Anatomy flashcard Set 3 (Post Midterm 2 Content)
1/182
Earn XP
Description and Tags
Endocrine, Repsiratory, GIT, Urinary and Reproductive
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
183 Terms
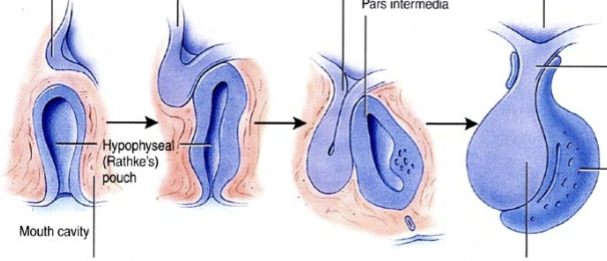
Pituitary gland development
Anterior lobe = externally attached during development, an outgrowth of the oral ectoderm which budded off and attached to the posterior lobe
Posterior lobe = direct outgrowth of CNS via stalk (infundibulim)
Anterior pituitary hormones
FSH, LH, GH, TSH, ACTH, Prl and MSH
Posterior pituitary homrones
Vasopressin (ADH) and oxytocin
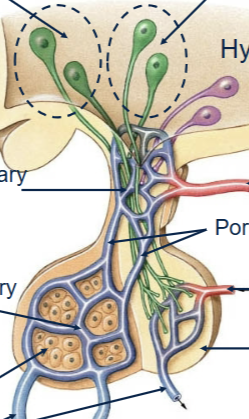
Hypothalamus connection to anterior pituitary
From nerves which send their messanger hormones in through a primary capillary, which links up via a portal vein to a secondary capillary system within the target site.
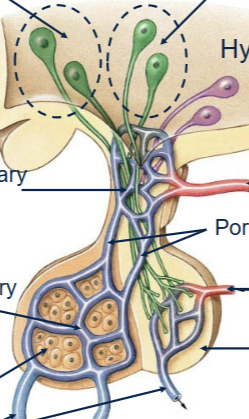
Hypothalamus connection to posterior pituitary
Supraoptic nucleus travels down stalk and initiates majority release of Vassopressin; Paraventriculular nucleus travels down stalk and initiates majority release of oxytocin (neurons direclty).
Thyroid gland
Activated by TSH release from anterior pituitary. Within thryoid follicle, thryoglobuline is released and Iodine is added to create T3 and T4. These are then released to the blood and help regulate metabolism (stimulate oxygen use, metabolic rate, cellular metabolism and growth/development).
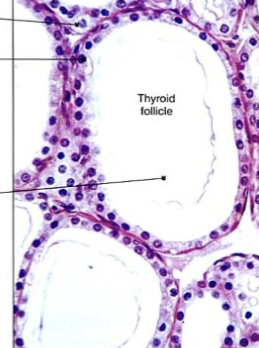
Parafollicular cells (C-cells)
Contained wtihin the thyroid, produce calcitonin (decreases Ca in body fluids, increases Ca in bones)

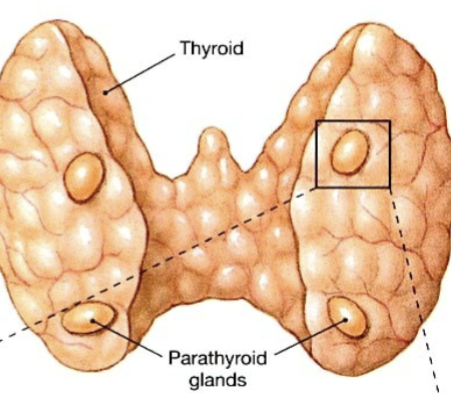
Parathyroid glands
4 total, placed on each of the 4 corners of the posterior surface of the thryoid gland. Produce parathyroid hormone (decreases Ca in bones, increases Ca in body fluids)
Adrenal cortex hormones
Made of 3 different cells = 3 different hormones produced. Outermost: Mineralcorticoids (aldosterone); Glucocorticoids (cortisol) and Androgens
Chromaffin cells
Post ganglion neuronal cells within the medulla of the adrenal gland that do not contain an axon. Instead, they directly release hormones into the bloodstream (epinephrine and norepinephrine).
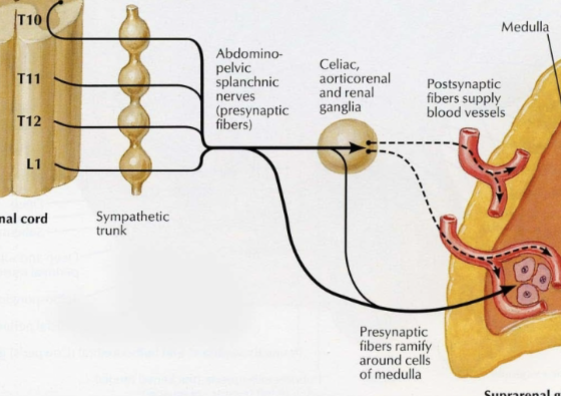
Adrenal medulla
Release epinephrine and norepinephrine (fight or flight response).
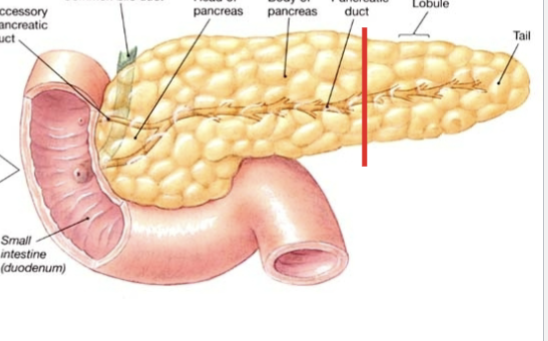
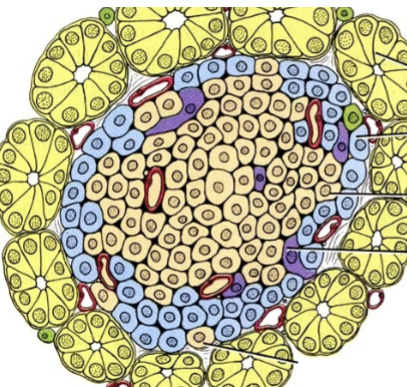
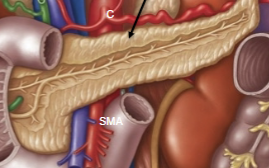
Pancreas (endocrine function)
Made up of exocrine portions which are ducts and inner islets that contain capillaries. The islets are the main endocrine regulator/component and contain 3 different cell types for 3 different hormones
Pancreatic hormones (endocrine function)
All within the islet:
Alpha cells = glucagon (glucose synthesis, raises blood sugar)
Beta cells = insulin (glucose uptake, decreases blood sugar, synthesis of glycogen)
Delta cells = Somatostatin (Inhibits secretion of glucagon and insulin)
Diabetes Mellitus
Inability to produce or use inuslin to manage blood sugar levels (causes hyperglycermia and excretion of glucose in the urine). Two types:
(10%) = Automimmune disease which destroys isulin secreting (beta) cells. Can be managed with injections of insulin. Called insulin-dependent
(90%) = Target cells become less responsive to insulin, correlating with obesity and age. Called insulin independent (insulin is there, the cells just aren’t reacting to it). Managed with diet and exercise.
Pineal gland
Physiological role unclear, secretes melatonin (thought to help with internal clock/sleep cycles).

