260 Exam #2 Study Guide
1/120
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
121 Terms
Anxiety
emotional response to anticipation of danger, NOT the same as stress
subjective/normal response that helps people cope with threatening situations
beneficial warning system for survival
problematic when it becomes disabling and functioning becomes adversely affected
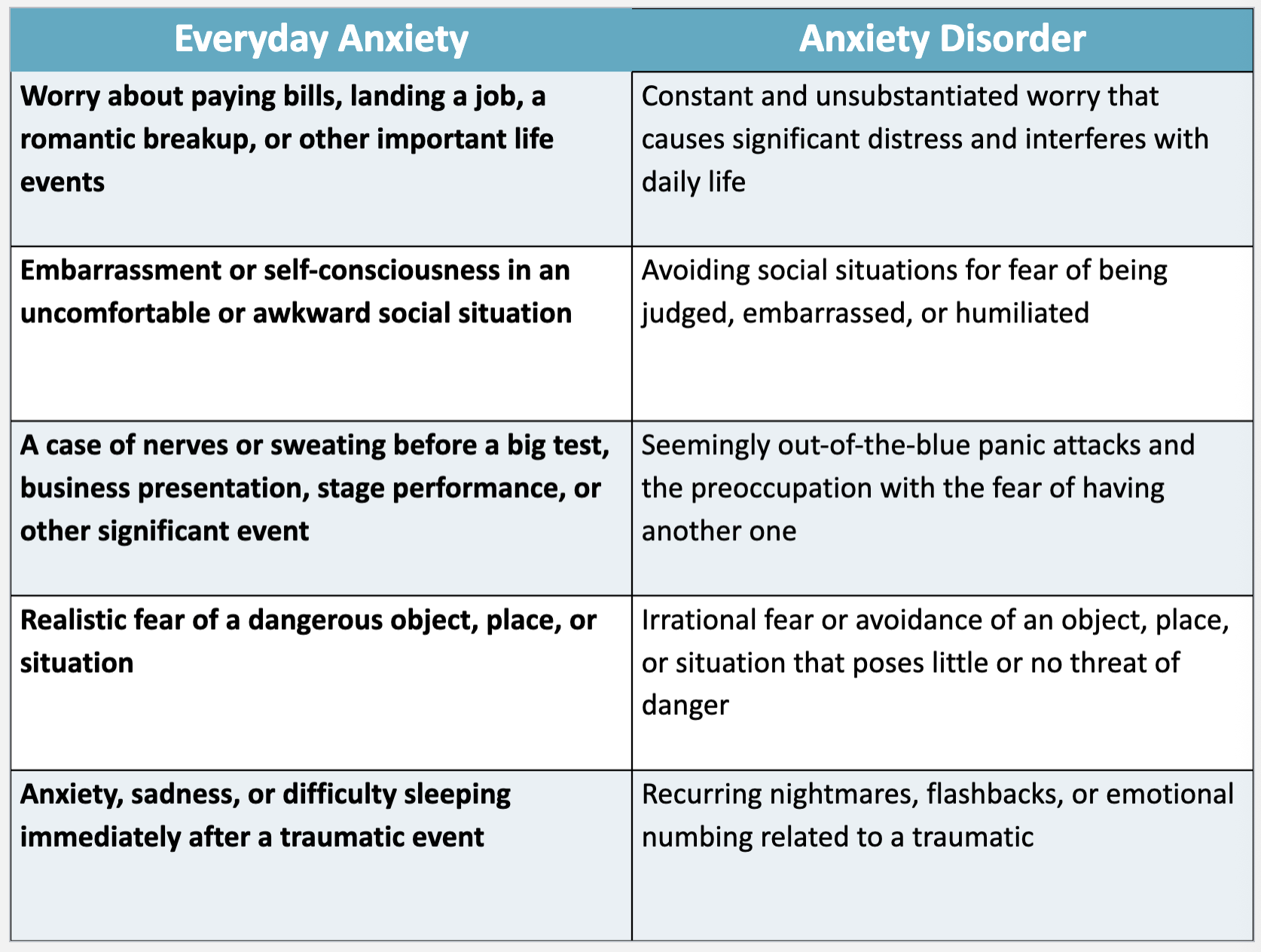
Everyday Anxiety vs. Anxiety Disorder
Anxiety Disorders
Generalized Anxiety Disorder (GAD)
Panic Disorder
Agoraphobia
Social Anxiety Disorder
Separation Anxiety Disorder
Phobias
Generalized Anxiety Disorder
DSM 5 Criteria:
the presence of excessive anxiety and worry about a variety of topics, events, or activities
worry occurs more often than not for at least 6 months
worry in both adults and children may easily shift from one topic to another
accompanied by at least three or more of the following physical or cognitive symptoms (only one required for children): edginess or restlessness, tiring easily or more fatigued than usual, impaired concentration or feeling as though the mind goes blank, irritability (which may or may not be observable to others), difficulty sleeping
patients often become: indecisive, irritable, and lose motivation to participate in life
can cause many issues in relationships and family support systems
Defense Mechanisms
serve to help the patient subconsciously distance themselves from unwanted feelings and prevent new unwanted ones from forming
tension reduction is the overall goal of defense mechanisms because it is a protective mechanism
Recovery
the patient must explore and acknowledge their feelings rather than displace or ignore them
Panic Disorder
DSM 5 Criteria:
characterized by a discrete period of intense fear or discomfort in which at least 4 of 13 symptoms develop abruptly and reach a peak within 10 minutes
palpitations (pounding heart or accelerated hear rate), sweating, trembling, shaking, sensations of SOB or smothering, feelings of choking, chest pain or discomfort, nausea or abdominal discomfort, feeling dizzy, unsteady, or lighthearted, de-realization (feelings of unreality) or depersonalization (being detached from oneself), fear of losing control or going crazy, fear of dying, parasthesias, chills or hot flashes
Phobias
an irrational and disproportionate fear of an object or situation
person is generally aware that the fear is unreasonable and excessive
these clients have overwhelming symptoms of panic when exposed to the phobic stimulus. if the stimulus is removed, the anxiety goes away.
