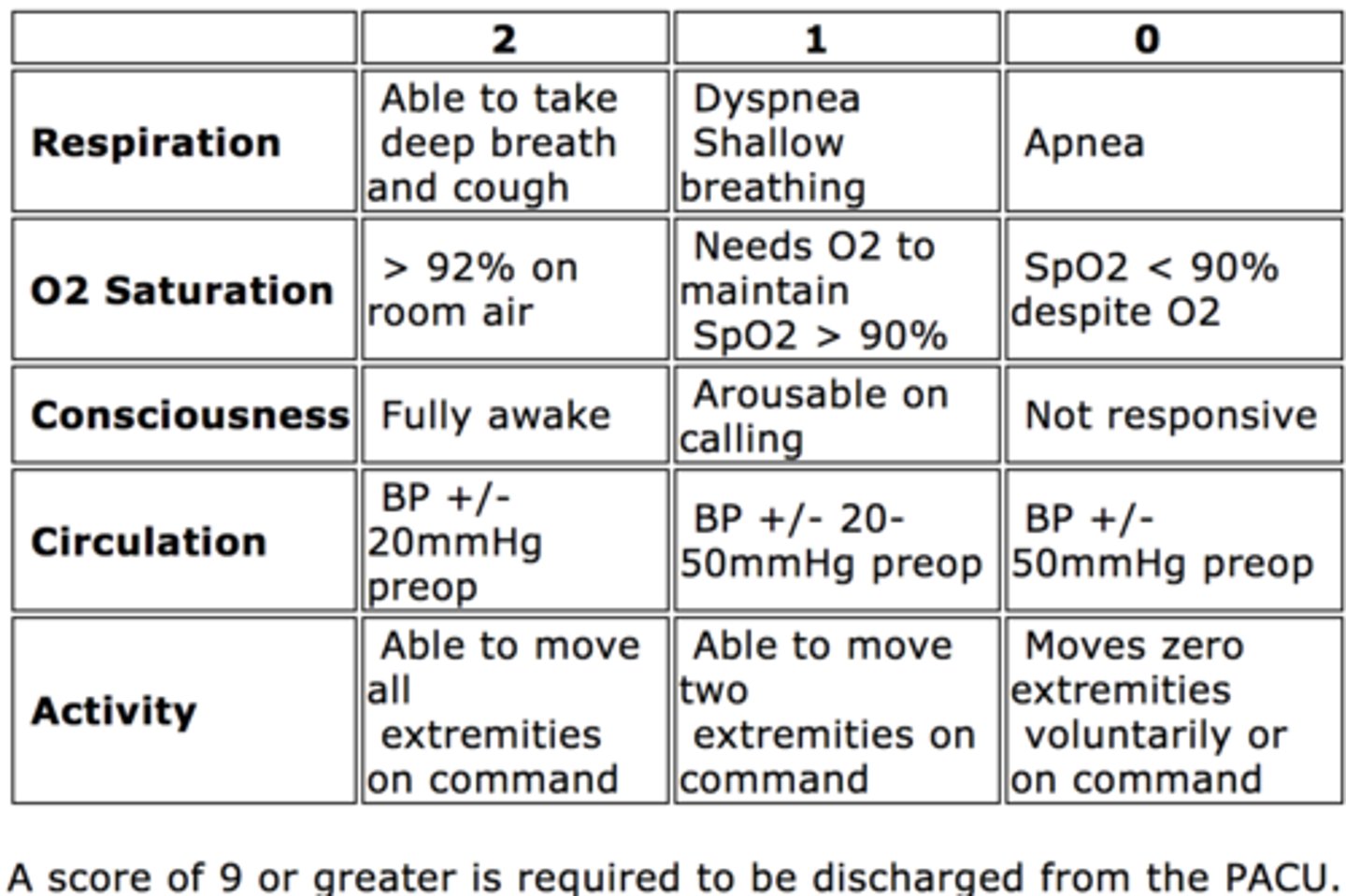
What is the Aldrete Score and what does it quantify?
Quantifies recovery from anesthesia
Drug eluding stent vs metal stent
How long after stent placement should another surgery be delayed?
DES: delay surgery for 6 months if possible
metal stent: delay surgery for a minimum of 30 days
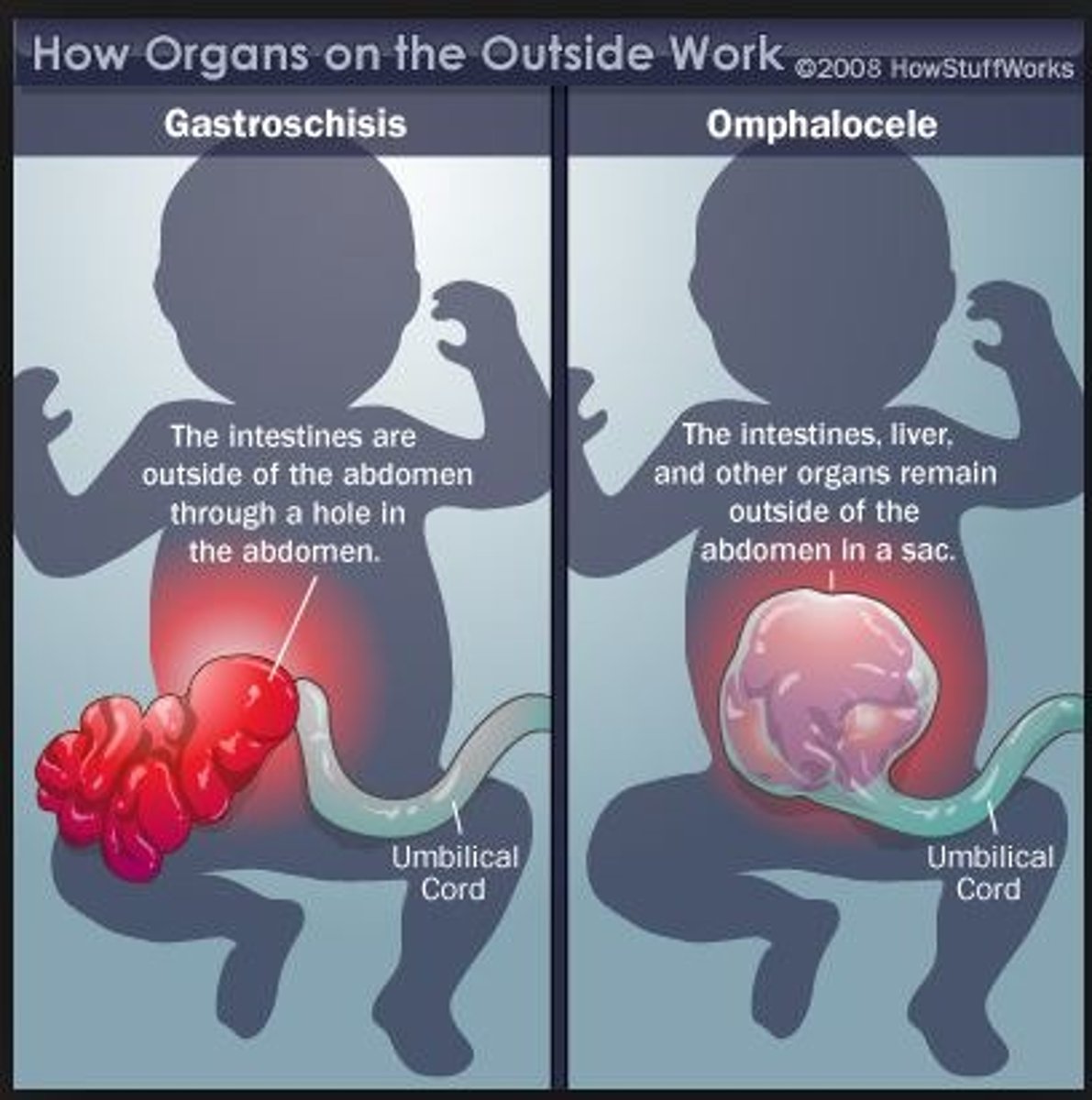
Gastroschisis vs. Ompahlocele
Where do abdominal contents spill out from?
