Echo Evaluation of Prosthetic valves
1/84
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
85 Terms
What is the first modality to assess prosthetic valves?
Transthoracic Echo is the first modality to assess prosthetic valves
Our assessment will includes reviewing for what? (name 5)
Our assessment will includes reviewing for valvular stenosis, valvular
regurgitation, endocarditis, and aortic dissections, and valve complications
Prosthetic Valve Complications
Complications to consider: name 15
Calicification/degeneration (Bioprosthetic)
Thrombus (mechanical)
Infective endocarditis (vegetation, valve ring abcess, fistula)
Perivalvular leaks
Dehiscence
Stenosis
Pericardial Effusion
Regurgitation
Valve bed abnormalities (pseudoaneuysrm, hematoma)
Pannus
Ventricular dysfunction
Hemolysis/anemia
PPM
LVOT Obstruction
Ventricular Septal Defects
Prosthetic Aortic Valves, Interrogation in
PLAX what do you interrogate of the aortic root?
PSAX what do interrogate and give me an example of a prosthetic valve for the AV
talk about the appostion (the positioning of things or the condition of being side by side or close together.)
want to look for the presence of what two things
sweeping through the valve is necesssary to detect what and explain why
what 3 things you would want assess on the left side knowing there is a prosthetic AV?
PLAX Valve position in the aortic root
PSAX valve shape (TAVRs)
apposition of the valve stent to native aortic tissue
Presence of aortic annular injury or ventricular septal defects
Sweeping through the valve is necessary to detect valve regurgitation as regurgitant jets may not be seen adequately in a single valve plane
LV size, function, and hypertrophy
Prosthetic Aortic Valve
In valve stenosis what is performed in standard windows?
Valve Stenosis (pedoff performed in standard windows)
Prosthetic Aortic Valves:
Low deployment of a TAVI prosthesis:
can limit what of the valve
This increases the risk for what
what function can it affect causing what
can limit anchoring of the valve
This increases the risk for delayed migration of the valve into the LVOTor left ventricle
can affect mitral valve function, causing MR
What the slide is saying (simple)
👉 If the valve is placed too low
➡ It doesn’t anchor (stick) well
➡ So it can move later
🧠 Break it step-by-step 1. “can limit anchoring of the valve”
👉 “Anchoring” = how well the valve stays fixed in place
If it’s too low → ❌ not secured well
Think: loose fit
2. “This increases the risk for delayed migration”
👉 “Migration” = the valve moves after placement
Not immediately
But later on
3. “into the LVOT or left ventricle”
👉 The valve can slip downward into:
LVOT (left ventricular outflow tract)
Or even into the left ventricle
🔥 Put it together
👉 Valve placed too low
➡ Not secured properly
➡ Can slide downward later into the heart
📍 This is exactly what your slide shows (page 9)
⚠ Why this is bad
If the valve moves:
❌ Can block flow
❌ Can cause regurgitation
❌ Can affect mitral valve (MR)
❌ Can require urgent intervention
🧪 One-liner (exam ready)
“Low deployment of a TAVI valve can impair anchoring, increasing the risk of delayed migration into the LVOT or left ventricle.”
🔥 Super simple version
👉 “If the valve is placed too low, it can come loose and slide down into the heart”
Prosthetic Aortic Valves:
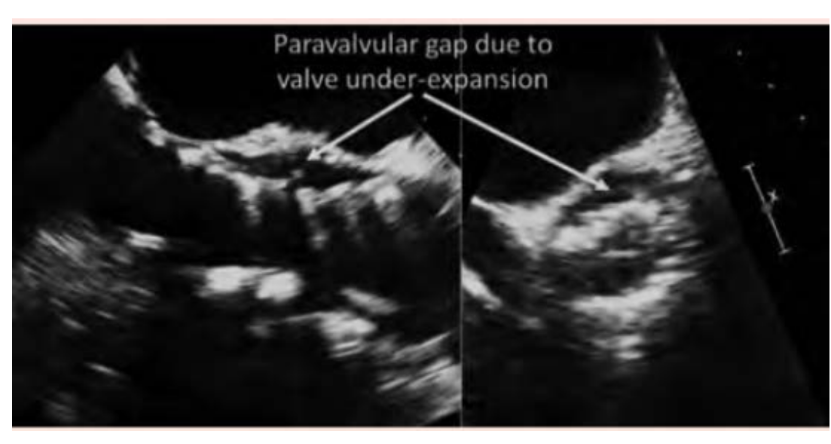
Incomplete expansion of the TAVI valve because of what can result in what 3 things?
Incomplete expansion of the TAVI valve because of calcium can result in
paravalvular and valvular regurgitation and higher valve gradient
Prosthetic Aortic Valves:
Doppler interrogation and Quantitative assessment include what? name 6
peak velocity through the valve (TVI)
mean gradient
EOA
DVI
Contour of the jet
acceleration time
Prosthetic Aortic Valves
Color Doppler evaluation of the AR.