sudden onset which may occur in situations that previously did not cause any discomfort or anxiety
diagnosis made only if avoidant behavior causes problems in functioning (occupational or social relationships) or if pt. is distressed about having the fear
Specific Phobia
fear of a specific object
Social Phobia
fear of being scrutinized by others or fears of being humiliated (evaluated by others)
Agoraphobia
with panic
without panic
Physical Symptoms of Phobias
overwhelming feelings of anxiety, panic attacks (frightening without warning), sweating trembling, hot flushes or chills, shortness of breath or difficulty breathing, a choking sensation, rapid heartbeat (tachycardia)
pain or tightness in the chest, a sensation of butterflies in the stomach, nausea, headaches, dizziness, feeling faint, numbness or pins and needles, dry mouth, a need to go to the toilet, a ringing in your ears
Psychological Symptoms of Phobias
confusion or disorientation, fear of losing control, fear of fainting, feelings of dread, fear of dying
Assessing Anxiety - Recognizing Cues
assess and acknowledge presence of anxiety (behavioral and somatic symptoms)
assess patient’s perception of the situation
evaluate psychosocial stressors, and developmental issues
assess for suicidal ideation, intent and/or plan
conduct head-to-toe (identify cues and vital signs)
explore history of mental illness or substance use
assess patient’s ability to focus and concentrate
observe and assess patient’s speech
assess current coping mechanisms
request labs, including thyroid function, blood glucose, echo, tox screen
GAD-7 screening tool
Assessment
Review past medical history
Many medical disorders present with anxiety as a primary symptom
Angina and myocardial infarction (eg, dyspnea, chest pain, palpitations, diaphoresis)
Cardiac dysrhythmias (palpitations, dyspnea, syncope)
Mitral valve prolapse
Pulmonary embolus (dyspnea, hyperpnea, chest pain)
Asthma (dyspnea, wheezing)
Hyperthyroidism (palpitations, diaphoresis, tachycardia, heat intolerance)
Hypoglycemia
Pheochromocytoma (headache, diaphoresis, hypertension)
Hypoparathyroidism (muscle cramps, paresthesia's)
Transient ischemic attacks (TIAs)
Seizure disorders
Defense Mechanisms
the way individuals seeks to reduce anxiety
it is a protective mechanism
overall goal is tension reduction
recognize
don’t try to eliminate
conversion, compensation, denial, displacement, identification, idealization, intellectualization, introjection, isolation, projection, rationalization, reaction formation, regression, repression, splitting, sublimation, suppression, undoing
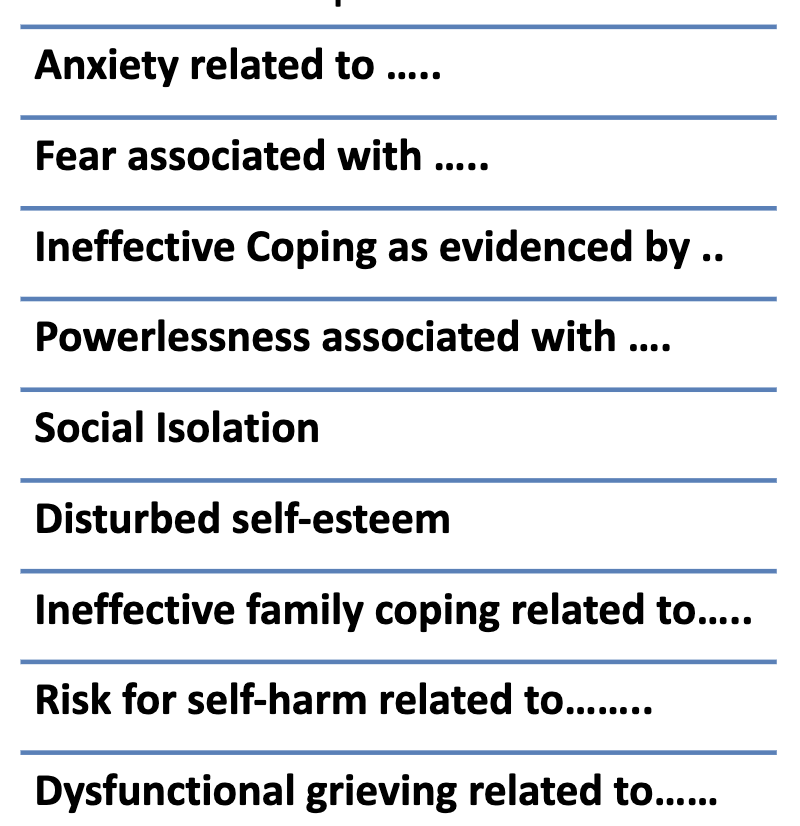
Diagnosis/Analysis
review data, determine what they mean or identify potential complications for which the individual is at risk
Nursing Interventions for GAD
actively listen to the individual and encourage exploration of feelings
reassure the individual about their safety
validate their feelings and concerns
help acknowledge anxiety rather than deny or intellectualize it
assist in identifying behaviors that indicate individual is feeling anxious
assist individual with connecting anxiety with uncomfortable physical, emotional, or behavioral responses
discourage use of caffeine, nicotine, or alcohol to cope with anxiety
Nursing Interventions for Panic Attack
recognize signs, remain calm, stay with individual, don’t make assumptions, speak in short sentences, avoid saying “don’t worry”
be predictable, teach breathing techniques, do not touch individual unless invited to do so
Nursing Interventions for Phobias
psychotherapy: individual talk therapy, CBT
medication: benzodiazepines (episodic) → xanax for social phobias, beta blockers, SSRIs
behavioral: systematic desensitization → creation of graduate exposure to fear stimuli, encouraged to refrain from using avoidance response, implosion → bombarding or flooding the pt. with an exaggerated version of the phobic stimuli
education: explore the concept that phobias are learned behaviors that can be unlearned an discuss how new behaviors can be learned
Goals & Outcome Criteria for Phobias
The patient will:
acknowledge and discuss fears and concerns