Are abdominal contents covered in a sac?
Which one is more associated with prematurity?
Which one is associated with congenital abnormalities?
Gastroschisis
-abdominal contents coming from right of umbilicus
-abdominal contents NOT covered by a sac
-happens more commonly with prematurity
-not associated with congenital abnormalities
Ompahlocele
-abdominal contents coming from midline defect
-abdominal contents covered by sac
-associated with congenital abnormalities
Name some drugs that interfere with SSEP monitoring.
What drugs are safe to use when SSEP monitoring is happening?
Drugs that impair SSEPs (decrease SSEP amplitude and increase SSEP latency)
-volatiles, N2O
-propofol
-barbiturates
-midazolam, diazepam
Drugs that do not impact SSEP monitoring
-ketamine
-dexmeditomidine
-opioids
-droperidol
In a 70 kg patient, figure out how much HCO3- needs to be administered to go from a serum bicarb level of 20 mEq/L to a serum bicarb level of 25 mEq/L.
1. goal bicarb level MINUS current bicarb level --> 25- 20= 5 mEq/L
2. multiply 5 by patient weight (kg) and 0.3 (constant) --> 5 x 70 x 0.3= 105 mEq/L
3. divide 105 mEq/L by 2 --> 52.5 mEq/L
This patient needs 53 mEq/L of bicarb to go from 20 to 25.
Mannitol dosing
0.25- 1 GRAM/kg
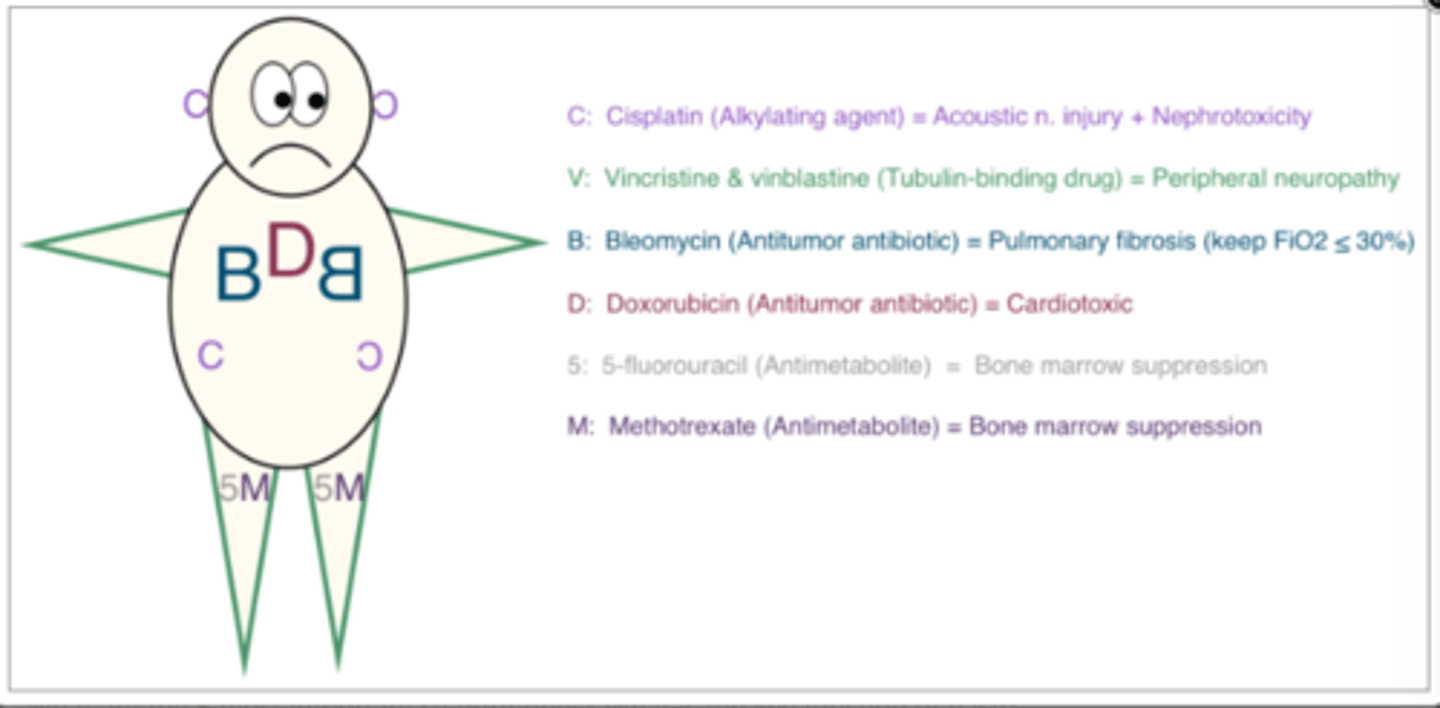
Which chemo agents are alkylating agents, antitumor antibiotics and tubulin binding agents?
