Uterine cycle
1/36
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
37 Terms
Formation of Corpus luteum
After ovulation, ruptured follicle collapses → antrum fills with clotted blood → corpus hemorrhagicum
Remaining granulosa + theca cells enlarge, fill with yellow lipid → corpus luteum (“yellow body)
Capillaries invade→ richly vascularized (provides cholesterol for steroidogenesis)
endocrine output of corpus luteum
Progesterone: Dominant hormone; prepares endometrium for implantation; thickens cervical mucus; inhibits uterine contractions
Estrogen: contributes to negative feedback on FSH/LH
Inhibin: contributes negative feedback on FSH (prevents new follicle development
lifespan and fate of corpus luteum
During non-pregnancy:
Without continued LH (suppressed by progesterone/estrogen negative feedback),
CL degenerates → corpus albicans (white scar).
Progesterone + estrogen fall → releases negative feedback → FSH rises → new cycle begins
Lasts 12 days
During pregnancy:
Embryo produces hCG (human chorionic gonadotropin) →
rescues corpus luteum →
maintains progesterone production until placenta takes over ( 3 months)
What do prenancy tests detect
hCG in blood and urine
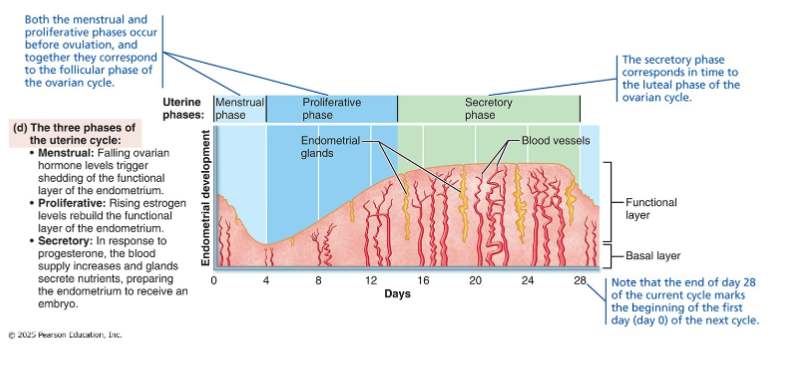
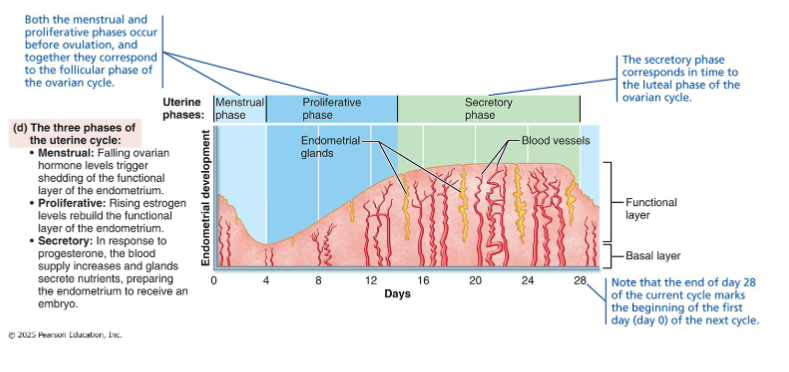
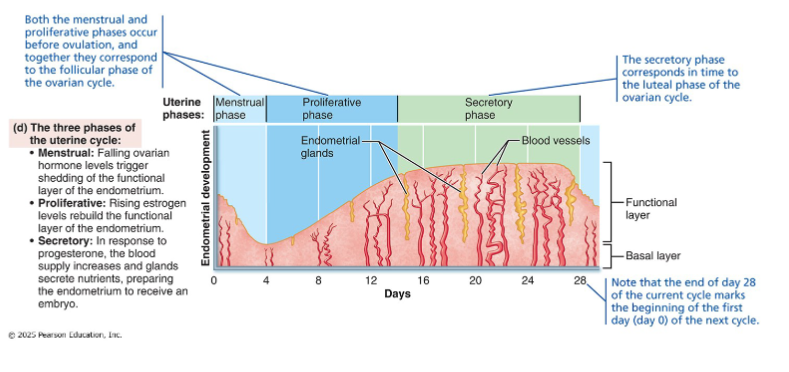
3 phases of uterine(menstrual) cycle
Driven by ovarian hormones acting on the endometrium
Menstrual phase
Proliferative phase
Secretory phase
The uterine cycle is entirely dependent on the ovarian cycle. Remove the ovaries → uterine cycle stops. The endometrium is a hormone-responsive tissue that faithfully reflects what the ovary is doing
Menstrual phase
Occurs on days 1-5 of the 28 day cycle
corresponds to early follicular (ovarian)
Dominant hormone is estrogen
progesterone is at lowest