Lower level vertebrate pineal gland
Closer to the surface of the skin so that it can be impacted/receptive to light changes (bright during day, dark at night etc). Humans have evolved away from this
Thymus gland
Produces T-lymphocytes (maturation).
Kidneys hormones
Erythropoitein (increase RBC production) and renin (increase blood pressure through RAS pathway)
Heart hormones
Atrial natiuretic peptide (decreases blood pressure)
Adipose tissue hormones
Leptin (decreases hunger, feeling of fullness = appetite suppressant)
Is breathing the same as respiration?
No. Breathing = inhalation/exhalation of air; respiration = physiological process by which gases are exchanged in the body
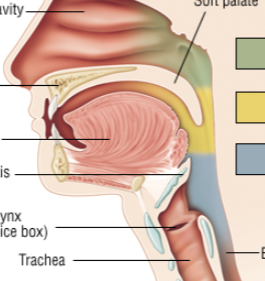
Concha/Turbinates
3 ridges of cartilage in nasal cavity, off the lateral wall. Generates turbulance of inspirated air and coated in mucous membrane to warm the air up (lots of warm blood supplied; increased contact)

Pharynx (Naso, Oro and Laryngo)
Common tube for air and food; continues on as the esophagus once it passes the larynx (very posterior in body)
Larynx
Cartilagenous organ which produces speech and seperartes the trachea from the pharynx/rest of esophagus.

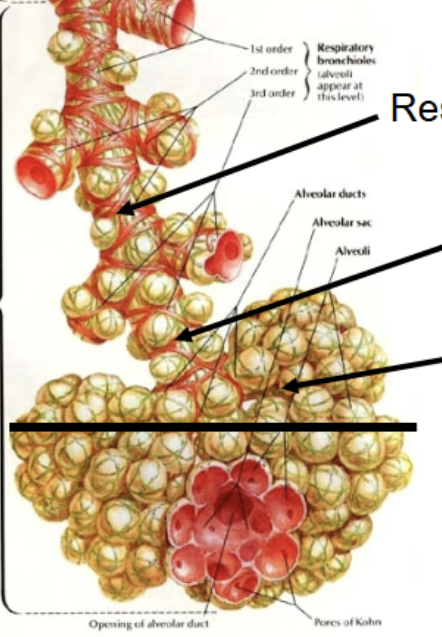
Conducting portion
Within the lower portion of the airway system (Larynx onward), the set of tubes through which air is fed into. Includes trachea, lungs, primary, secondary and tertiary bronchi, and ends with terminal bronchioles.
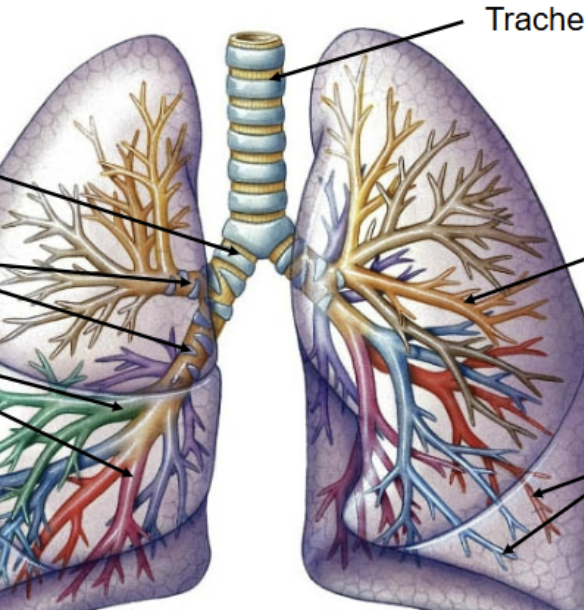
Respiratory portion
From respiratory bronchioles (the first to contain alveoli) and onwards (to alveolar sacs). The portion of the system that can actually partake in gas exchange.
Eustachian tube
Hole in nasopharynx that connects to the ears to equalize pressure differences (forcing air back against the tympanic membrane when descending under water or descending during flight, so the eardrum doesn’t burst from the high pressure outside).
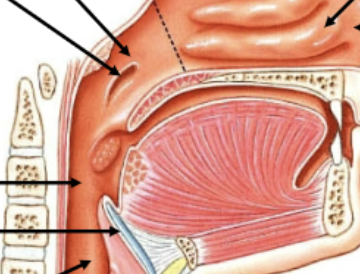
Soft palatte function in swallowing
At the back of the throat/oropharynx. Tongue/food pushes it upwards, blocking off acces to the nasopharynx and nasal cavity (ensures food cannot come out our nose)