Alkylating: Busulfan, Carmustine, Cyclophosphamide, Cisplatin
Antitumor ABX: Doxorubicin, Danorubicin, Bleomycin
Tubulin Binding: Vinicristine (Vinca alkaloids), taxanes
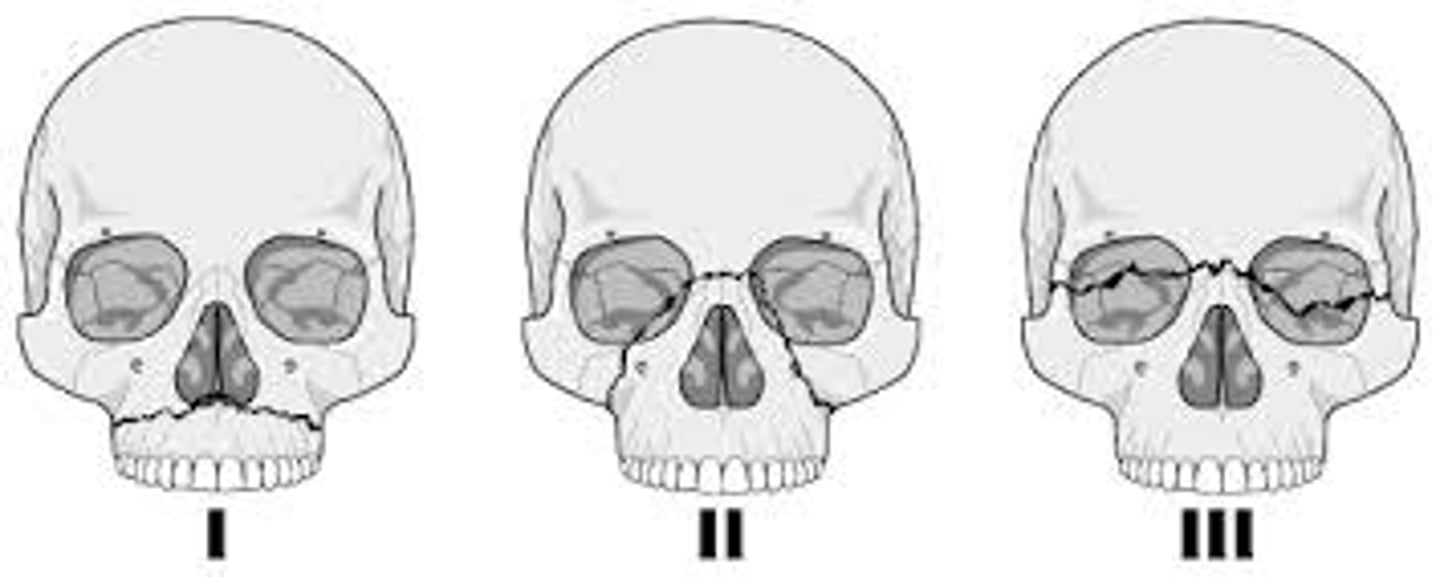
Where is a LeFort II fracture located?
Which LeFort fracture is associated with an intact cribiform plate?
Which LeFort fracture are nasal intubations contraindicated in? Why?
LeFort II: upside down V- goes above bridge of nose and under the eye sockets
LeFort 1: intact cribiform plate- nasal intubations are okay because CSF leak is unlikely
LeFort II & III: nasal intubations contraindicated, could have basilar skull fracture (raccoon eyes, CSF leak likely)
After a tourniquet on a lower extremity is released, what do you expect to see an increase in on your monitors?
Increase in ETCO2
Will see a decrease in BP, HR, SVO2, PAP and pH due products of lactic acid metabolism being released into systemic circulation
How many ml of 0.9% NS needs to be added to 1 mL of 1:1000 epinephrine to make the concentration 2.5 mcg/ml?
1:1000 --> 1000 mg/1000 ml --> 1 mg/ml
1mg/ml = 1000 mcg/ml
dose on hand (1000 mcg/ml) / dose desired (2.5 mcg/ ml) = 400 ml TOTAL
399 ml of NS needs to be added to 1 ml of epi to make it 2.5 mcg/ml
How do you find the hemoglobin value from a question with only hematocrit values?
Ex: Patient's Hct is 24. 2 units of PRBCs are transfused. What is this patient's new hemoglobin after transfusion?
Hgb can be estimated to be 1/3 of Hct
Each unit of PRBCs increases Hgb by ~1 g/dL and Hct by ~1-3%
starting Hgb ~ 8 g/dL
after 2 units of PRBCs, new Hgb ~ 10 g/dL (new Hct ~ 30%)
Which antidysrhythmic drug should not be given to an asthmatic?
Adenosine
Could cause adenosine- induced bronchospasm in someone with a reactive airway (thought to be from bronchoconstriction and histamine release)
Compare the following epidural infusions and where the opioid is exerting its analgesic effects:
a) epidural infusion of fentanyl
b) epidural infusion of morphine
a) epidural infusion of a lipophilic opioid (fentanyl, sufentanil) exerts its analgesic effects systemically (lipophilic drugs will leave the epidural space and enter the plasma more readily compared to more hydrophilic drugs)
b) epidural infusion of a hydrophilic opioid (morphine, hydromorphone) exerts its analgesic effects in the dorsal horn of the spinal cord
BMI equation
BMI = kg/m2
1. be sure to change pounds to kg (divide pounds by 2.2)
2. change height in inches to height in cm (inches x 2.54)
3. change height in cm to height in m (divide by 100)
A neonate with pyloric stenosis is likely to have what disturbances?
a. metabolic alkalosis
b. metabolic acidosis
c. hyperkalemia
d. hypokalemia
e. hyperchloremia
f. hypochloremia
vomiting of acids, chloride and potassium leads to hypokalemic, hypochloremic metabolic alkalosis
a, d, f
If a pregnant patient needs to have surgery, what is the fetus at risk for?
surgery in a parturient can lead to:
-preterm labor
- low birth weight
- growth restriction
- fetal demise
anesthesia for surgery will not necessarily lead to congenital abnormalities (but always avoid N2O in the pregnant patient)
What makes up the afferent limb of the oculocardiac reflex? (3)
a) Vagus nerve
b) Trigeminal nerve
c) ciliary nerves
d) SA node
e) gasserian ganglion
f) stellate ganglion
B, C, E
afferent limb: ciliary nerves--> ciliary ganglion --> trigeminal nerve --> gasserian ganglion
efferent limb: Vagus nerve --> SA node
Hydralazine
afterload/preload reducer?
what happens to heart rate?
takes how long to start working?
can cause what drug induced autoimmune disease?
direct acting vasodilator (afterload reducer)
decreased BP with reflex tachycardia
10-15 minutes before effects are seen
can cause drug induced Systemic Lupus Erythematosus
What is the weight based dose for cocaine?
Max dose of cocaine is ___ mg
1.5-3 mg/kg
max dose of 200 mg
What can be seen in someone with hyperparathyroidism? (3)
a) prolonged QT interval
b) shortened QT interval
c) HTN
d) hypotonia
e) CHF
f) Chvostek's sign
B, C, D
hyperparathyroidism causes s/sx of hypercalcemia (stones, thrones, bones, groans, psych overtones)
s/sx of hypercalcemia:
-shortened QT interval
-HTN
-hypotonia
-kidney stones
- cognitive dysfunction
s/sx of hypocalcemia:
-prolonged QT interval
-Chvostek's sign
- CHF
-tetany
How many Joules should be delivered during the 1st cardioversion attempt?
1st attempt: 50-100J
if that does not fix rhythm, 2nd attempt at 100-200 J
do not exceed 360J
What are the physiologic consequences of a pneumoperitoneum?
MAP
CO
FRC
A-a gradient
ICP and CPP
Renal and liver blood flow
-increase in MAP (CO2 absorption from insufflation causes hypercarbia, which causes an increase in MAP)
-decreased CO (d/t decreased venous return)
-decreased FRC (which increases A-a gradient)
-increased ICP and CPP (from increased MAP)
-decreased renal and hepatic BF (d/t compression of kidney and liver)
What ventilator setting will have a change in delivered TV if lung compliance or airway resistance changes?
