human phys exam 4
1/71
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
72 Terms
what are the functions of the kidney?
functions of the kidney:
regulation of water, inorganic ion balance, acid-base balance
removal of metabolic waste products & foreign chemicals from blood + excretion in urine
gluconeogenesis
production of hormones/enzymes (erythropoietin, renin, vitamin D)
what is the renal cortex vs. renal medulla?
renal cortex: outer region
renal medulla: inner region pyramids
distinguish between the two types of nephrons
cortical nephron: located mostly in cortex; performs filtration & bulk reabsorption
juxtamedullary nephron: located deep into medulla; responsible for urine concentration & creating osmotic gradient
what is the difference between filtration, secretion, and reabsorption?
filtration: blood → glomerulus → Bowman’s capsule
reabsorption: kidney (tubule) → blood (peritubular capillaries)
secretion: blood (peritubular capillaries) → tubule (kidney); will be excreted via. urine
what is the organization of the nephron?
glomerulus → Bowman’s capsule → proximal convoluted tubule (PCT) → Loop of Henle → distal convoluted tubule (DCT) → cortical collecting duct
why are some molecules actively secreted vs. reabsorbed?
homeostatic control
secreted - eliminate molecules that the body doesn’t need (e.g., waste products, toxins, in excess)
reabsorbed - conserve molecules that are valuable to the body (e.g., glucose, amino acids)
secreted & reabsorbed - regulation of pH, K+
what is the sequence of blood flow in the glomerulus?
afferent arteriole → glomerular capillaries → efferent arteriole
**highest blood pressure/hydrostatic pressure in the glomerulus
what are podocytes?
foot processes that create filtration slits
provide selective barrier for size & charge
what is Bowman’s capsule?
surrounds glomerulus to collect filtrate and send to PCT
what is juxtaglomerular apparatus (JGA)?
controls filtration & blood pressure
composed of…
macula densa: senses NaCl concentration to regulate renin & GFR
juxtaglomerular cells: modified smooth muscle cells that secrete renin to regulate blood pressure
what are mesangial cells?
modified smooth muscle
can contract → ↓ surface area → ↓ GFR
what molecules can and can not be filtered through podocytes?
filtered: H2O, electrolytes, glucose, amino acids, vitamins, urea, uric acid, creatinine
NOT filtered (large molecules): blood cells, plasma proteins, large anions, minerals (e.g., Ca2+), hormones
what factors are involved in glomerular filtrate rate.
podocyte pores - filtration barrier affecting what can and can’t be filtered
hydrostatic (blood) pressure - driving factor of filtration; pushes filtrate OUT
ideally wide afferent arteriole & narrow efferent arteriole to push fluid out of glomerular capillaries into bowman’s capsule
forces opposing filtration
bowman’s capsular hydrostatic pressure: pressure in Bowman’s capsule pushing fluid back into capillaries
glomerular oncotic pressure: caused by plasma proteins pulling water back into capillaries
*net glomerular filtration rate (GFR) = glomerular hydrostatic pressure - bowman’s hydrostatic pressure - glomerular oncotic pressure
what factor regulates the glomerulus filtration rate?
arteriole diameter
afferent arteriole
↓ diameter (constriction) → ↓ GFR (less filtration)
↑ diameter (dilation) → ↑ GFR (more filtration)
efferent arteriole
↓ diameter (constriction) → ↑ pressure → ↑ GFR
↑ diameter (dilation) → ↓ pressure → ↓ GFR
what is the PCT?
Proximate Convoluted Tubule (PCT): major site of water and solute reabsorption in blood
How is water and sodium reabsorbed in the PCT?
sodium
Na+ moves down concentration gradient from lumen → PCT/tubule cell
Na+ is actively transported/pumped into interstitial fluid
water
water follows sodium via. osmosis
how are molecules reabsorbed and secreted in the PCT?