verbalize feelings of anxiety and present ideas for how to manage those feelings
recognize signs of escalating anxiety and intervene before reaching panic level
function adaptively in the presence of the phobic object or situation without experiencing panic anxiety (phobic disorder)
verbalize a plan of action for responding in the presence of the object or situation without developing panic anxiety (phobic disorder)
Coping Strategies
a process used by individuals to manage anxiety
general life management strategies: time management, nutrition, exercise, sleep
problem focused coping: work to eliminate or change the source of anxiety
emotional focused coping: reinterpreting the meaning for the situation
Cognitive Behavioral Therapy
premise: “how people think significantly influences their feelings and behavior.”
short term, highly structured, goal oriented
3 components: didactic/educational, cognitive techniques, behavioral interventions
Focus (teaching)
the relationship between illness and distorted thinking patterns
helps individualize recognize their negative thoughts
using cognitive and behavioral techniques to assist the individual in modifying the dysfunctional patterns
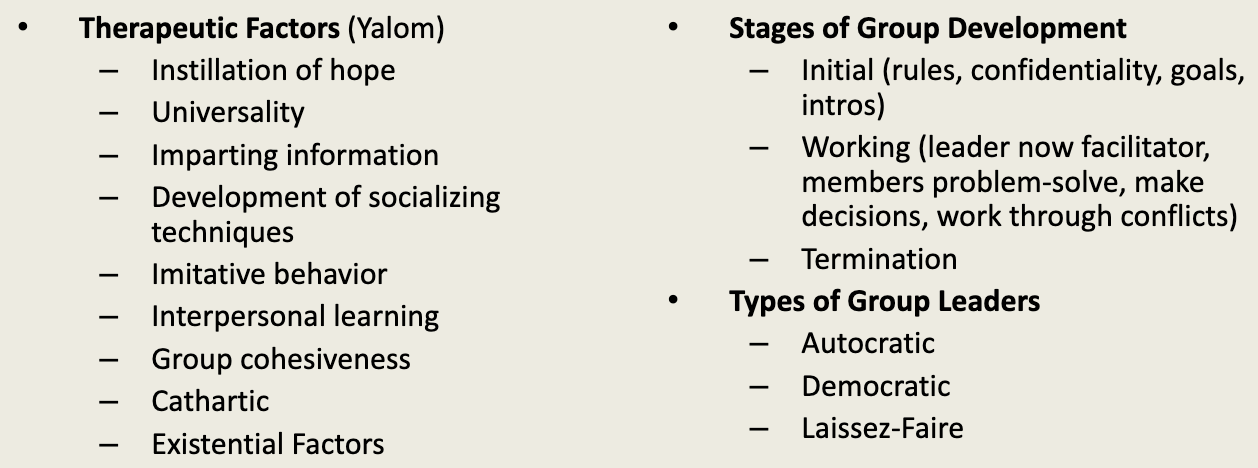
Group Therapy
a form of psychosocial treatment in which several clients meet together with a therapist for purposes of sharing, gaining personal insight, and improving interpersonal coping strategies
Medications Used to Treat Anxiety
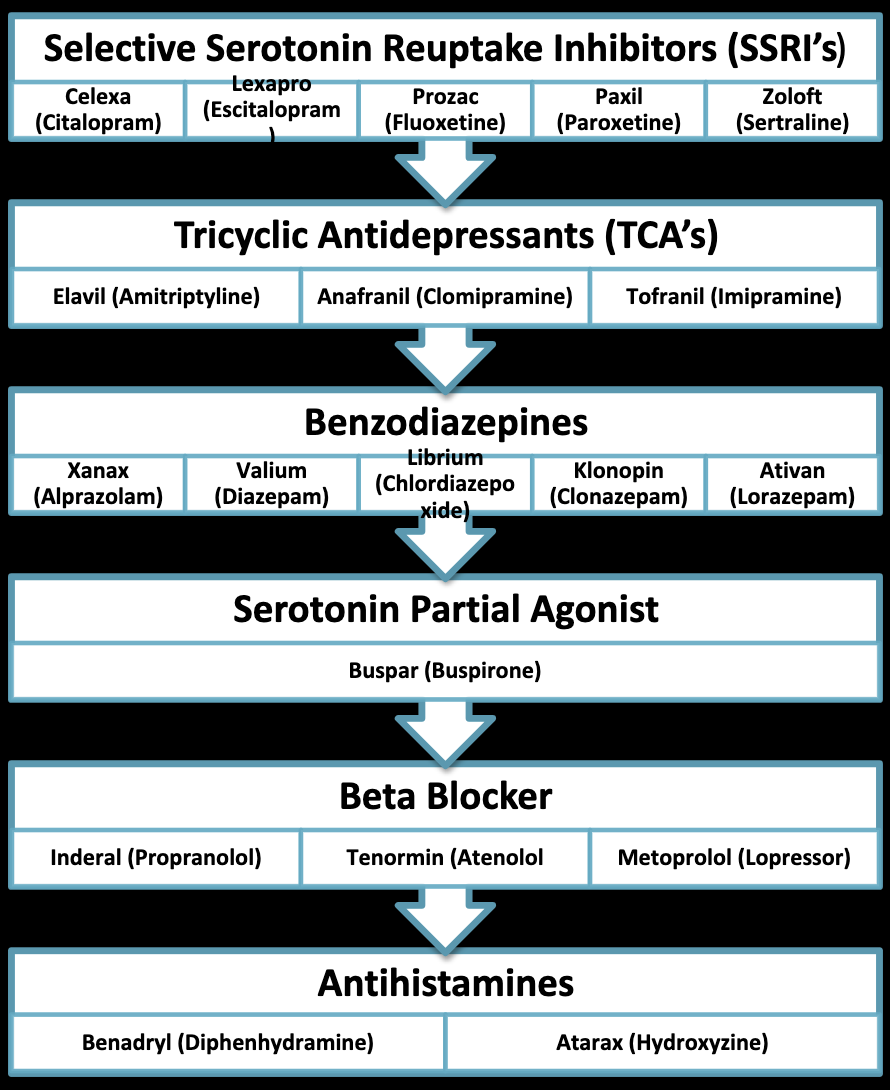
antidepressants, anxiolytics, MAOIs, beta blockers, alpha-2 agonists, antihistimines
Antidepressants (first line of treatment for anxiety disorders)
Indication: MDD and anxiety disorders
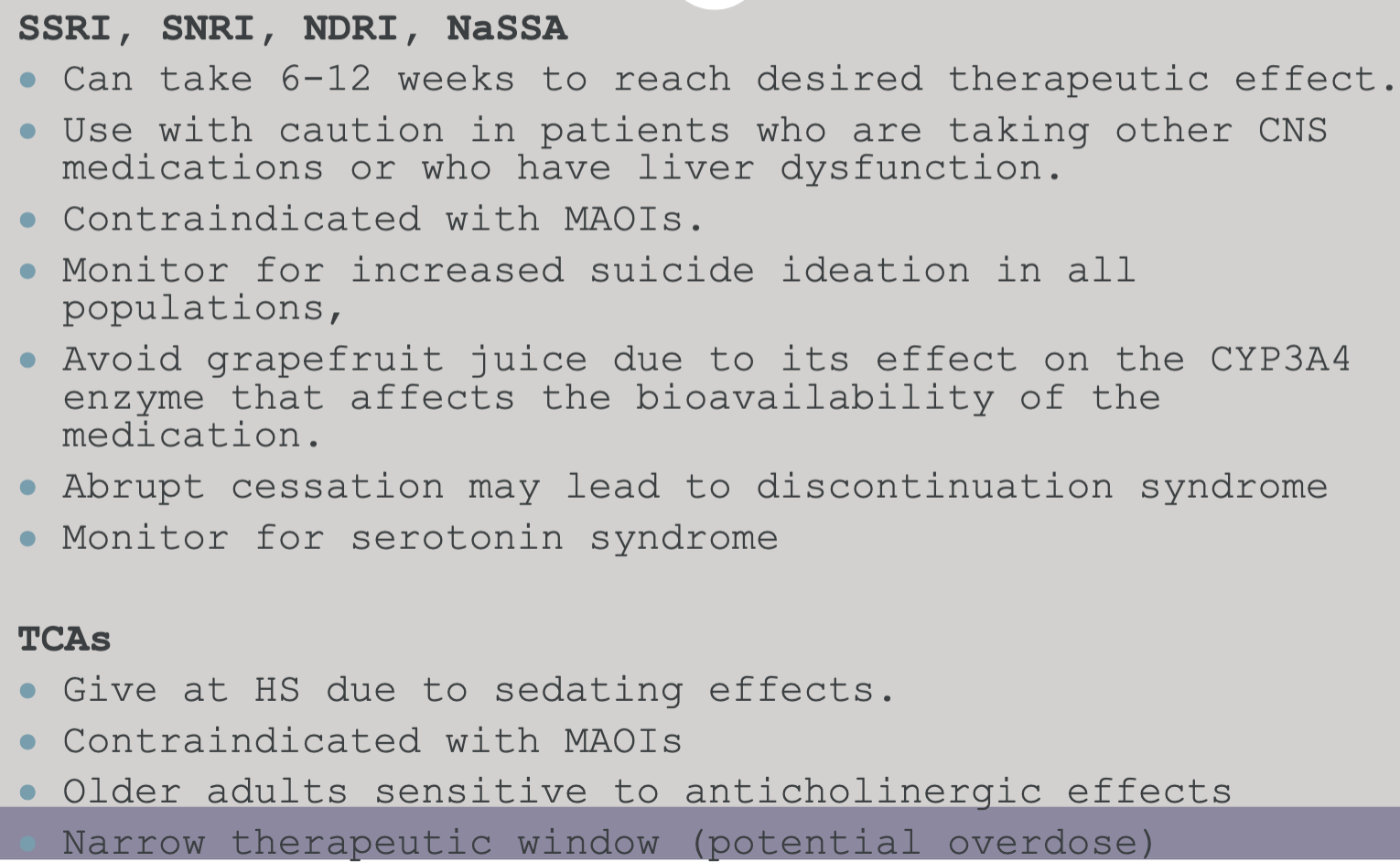
Course of Treatment: 6-9 months, taper off if symptom free, relapse = more maintenance, does not usually develop tolerance, addiction, psychological dependence, or long term adverse effects
SSRIs
serotonin and norepinephrine help regulate mood and anxiety
all SSRIs inhibit the reuptake of serotonin at the presynaptic membrane → increase of available serotonin in the synapse and at the post-synaptic receptors, promoting serotonin neurotransmission
SNRI: Venlafaxine (Effexor)
SNRI: Venlafaxine (Effexor)
Mechanism of Action: inhibits the reuptake of the serotonin and norepinephrine, resulting in an increase in the extracellular concentrations of serotonin an norepinephrine (better for pain control and increased energy)
Side Effects: dizziness, headache, insomnia, nausea, diarrhea, palpitations, increased blood pressure, dry mouth, and sexual dysfunction
NsSSA (Noradrenergic and specific Serotonin Antidepressant): Mirtazapine (Remeron)
Medication: Mirtazapine (Remeron)
Mechanism of Action: increase norepinephrine and specific serotonin neurotransmission without inhibiting reuptake (provide better sedation, less sexual dysfunction), used when patient cannot tolerate S/S of other meds
Side Effects: dizziness, sedation, weight gain, increased appetite
NDRI: Wellbutrin (Bupropion)
Medication: Wellbutrin (Bupropion)
Mechanism of Action: enhances monoaminergic neurotransmission by reducing the reuptake of dopamine and norepinephrine increasing extracellular dopamine and norepinephrine concentrations
Side Effects: tremors, dizziness, headache, insomnia, lowers the seizure threshold, nausea, dry mouth, tachycardia, diaphoresis, dry mouth
TCAs
Mediations: amitriptyline (elavil) and imipramine (tofranil)
Mechanism of Action: works by raising the levels of serotonin and norepinephrine by slowing the rate of reuptake (reabsorption) by nerve cells
Side Effects: dizziness, tremors, constipation, nausea, vomiting, weight gain, postural hypotension, tachycardia, prolonged qt interval, dry mouth blurred vision, lethal in overdoes
Nursing Implications for Antidepressants
Benzodiazepines
Mechanism of Actions: increases the efficiency of GABA to decrease the excitability of neurons, blocking the release of stress hormones (cortisol) associated with anxiety and panic. → reduces the communication between neurons and therefore has a calming effect on many of the functions of the brain especially the limbic system.