Epiglottus function in swallowing
Folds over due to larangyeal muscle movement, blocking off access to the trachea/larynx.

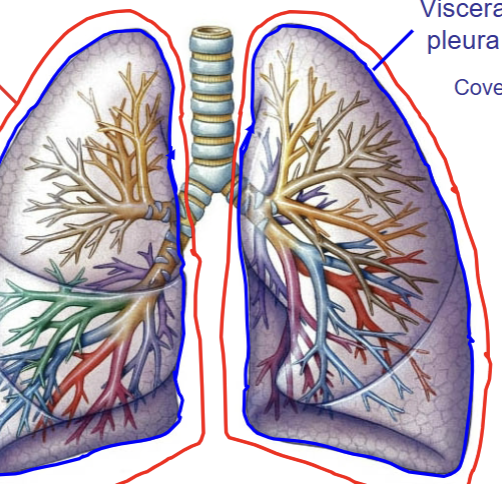
Hilum/Root of lungs
The only opening into the lungs; where the trachea, blood vessels, lymphatics and nerves enter/leave.

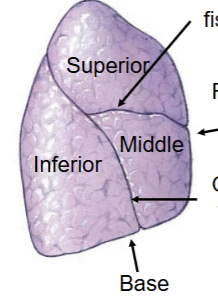
Right lung characterstics
Commonly has 3 lobes: Superior, Middle and Inferior. Contains horizontal fissure seperating superior and middle, and oblique fissure seperating inferior from both middle and superior. Commonly has 3 secondary bronchi lobules. Apex at the top portion (reverse from the heart).
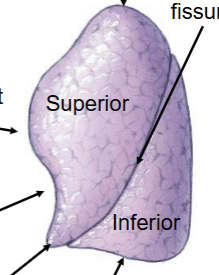
Left lung characteristics
Commonly has only 2 lobes (superior and inferior). Seperated by a single fissure = oblique. Superior lobe has special lingula feature (drops down lower than most of the inferior lobe). Cardiac notch present for heart to rest in. Only has 2 secondary bronchi lobules. Apex at the top portion (reverse from the heart).
Pleura
Casing where the lung rests in. Visceral portion lies intimately against the lung structures, parietal pleura covers the body wall - forms the pleural cavity. Both are serous membranes and secrete slippery fluid into pleural cavity to reduce friciton of the lung when breathing in/out. Also effectively cuts off the right and left lung from one another (once air has entered into one lung, it is not able to be shared with the other lung).
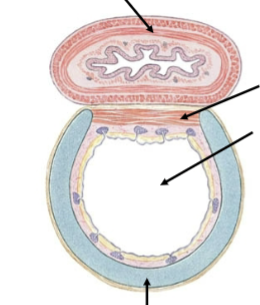
Trachea cartilage
C-shape ring around the anterior portion of the tube. Ensures that the tube remains open (even during sharp inhalation).
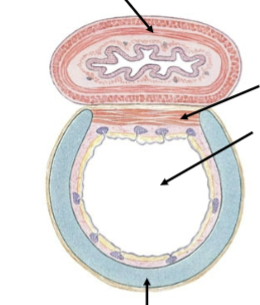
Trachea smooth muscle
Located on the posterior portion of the tube, which comes into contact with the esophagus. Allows for easy expansion of the tube when swallowing large pieces of food, so we don’t feel the food moving down against cartilage ridges when eating.
Airway wall make-up in larger airways
Majority cartilage in order to keep the airways open
Airway wall make-up in smaller airways
Increasing smooth muscle (to control airway diameter and thus slow down airflow) and elastic fibers (to provide recoil for expiration)
Airway wall make up in alveoli (smallest)
Simple squamous epithelium (for effecient gas exchange, want a thin layer). Means that damage here can have a large impact.
Asthma attack
Caused by smooth muscle over-contracting, restricting the airway wall due to allergies or parasympathetic impacts. Unable to take in enough air to properly respire.
Emphysema
Reduced ability to expel air (exhale fully) from the lungs, due to alveolar wall breakdown, causing larger respiring spaces and thus reducing the available surface area for gas exchange. Elastic recoil is also reduced due to loss of elastic fibers. Causes = Smoking, pollution or dust
Expansion of airways?
Not truly possible using muscles, we can only use sympathetic signals to stop the contraction of smooth muscle form occuring, thus leaving the airways as wide open as possible, in their relaxed state.
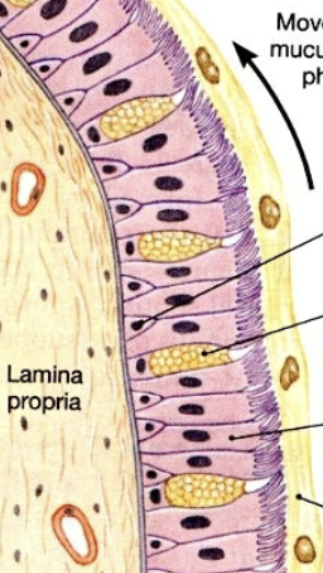
Respiratory epithelium
Begins with pseudostratified (in nasal cavity/nasopharynx/large ariways); coated in a mucous layer, which floats on a serrous/watery layer → stratified squamous (oropharynx) → simple columnar (smaller tubes) → simple cuboidal (smaller tubes) → simple squamous (alveoli)
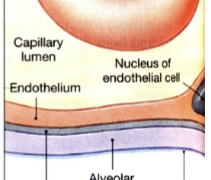
Oxygen molecule membrane crossings
From air space → alveolar epithelium → fused basement side 1 → fused basement side 2 → capillary endothelium → RBC membrane = 5 total
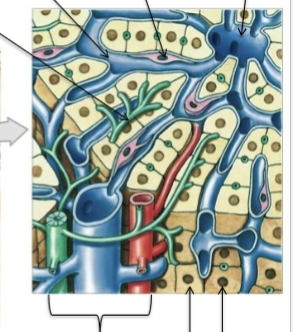
Type II alveolar cells
Secrete surfactant, which lowers the surface tension within the alveoli. Small, able to divide and differentiate into Type I cells (Yellow things)
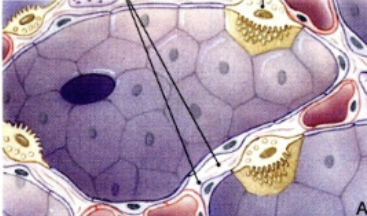
Type I alveolar cells
The ones that are actually involved in gas exchange, surrounded by continous simple epithelium. Not able to regenerate (if they die, they die). (purple cells)
Respiratory distress syndrome
Occurs in premature children, where type II cells are not fully mature yet. Results in very little or no surfactant, preventing the alveoli from properly inflating = insufficient blood oxygenation.
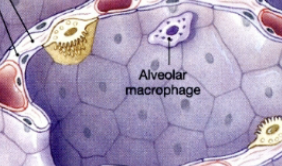
Alveolar macrophages
Ingest debris in alveoli. Become trapped in mucous upon entering airways. Mucous carried up towards the pharynx via cilliary action and mucous expelled or swallowed.