Processes of menstrual phase
triggered by progesterone withdrawal
Progesterone relaxes myometrium. Its loss leads to contraction
spiral arteries spasm → ischemia(blood flow is cut off) → functionalis dies and detaches
Spiral arteries depend on progesterone to maintain vasodilation
“Menstruation is a vascular event first
Functional layer detaches and is shed (menstrual flow= blood + tissue)
Basalis survives (supplied by straight arteries — unaffected by hormonal withdrawal)
Meanwhile: rising FSH begins new follicle recruitment in the ovary
Proliferative phase
Occurs on days 6-14 days of 28 day cycle
Corresponds to follicular (ovarian)
Dominant hormone is estrogen
Consists of functionalis rebuilding from basalis→ glands enlarge; spiral arteries regrow; endometrium thickens 1-6 mm
Process of Proliferative phase
Rising estrogen from growing follicles drives regeneration from basalis stem cells
Estrogen also upregulates progesterone receptors in endometrium → primes tissue to respond to progesterone in the secretory phase
Cervical mucus thins → forms channels that facilitate sperm passage
Ends with ovulation (day 14)
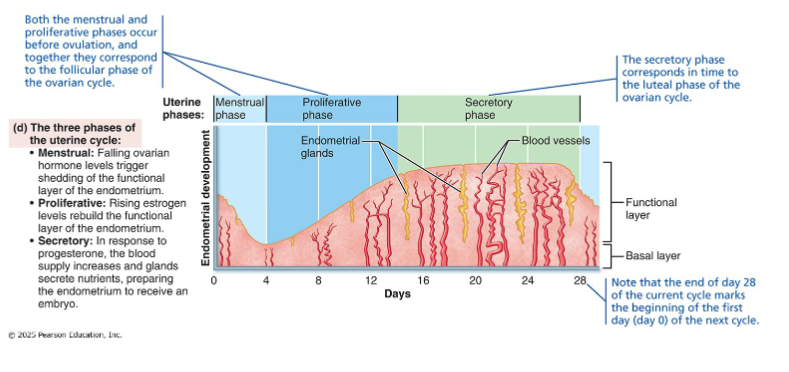
Secretory phase
Occurs on days 15-28 days of the 28-day cycle
Corresponds to luteal phase
Dominant hormone is progesterone
functionalis becomes secretory mucosa→ glands coil and secrete glycogen + nutrients→ spiral arteries elaborate
Processes of secretory phase
Progesterone (from corpus luteum) converts endometrium into secretory mucosa
Endometrial glands actively secrete glycogen + nutrients into uterine cavity (preparing to feed a potential embryo)
Cervical mucus thickens → re-forms cervical plug (blocks sperm + pathogens)
Implantation window: uterus maximally receptive days 20-22 ( 6-7 days after ovulation)