Pressure control ventilation--> change in delivered TV if compliance or resistance changes (VCV will not have a change in TV if compliance or resistance changes)
What SSEP changes suggest increased risk for nerve injury?
__% increase/decrease in latency
__% increase/decrease in amplitude
10% increase in latency
50% decrease in amplitude
How long must you avoid N20 after the following gas bubbles are placed for retinal detachment surgery
Silicone oil bubble
Air bubble
Sulfur hexafluoride bubble
Silicone oil bubble- 0 days
Air bubble- 5 days
Sulfur hexafluoride bubble- 10 days
Match the following hormones to their action:
secretin, gastrin, cholecystokinin
Stimulates pepsinogen secretion
Stimulates gallbladder contraction
Stimulates bile flow
Gastrin- secreted by G cells; stimulates pepsinogen secretion
Cholecystokinin- secreted by I cells; stimulates gallbladder contraction
Secretin- secreted by S cells; stimulates bile flow
Gap acidosis
What are the causes?
Gap acidosis= too much H production or not enough H elimination (A MUD PILE)
A aspirin
M methanol
U uremia/renal failure
D diabetic ketoacidosis
P propylene glycol
I infection
L lactic acidosis
E ethylene glycol
Non- gap acidosis
-also called ________ acidosis
-What are the causes?
aka hyperchloremic metabolic acidosis- caused by excessive loss of HCO3- or too much Cl- (USED CAR)
U ureteral diversions
S small bowel fistulas/ pancreatic fistulas
E excessive Cl-
D diarrhea
C carbonic anhydrase inhibitors
A adrenal insufficiency
R renal tubular acidosis
Considerations for TOF monitoring in a patient who has hemiparesis on one side of the body (could be from CVA or tumor)...
hemiparesis= weakness --> less use of the affected side results in denervation + increased number of extrajunctional receptors at the NMJ
- they have decreased sensitivity to NDMR and increased sensitivity to succ (potential for extreme hyperkalemia)
TOF should not be monitored on the affected side because it will give a falsely elevated response (strong twitches may indicate adequate reversal but its not accurate due to the extrajunctional receptors)
TOF should be monitored on the non affected side.
What are the NMBD considerations in disease states that are associated with extrajunctional receptors at the NMJ?
extrajunctional receptors= a2b1d1g1 or a7 = more Ach binding sites
depolarizers= increased sensitivity
non depolarizers= decreased sensitivity
since succ / depolarizing NMBD are Ach agonists, there is increased sensitivity of these drugs because there are more Ach receptors.
non-depolarizing NMBD act as competitive antagonists at the Ach receptor. More Ach receptors means NDMR have less effect at the normal dose, there is decreased sensitivity of these drugs.
What syndrome is associated with the following triad:
1. Obesity
2. Hypertension
3. Type 2 diabetes mellitus
Metabolic syndrome
Always associate a patient with previous meninogomyelocele surgery to have __________
allergy to latex
Necrotizing Enterocolitis (NEC)
What kind of induction?
What induction meds are good to use?
What induction meds should be avoidied?
These babies ARE SICK and probably already in an acidotic state
RSI induction with roc (avoid succ d/t hyperkalemia)
Ketamine and opioids are good options. (as opposed to pyloric stenosis where you want to avoid opioids)
avoid halogenated agents and propofol (d/t hemodynamic Instability)
Covert:
Celsius to Fahrenheit
Celius to Kelvin
F= (C x 1.8) + 32
K= C + 273
Classic LMA will allow for PPV up to ____ cm H2O
Proseal LMA will allow for PPV up to ____ cm H2O
What is the maximum cuff pressure for a Classic LMA?
Classic LMA PPV up to 20 cm H2O
Proseal LMA PPV up to 30 cm H2O
Classic LMA maximum cuff pressure= 60 cm H2O (never exceed this pressure)
When properly placed, the distal tip of the LMA should sit where?
distal tip should sit at the cricopharyngeus muscle (right at the upper esophageal sphincter)
Which antiemetics can prolong the QT interval and should be avoided in patients with known Prolonged QT Syndrome?
Avoid:
droperidol
ondansetron
decadron and scopolamine would be good to give these patients
Find the TV delivered to a patient when there is fresh gas flow coupling.
O2 flow= 2L/min
air flow= 1L/min
set TV= 450 mL/min
RR= 10 breaths per min
I:E= 1:2
1. add the coupled flows together and change from L to mL
2L/min + 1L/min = 3L/min = 3000 mL/min
2. multiply by the time spent in inspiration (1 sec I, 2 sec
E, total of 3 sec)
3000mL/min * 1/3 = 1000 mL/min
3. divide by RR
(1000 mL/min) / (10 breaths/min) = 100 mL/breath
4. add 100 mL to the set TV of 450 mL --> 550 mL
550 mL is the TV actually delivered
How many L of CO2 does a 70 kg male produce in one hour?
Resp quotient= CO2 produced/ O2 consumed (per minute)
0.8= x/250 ml/min
x= 200ml/min --> 0.2 L/min --> 0.2 x 60 minutes= 12 L/hour
12 L/hour
Match the vasodilator with its site of action
Prazosin
Nitroglycerin
Nitroprusside
Arterioles and venules
Arterioles
Venules
Prazosin --> arterioles
Nitroglycerin (preload reducer)-- > venules
Nitroprusside (preload and afterload reducer) --> arterioles and venules
Which of the following poses the highest risk of 30- day mortality in an elderly patient?
age > 90 yrs
ASA 4
acute renal impairment
emergent surgery
unplanned ICU admission
1. highest risk of 30 day mortality= ASA 4
2. age >90
3. acute renal impairment
4. unplanned ICU admission
5. lowest risk of 30 day mortality from options provided= emergent surgery
Acute intrinsic lung disease is characterized by ___
what are some examples?
fluid moving into alveoli and interstitial space of lung parenchyma
examples: pulmonary edema, aspiration pneumonia, ARDS
When used in a balanced anesthetic, CV effects of N2O include:
SNS activation: increased SVR, increased BP and increased HR
with combined with opioids, N2O can cause myocardial depression
Asynchronous pacing
-best to use in what kind of patients?
-what does this pacing mode do?
-what are some examples of this mode?
best to use in patients with no underlying intrinsic rhythm (that way it can't produce R on T)
PaSeR
Asynchronous pacing = PACES ONLY
does not sense or respond to sensed electrical event
examples: AOO, VOO, DOO
Autonomic hyperreflexia
what are the 2 most common symptoms?
what can occur to the heart, lungs and brain if not kept under control?
Classic presentation= HTN and bradycardia
stimulation of area below level of injury causes massive SNS activation below the injury
Increased SVR --> HTN --> reflex bradycardia
Increased SVR --> LV failure --> pulmonary edema
Extreme HTN (beyond auto-regulation parameters) can cause increase in CPP and ICP and can cause seizures
What is the initial dantrolene dose for treating MH?