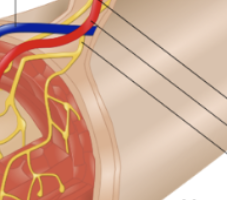
Pulmonary arteries
Travel and branch with airways, carry deoxygenated blood towards alveoli (blue)

Pulmonary veins and lymphatics
Travel in interlobular connective tissue. Blood vessel carries oxygenated blood away from lungs. (red and yellow)

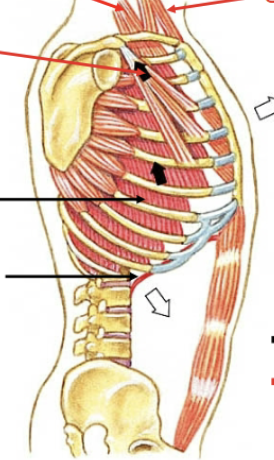
Relaxed inspiration muscles
Diaphragm contracts (not all the way) and external intercostal muscles pull ribs up and out to make more room in the chest cavity, as well as move sternum anteriorly
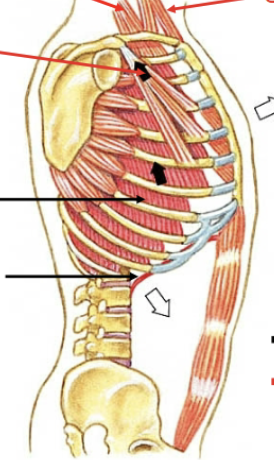
Forced/maximal inspiration muscles
Pectoralis minor (opens chest cavity = elevates ribs 3-5), scalenes (elevates ribs 1-2) and sternocleidomastoid (Elevates sternum)
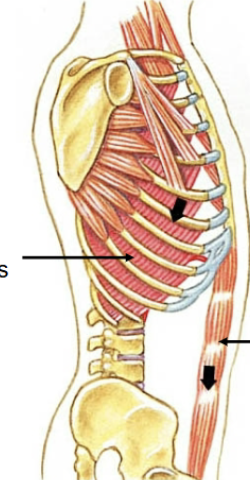
Relaxed expiration muscles
N/a, done by elastic recoil alone
Forced/maximal expiration muscles
Abdominal and internal intercostals (move inferior ribs inferiorly and compress viscera = diaphragm moved superiorly)
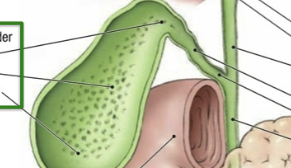
Is the gallbladder a gland?
NO. Only a storage compartment for bile that was synthesized by the liver.
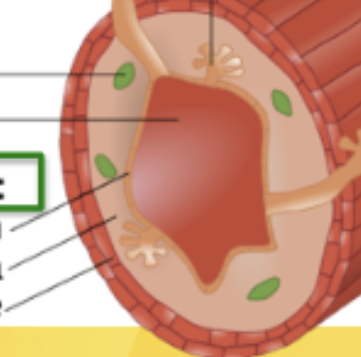
Mucosa Layer
Outermost layer of the GIT. Made of 3 sections: epithelium(stratified or simple depending), lamina propria (connective tissue with glands and immune cells) and muscularis mucosa (smooth muscle that propels gland contents into lumen)
GIT regions with statified epithelium
Pharynx, esophagus and anus (need to be able to withstand abrasion)
GIT region with simple epithelium
Intestines (more important to have absorption carried out here)
Submucosa (connective tissue)
Second layer of GIT, contains vasculature, lymphatics and nerves. Also has immune cells, exocrine glands and the submucosal plexus (acts on glands)
Muscularis externis
3rd layer of GIT. Contains smooth muscle (inner circular layer surrounding tube and outer longitudinal layer that runs along tube). Contains myenteric plexus. Important: at the beginning and end of GIT, this layer transitions from smooth to skeletal, just briefly (to allow conscious control of swallowing and defecation).