most commonly used anti-anxiety (anxiolytic drugs) that act through the CNS and have muscle relaxation, sedative, anxiolytic and anticonvulsant effects → wide safety margin, rapid onset, cause dose-related suppression of the CNS, varying from slight impairment to hypnosis
Clinical Use: anxiety, panic, alcohol withdrawal, skeletal relaxation, dental procedures, insomnia, substance-induced agitation
Short Acting Benzodiazepines
short-acting metabolites
not used for anxiety
median half life of less than 6 hours
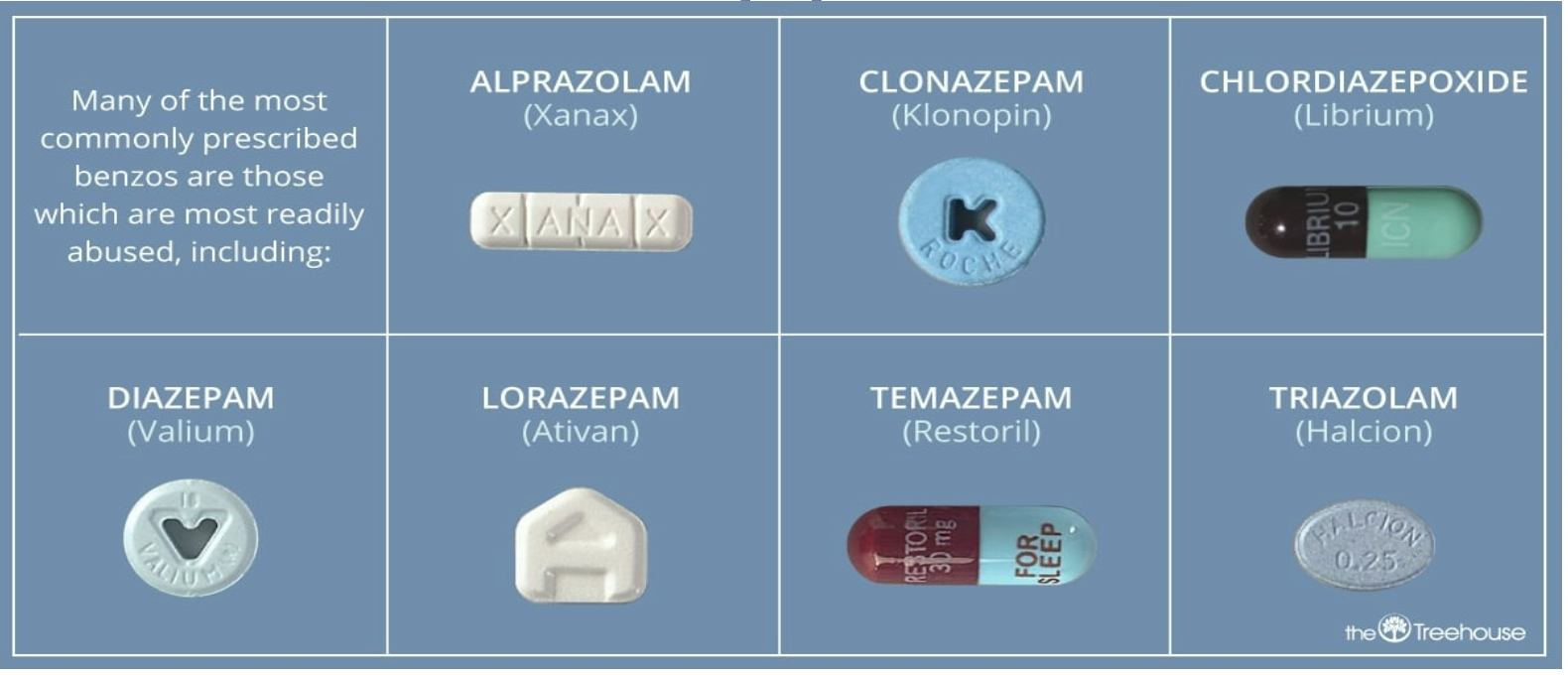
Medication: versed (midazolam) and halcion (triazolam)
Long Acting Benzodiazepines
Medications: librium (chlordiazepoxide), valium (diazepam), xanax (alprazolam), klonopin (clonazepam), ativan (lorazepam)
used in conjunction with antidepressants in the treatment of panic
fast acting with acute symptoms of panic (racing pulse, and SOB) but long enough to control residual anxiety and worry about future panic episodes
rate of absorption varies
important to know half-life
treatment should be brief
highly addictive
Alprazolam (Xanax)
fast-intermediate → 12-15 hours
Lorazepam (Ativan)
intermediate → 12-20 hours
Chlordiazepoxide (Librium)
intermediate → 8-28 hours
Diazepam (Valium)
fast → 20-80 hours
Clonazepam (Klonopin)
slow → 18-50 hours
Side Effects of Benzodiazepines
drowsiness, sedation, confusion, ataxia, respiratory depression, increased irritability, tolerance, dependency, rebound insomnia, anxiety
overdose → slurred speech and memory problems
Benzodiazepine Withdrawal Syndrome → potentially life-threatening!
do not suddenly stop
withdrawals begin 6-8 hours after last dose of short acting benzos, and within 24-48 hours after last dose of long acting benzos
more common with higher doses of short acting benzos
alcohol/sedatives increase the risk of dependence
high dose withdrawals can lead to psychosis, altered mental status, seizures, and status epilepticus
moderate dose withdrawals can lead to rebound anxiety and insomnia
Treatment of Withdrawal Syndrome
gradual titration (7 days to 3 months)
replacement therapy → use same or a longer acting benzo to taper and/or adjunctive (barbiturates and/or anticonvulsants) to mitigate withdrawal symptoms
shorter acting → intense, serious and life-threatening symptoms (Xanax)
Longer acting: less intense symptoms (Valium, Klonopin, Librium)
withdrawal symptoms highly variable based on the type, amount, duration, tolerance, half-life
Benzodiazepine Withdrawal Syndrome Symptoms
agitation, anorexia, rebound anxiety, generalized seizures, psychosis (hallucinations)
diaphoresis, autoimmune arousal, dizziness, hyperactivity, irritability, n/v, sensitivity to light, tinnitus, tremulousness
Nursing Implications for Benzodiazepines
there is a significant risk of dependence → ordered for short time periods
dangerous in overdose, especially with alcohol
severe withdrawal symptoms if abruptly withdrawn
Warnings!