2.5 mg/kg
What is the most common complication of mediastinoscopy?
a) pneumothroax
b) phrenic nerve damage
c) hemorrhage
d) MI
C) hemorrhage
What is the most common cause of death in patients having a carotid endarterectomy?
a) stroke
b) MI
c) hemorrhage
d) pulmonary embolism
b) MI
Which NMBD has antimuscarinic properties?
Antimuscarinic = anticholinergic
Pancuronium
What virus is most easily transmitted by blood transfusion?
a) hep A
b) hep B
c) hep C
d) cytomegalovirus
d) cytomegalovirus
What is the most frequently damaged nerve in the upper extremity and lower extremity?
UE= ulnar nerve
LE= common peroneal nerve
Which change increases intraocular pressure the most?
a) increased arterial blood pressure
b) increased central venous pressure
c) increased PaCO2
d) metabolic alkalosis
b) increased CVP
The most frequent law suit involving the anesthetist is related to:
a) airway management
b) positioning
c) preop treatment
d) postop care
a) airway management
What is true of bronchial blockers?
a) allow the isolated lung to be suctioned
b) allow the isolated lung to be ventilated
c) can be used in children < 12 years of age
d) can be used in someone who requires nasotracheal intubation
e) can be used for lung separation in someone who has a tracheostomy
f) do not need a fiberoptic bronchoscope to place
a, c, d, e
bronchial blockers:
-allow the isolated to be suctioned of air
- allow the nonisolated lung to be ventilated
- can be used in children
- can be used with nasotracheal intubations
- can be used for lung separation in someone who has a trach or single lumen ETT in place
- you do need a fiberoptic bronchoscope to place it
What is the correct size and depth of insertion for DLT in males and females?
How can you confirm correct placement and position?
Can you use a DLT in kids?
Women: 37-39 F, 27 cm
Men: 39-41 F, 29 cm
Confirm with fiberoptic bronchoscope. Assess 3 take offs for right bronchus and 2 take offs for left bronchus
No!!! The lumens would be too small, and would increase resistance to flow tremendously. Kids requiring lung separation can use a bronchial blocker.
You've placed a left DLT. When auscultating breath sounds, what would you hear if the following complications occurred:
1. DLT is too far on the left side
2. DLT enters the wrong bronchus/ in too far on right side
3. DLT sitting in the trachea
1. DLT in too far on left side= right breath sounds absent due to tracheal cuff occluding flow to right lung
2. DLT in too far on the right side= left breath sounds absent (you collapse the wrong lung)
3. DLT in the trachea= breath sounds present on both sides (this would cause failure of lung seperation)
If your DLT enters the right bronchus, what must you be extremely careful of not occluding?
The right upper lobe takeoff is right after the carina, so if the DLT is in the right bronchus, cuff inflation could occlude the RUL, extreme risk of hypoxemia)
In someone who has severe carotid artery stenosis, indicate if a carotid endarterectomy or coronary artery stenting would be most appropriate for the following scenarios:
CHF with EF <30%
severe renal impairment
CAD/unstable angina
valvular heart disease
morbid obesity
intolerance of antiplatelet agents
contralateral RLN dysfunction
Pt with severe carotid artery stenosis should receive carotid artery stenting instead of a CEA if they have:
- CHF with a low EF
- CAD/ unstable angina/ valvular disease
- morbid obesity
- contralateral RLN dysfunction
Pt should receive a CEA instead of stenting if they have:
- severe renal impairment (use of dyes in stenting would further impair renal function)
- intolerance of antiplatelet agents (stents require antiplatelet agents)
A patient with chronic pain presents to the hospital with a possbile MI. The patient has a history of gastric ulcers and renal impairment. What is his pain likely being treated with?
non-selective COX inhibitors
MOA: inhibit platelet aggregation, impair gastric lining which can lead to ulcers, impair renal blood flow)
examples: aspirin, toradol/ ketorolac, ibuprofen, naproxen, diclofenac
What are the 5 branches of CN7?
5 branches of the facial nerve (most superior to inferior)
1. temporal
2. zygomatic
3. buccal
4. mandibular
5. cervical
two zebras bit my cupcake
What is the most common comorbidity in children presenting for surgery?
URI
(don't be tempted to pick asthma or obesity because those will likely be options to distract you)
What block is most useful in patients with abdominal visceral pain (cancer of abdominal organs)?
What block is most useful in patients with cancer pain in the pelvic organs?
what block is most useful for first stage of labor pains?
What block is most useful for second stage of labor pains?
abdominal visceral pain = celiac plexus block (done at L1)
cancer pain in pelvic organs = superior hypogastric plexus block
1st stage of labor- need T10- L1 coverage (contractions to full cervical dilation, dull and cramping pain) = paracervical block (risk of fetal bradycardia), superior hypogastric block
2nd stage of labor - need S2-S4 coverage (full dilation to delivery of baby, sharp pain) = pudenal block
Regarding the geriatric population- what organ system is the primary cause of M&M risk throughout the perioperative period?