Serosa
Last layer of GIT, forms abdominal wall. Simple squamous epithelium + serosa membrane connective tissue. Continually produces watery secretions that lubricate peritoneal surface. Two layers of mesentery.
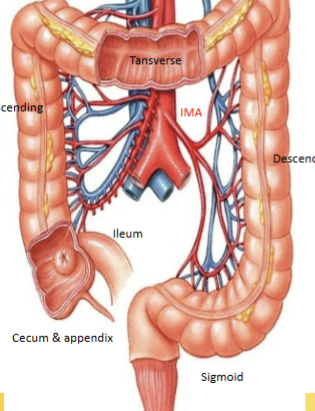
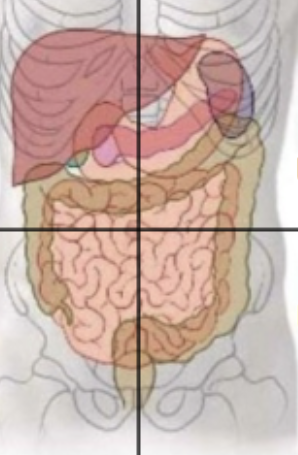
RUQ organs
Liver, gall bladder, duodenum, head of pancreas, transverse colon (portion) and right kidney
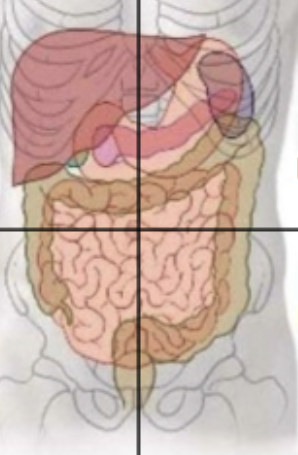
LUQ organs
Stomach, pancreas body/tail, Left kidney, transverse colon (portion), jejenum and spleen
RLQ organs
Ilium (portion), cecium, appenidx, ascending colon
LLQ organs
Ilieum (portion), descending and sigmoidal colon
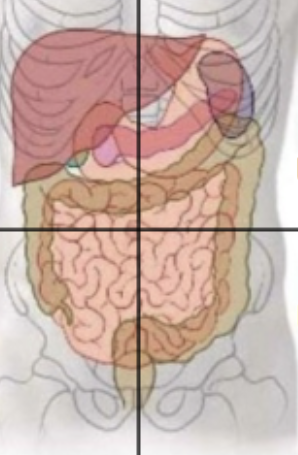
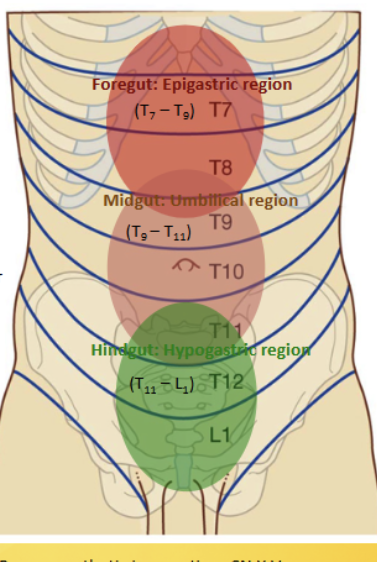
Epigastric region
Contains the foregut, located at the superior midclavicular and above the subcostal planes. Contains the esophagus, stomach, spleen, liver, gallbladder, pancreas (1/2) and duodenum (1/2). All supplied with blood (and nerves) from the celiac trunk = T7-9
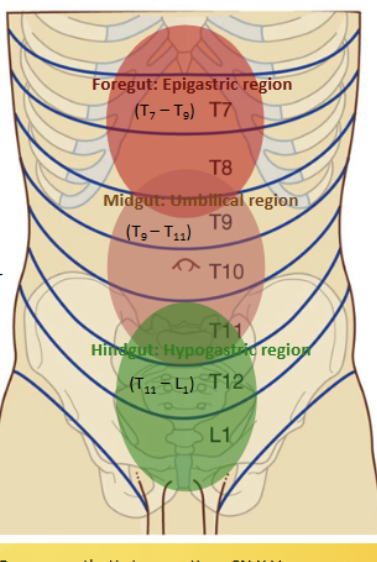
Umbilical region
Contains the midgut, located inferior to the subcostal and superior to the intertubercular planes. Contains the pancreas (2/2), descending duodenum (2/2), jejnum, ileum, appendix, cecum, ascending and transverse colon. All supplied with blood (and nerves) from the superior mesentaric = T9-11
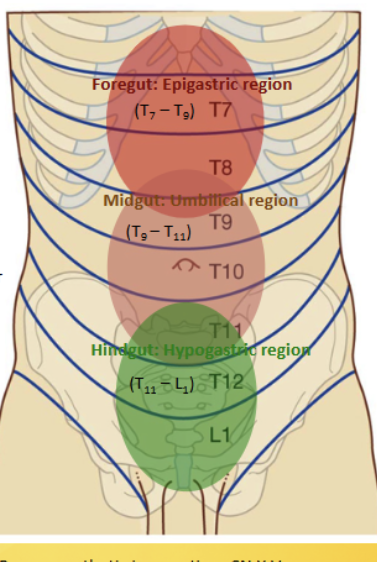
Hypogastric region
Contains the hindgut, located in the inferor midlavicular and inferior to the intertubercular planes. Contains the transverse colon, descending/sigmoidal colon and rectum. All supplied with blood (and nerves) from the inferior mesentaric = T11-L1
In place of celiac vein
Contains a splenic vein instead
All blood leaving GIT (in veins) ends up where?
In the hepatic portal vein, so that the liver can filter all the nutrients from the blood before sending it back to the heart