CNS depressant → don’t operate machinery or drive, dangerous with alchol,
Glaucoma → do not use with people with glaucoma unless they are receiving appropriate anti-glaucoma therapy
Pregnancy → don’t use when pregnant or breastfeeding
elderly are more vulnerable to side effects ½ to 1/3 of dose
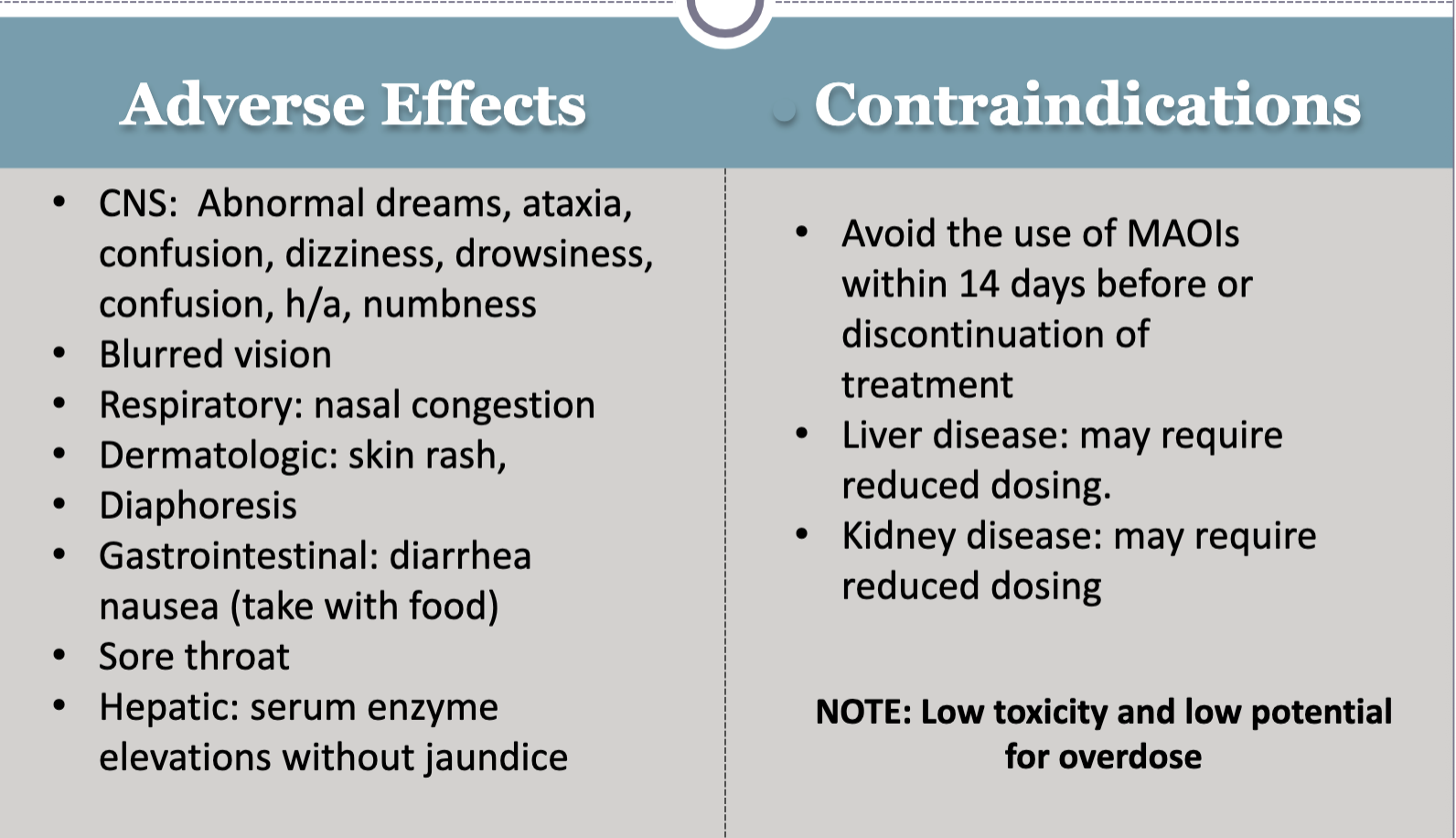
Buspirone (Non-Benzodiazepine)
initially developed as an anti-psychotic but was not effective → not used for withdrawal or panic
binds to serotonin and dopamine receptors (partial agonist) → has no effect on gaba
no CNS depression or potential for abuse, dependence, tolerance, or potentiation with alcohol
may have paradoxical effects (anxiety, depression, insomnia)
slow onset of action. may not be fully effective for 6-8 weeks
use with caution with individuals with liver or kidney damage
Beta Blockers
Inderal (propranolol)
Atenolol (tenormin)
act by blocking peripheral or central norepinephrine activity and symptoms of anxiety including palpitations, sweating and tremors
used for PTSD & performance anxiety: weakness, fatigue, bradycardia, hypotension, depression
contraindicated in people with asthma and emphysema
Alpha 2 Agonist
Catapres (clonidine)
effective in easing peripheral symptoms associated with opiate and alcohol withdrawal: tremulousness, profuse sweating, motor restlessness, anxiety, agitation
eases insomnia due to sedation effects
side effects: dizziness, drowsiness, postural hypotension, bradycardia, dry mouth
Antihistamines
Benadryl (diphenhydramine)
can be used to reduce anxiety through sedative effects, sometimes used to treat insomnia
will help individual fall asleep, but not stay asleep or prevent early morning wakening
may produce a hangover
A patient has beenprescribed alprazolam(Xanax) and paroxetine(Paxil).
assess for suicidal ideation
monitor sedation level
teach about avoiding alcohol
educated about delayed SSRI effects
evaluate medication adherence
Psychosis
a syndrome of neurocognitive symptoms that impairs cognitive capacity, leading to deficits in perception, functioning, and social relatedness
severe mental condition in which there is disorganization of the personality, deterioration in social functioning, and loss of contact with, or distortion of reality
there may be evidence of hallucinations and delusional thinking
can occur with or without the presence of organic impairment
no specific cause
associated with symptoms of mental illness, sleep deprivation, medical conditions, and prescription medications
Psychotic Disorders
mental health disorders that feature abnormal thinking, perceptions (hallucinations, delusions)
Schizophrenia
one type of psychotic disorder that features psychotic symptoms like hallucinations and delusions, reduced emotional expression, difficulty in social relationships, and motor impairment
a primary psychotic disorder → disturbances in thought processes, perception, and affect resulting in severe deterioration of social and occupational functioning
DSM 5 Criteria for Schizophrenia
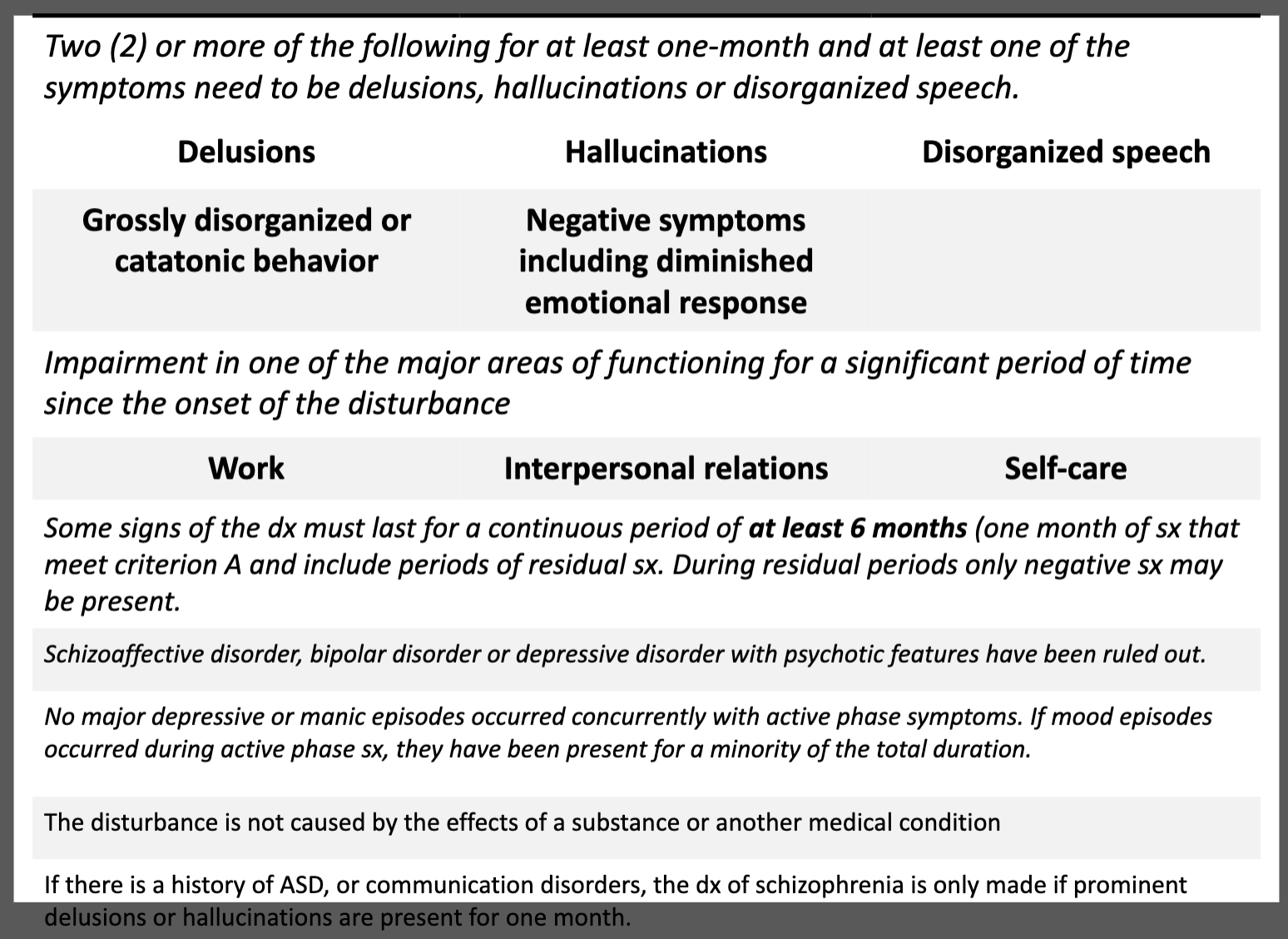
Positive Symptoms of Schizophrenia
additions to a person’s experience (not normally present)
Disturbances in Thought Content: hallucinations, delusions, illusions
Disturbances in Thought Process: disorganized thoughts and speech
Disturbances in Behaviors (4th dimension): erratic, strange, unexpected movements, posturing, waxy flexibility; interpersonal interactions may be unpredictable or inappropriate in social situations.