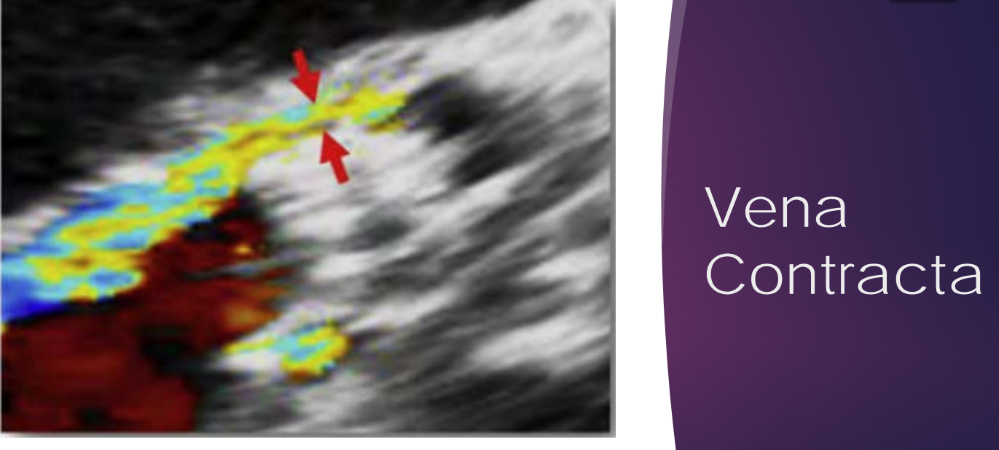
what measurement/things you need to do (3 things to name )
Flow convergence, VC, and proximal jet extension into the LVOT and left ventricle
Prosthetic Aortic Valves
Color Doppler evaluation of the AR.
Limitations of Flow convergence, VC, and proximal jet extension into the LVOT and left ventricle method include what (two things)
Limitations of this method include reverberation and shadowing from the prosthesis
Prosthetic Aortic Valves
Color Doppler evaluation of the AR.
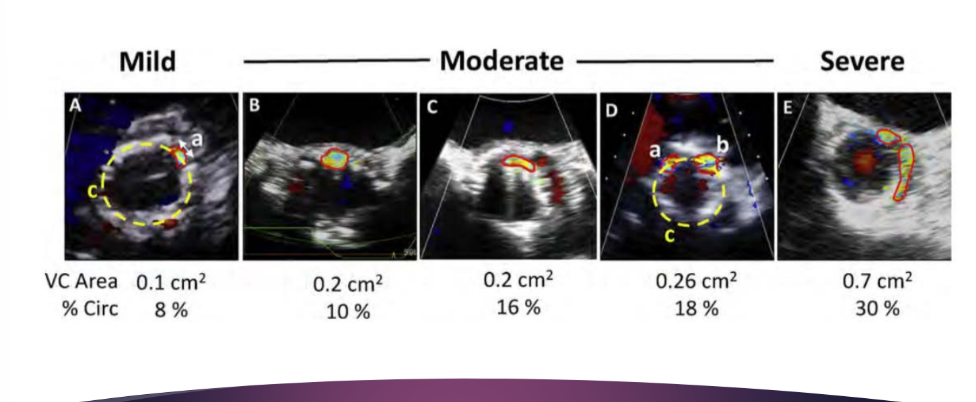
The VC width, area, and circumferential extent could be assessed from a carefully obtained what view?
The VC width, area, and circumferential extent could be assessed from a carefully obtained short-axis view
Prosthetic Aortic Valves
Color Doppler evaluation of the AR.
Measuring the width of an what jet in the what view may overestimate or underestimate ? - which one? regurgitation severity
Measuring the width of an eccentric jet in the outflow tract may overestimate
regurgitation severity
Prosthetic Aortic Valves
Color Doppler evaluation of the AR.
Wall-impinging aortic paravalvular jet may lead to over or underestimation because why?
Wall-impinging aortic paravalvular jet may lead to underestimation because of an unimpressive color Doppler jet area
A paravalvular leak jet that hugs the wall
➡ can look smaller than it actually is on color Doppler
🧠 Break it down 1. “Wall-impinging jet”
👉 The regurgitant jet:
Sticks to the wall of the vessel (aorta or LVOT)
Instead of shooting straight out
2. “Unimpressive color Doppler jet area”
👉 On color Doppler:
The jet looks small / weak / not obvious
3. “Underestimation”
👉 You might think:
“Oh this is mild regurgitation”
❗ But actually:
It could be moderate or severe
🔥 Why does this happen?