If no fertilization: CL degenerates ( day 24) → hormones drop → ischemic phase (last 2-3 days) → menstruation
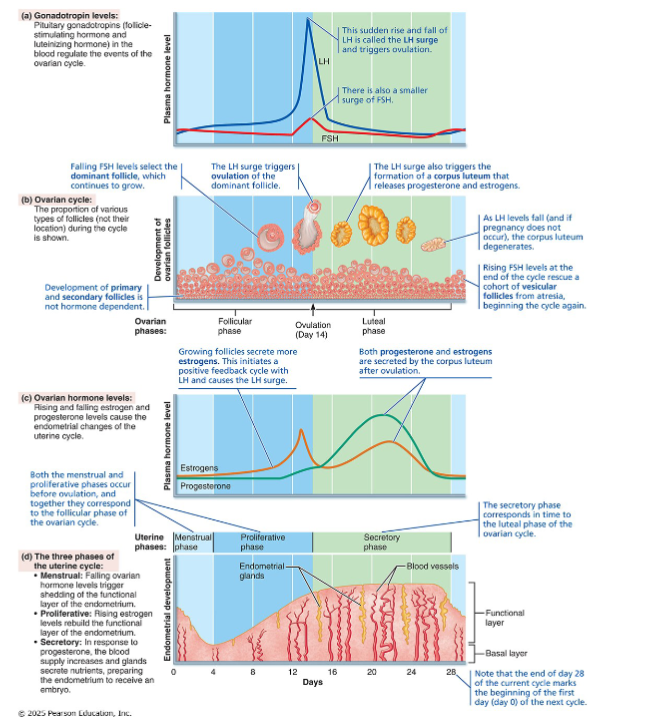
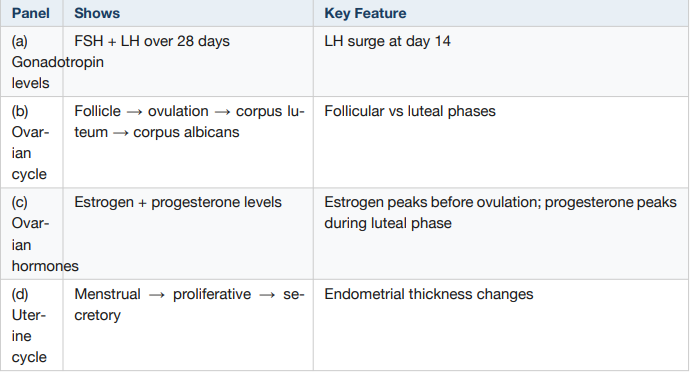
Anchor figure
Four panels, aligned by day, showing how everything connects:
• Panel (a): Gonadotropin levels (FSH + LH) — the pituitary signals
• Panel (b): Ovarian cycle (follicle → ovulation → corpus luteum) — the
events
• Panel (c): Ovarian hormones (estrogen + progesterone) — the output
• Panel (d): Uterine cycle (menstrual → proliferative → secretory) — the
response
• Read top to bottom at any day: what's the pituitary doing? → what's the
ovary doing? → what hormones are out? → what's the uterus doing?
Big coordination
Day by day intergration
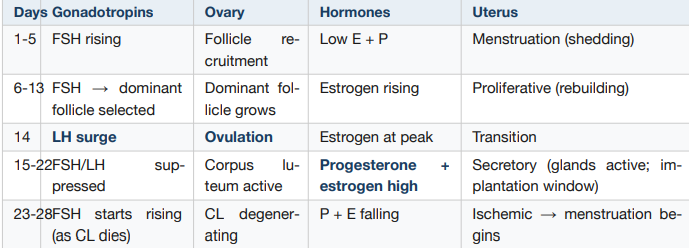
How does uterine cycle depend entirely on ovary
Remove the ovaries → uterine cycle stops
• The endometrium is a hormone-responsive tissue that faithfully reflects what the ovary is doing
• Estrogen builds. Progesterone stabilizes. Without both, the functionalis is shed.
• If pregnancy: embryo produces hCG → rescues CL → progesterone maintained → no menstruation
• If no pregnancy: CL dies → progesterone falls → spiral arteries spasm → menstruation → cycle restarts
What happens if pregnancy occurs during uterine cycle
Embryo produces hCG → rescues corpus luteum →
progesterone maintained →
endometrium maintained →
no menstruation. hCG is detectable in urine/blood = basis of pregnancy tests.
Hormonal regulation at puberty
Same initial event as males: hypothalamus becomes less sensitive to low levels of gonadal hormones → GnRH rises → FSH + LH rise
In females, onset is linked to adipose tissue and its secretion of leptin
A woman takes combined oral contraceptive pills containing estrogen + progesterone continuously. Why does this prevent ovulation?