Cardiovascular system
the elderly commonly have HTN
some could have underlying CAD, MI, CHF
MI is the most common cause of perioperative death for the geriatric population
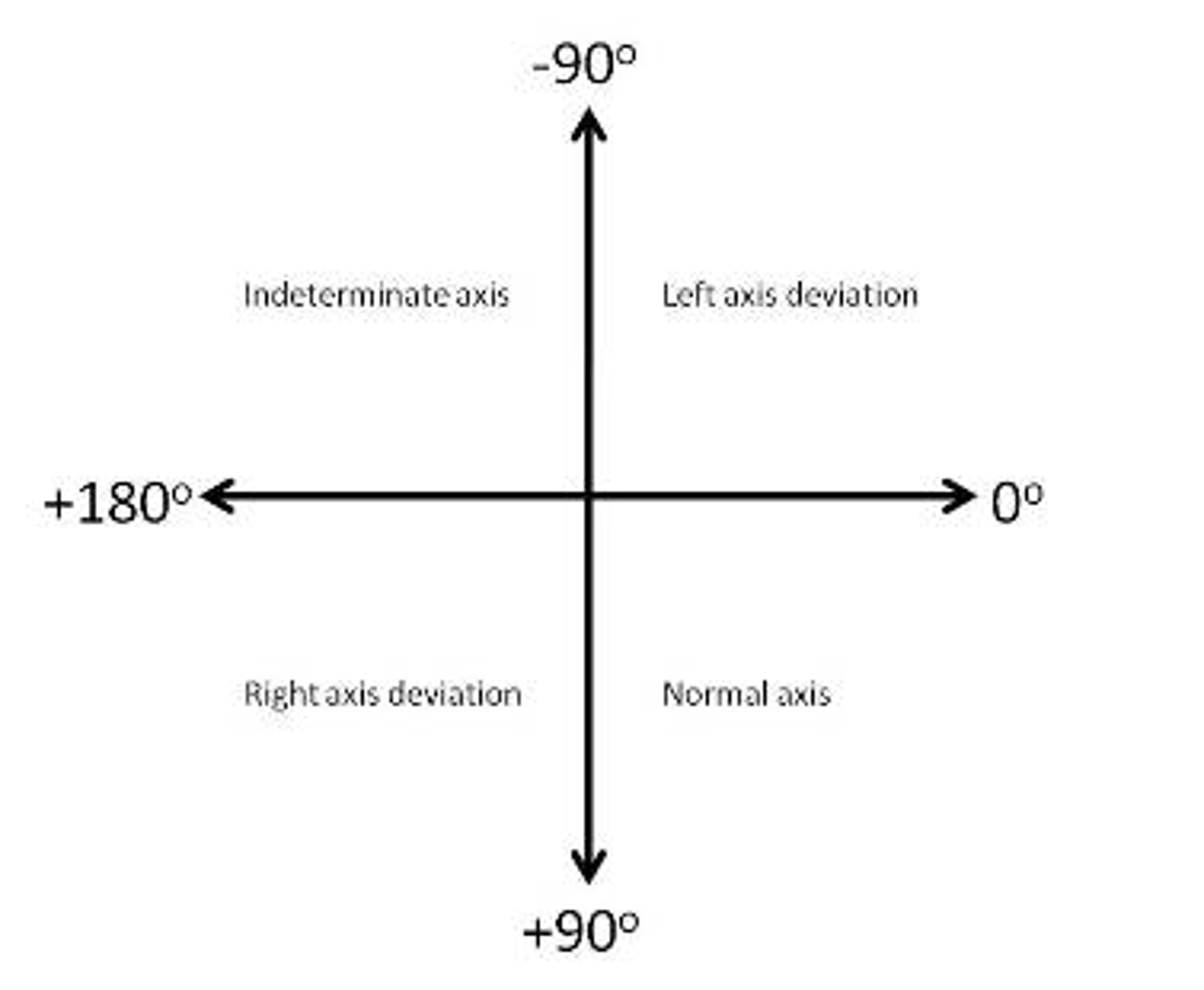
Positive R wave in lead I and negative R wave in lead aVF indicates:
left axis deviation
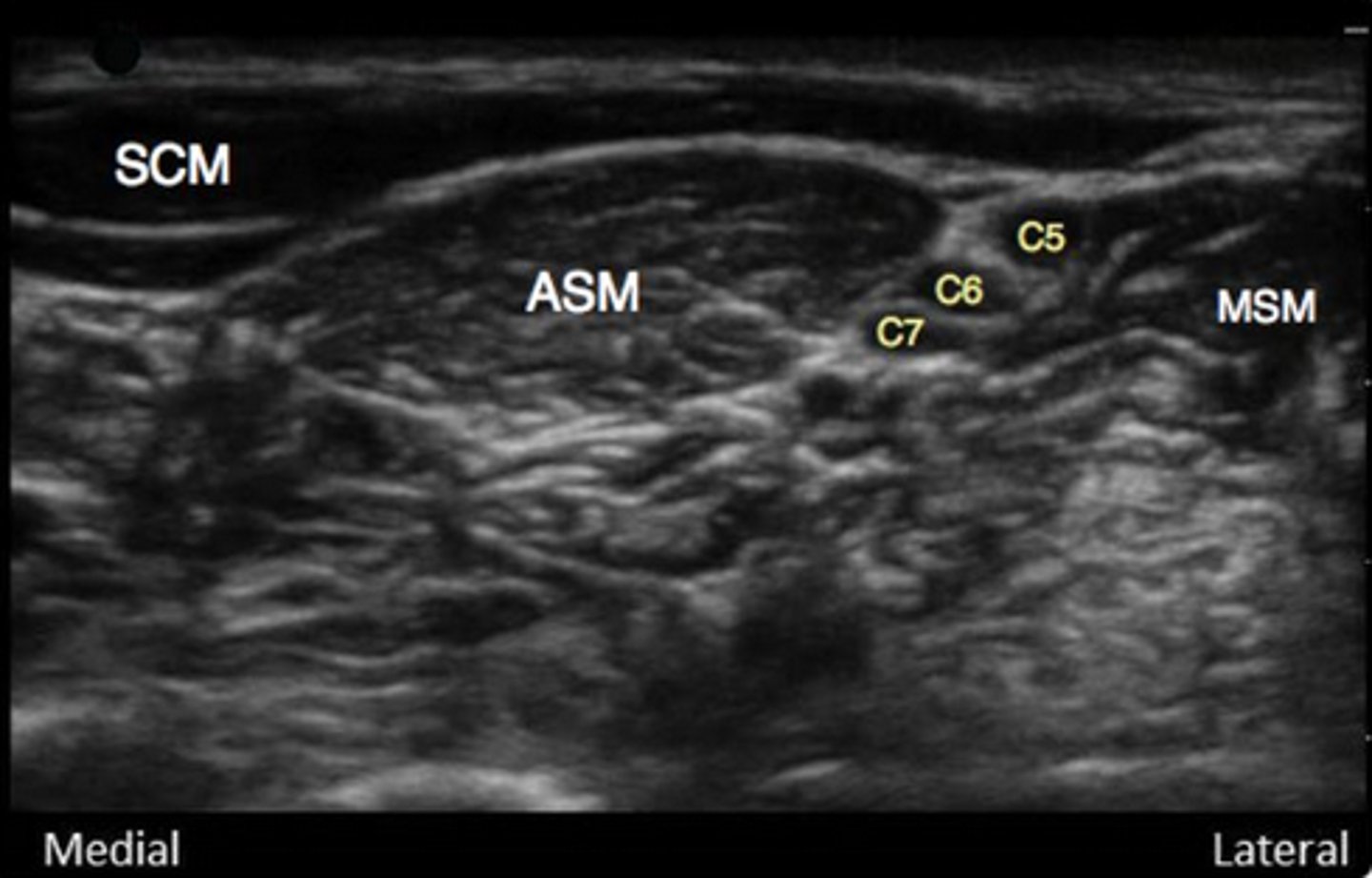
What muscles are landmarks for the interscalene block?
anterior scalene muscle (medial to nerve bundle)
middle scalene muscle (lateral to nerve bundle)
sternocleidomastoid (above ASM and nerve bundle)
What nerves can get damaged from improper lithotomy positioning?
common peroneal - lateral side of leg against stirrups
saphenous- medial side of leg against stirrups
What is the major building block for all steroidal hormones?
cholesterol
needed for synthesis of mineralcorticoids, glucocorticoids and androgens)
What are the 3 best techniques to avoid postop cognitive dysfunction in the elderly?
1. use short acting/ rapidly metabolized drugs (remi)
2. avoid drugs that cross BBB
3. use inhalation agents over IV agents if possible
Which volatile is most likely to cause a circuit fire? (incidence is still extremely rare...)
Sevoflurane
Aneurysm classifications: what part of the aorta is involved in each?