👉 When the jet hugs the wall:
It loses energy
It spreads less
It doesn’t show a big color area
➡ This is called the Coandă effect (high-yield concept)
⚠ Clinical mistake
👉 If you rely ONLY on:
Color jet size
❌ You will underestimate severity
💡 What should you do instead?
Look at:
Vena contracta
Flow convergence
Aortic flow reversal
Multiple views
🧪 One-liner (exam ready)
“Wall-impinging paravalvular jets may appear small on color Doppler, leading to underestimation of regurgitation severity due to the Coandă effect.”
“If the jet hugs the wall, it looks smaller than it really is”
what is the severe VC area and % circ?
Greater than 30%
Prosthetic Aortic Valves
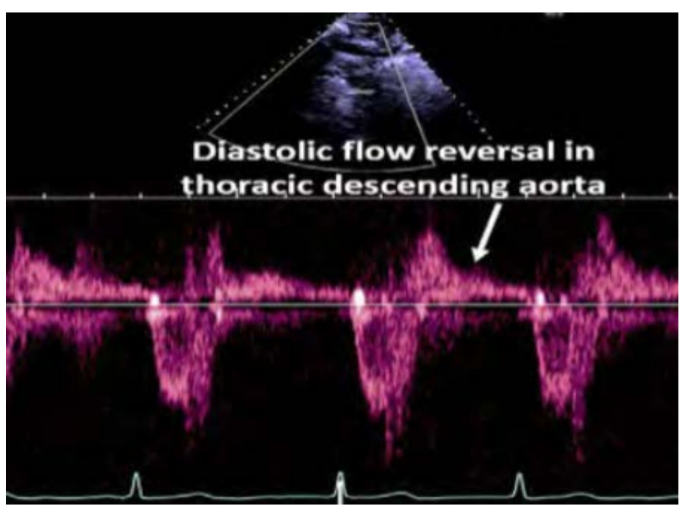
PHT <200 msec or what flow BLANK in the abdominal aorta suggests
the presence of severe regurgitation?
PHT <200 msec or holodiastolic flow reversal in the abdominal aorta suggests
the presence of severe regurgitation greater than 15
Prosthetic Aortic Valves
AR severity may be more complicated because of the presence of combined
what jets? name 4
AR severity may be more complicated because of the presence of combined
valvular and paravalvular regurgitant jets, multiple regurgitant jets, or eccentric jets
Prosthetic Aortic Valves
Differentiate between what 3 things
other causes of elevated doppler gradients such as 3 things should be excluded
what are essential for prosthetic AV
Patients with poor LV function, elevated blood pressures may not show what despite significant stenosis
Differentiate between Stenosis, SVD, or PPM
Other causes of elevated Doppler gradients such as high-flow states,
supra- or subvalvular obstruction, and pressure recovery should be excluded
Comparison to baseline echos and serial echos are essential
Patients with poor LV function, elevated blood pressures may not show high gradients despite significant stenosis
Special Considerations for TAVRs
Special consideration for TAVI; In-stent flow acceleration occurs at two locations, where are these locations?
In-stent flow acceleration occurs at two locations, below the valve and at the
level of the cusps
Special Considerations for TAVRs
Special consideration for TAVI;
LVOT diameter and flow measurements should be obtained immediately where to the stent to prevent over or underestimation of the what by flow acceleration within the stent
LVOT diameter and flow measurements should be obtained immediately
proximal to the stent to prevent overestimation of the EOA by flow acceleration within the stent
Special Considerations for TAVRs
Special consideration for TAVI;
It is recommended that what measurement be used to
assess prosthetic aortic valve stenosis?
It is recommended that one highly flow-dependent (e.g., peak velocity, mean
gradient) and one less flow-dependent (e.g., EOA) measurement be used to
assess prosthetic aortic valve stenosis
Special Considerations for TAVRs VIV
For TAVI ViV,
Note the type and size of both what?
Look for what echocardiographic ViV gradients? (mean gradient of what mmhg) are found in 28% of Patients after ViV
Significant what has also been observed after ViV,with moderate or greater what in 60% of pateints and severe what in 25%
Note the type and size of both the original implanted surgical or TAVI valve and the second implanted valve
Look for elevated echocardiographic ViV gradients (mean gradient > 20
mm Hg) are found in 28% of patients after ViV
Significant PPM has also been observed after ViV, with moderate or greater PPM in 60% of patients and severe PPM in 25%
Special Considerations for TAVRs VIV
Sweeps in both what -axis views are often needed to ensure that all jets are identified?
what-axis views may be needed to determine jet origin. and tell me why?
Sweeps in both the parasternal long- and short-axis views are often
needed to ensure that all jets are identified
Off-axis views may be needed to determine jet origin.