*driven by Na+ gradient (created by Na+/K+ ATPase
Cotransport (symport) → reabsorption of glucose & amino cells from lumen → cell
Countertransport (antiport) → secretion of H+ from cell → lumen
how does PCT regulate pH?
normal conditions:
H+ recycled back into lumen
HCO3- reabsorbed into blood
alkalosis: more HCO3- > H+ in lumen
↓ H⁺ secretion, ↑ HCO₃⁻ excretion
some reform H2CO3 → CO2 + H2O, rest of HCO3- stays in lumen and excreted out via. urine
acidosis: more H+ > HCO3-
↑ H⁺ secretion via. urine, ↑ buffers (phosphate, ammonia), ↑ new HCO₃⁻ reabsorbed
HPO42- (buffer) + H+ → H2PO4- → urinated out
NH3 (buffer) +H+ → NH4+ → urinated out
what is the Loop of Henle? what are the two parts of it?
creates gradient (countercurrent multiplier) via. active transport (pump)
descending limb: goes into renal medulla
permeable to water → water leaves descending limb to interstitial fluid
filtrate/urine becomes more concentrated (hyperosmotic)
ascending limb: goes back to renal cortex
impermeable to water
actively pumps ions (Na+, K+, Cl-) out to interstitial fluid via. NKCC
filtrate becomes dilute (hypoosmotic), interstitial fluid becomes hyperosmotic
medulla gradient: further down medulla = saltier
how to loop diuretics work?
targets NKCC in Loop Henle to treat hypertension
blocking NKCC → less salty medulla → less water reabsorbed into interstitial fluid, more water retained in kidney → more water urinated, lower blood volume, lower blood pressure
what is the vasa recta?
vasa recta: capillary network that runs parallel to loop of Henle
maintains osmotic gradient in medulla (countercurrent exchange) via. passive transport
collects water from interstitial tissue
both limbs permeable to water but not permeable to colloid proteins
what are the two portions of the vasa recta?
descending portion (going into medulla): NaCl diffuses INTO blood, water diffuses OUT of blood → blood becomes more concentrated (hyperosmotic)
ascending portion: NaCl diffuses OUT of blood, water diffuses INTO blood → blood becomes diluted
which nephron structures are regulated via. osmosis vs. hormones?
osmosis: PCT, Loop of Henle, vasa recta
hormones: DCT, collecting duct
what effects do vasopressin have on collecting duct?
vasopressin = anti-diuretic hormone (ADH)
controls water permeability by inserting aquaporins (water channels) into membrane to allow movement of water from lumen → interstitium
dehydration → sensed by osmoreceptors in hypothalamus → hypothalamus signals to posterior pituitary gland to release vasopressin/ADH → add aquaporins → urine becomes concentrated/less urination, blood volume increases
when is ADH inhibited? what effect does that have on the body?
inhibited when…
blood is too dilute → ↓ signaling of osmoreceptors in hypothalamus → ↓ ADH release from posterior pituitary
blood volume/pressure is too high → ↑ baroreceptor firing → siginal ↓ ADH release
alcohol
effects:
fewer/no aquaoprins → ↓ water reabsorption → ↓ blood volume, ↑ urine volume → frequent urination & dehydration
what effect does aldosterone have on collecting duct?
aldosterone: increases Na⁺ reabsorption and K⁺ secretion → retains water & increases blood volume/pressure
what controls aldosterone release?
low Na+ → activates RAAS (indirect) → ↑ aldosterone release
high Na+ → activates RAAS (indirect) → ↓ aldosterone release
high K+ → ↑ aldosterone release (direct control) → ↑ K+ excretion, ↓ plasma K⁺
low K+ → ↓ aldosterone release (direct control) → ↓ K+ excretion, ↑ plasma K⁺
How is aldosterone regulated by renin system?
macula densa senses low Na+
triggers JG (juxtaglomerular) cells to release renin
triggers RAAS pathway (renin-angiotensin-aldosterone system)
ACE converts angiotensin I → angiotensin II → vasoconstriction → ↑ blood pressure
aldosterone → Na/K+ ATPase pumps Na+ out (lumen → blood) and K+ in (blood → lumen) → ↑ Na⁺ reabsorption + ↑ K⁺ secretion → more water reabsorption in blood → ↑ blood volume → ↑ blood pressure
what influences JGA renin secretion?
macula densa senses NaCl concentration in tubular fluid
low NaCl → ↓ GFR, ↓ flow → stimulates JG cells to ↑ renin release
high NaCl → afferent arteriole constriction + ↓ renin release
afferent arteriole pressure (baroreceptor mechanism)
low pressure → ↓ stretch → ↑ renin release
high pressure → ↑ stretch → ↓ renin release
sympathetic nervous system (β₁)
↑ sympathetic (β₁) → ↑ renin
what is the difference between endocrine vs. exocrine glands?