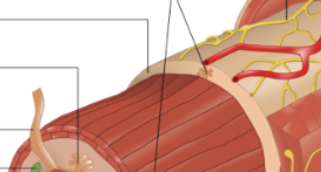
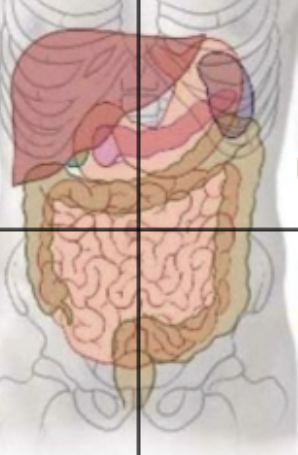
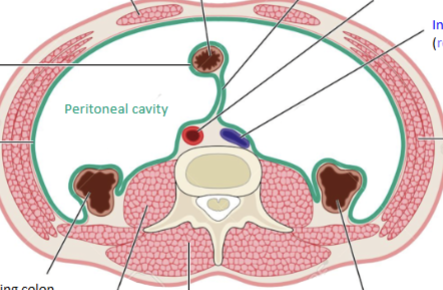
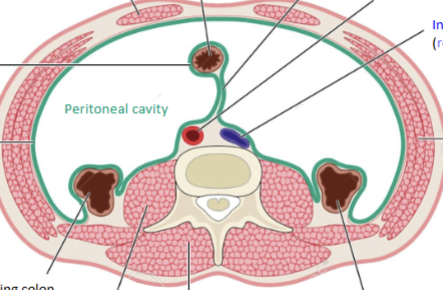
Parietal peritoneum
Serous membrane surrounding the external portion of the perotineal cavity (body wall = somatic innervation) (orange)
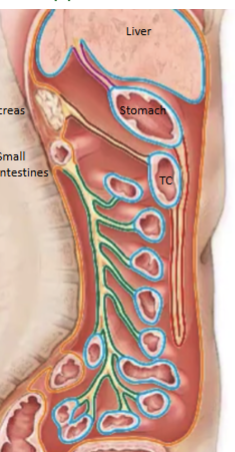
Visceral peritoneum
Serous membrane surrounding the peritoneal cavity organs (stomach, liver etc etc) (blue)
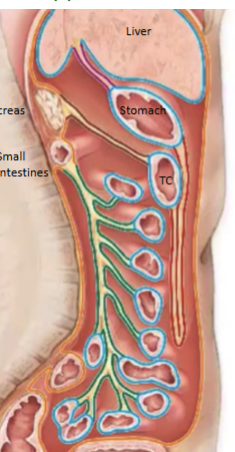
Mesentary
Sandwich of peritoneum (2 layers = folded back) within peritoneal cavity that serves as a conduit for blood, nerves and lymph vessels (green)
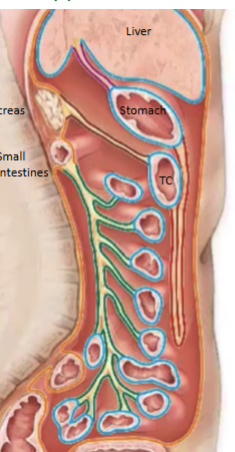
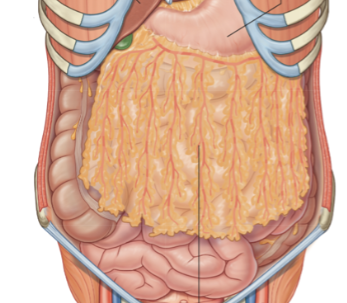
Greater omentum
Large mesentary that drapes down from the stomach to the transverse colon (first thing you would see upon cutting into the abdominal cavity). Has temperature control and immunological function
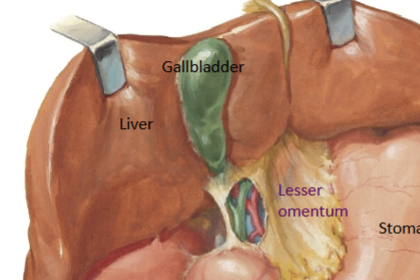
Lesser omentum
Mesentary running from liver to stomach (purple). Contains the portal triad (hepatic artery, hepatic portal vein and bile duct)
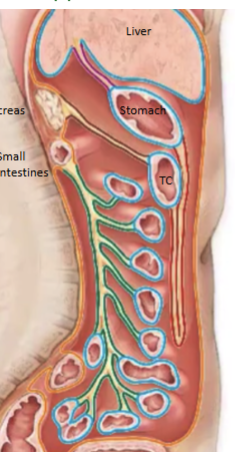
Intraperitoneal structures
Completely contained within peritoneum (small intestine, stomach, liver). Due to this, surface is slippery, and generation of friction is not possible therefore it is more difficult to propel contents through these tubes (takes a longer time, increases contact with surface area, increases absorption)
Retroperitoneal structures
Portions sticking out behind the peritoneum (large intestine, adrenal glands, kidneys, pancreas, ureters, inferior vena cava and descending aorta = everything not associated with GIT absoprtion). Enables the generation of friction against posterior body wall, propelling contents through the tubes much easier.
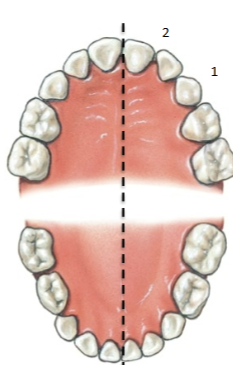
Oral cavity features
Stratified squamous epithelium (gives sensory info about food = tastes), mechanical digestion begins, chemical digestion begins (amylase), salivary glands (perotid, subling and submand) lubricate. 3 tonsils present (pharyngeal, palatine = the ones we see and lingual)
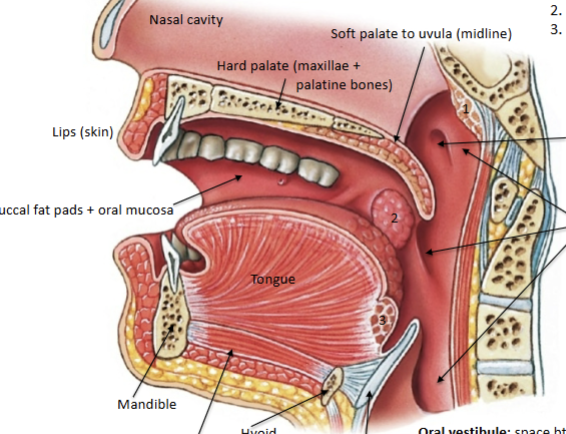
Incisor teeth (8 total)
First two on either side of midline; blade like, for cutting and clipping food