Because of reverberation and shadowing from the prosthesis, posterior paravalvular AR may be obscured with TTE,
Prosthetic Mitral Valves
what valves are prone to pressure recovery from the small orifice between what?
Bileaflet mechanical valves are prone to pressure recovery from the small
orifice between the two tilting disks
Prosthetic Mitral Valves
Bileaflet mechanical valves are prone to pressure recovery from the small
orifice between the two tilting disks, result in a slight over or underestimation of the what by doppler and over or underestimation of what with the continuity equation?
Result in a slight overestimation of the gradient by Doppler and underestimation of EOA with the continuity equation
Prosthetic Mitral Valves
EOA of mechanical mitral valves is in the what range and the mean gradient ranges from what mmhg?
EOA of mechanical mitral valves is in the 2- to 3-cm2 range and the mean
gradient ranges from 2 to 3 mm Hg
Mitral bioprosthetic valves are what only
Mitral bioprosthetic valves are stented only
Mitral bioprosthetic valves are stented only.
they have an expected EOA of 2.2 to 3.5 cm ² and a mean gradient of what mmhg at physiologic heart rate ?
They have an expected EOA of 2.2 to 3.5 cm 2 and a mean gradient of 3
to 5 mm Hg at physiologic heart rate
Prosthetic Mitral Valves
Comprehessive evaluation of the mitral valve prothestis includes: name 8
heart rate
peak early velocity ( E- wave )
Mean gradient
PHT
Presence or absence of significant regurgitation
LV, right ventricular (RV), and left atrial size
Estimation of PA pressure and right atrial (RA) pressure
EOA and DVI
Prosthetic Mitral Valves
Diagnostic criteria of prosthetic mitral stenosis by Doppler
echocardiography remain the same, name 4 Severe numbers
Mean gradient
PHT
DVI
EOA
Mean gradient >10 mm Hg at a normal heart rate
PHT >200 msec
DVI >2.5 (VTI PrMV /VTI LVOT)
EOA <1 cm 2 (EOA = stroke volume/VTI PrMV)
Causes of mitral prosthetic stenosis include: what 4 things
Degeneration
Thrombus
Pannus
Vegetations
PPM is significantly less common in the what valve compared with the what valve
position
PPM is significantly less common in the mitral compared with the aortic
position
Evaluation of MR: MR jets by TTE is frequently limited by what artifacts from the mitral prosthesis?
MR jets by TTE is frequently limited by acoustic reverberation or shadowing from the mitral prosthesis
Evaluation of MR: what is often the optimal view for evaluation of prosthetic MR jets?
Parasternal window is often the optimal view for evaluation of prosthetic MR jets, PLAX
Apical views may be helpful to identify what for MR?
Apical views may be helpful to identify a suspected eccentric regurgitant jet or
paravalvular regurgitation
for MR, Apical views may also provide better visualization of what 5 things
Apical views mayalso provide better visualization of the prosthetic valve
leaflets for identification of vegetation, thrombus, pannus, or leaflet
degenerative changes
Prosthetic Mitral Valves
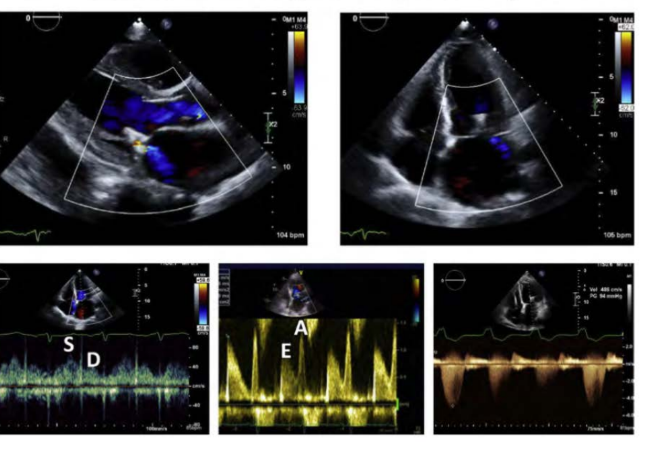