endocrine: secrete hormones directly into bloodstream; does not have ducts; acts on distant targets
exocrine: secrete via. duct to lumen/surface; local effects (e.g., sweat, digestive enzymes)
what are the three major classes of hormone molecules?
amines - derived from amino acids (e.g., tyrosine)
peptides - protein-based hormones
water-soluble → travels freely without needing a carrier
acts on cell surface receptor (bc can’t to through plasma membrane)
steroids - cholesterol-based
lipid soluble → travels bound to hormone binding protein to form hormone-protein complex
acts on intracellular receptors
what are examples of amino hormones?
e.g., dopamine, epinephrine, norepinephrine
what are examples of peptide hormones?
e.g., vasopressin, oxytocin, insulin
what are examples of steroid hormones?
e.g., cortisol, aldosterone, testosterone, estradiol
what is congenital adrenal hyperplasia?
congenital adrenal hyperplasia: inherited genetic disorder that impairs the adrenal glands’ ability to produce essential hormones (cortisol and aldosterone) and overproduce androgens
how are levels of testosterone vs. estradiol regulated?
**ratio of testosterone to estradiol is dependent on amount of aromatase (enzyme that converts testosterone to estradiol)
what is the significance of cholesterol being the base molecule for steroid
interconnected pathways
lipid-soluble → cross cell membrane and bind to intracellular receptors
slower onset but long-lasting effects
bound to carrier proteins to be transported in blood
what is the difference between total vs. free hormone levels?
total hormone = free hormone + protein-bound hormone
free hormone = unbound hormone
what are the types of hormone interactions?
Synergistic: effect of each hormone is independent, but combined effect is greater/additive
Antagonistic: one hormone opposes/inhibits another
Permissive: one hormone enhances/affects another hormone’s effect/physiology
what is an example of synergistic interaction?
ex: combo of epinephrine + norepinephrine have a greater increase on heart rate together than independently
what is an example of antagonistic interaction?
ex: insulin + glucagon → maintains blood sugar levels
what is an example of permissive interaction?
ex: epinephrine + thyroid hormone
ex: peak in estrogen/estradiol in uterus causes increase in progesterone receptors
what is the difference between physiologically relevant and pharmacological level?
physiologically relevant levels: normal concentration of hormone in the blood that naturally occurs in the body
controlled by feedback mechanisms to maintain homeostasis
reflects balance of secretion, circulation, uptake and removal
pulsatile secretion release hormones in bursts rather than constantly to prevent excess hormone buildup
pharmacological levels: higher than natural/physiological levels
what is the initial vs. long-term effect of pharmacological levels of hormones?
initial effect: higher binding → ↑ activity
long term effect:
stress → ↓ sensitivity (downregulation)
binding to unintended low-affinity receptors → change other hormone levels → downstream effects
what inputs regulate endocrine cell secretions?
ions/nutrients, neurotransmitters, hormones
**key idea: each input can act independently or dependently (permissive effects, influence/interact with each other)
ex: high blood sugar → insulin release → lowers blood sugar → releases glucagon
what mechanisms limit hormone concentrations in blood?
negative feedback
uptake by target tissues
hormone half-life (time it takes hormone levels to drop by 50%)
liver metabolism/degradation into inactive forms
receptor regulation (up/downregulation)
naturally avoid downregulation through pulsatile secretions
what are tropic vs. trophic hormones?
tropic: any hormone that acts on other endocrine glands as their target
trophic: any hormone that causes tissue growth
what are the two parts of the pituitary gland?
Anterior pituitary (adenohypophysis) → makes hormones
Posterior pituitary (neurohypophysis) → stores & releases hormones made in hypothalamus
what hormones are secreted from the anterior pituitary gland?
tropic hormones:
TSH (thyroid stimulating hormone) - targets thyroid gland for T3/T4 production
ACTH (adrenocorticotropic hormone) - targets adrenal cortex for cortisol section
LH (luteinizing hormone) - targets gonads for ovulation & testosterone production
FSH (follicle-stimulating hormone) - targets gonads for follicle development + sperm production
direct/non-tropic hormones:
growth hormone
prolactin - targets mammary glands to produce milk
what hormones are secreted from the posterior pituitary gland?