Canine (4 total)
3rd tooth from center, for tearing/slashing food

Premolars (8 total)
Bicuspid - for crushing/mashing/grinding

Molars (12 total)
Multicuspid - for crushing/grinding

Decidous teeth
20 total, No premolars, only 2 molars. Begin eruption between 6-24 months and shed 6-12 years old
Pharynx features
Stratified squamous epithelium. Divided into naso, oro and laryngo-. Glands throughout that secrete mucous. Ends at the esophagus/trachea divide. Innvervation via cn X. Many skeletal muscles for swallowing (tensor and levator palatini = elevation of soft palate; sup/mid/inf pharyngeal constrictors and suprahyoid = elevate larynx, push bolus down)
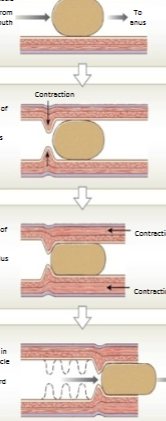
Peristalsis
Propulsion of bolus via coordination of:
Circular muscle: Causes narrowing of lumen (constriction)
Longitudinal muscle: Shortens (pulls in/inchworms) the tube
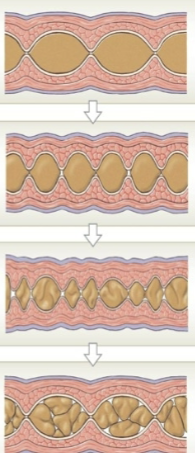
Segmentation
Mainly circular muscle, contracting and relaxing repeatedly. Just churning/mixing the food in one spot, does not propel it anywhere. Mechanical digestion; increases absorption time.
Esophagus features
Stratified squamous epithelium; extends from C6 - T7. Skeletal and smooth muscle. Bolus moved via peristalsis to the cardiac sphincter (gaurds opening of stomach). Lots of mucous secretion; tube innervated via cn X
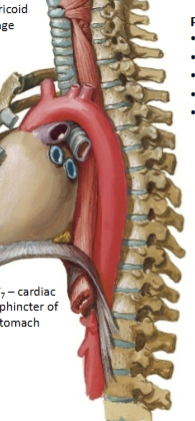
Stomach features
Simple columnar epithelium (more exocrine functions). Completley intraperitoneal. Celiac trunk = artery (foregut structure); splenic vein = vein. Greater curvature attaches to greater omentun; lesser to lesser. Pyloric sphincter at bottom. Stomach wall main difference = 3 layers of muscle (smooth, long and oblique). Gastric pits increase surface area, create canals where glands secrete into. First place where we see enteroendocrine cells appear (respond to the contents of the lumen and adjust secretions accordingly = G cells).
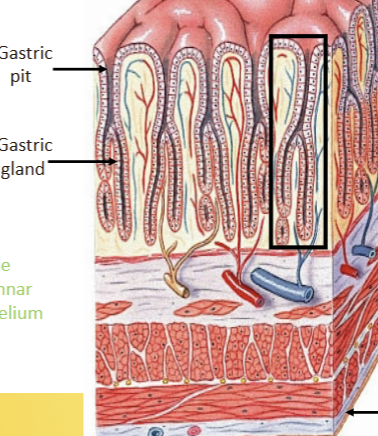
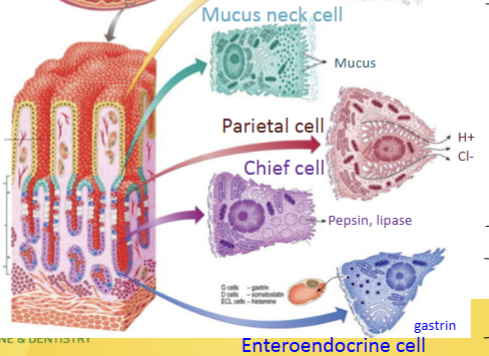
Gastric (stomach) gland secretory cells
Surface and mucus neck cells = mucus secretion; Parietal cell = HCl secretion; Chief cell = Pepsin and lipase secretion (active only at low pH = stomach environment); Enteroendocrine cell = Gastrin release
Small intestine
Simple columnar epithelium. Where the majority of digestion/absorption takes place. D, J, I. Foregut and midgut structures, mostly intraperitoneal. Small in width, NOT in LENGTH.