Negative Symptoms of Schizophrenia
a loss or deficiency in normal functioning
Disturbances in Emotion: affective flattening, anhedonia, avolition (decrease in the ability to initiate or sustain purposeful activities), alogia (poverty of speech), asociality
Cognitive Symptoms (3rd dimension): attention issues, verbal fluency, executive function, decreased ability to understand social situations, memory issues, reasoning
Hallucinations
false sensory perceptions not associated with real external stimuli and may involve any of the five senses
auditory, visual, tactile, gustatory, olfactory
Hallucination Interventions
observe the patient for signs of hallucinations
do not reinforce but validate the hallucination
provide an attitude of acceptance
ask about content
ask if the voices are familiar
distract the patient from the hallucinations
educate: voice dismissal
avoid touching the patient
assess for suicide risk
assess the level of anxiety
Illusions
a perception that occurs when a sensory stimulus is present but incorrectly perceived and misinterpreted, such as hearing the wind as someone crying
Depersonalization
feeling disconnected from one’s body and thoughts
Derealization
alteration in the perception or experience of the external world so that it seems unreal
Delusions
fixed, false beliefs
irrational and cannot be corrected by reasoning, even with evidence to the contrary
beliefs are not explainable as part of the person’s usual religious or cultural precepts
experienced as real
75% of individuals with schizophrenia will experience delusions
can be intertwined with hallucinations and can be further complicated by thought, withdrawal, insertion, control, and broadcasting
Delusion Interventions
most do not realize their delusions are problematic or incorrect, so do not try to talk a person out of their delusional thought process → disputing rationality of delusions isn’t likely to have the intended outcome
pay attention to the emotions the person is expressing and reinforce focus on reality
convey acceptance of the patient’s need for the false belief but indicate that you do not share the belief → the patient must understand that you do not view the idea as real
Disturbance in Thought Process as Manifested through Speech Core of Communication
disorganized or alterations in speech (form/organization)
arises from alterations in though process or how thoughts are connected
the threads are missing and connections are interrupted
ex. loose associations, word salad, tangentiality, circumstantiality, pressured speech, alogia, poverty of speech or distractible speech, clanging
Impaired Communication Interventions
facilitate trust and understanding by maintaining staff assignments
attempt to decode incomprehensible communication patterns by seeking validation and clarification
anticipate and fulfill the patient’s needs until functional communication has been established
orient the patient to reality as required to facilitate restoration of functional communication
call the patient by name
validate those aspects of communication that help differentiate between what is real and not real
Affect (Negative Symptom)
diminished affective response
hypoexpression
inappropriate affect/incongruent affect
emotional tone is incongruent with circumstances
flat affect
mask-like: void of emotional tone
no modulation
Disturbance in Emotion ( Negative Symptoms)
Alexithymia: difficulty naming and describing emotions
Anhedonia: inability or decreased ability to experience pleasure, joy, intimacy, closeness
Anosognosia: lack of awareness of having an illness even though symptoms are obvious to others
Apathy: lack of feelings, emotions, interests, concern, indifference, bland
Avolition: inability to initiate goal directed activity, lack of emotion, neglect ADLs
Anergia: chronic state of lethargy or lack of energy
Impaired Cognition/cognitive Deficit: Memory
memory problems associated with schizophrenia include: forgetfulness, disinterest, difficulty learning new information (when in symptoms), lack of compliance
Impaired Cognition: Attention
The ability to focus on one activity in a sustained, concentrated manner
impairment in ability to pay attention
difficulty completing tasks
difficulty concentrating
easily distracted
auditory hallucinations often distract the individual: problems with attention
Impaired Cognition: Concrete Thinking
tend to place an overemphasis on specific details and literal interpretation of ideas
the answer is literal; the ability to use abstract reasoning is lessened or absent
represents regression to an earlier level of cognitive development
Impaired Cognitions: Decision Making
problems with decision making affects: insight, logic, judgment, decisiveness, planning, ability to carry out decisions, abstract thought
Deterioration of Social Skills
Direct Effects:
deterioration of social skills
inability to communicate coherently
loss of drive and interest (avolition)
poor personal hygiene: deterioration of appearance
paranoia
agitation/aggression
Indirect Effects:
low self-esteem related to poor academic achievement
specific problems in the development of relationships
social inappropriateness
disinterest in recreational activities
inappropriate sexual behavior
stigma related withdrawal by friends, family, and peers
Phases of Schizophrenia
premorbid phase
prodromal phase
acute (active) phase
stabilization phase
residual or recovery phase
Premorbid Phase of Schizophrenia
occurs before clear evidence of illness
may include personality traits and behaviors
shy and withdrawn
poor peer relationships
poor academic performance
asocial behaviors
Prodromal Phase of Schizophrenia
early signs and symptoms indicating an onset of disease → may be barely noticeable
mood swings, anxiety, difficulty sleeping, difficulty concentrating, early signs of memory loss, lack of appetite, fatigue, usually recognized retrospectively but can be seen weeks, months, years before
not experienced by everyone
allows for early initiation of treatment with improved outcomes and decreased functional deficits
Active Phase of Schizophrenia
can start subtlety
symptoms include positive, negative, and affective: hallucinations, delusions, disorganized thinking
thoughts and behaviors become: confusing and frightening to individual and family; bizarre and can no longer be overlooked (ex. staying up all night, incoherent conversations, aggressive acts towards self or others, failing school, isolating)
less and less able to attend to basic personal needs
Stabilization Phase of Schizophrenia
Goal: prevent psychotic relapse and improve level of functioning
symptoms become less acute but remain present
treatment is intense as medication regimes are being established
patient and family trying to adjust to family member having a chronic, long term mental illness
use of substance eliminated (hopefully)
stable patients (patients who are maintained on neuroleptics) have a much lower relapse rate than those who discontinue their medication
rehabilitation/recovery begins
Recovery or Residual Phase of Schizophrenia
Focus of Care: regaining a level of functioning and quality of life that provides a meaningful life
medication is necessary but not a cure
reduce stress because it can exacerbate symptoms
family support and involvement are crucial
educate to anticipate and expect relapse and know how to cope when it does occur
Relapse of Schizophrenia
can occur anytime during treatment/recovery
detrimental but not inevitable
with each relapse, recovery is longer and more difficult
factors triggering relapse: refusal to follow medical regime, impairment in cognition and coping leave patient vulnerable to stressors
limited availability to community resources (public transportation, housing, entry level jobs,)
stigma attack self-concept of patients
family/peer support are vital
Schizophrenia Treatment Goals
targeting symptoms
preventing relapse
increase adaptive functioning
Treatment Options for Schizophrenia
medical, psychological treatment
therapeutic mileu
supportive care
assertive community treatment
Neuroleptic/Antipsychotic Medications
used to treat schizophrenia, schizoaffective disorder, organic brain syndrome with psychosis and delusional disorder, agitation associated with alzheimer’s disease, bipolar disorder, depression with psychotic features, substance-induced psychosis, pdd, tourette’s syndrome
Antipsychotic Medications
Mechanism of Action: blocking dopamine transmission (block D2 receptors)
typical antipsychotics more than atypical antipsychotics
Concern: the anti-dopamine effect is not specific to the mesolimbic and mesocortical tracks associated with schizophrenia; but instead travel to all of the dopamine receptor sites throughout the brain
this results in desirable anti-psychotic effects and creates undesirable and unpleasant side effects i.e. dystonia
Typical → first generation (can cause tardive dyskinesia)
Atypical → second generation (associated with metabolic syndrome)
these do not differ in efficacy but they do differ in their side effect profile
both can cause EPS and dystonia
First Generation (Typical) Antipsychotics
Dopamine Antagonists
Mechanism of Action: blocks dopamine receptors in a number of CNS receptor sites
effective in treating positive symptoms, less effective with negative symptoms
also effective in the treatment of bipolar disorder, acute mania, and agitations
Some meds include: thorazine (chlorpromazine), haldol (haloperidol), prolixin (fluphenazine)
Thorazine (Chlorpromazine)
very first antipsychotic (1950)
develops as an anesthetic, not effective, but had calming effects
supplanted by new antipsychotics due to wide undesirable side effect profiles including:
blocks dopamine and antagonizes acetylcholine, norepinephrine, and histamine receptors causing memory impairment (anticholinergic), hypotension (antiadrenergic), and sedation (anti-histaminergic))
use primarily when sedative effect is desired
Haldol (Haloperidol)
most popular of the FGA’s
frequently used to treat schizophrenia and agitation
for agitation often used with Ativan and Benadryl
also used for delirium in acute care
generally requires IV administration and cardiac monitoring as haldol prolongs the QT interval
less anticholinergic, antihistaminic or antiadrenergic effects, but significant EPS
dystonia, akathisia, parkinsonian, and tardive dyskinesia
Side Effects of First Generation (Typical) Antipsychotic Medications
anticholinergic effects, EPS, agranulocytosis, orthostatic hypotension, tardive dyskinesia, neuroleptic malignant syndrome
agitation, N/V, elevation in prolactin levels, sedations, seizures
Nursing Interventions for Anticholinergic Side Effects

Agranulocytosis
rare and life threatening, with no known etioglogy
neutropenia less than 500
cold symptoms: sore throat, fever, chills
increase heart rate and hypotension
muscle weakness and fatigue
Psychotropic Adverse Effects: Extrapyramidal Symptoms
Definition: neurologic and motor symptoms that occur in the context of anti-psychotic use
Caused by: blocakde of D2 receptros in the basal ganglia; throwing off the normal balnace between acetylcholine and dopamine therby increasing acetylcholine transmission
occur more often with first generation anti-psychotic agents
Akathisia
Caused by the same biologic mechanisms as EPS.