ADH (Antidiuretic hormone/vasopressin) - targets kidney for water reabsorption
oxytocin - uterine contractions + milk ejection
what are the hormones produced and secreted by the thyroid gland?
T4 (thyroxine) hormone (80%): longer half-life → travels longer distances than T3
T3 (triiodothyronine) hormone (20%): 4x as potent as T4; strong effect but degrades faster (short half-life)
what is the pathway to make thyroid hormone?
follicular cells secrete thyroglobulin into colloid/lumen
thyroglobulin + iodine → MIT (1 iodine) or DIT (2 iodine)
DIT + DIT → T4
MIT + DIT → T3
what are the structures of the thyroid?
thyroid follicles: main unit made of follicular cells (outer layer) and central lumen filled with colloid
follicular cells: produce thyroglobulin, takes up iodine, process/release T3/T4
colloid: gel-like material inside follicles; site of hormone synthesis + storage
parafollicular cells: located between cells; secrete calcitonin
what is TSH?
TSH (thyroid stimulating hormone): tropic hormone that stimulates iodine uptake + TG synthesis → leads to synthesis + release of T3/T4
What are the functions of thyroid hormone?
binds to intracellular receptors → induce gene transcription
↑ metabolism - stimulates carb absorption in small intestine, fat breakdown, protein turnover
↑ heat production - stimulates Na+/K+ pump activity → heat byproduct to maintain body temp
improves muscle performance via. myosin ATPase
Permissive effects
T3 + epinephrine → fatty acid + glycerol release
b-adrenergic receptors respond to thyroid hormone → ↑ heart rate
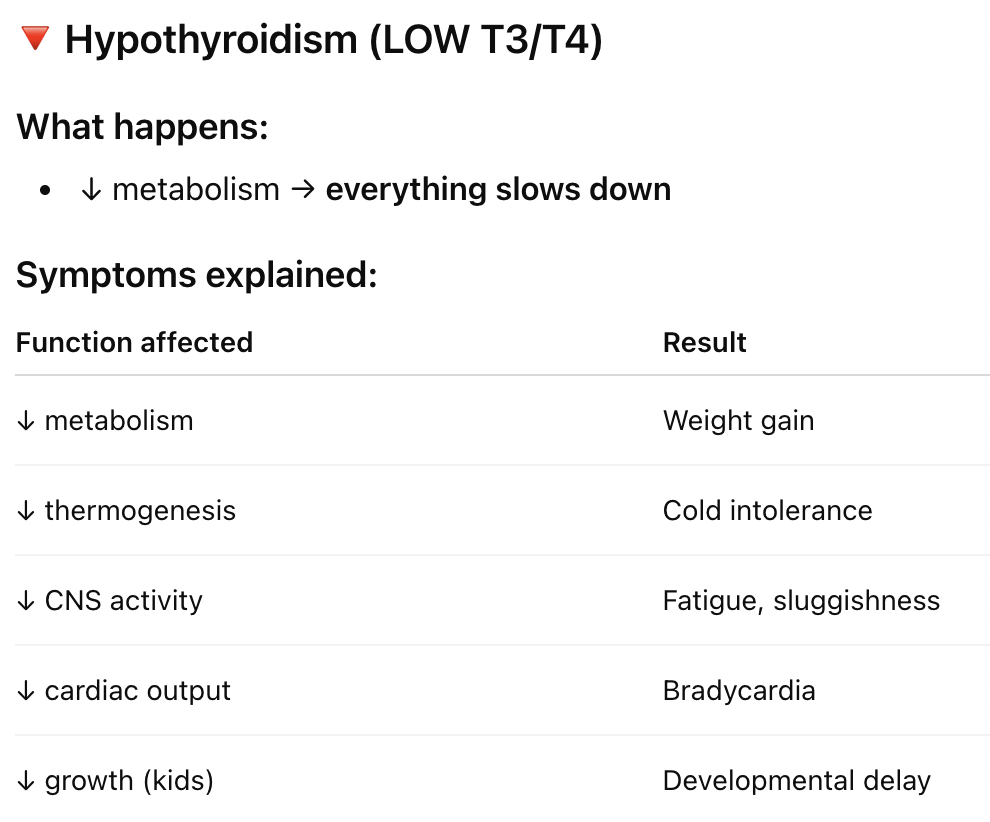
what is hypothyroidism?