Duodenum
First section of small intestine, after pyloric sphincter. Intraperitoneal at beginning and end, retroperitoneal in the middle (associated with the pancreas). Recieves blood from celiac trunk and superior mesentaric. Combines bile (from gall bladder/liver), chyme (from stomach) and digestive enzymes from pancreas. Digests fats, proteins and sugars. Contains brunner’s glands in the submucosal layer to produce alkaline mucus (neutralize HCl).
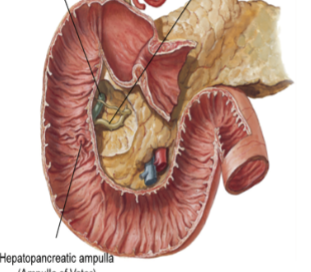
Pancreas (exocrine/GIT function)
Recieves blood from celiac (splenic artery) and superior mesentaric. Completley retroperitoneal. Secretes digestive enzymes (amylase, lipase and proteinase) from acinar cells and bicarbonate buffer from centroacinar cells. These all combine into the central pancreatic duct, which moves from the tail towards the head of the organ. It combines with the bile duct, and then can move into the duodenum through the hepatopancreatic sphincter.
Control of hepatopancreatic sphincter
Done via CCK, upon presence of chyme in the duodenum, causing relaxation and gallbladder contraction.
Liver
Celiac trunk (hepatic artery) and hepatic portal vein vasculature (recieves deoxygenated but nutrient rich blood from all other GIT organs). Lots of functions (carb, fat, protein metabolism; detoxify; blood maintence = old RBC/WBC breakdown, plasma protein secretion; synthesis of bile). Arragned in functional hepatic lobules.
Hepatic lobules
Hexagonal (bounded by 6 portal systems = lymphatics, vein and blood vessel) around a central vein = portal triads. Contain Kupffer cell macrophages and bile canniculi (which produce bile). Canniculi created via tight junctions between hepatocytes (epithelial tight junctions). Other side of eptihelium is fenestretated, allowing for easy access of materials into/out of the blood
Gallbladder
Connected to the liver via hepatic ducts, which feed into the cystic duct. Stores bile until it is needed by the pancreas, when it is released into the bile duct. NOT a GLAND.
Jejenum
2nd segment of small intestine. Increase in villi/circular folds and therefore surface area (compared with rest of small intestine). Majority of nutrient absorption. Intraperitoneal. Supplied by superior mesentaric vein/artery (true midgut).

Ileum
Third segment of small intestine. Intraperitoneal; superier mesentaric artery/vein (true midgut). Contains lymph nodules (peyer’s patches)
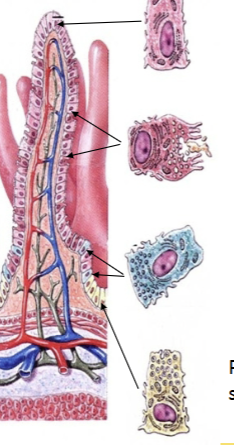
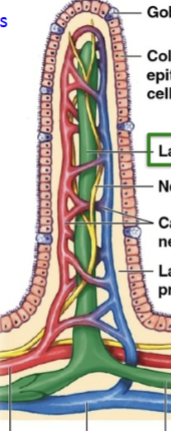
Villar epithelium
Microvilli (absorptive); Goblet cell (mucus); Enteroendocrine cell (regulation via many hormones); Paneth cell (immunity = secretions kill bacteria).
Villi absorption
In the small intestine: Carbs/Proteins can be absorbed directly and fed through to the hepatic portal vein. Fats are too large (and not water soluble), so they are broken into small fatty acids + bile (chylomicrons, chyle) and absorbed via lymphatic system into the lacteal
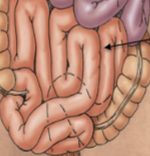
Large intestine
Intraperitoneal (cecum, transverse and sigmoidal) and retroperitoneal (ascending, descending, rectum). Superior/Inferior mesentaric vasculature. Reabsorbs water, electroyltes, important vitamins (vit K, B12), contains digestive bacteria (no enzymes). Teniae coli = external longitudinal smooth muscle layer, slightly shorter than intestine (scrunches it together). Contains crypts to increase surface area with absorptive cells and goblet cells (lots of mucus). Large in DIAMETER