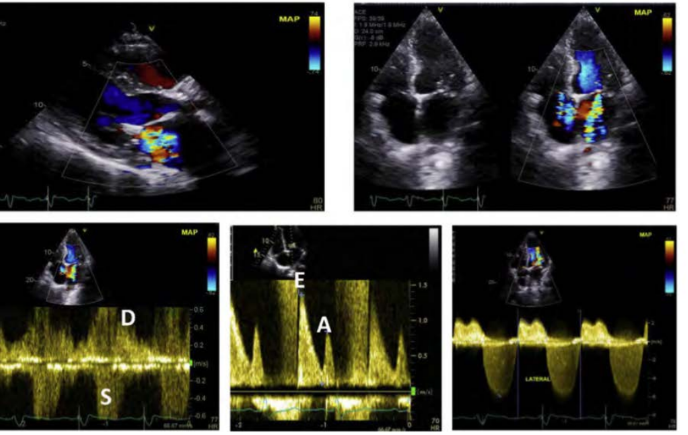
Spectral Doppler is key for evaluation of Mitral Prosthesis Regurgitation, name 7 things
what is the CW MR jet look like
How is the mitral E velocity
how is the systemic output and VTI LVOT despite a Hyperdynamic LV
how is the VTI PrMV/VTI Ratio
a large zone of what seen on the LV sie of the mitral prosthesis ****
a what in pressure compared with previous study
flow of the pulmonary veins
the shape changes from a trigu;nar shape to what
Dense CW MR jet
Elevation of the mitral E velocity (>1.9 m/sec in mechanical valves)
Low systemic output and VTI LVOT despite a hyperdynamic left ventricle
An elevated VTI PrMV/VTI LVOT ratio (>2.5)
A large zone of systolic flow convergence seen on the LV side of the mitral prosthesis
A significant rise in the PA pressure compared with a previous study
Reversal of flow in the pulmonary veins (signifcant MR)
to u shape
First — what do these mean? 👉 VTI PrMV
Velocity Time Integral through the Prosthetic Mitral Valve
= how much blood flow (velocity over time) across the mitral valve
👉 VTI LVOT
VTI in the Left Ventricular Outflow Tract
= forward flow leaving the heart
🔥 What the ratio compares
👉 It compares:
Flow through the mitral valve (inflow)
vsFlow out of the heart (outflow)
⚡ What does > 2.5 mean?
👉 The mitral valve flow is much higher than it should be
➡ This suggests:
❗ Obstruction at the mitral valve
🚨 Why does this happen?
If the mitral valve is:
Narrow (stenosis)
Blocked (thrombus, pannus)
Too small (PPM)
👉 Blood speeds up → VTI increases
💡 KEY concept
👉 High ratio = something is wrong with the mitral valve
Because:
More resistance → higher velocity → higher VTI
📍 From your slide context (mitral valve section)
👉 This is used to identify:
Prosthetic mitral stenosis
Significant dysfunction
🧪 One-liner (exam ready)
“A VTI PrMV / VTI LVOT ratio >2.5 suggests prosthetic mitral valve obstruction or stenosis.”
🔥 Super simple version
👉 “If flow across the mitral valve is way higher than normal compared to outflow → the valve is likely obstructed”
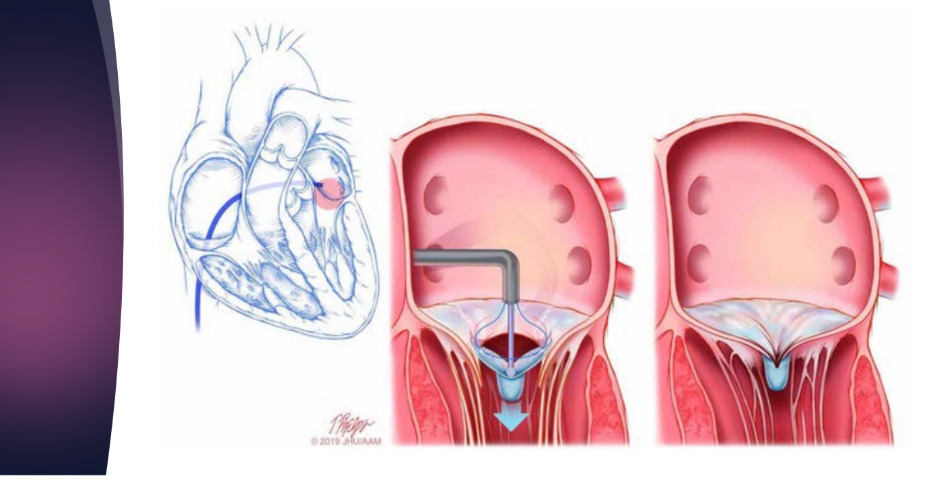
Evaluation of Mitraclip,
approves for what?
converts the MV in to a what MV by clipping the what leaflets
what is it the apparence on echo
Approved for degenerative mitral valve lesions
Converts the MV in to a double orifice mitral valve by clipping
the anterior and posterior leaflets together
echogenic clip
Post Mitraclip evalauation name 5
Peak velocity
Peak pressure gradient
Mean pressure gradient
EOA (planimetry, PHT, and continuity equations)
Severity of MR with native valve recommendations
mild MR after edge to edge MV repair
greater than or equal moderate MR after edge to edge MV repair
Prosthetic Pulmonary Valves
The prosthetic valve is what always in the what position as the native
pulmonary valve, especially when a what is involved
The prosthetic valve is not always in the same position as the native
pulmonary valve, especially when a conduit is involved
Prosthetic Pulmonary Valves, Anatomy of the what 5 things are important to include?