hypothyroidism: underactive thyroid; low T3/T4
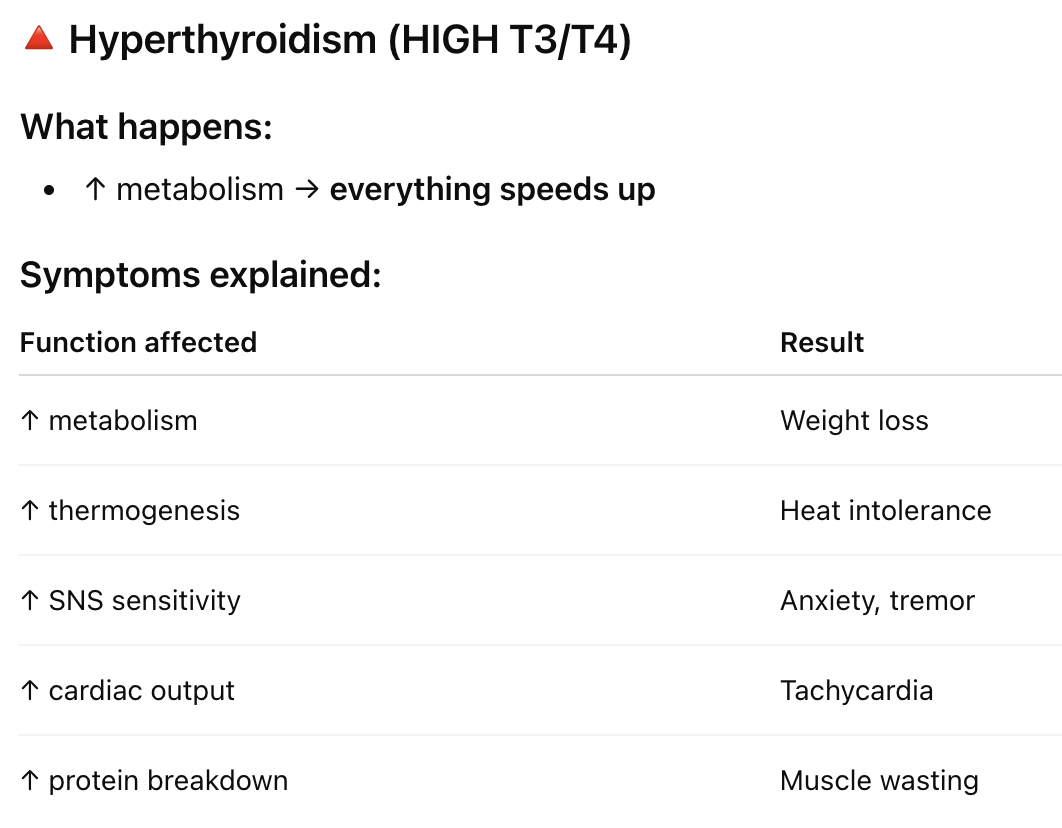
what is hyperthyroidism?
hyperthyroidism: overactive thyroid; high T3/T4
what is goiter? how can it present as both hyper and hypothyroidism?
goiter: thyroid enlargement
if caused by hyperthyroidism: overactive thyroid → excess trophic hormones (T3 + T4) → cell enlargement
if caused by hypothyroidism: underactive thyroid → stimulates TSH release → tumor growth
what are parafollicular cells?
secrete calcitonin (hormone)
inhibits osteoclast activity (breakdown bone)
opposite effect of PTH (parathyroid hormone)
↓ blood Ca²⁺ → ↓intestine Ca2+ absorption, ↓ bone resorption (osteoclast activity), ↓ renal Ca2+ reabsorption, ↑ Ca2+ secretion, ↓ vitamin D synthesis
what are parathyroid glands?