Which ones are likely to cause Aortic Insufficiency?
DeBakey type 1, 2, 3
Stanford type A, B
Crawford type 1, 2, 3, 4, 5
Aneurysms involving ascending Ao can contribute to AI (DeBakey type 1 and 2 and Stanford type A)
DeBakey:
-type 1: ascending and descending Ao involved
-type 2: ascending Ao involved
-type 3: descending Ao involved
Stanford:
-type A: ascending Ao +/- descending Ao
-type B: descending Ao only
Crawford: types 1-5 involves descending Ao and thoracoabdominal Ao only
During shoulder surgery in the beach chair position, MAP in the arm is measuring to be 60 mmHg. The external auditory meatus is 14 inches higher than the arm where the cuff is taking pressures. What is the MAP at the Circle of Willis?
for every inch above the heart, the real MAP is 2 mmHg below what the monitor is reading
for every inch below the heart, the real MAP is 2 mmHg above what the monitor is reading
MAP at the Circle of Willis= 32 (60- (2*14))
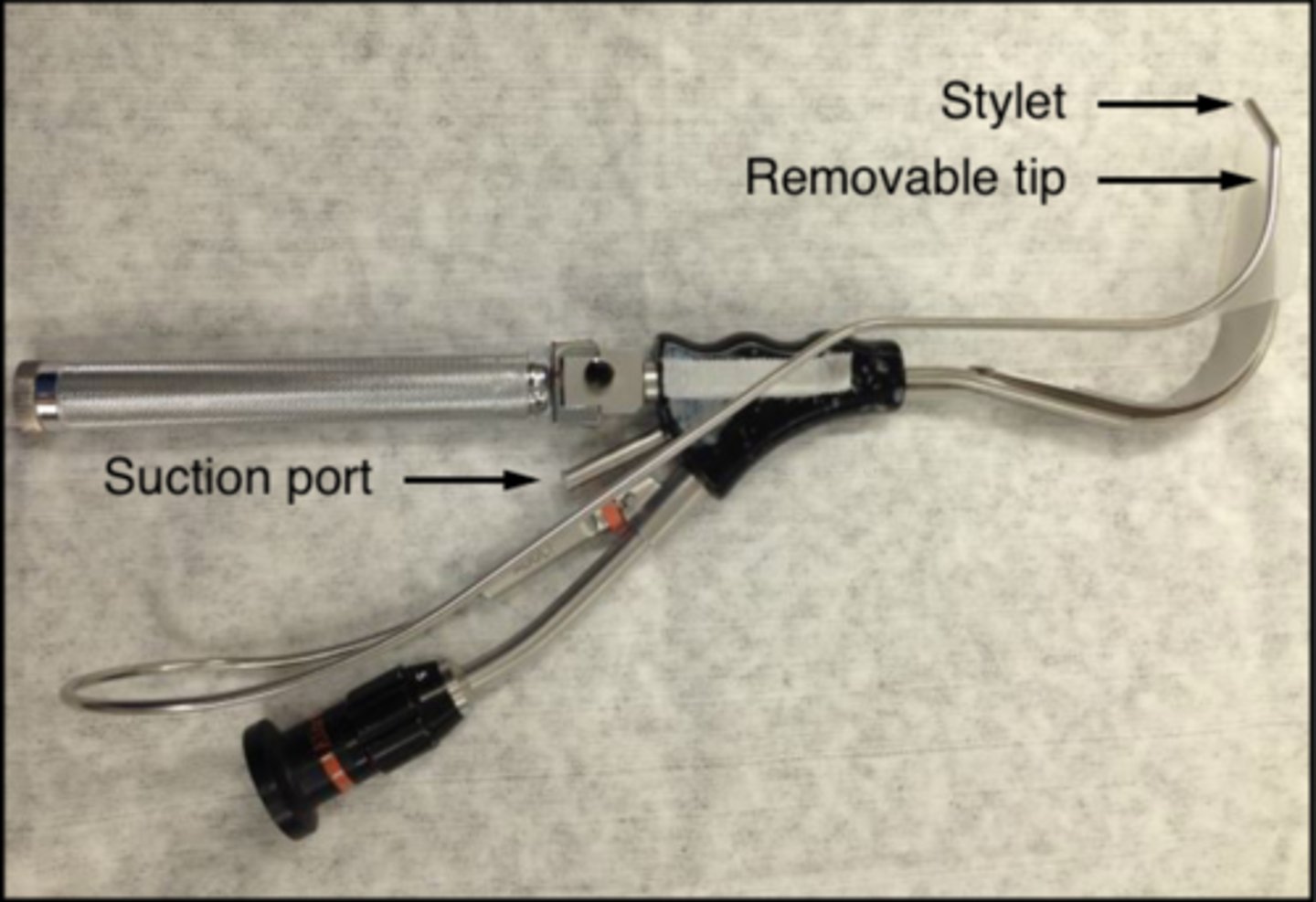
What scenarios indicate the use of a Bullard Laryngoscope?
If the tube gets hung up, what can you do?
Anything that requires indirect laryngoscopy, examples:
1. small mouth opening
2. unstable C-spine
The stylet and ETT sit to the right of the blade. If it gets hung up around the glottic opening, apply cricoid pressure or try lifting the blade anteriorly to get the tube to pass.
What valvular disorder is commonly associated with akylosing spondylitis?
Aortic insufficiency
listen for a diastolic murmur on the left substernal border
match the following diagnoses to their characteristic hemodynamic data:
Pulmonary HTN, RV failure, LV failure, hypovolemia
1. decreased CVP, decreased PADP, decreased PAOP
2. normal CVP, increased PADP, increased PAOP
3. increased CVP, normal PADP, normal PAOP
4. increased CVP, increased PADP, normal PAOP
According to Nagelhout: PADP is an estimate of PAOP (except in cases where PVR is increased like pHTN, then PADP> PAOP) and PAOP is an estimate of LAP which is an estimate of LVEDP
hypovolemia: decr CVP, decr PADP, decr PAOP
pHTN: incr CVP, incr PADP, normal PAOP
RV failure: incr CVP, normal PADP, normal PAOP
LV failure: normal CVP, incr PADP, incr PAOP
When performing a jaw thrust, what structures are displaced anteriorly?
Displaced anteriorly:
-Mandible
-Epiglottis
-Hyoid bone
-Supporting tissues
The mastoid process (posterior border of the laryngospasm notch) is fixed and does not move with the mandible
According to the SCIP, all antibiotics must be started within ____ of surgical incision. The only exception is vancomycin, which gets started within ___ of surgical incision.
All ABX must be started within 60 min/1 hour of incision
Vanc must be started within 120 min/2 hours of incision
What are the mortality rates related to ASA status per 10,000 anesthetic cases?
ASA 1= 0.04 deaths per 10,000
ASA 2= 0.5 deaths per 10,000
ASA 3= 2.7 deaths per 10,000
ASA 4= 5.5 deaths per 10,000
Considerations for a patient undergoing a mastectomy with sentinel node biopsy.