Anatomy of the RVOT and PA as well as RV size, function, and pressures
are important to include
pulmonary valve may be replaced either by a what for
complete repair of a congenital defect or by what
pulmonary valve may be replaced either by a valved conduit for
complete repair of a congenital defect or by a prosthetic valve
Prosthetic Pulmonary Valves, occurring more in what people (age)
Occurring more in younger people
Prosthetic Pulmonary Valves, The most common indication for a valved conduit is what? (condition)
The most common indication for a valved conduit is tetralogy of Fallot
Prosthetic Pulmonary Valves, what procedure for (congenital aortic valve stenosis)
or as part of a Ross procedure (congenital aortic valve stenosis)
Prosthetic Pulmonary Valves, valved conduit is what tissue ( and give me two examples)
valved conduit is biologic tissue (e.g., homograft, xenograft)
Prosthetic Pulmonary Valves
Stented biologic prostheses are generally implanted for what?
Stented biologic prostheses are generally implanted for pulmonary valve
regurgitation
Prosthetic Pulmonary Valves: (Stented biologic prostheses are generally implanted for pulmonary valve
regurgitation)
most commonly occurs in patients who have previously undergone what reconstruction?
most commonly occurs in patients who have previously undergone RVOT
reconstruction
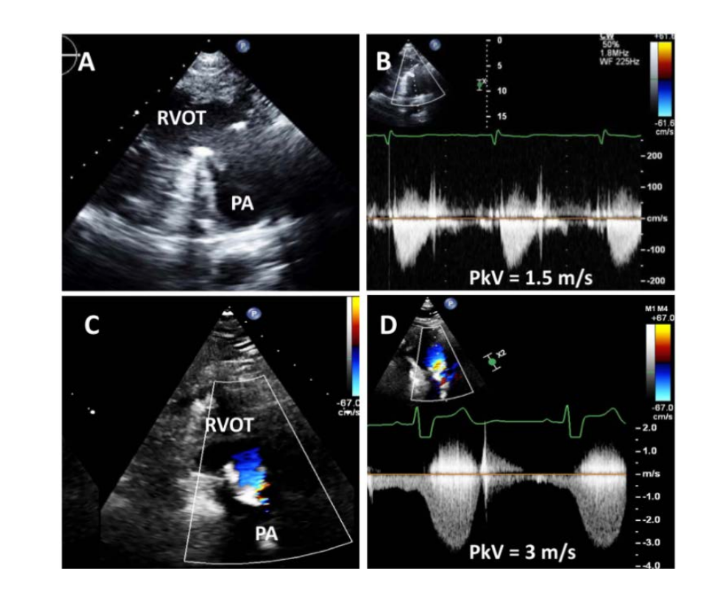
Prosthetic Pulmonary Valves
when evaluating the severity of prosthetic stenosis, that what flow velocities
may be encountered in locations other than the prosthetic valve?
what stenosis may also be present
when evaluating the severity of prosthetic stenosis, that high flow velocities
may be encountered in locations other than the prosthetic valve
Branch vessel stenosis or conduit edge stenosis may also be present
Prosthetic Pulmonary Valves
Echocardiographic assessment of valve obstruction should include what 5 things
what about the prosthesis
observaation of qualitative indicators of what
quantitation of severity of what
any changes from what assessments in…
what does using the jet of TR determine?
Type and size of prosthesis
Observation of qualitative indicators of obstruction (e.g., thrombus, pannus)
Quantitation of severity of stenosis
Any changes from previous assessments in serial examinations
RV systolic pressure should be determined using the jet of TR
Prosthetic Pulmonary Valves
Prosthetic valve failure or dysfunction predominantly manifests as what?
Prosthetic valve failure or dysfunction predominantly manifests as stenosis
rather than regurgitation
Prosthetic Pulmonary Valves
Identifying the location of stenosis is important
Obstruction may occur further along a what rather than at where?
what Doppler is helpful in determining the precise location of obstruction
Quantitative parameters are generally limited to what two things
Obstruction may occur further along a conduit or in the PA rather than at the
valve
PW Doppler is helpful in determining the precise location of obstruction
Quantitative parameters are generally limited to peak velocity and mean
gradient
Prosthetic Pulmonary Valves
Echocardiographic assessment of PR should include: name 5
what of the prosthesis
the presence of relevant anatomic abnormalities such as what two things
quntitation of severity of what
any changes from what assessment….
assessment of the what 3 things during what cardiac cycle is needed?
The type and size of prosthesis
The presence of relevant anatomic abnormalities, such as degeneration or
vegetations
Quantitation of severity of regurgitation
Any changes from previous assessments in serial exams
Assessment of the RV size and interventricular septal position and motion during diastole is needed
Prosthetic Pulmonary Valves
When a valved conduit is present, both what of the conduit and
what of the valve can occur,
what Doppler are used to assist with the evaluation?