release PTH (parathyroid hormone)
opposite effect of calcitonin
↑ blood Ca2+ → ↑intestine Ca2+ absorption, ↑ bone resorption (osteoclast activity), ↑ renal Ca2+ reabsorption, ↓ Ca2+ secretion, ↑ vitamin D synthesis
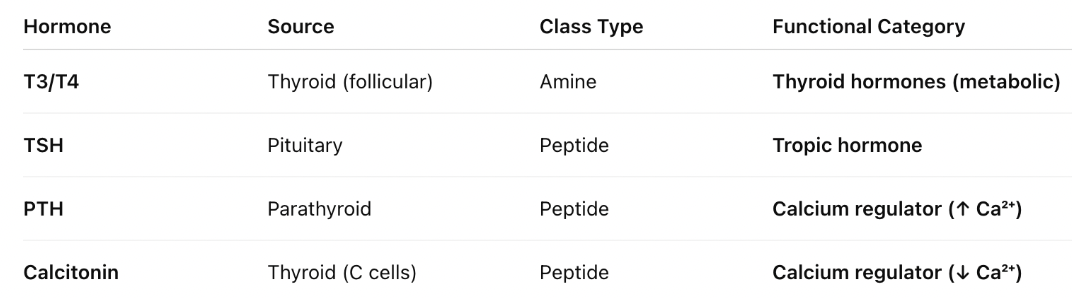
what are all the hormones related to the thyroid?
what is the pathway of Vitamin D?
Skin: UV light converts 7-dehydrocholesterol → Vitamin D₃ (cholecalciferol)
Liver: converts Vitamin D₃ → 25-hydroxyvitamin D (25(OH)D) (circulating inactive form)
Kidney: 1α-hydroxylase (enzyme) converts 25(OH)D → 1,25-dihydroxyvitamin D (calcitriol) (active form)
how does PTH and kidney play a role in Vitamin D synthesis?
kidney - activation site
PTH - regulator of activation’
Low Ca²⁺ → ↑ PTH
PTH → ↑ 1α-hydroxylase activity → ↑ active Vitamin D (calcitriol) → ↑ Ca²⁺ absorption
what is the function of Vitamin D?
increase blood Ca2+
intestine - ↑ Ca²⁺ absorption from diet
bone - works with PTH to ↑ Ca²⁺ release
kidney - supports Ca²⁺ reabsorption
what is the morphology/structure of the adrenal gland? what hormones are released?
adrenal cortex (outer): made of epithelial cells; produces steroid hormones
zona glomerulosa: salt → aldosterone
zona fasciculata: sugar → glucocorticoids (cortisol)
zona reticularis: sex steroids (androgens)
adrenal medulla (inner): functions like modified sympathetic ganglion; produces amine hormones
epinephrine
norepinephrine
what is the relationship between glucocorticoids with innate and humoral/adaptive immune function?
innate → reduced inflammation & decrease activity of macrophages & neutrophils
adaptive → lymphocyte suppression and ↓ cytokine signaling → reduced antibody response and immune coordination
How is glucocorticoid stress response adaptive and maladaptive?
adaptive (short-term): prevents excess inflammation, protects tissues during stress/injury, conserves energy for survival
maladaptive (chronic): long-term cortisol elevation leads to immunosuppression, increased infection risk, and poor wound healing
what is the function of cortisol in daily physiological maintenance?
**maintains homeostasis (baseline regulator) by…
maintains blood glucose
supports normal metabolism (protein, fat)
maintains vascular tone + blood pressure
regulates immune activity
what are the pathologies relating to adrenal glands?
Addison’s Disease (Hyposecretion): low cortisol → leads to fatigue, weight loss, low blood pressure
Cushing’s Syndrome (Hypersecretion): excess cortisol → leads to muscle/bone breakdown, high blood glucose, immunosuppression, hypertension
how is cortisol related to diabetes?
cortisol causes ↑ gluconeogenesis (makes new glucose), ↓ insulin sensitivity, ↑ fat & protein breakdown
elevated cortisol causes ↑ blood glucose level + ↑ insulin requirements (especially during stress/infection)
how is cortisol related to respiratory distress syndrome (RDS)?
cortisol stimulates surfactant production in lungs → reduces surface tension + prevents lung collapse
low cortisol → ↓ surfactant → RDS
how does cortisol relate to congenital adrenal hyperplasia?
adrenal hyperplasia = enlargement of adrenal gland
↓ cortisol production → signals ↑ ACTH → ↑ androgens