1. Where is the most common site of metastasis for breast cancer?
2. What electrolyte imbalance may be seen in cancer patients?
3. What monitor reading may be incorrect?
1. breast ca most commonly mets to bone
2. hypercalcemia d/t osteoclastic break down of bone
3. SpO2 may read falsely low if dye was injected during the sentinel node biopsy
DO NOT PARALYZE THESE PATIENTS
Which of the following conditions will increase the release of Ach from the presynaptic Nn onto the NMJ?
a) hyponatremia
b) hypomagnesemia
c) hypocalcemia
d) hypokalemia
b) hypomagnesemia
Mg is a Ca antagonist- you need Ca to enter the presynaptic nerve in order for the nerve to release Ach onto the motor end plate. If you have low Mg, you have high Ca, which would increase the release of Ach
What is the earliest sign of MH under GA? What other early s/sx present with MH?
What are the later s/sx of MH?
What is the first sign of MH in the spontaneously ventilating patient receiving a volatile?
Under GA:
earliest sign: increased ETCO2
other early s/x: tachycardia, masseter muscle spasm
later s/sx: hyperthermia, rhabdomyolysis (cola colored urine), DIC
SV patient:
first sign: tachypnea (as evidence by increased MV--> increased RR and TV)
What is the initial dantrolene dose for MH treatment?
What class of medications should be avoided in the MH patient?
2.5 mg/kg IV
AVOID CCB
What will happen to the neuromuscular blockade if the patient receives a -mycin antibiotic? (neomycin, clindamycin, gentamycin...)
Non-depolarizing block will be increased/decreased?
Depolarizing block will be increased/decreased?
-mycin ABX prolong your NMBD duration
Increase in both the non-depolarizing block, and the depolarizing block
What SE of succinylcholine can be attenuated with a pretreatment of NDMR? (pick 2)
a) massester spasm
b) myalgia
c) serum potassium
d) intracranial pressure
attenuated= decreased effect
b, d
fasiculations can cause myalgia and increased ICP/IOP so giving a de-fasiculating dose of NDMR will decrease myalgia and ICP
massester muscle spasm and serum K levels are not attenuated by a de-fasiculating dose
What effects does neuraxial anesthesia have on a patient's glucose?
reduced surgical stress response from neuraxial anesthesia reduces circulating epinephrine which reduces glucose metabolism in the following ways:
1. decreases gluconeogenesis
2. increases glucose sensitivity
3. improves body's glucose utilization
4. improves post op glucose tolerance
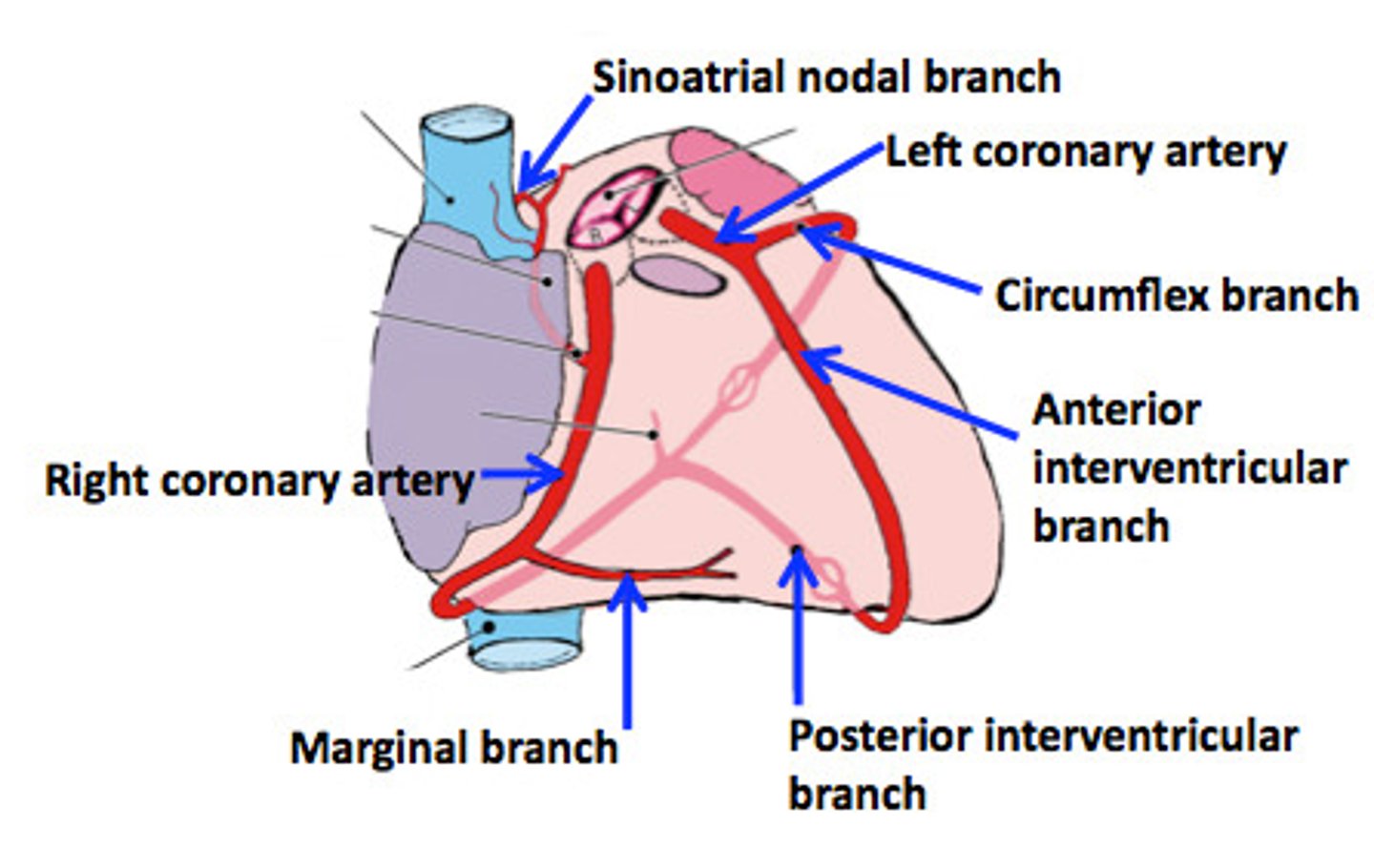
What do the right and left coronary arteries give rise to?
RCA gives rise to:
1. marginal artery
2. posterior descending artery (PDA)
LCA gives rise to:
1. circumflex artery (LCx)
2. anterior descending artery (LAD) (aka interventricular artery)
3. diagonal artery
Calculate FiO2 delivered to a patient wearing a nasal cannula at:
1 L/min
2 L/min
3 L/min
4 L/min
what is the max FiO2 that can be delivered with a nasal cannula?
room air= 21%; after each liter above 1 L/min, you add 4
1 L/min= 24%
2 L/min= 28%
3 L/min= 32%
4 L/min= 36%
max is 6 L/min which delivers 44% FiO2