Continuous estrogen + progesterone → negative feedback on FSH/LH
• → no FSH rise → no follicle recruitment
• → no dominant follicle → no estrogen threshold
• → no positive feedback → no LH surge → no ovulation
• Primary mechanism: ovulation suppression
• Secondary: thickened cervical mucus + thinned endometrium
Estrogen
Reproductive: promotes oogenesis + follicle growth; drives proliferative phase
Secondary sex characteristics (puberty):
Breast development
fat redistribution (hips, breasts)
widening of pelvis
Growth: rapid growth spurt (ages 11-12) → epiphyseal plate closure (full height by 13-15)
Metabolic: maintains low total cholesterol / high HDL → cardiovascular protection
Skeletal: facilitates calcium uptake → bone density maintenance
Progesterone
‘prgenancy hormone’
Uterine: drives secretory phase; quiets myometrium (inhibits contractions — critical in pregnancy)
• Cervical: thickens cervical mucus → forms cervical plug
• Breast: promotes breast development for lactation (with estrogen)
• Metabolic: promotes diuresis; raises basal body temperature
• Clinical use: basal body temperature ↑ confirms ovulation (progesterone from CL)
• Works alongside estrogen — estrogen builds, progesterone stabilizes and
maintains
Puberty in females
Same initial event as males:
• Hypothalamus becomes less sensitive to low gonadal hormones → GnRH rises → FSH + LH rise
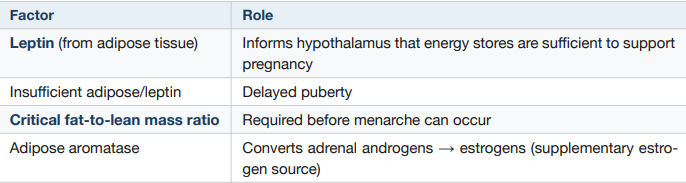
• In females, onset linked to adipose tissue and leptin
• Leptin: adipose-derived hormone that informs hypothalamus energy stores are sufficient for pregnancy
• FSH → estrogen from granulosa cells (via two-cell model)
• Estrogen drives puberty over ~4 years
Leptin-fat connection
Estrogen-driven puberty
lasts 4 years
Growth and maturation of breasts + reproductive organs
Fat redistribution (hips, breasts)
Bone maturation: growth spurt → epiphyseal plate closure (earlier than males → full height by ages 13-15)
Cycles initially anovulatory → first menstruation = menarche
First ovulatory cycle may not occur until months after menarche
FSH-Driven process
FSH stimulates estrogen secretion by granulosa cells (LH provides androgen precursor from theca cells — two-cell model callback
Exercise-induced Amenorrhea
Extreme exercise or eating disorders → low body fat → low leptin → insufficient GnRH stimulus → low FSH/LH → inadequate follicle development → anovulation → amenorrhea (loss of menses).
Result: Loss of estrogen → bone loss (estrogen protects bone density) → osteoporosis-like changes in young women.
An athlete with very low body fat stops menstruating.
Explain the mechanism — trace it from adipose tissue to the uterus.
Menopause
cessation of menses for ≥ 12 consecutive months. Mean age: 51.4 years in North America.
Diagnosed retrospectively
Primary cause of menopause
Depletion of ovarian follicles
— after decades of monthly recruitment + atresia, the follicle supply is exhausted
→ ovary can no longer produce significant estrogen or progesterone.
Hormonal consequence of menopause
Without ovarian estrogen/progesterone → no negative feedback → FSH and LH levels rise dramatically
But no follicles remain to respond → elevated gonadotropins are a hallmark lab finding of menopause
Perimenopause
Transitional years extending from early 40s onward
Ovarian function wanes → cycles become irregular
Estrogen deprivation symptoms begin: hot flushes, insomnia, irritability, fatigue, headaches, mood changes, loss of libido
Post-menopausal effects on genital tissues
Atrophy, vaginal dryness, increased infections
Caused by loss of estrogen trophic support
Post-menopausal effects on Urinary tract
Frequency, urgency, incontinence
Caused by bladder + urethral linings have estrogen receptors
Post-menopausal effects on Breasts
Some atrophy
caused by loss of estrogen stimulation
Post-menopausal effects on Cardiovascular
Increased atherosclerosis + stroke risk
Caused by loss of estrogen’s cardiovascular protection (low cholesterol/high HDL effect)
Post-menopausal effects on Skeleton system
Leads to osteoporosis (accelerated bone resorption)
Caused by loss of estrogen’s bone-protective effect
Hot flushes
Hot flushes are caused by estrogen withdrawal (the change in levels, not the absolute level). Fluctuating estrogen levels disrupt the hypothalamic thermoregulatory center
Female sexual response
PNS-driven arousal: clitoral and vestibular bulb engorgement (erectile tissues homologous to male corpus cavernosum and corpus spongiosum)
Vaginal lubrication from interstitial fluid transudation across vaginal epithelium + cervical mucous glands
No refractory period (unlike males)
Orgasm not required for conception — oocyte capture and sperm transport occur independently of orgasm