Color Doppler demonstrates what flow into the what?
what assist in determining the severity?
When a valved conduit is present, both stenosis of the conduit and
regurgitation of the valve can occur,
Color, PW, and CW Doppler are used to assist with the evaluation
Color Doppler demonstrates diastolic flow into the RVOT
Jet duration and jet width assist in determining the severity
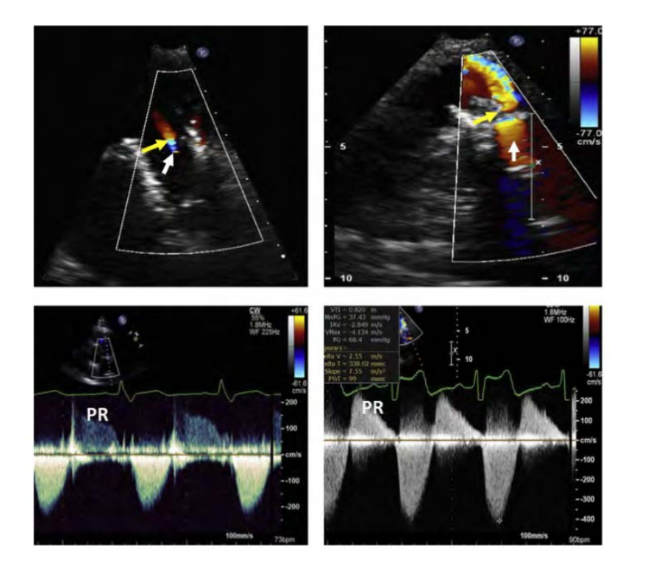
Severe PR has a what jet duration, as the PA and RV diastolic pressures do what
Severe PR has a short jet duration, as the PA and RV diastolic pressures equalize quickly
Prosthetic Pulmonary Valves
what flow in the distal main PA by what doppler is suggestive of at lease what level PR?
Reversal of flow in the distal main PA by PW Doppler is suggestive of at
least moderate PR
Prosthetic Pulmonary Valves
what is also suggestive of severe PR, but this is
also dependent on the compliance of the what
A brief diastolic deceleration time is also suggestive of severe PR, but this is
also dependent on the compliance of the right ventricle
Prosthetic Pulmonary Valves
A comparison of stroke volume obtained just below the PVR and stroke
volume obtained at the aortic or mitral valve can provide a measurement
of what? (in the absence of what?)
A comparison of stroke volume obtained just below the PVR and stroke
volume obtained at the aortic or mitral valve can provide a measurement
of regurgitant volume and fraction (in the absence of AR or MR)
Prosthetic Pulmonary Valves
A regurgitant fraction what % is considered mild, and what % is considered
severe
A regurgitant fraction <30% is considered mild, and >50% is considered
severe
The majority of TV repairs or TV replacements (TVRs) are performed at the time ofwhat surgery, most commonly what surgery?
The majority of TV repairs or TV replacements (TVRs) are performed at the time of
Most commonly mitral valve surgery
Almost 90% of TV procedures in the United States are what?
Almost 90% of TV procedures in the United States are repairs
The majority of TVRs are what
The majority of TVRs are bioprosthetic
Tricuspid Prosthetic Valves
Prosthetic valves and prosthetic rings have different presentations and modes
of failure:
Surgical bioprostheses can fail because of what?
Surgical bioprostheses can fail because of prosthetic stenosis or regurgitation
Tricuspid Prosthetic Valves;
Surgical bioprostheses can fail because of prosthetic stenosis or regurgitation;
the mean time period between what requiring what implantation was many years?
The mean time period between tricuspid bioprosthetic implantation and dysfunction requiring ViV implantation was 12 years
The assessment of prosthetic TV function this involves the evaluation of what 3 things
The assessment of prosthetic TV function thus involves the evaluation of
surgical and transcatheter TV repair and replacement, as well as ViV and
valve-in-ring procedures
Native and prosthetic TV velocity varies with what and therefore multiple cardiac sycles should be pbtained by doppler?
Native and prosthetic TV velocity varies with cycle length and respiration
and therefore multiple cardiac cycles should be obtained by Doppler
Tricuspid Prosthetic Valves
PHT is influenced by what 3 things and should be avoided?
PHT is influenced by heart rate, chamber compliance, and loading
conditions and should be avoided
TVR may fail early or late after what?
TVR may fail early or late after implantation
Echocardiographic evaluation of prosthetic TV function includes;
2D demonstrates what two things of bioprosthetic leaflets or what of one or more mechanical?
what should also be suspected when there is a narrowed, and what velocity color Doppler TV inflow pattern?