symptoms include: restlessness, movement of body, unable to keep still, movement of feet, discomfort
often mistaken for anxiety or increase in psychotic symptosm: unfortunately also given more psychotropic medications
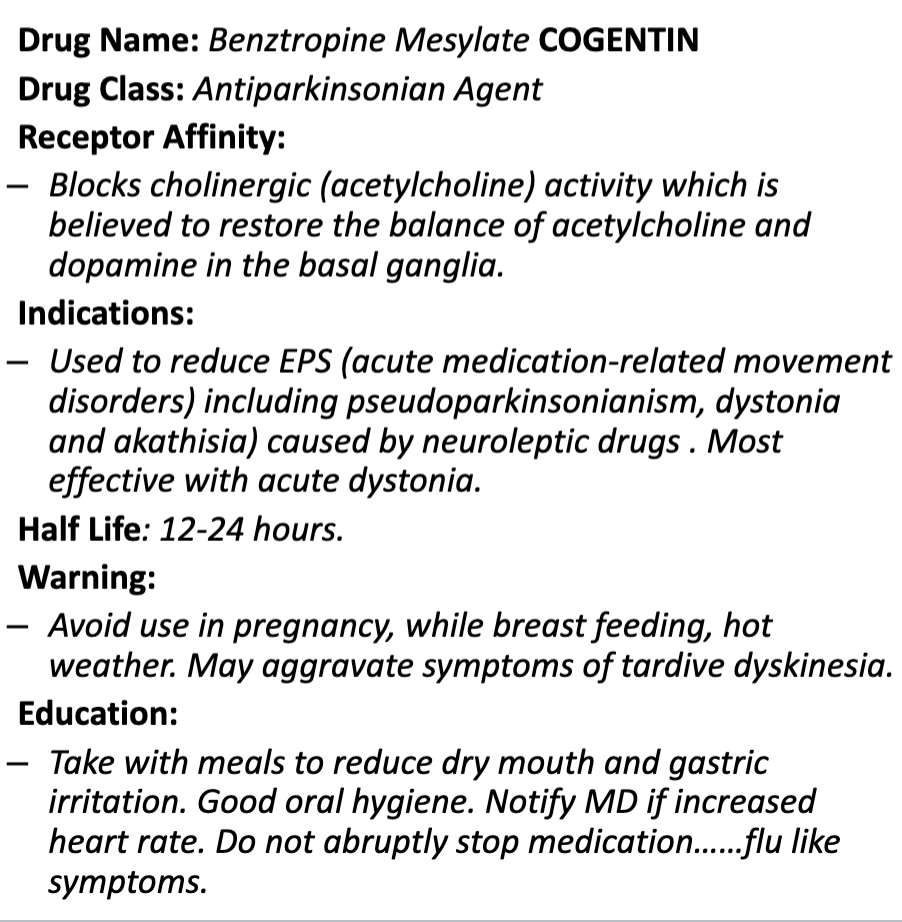
treatment: reduce antipsychotic medication, cogentin, benadryl, benzodiazepine, beta-blocker (comfort measures)
inderal
Akinesia
rigidity, bradykinesia
the inability to perform a clinically perceivable movement
presents as a delayed response, freezing mid-action, or even total abolition of movement
caused by dopamine-blocking medications like antipsychotics
treatment includes switching to atypical antipsychotics with lower risk (e.g., olanzapine) or using anticholinergic
Dystonia
spasmodic and painful spasm of muscle (torticollis)
a neurological movement disorder characterized by involuntary sustained muscle spasm or painful contractions of the face, neck, turnk of limbs
generally, occurs after initiating or increasing antipsychotic medications
caused by a dopamine receptor blockade
young men are most vulnerable to this type of EPS

Treatment of choice for Dystonia: Benztropine (Cogentin) → 1mg-2mg IM, Trihexypenidyl (Artane), Diphenhydramine (Bendadryl) → 25mg-50mg IM
Start daily administration of anticholinergic medications
decrease antipsychotic medication dosage
Pseudoparkinsonism
stimulates Parkinson’s disease with shuffling gait, drooling, muscular rigidity, and tremor
akinesia, badykinesia, cogwheeling, resting hand tremor, drooling, mask-like face, shuffling gait
treatment: lower antipsychotic dose, add anticholinergic, change to atypical antipsychotic agent
Cogentin
Rabbit Syndrome
rapid movement of the lips that stimulates a rabbits mouth movement
Tardive Dyskinesia
caused by the supersensitivity of the dopamine receptors in the basal ganglia
Long Term Effects:
choking (due to loss of control of muscles used for swallowing)
compromised respiratory function (infections, respiratory alkalosis)
neurological syndrome caused by long term use of neuroleptic medications especially first generation
characterized by repetitive, involuntary, purposeless movements: grimacing, tongue protrusion, lip smacking, puckering, and pursing, rapid eye blinking, rapid movement of arms, legs, trunk, fingers
Treatments:
if possible, fully withdraw from medication
switch from a first generation to a second generation antipsychotic with a lower D2 affinity
Clozapine (Clozaril)
Quetiapine (Seroquel)
use the minimum effective dose