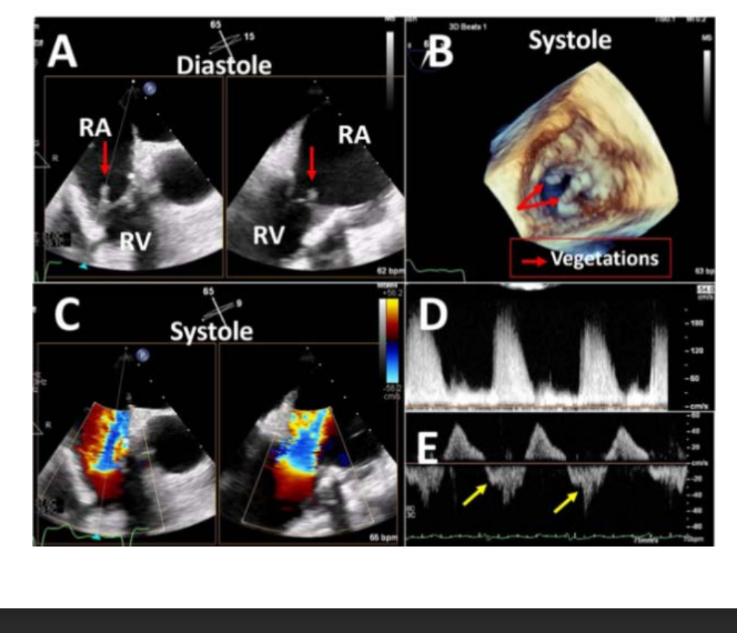
2D demonstrates thickened and/or restricted motion of bioprosthetic leaflets or reduced excursion of one or more mechanical
Stenosis should also be suspected when there is anarrowed, aliased high-
velocity color Doppler TV inflow pattern
Tricuspid Prosthetic Valves
Complications include: name 4
Degeneration
Thrombosis
Pannus
Vegetation
Tricuspid Prosthetic Valves
Mean gradient values of what mmHg have been assoicated with with normal
bioprosthetic function across a wide variety of bioprosthesis and mechanical
valves
Mean gradient values <6 to 9 mm Hg have been associated with normal
bioprosthetic function across a wide variety of bioprosthesis and mechanical
valves
Tricuspid Prosthetic Valves
In patients undergoing ViV or valve-in-ring procedures, a postimplantation
mean gradient of what mm Hg is considered evidence of what
In patients undergoing ViV or valve-in-ring procedures, a postimplantation
mean gradient of >10 mm Hg is considered evidence of stenosis
Mechanical bileaflet TV prostheses for PHT (<130 msec)
PHT is not recommended in the presence of what spectral Doppler contours?
PHT is influenced by what two things?
PHT is not recommended in the presence of rounded spectral Doppler contours
PHT is influenced by both heart rate and right-sided chamber compliance
Tricuspid Prosthetic Valves, DVI equation is what
DVI (DVI = VTI PrTV/VTI LVOT)
Tricuspid Prosthetic Valves,
EOA = calculated by what? Accurate if there is what?
EOA = calculated by dividing the stroke volume in the LVOT by the
diastolic tricuspid prosthetic VTI
Accurate if there is mild or less TR and AR
TR may be either what valvular?
TR may be either transvalvular or paravalvular
Tricuspid Prosthetic Valves TR
Color is needed for what 4 things , what views are needed
Color is needed for flow convergence, VC, and jet direction—as well as jet
effects on the right atrium
Off axis views and Subcostals are needed
what at follow-up may also be indications of a change in
prosthetic valve function? for TV (name 3)
Progressive dilatation of cardiac chambers or alterations in hepatic vein
size and flow at follow-up may also be indications of a change in
prosthetic valve function
Tricuspid Prosthetic Valves
On color Doppler imaging, a large flow convergence, increased VC width
(>0.7 cm), EROA > 0.4 cm2, and regurgitant volume > 45 mL all suggest what level of TR
severe TR
A what CW Doppler tracing with a what shape , when peaking velocity as
well as increased or decreased transvalvular what peak velocity and mean gradient also suggests severe TR
A dense CW Doppler tracing with a triangular, early peaking velocity as
well as increased transvalvular diastolic peak velocity and mean gradient
also suggests severe TR
A DVI of >3.3 in the context of increased or decreased transvalvular gradient and normal or abnormal ? PHT help confirm the presence of significant TR
A DVI of >3.3 in the context of increased transvalvular gradient and normal
PHT help confirm the presence of significant TR
Large flow convergence =
signifacnt regur
Prosthetic Aortic Valves what are the views for interrogation
PSAX, PLAX< A3C, A5C
what is the AV peak velocity that stenosis is present
prosthetic Aortic jet velocity > 3 m/s