minimize the duraton of therapy, consider a VMAT inhibitor (Deutetrabenazine → austedo and Valbenazine → ingrezza) MOA: cause a depletion of neuroactive peptides (like dopamine) in nerve terminals to regulate the amoungt of dopamine flow in the brain areas that control certain kinds of movements
Side effects: drowsiness, depression
Second Generation (Atypical) Antipsychotic Agents
MOA: transiently occupies D2 receptors and then rapidly dissociates to allow normal dopamine neurotransmission (dopamine blockade)
Assists in: keeping prolactin levels normal, spares some cognitive decline/changes, and eliminates EPS
improves positive and negative symptoms of schizophrenia
rarely causes EPS or TD (often cause of pt. non-adherence)
higher cost to patient
potential for metabolic syndrome
take several months to reach maximum efficacy
Medications:
Clozaril (clozapine)
Risperdal (risperidone)
Zyprexa (olanzipine)
Seroquel (quetiapine)
Abilify (aripiprazole)
Common Side Effects of Second Generation (Atypical) Antipsychotic Medications
drowsiness (fatigue, irritability, headache, insomnia), light-headedness, anticholinergic sx (constipation, dry mouth, blurred vision), metabolic syndrome (weight gain, hyperglycemia), QT interval prolongation, orthostatic hypotension
nausea/vomiting, NMS, salivation, hypertension, tachycardia, EPS
black box warning: elderly patients with dementia related psychosis treated with antipsychotic drugs are at an increased risk of death
Atypical Antipsychotic Medication Side Effect: Metabolic Syndrome
glucose dysregulation: new onset DM II or dysregulation of current DM II
lipid disturbance: hyperlipidemia and hypercholesteremia
weight gain: increased food intake, increased visceral fat, reduced motor activity
olanzipine and clozapine have the highest metabolic risk
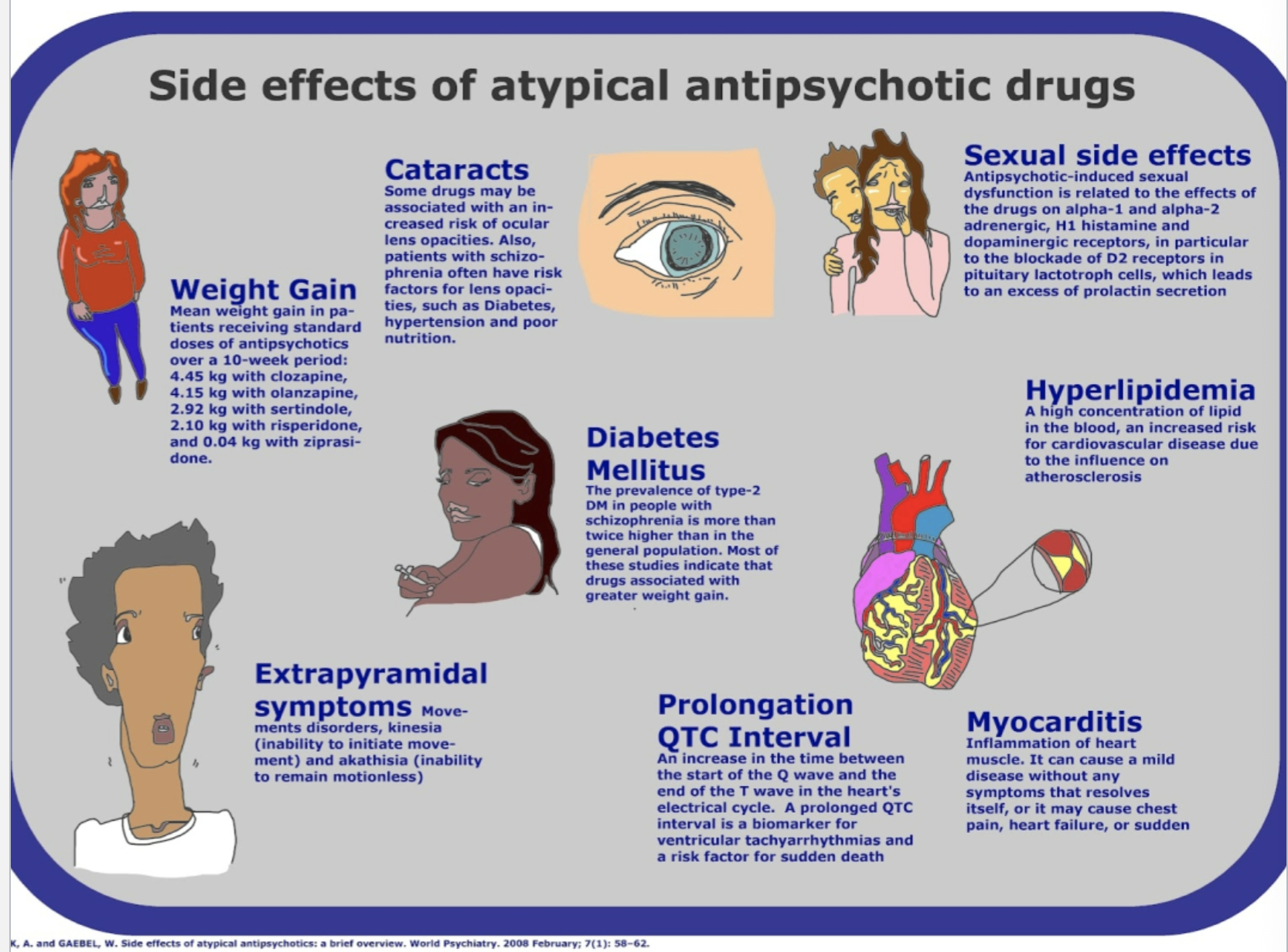
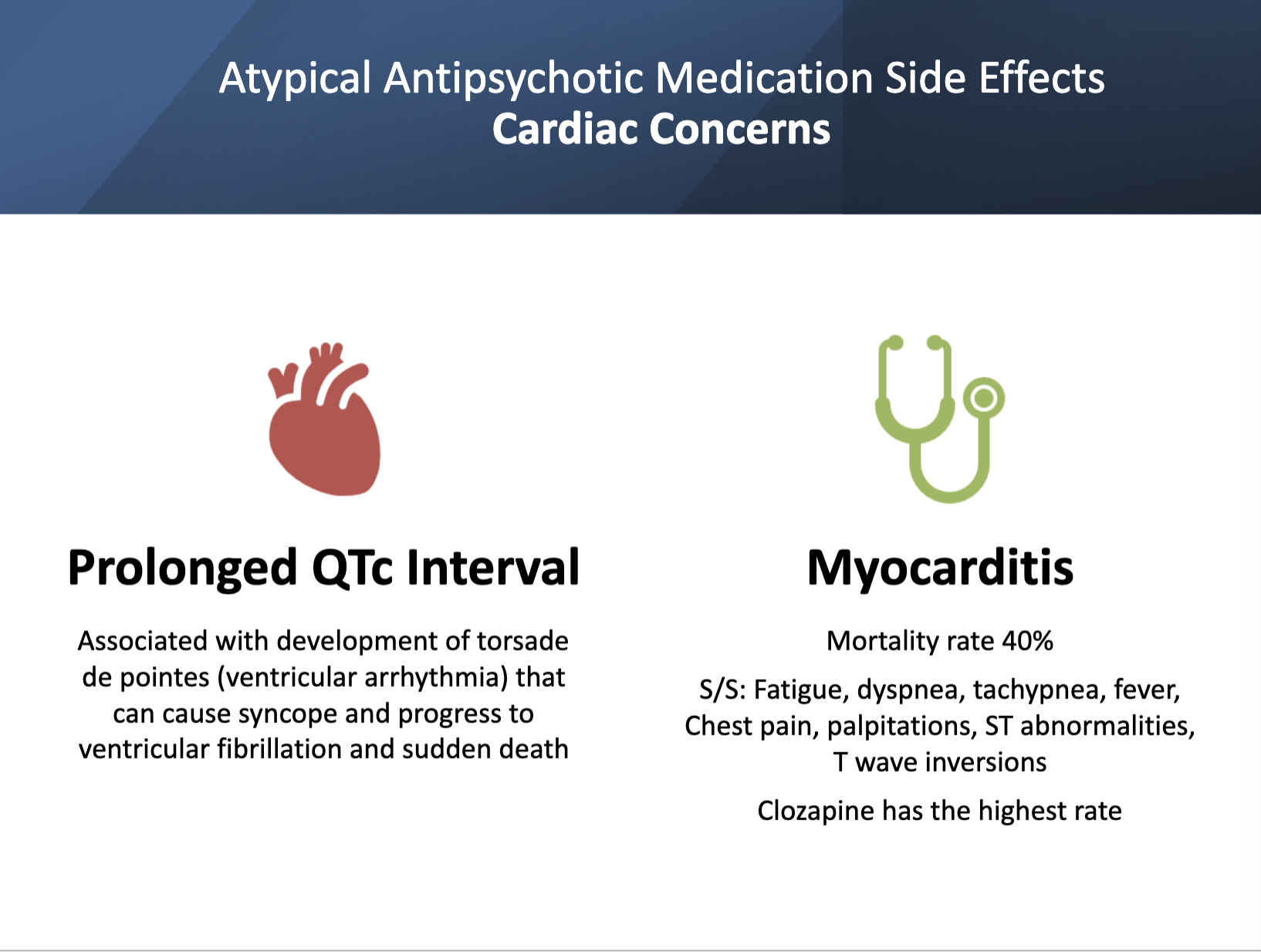
Prolonged QT Interval and Myocarditis
Nursing Implications for Monitoring and Administering Psychotropic Medications
takes 1-2 weeks to effect change
common: 6-12 weeks before changing prescription → a change in medication is indicated if a reduction in symptoms is not seen
do not withdraw suddenly unless du to a medical emergency
clazaril may be considered if a trial of atypical and typical anti-psychotic agents provided are ineffective
adherence is a challenge → medications are taken for a lifetime unless patient develops: neuroleptic malignant syndrome, agranulocytosis or tardive dyskinesia