Injuries and Burns (Ch, 24)
1/44
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
45 Terms
Most common site of PI
sacrum and heels
Stage 1 PI
- Nonblanchable erythema of INTACT skin
- Usually over bony prominence
- Changes in sensation, temp, or firmness may proceed

Stage 2 PI
i) Partial thickness skin loss with exposed dermis
ii) Blister
iii) Wound bed pink, red, moist

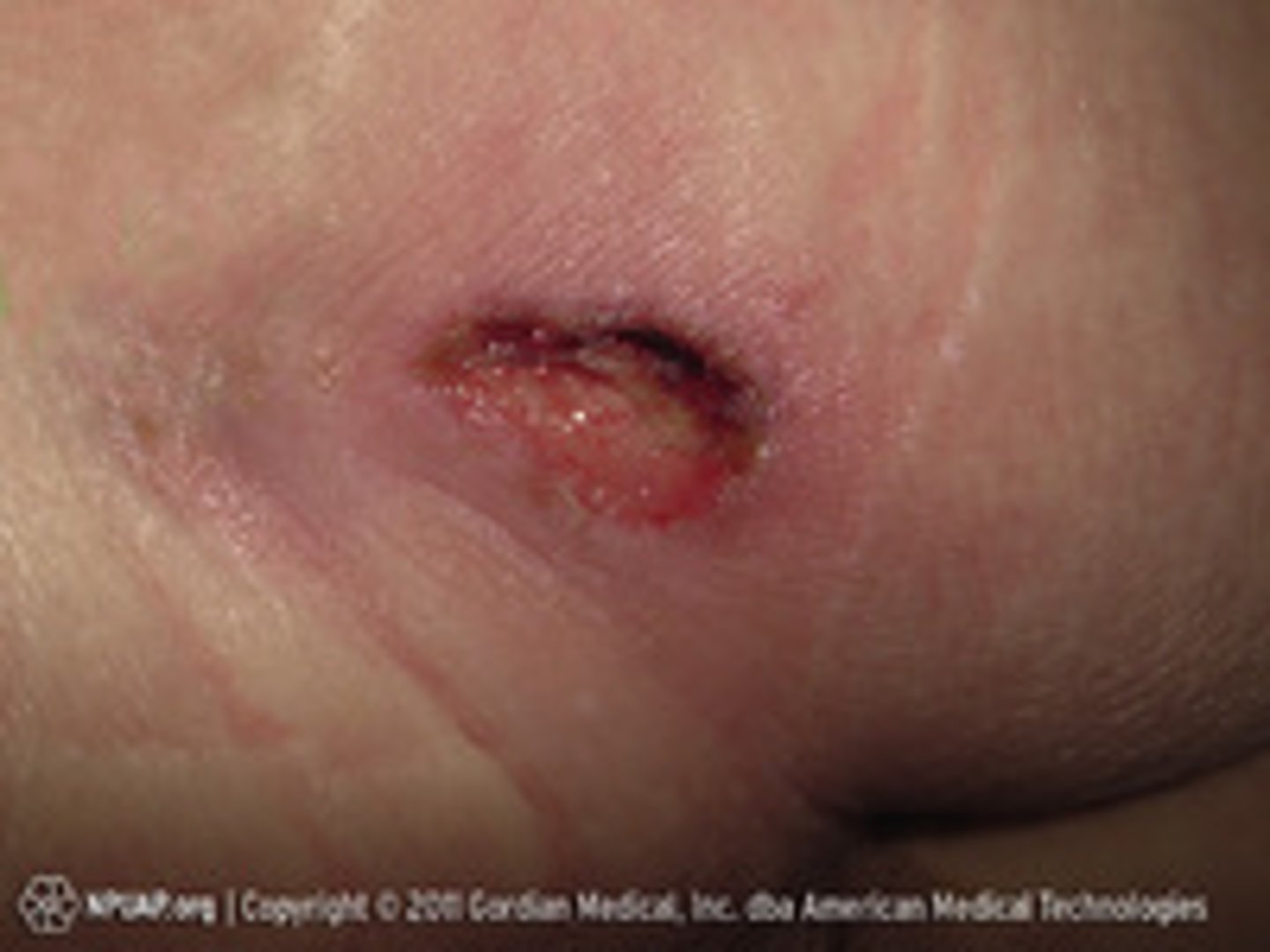
Stage 3
- Full-thickness tissue loss
- Subq fat may be visible, granulation tissue and rolled wound edges, slough and eschar
- Undermining and tunneling may occur
Stage 4 PI
i) Full-thickness skin and tissue loss
ii) Muscle, tendons, ligaments, cartilage, or bone involvement
iii) Slough and eschar
iv) Undermining and tunneling often

Unstageable
i) Obscured full-thickness skin and tissue loss
ii) Base of injury covered by slough or eschar (can't see how deep)
iii) Stage 4 is present after removing slough and eschar (stable, dry adherent, eschar on heel or ischemic limb should NOT be removed)

Deep Tissue Injury
i) Persistent, nonblanchable, deep red, maroon, or purple discoloration
ii) Intact or nonintact skin
iii) Can also be blood filled blister
iv) May eventually reveal tissue injury or resolve without tissue loss

Thermal Burns
i) Most common
ii) External heat source (flame, scald, hot material)
iii) Severity depends on temp, length of time in contact, location, and skin thickness
Chemical Burns
i) Acid or alkaline or organic compound
ii) Absorbed (quickly remove chemicals and clothes) , inhaled, or ingested
iii) Can continue to cause tissue damage long after initial exposure
Electrical
i) Electrical burns result from intense heat generated through electrical current
ii) Severity depends on voltage, tissue resistance, pathway of current, and length of time
iii) Iceberg effect: often hard to determine extent of injury
Electrical Priority
i) PRIORITY: stabilize the C-spine -> ABCs -> vitals -> contact points
(1) Electrical burns can cause muscle contractions that break bones
(2) Respiratory and metabolic acidosis risk
(3) AKI and rhabdo are concerns
Severity of Burns
Burn Depth
Extent of Burn
Location
Risk Factors
Associated Injuries
Burn Depth
(1) Depends on temp of agent, duration of contact, thickness of epidermis and dermis, blood supply to area
1. Superficial Partial Thickness
2. Deep partial thickness
3. Full thickness
(1) Superficial Partial Thickness (1st Degree)
(a) Red, blanches, mild swelling, NO BLISTERS
(b) Ex. sunburn
(1) Deep Partial Thickness (2nd Degree)
(a) Fluid filled vesicles, red and shiny, wet, moderate damage
(b) SEVERE pain d/t nerve damage
(1) Full Thickness (3rd and 4th Degree)
(a) Dry, white/brown charred, leathery
(b) NO PAIN (burnt all nerves)
(c) Muscle, tendon, and bone involvement
(d) Surgery to tx
Extent of Burn
(1) Calculated in relation to total body surface area
(2) Important to know for tx and fluid resuscitation
Location
(1) Neck, face and torso: concerned about gas exchange and chest movement
(2) Extremities: perfusion problem
(3) Hands/feet: mobility and self care
(4) Buttocks and perineum: infection risk
Risk Factors
(1) Chronic preexisting diseases
(2) PVD + DM = poor wound healing
Referral to Burn Center if...
(1) Partial thickness burns >10%
(2) Hands, face, feet, genitals, major joint burns
(3) Electrical burns
(4) Bad trauma
(5) Children
Phases of Burn Care
1. Prehospital and Emergency Care
2. Emergent Phase
3. Acute Phase
4. Rehabilitation Phase
Prehospital and Emergency Care
On scene where injury occurred
(1) ABC's, stabilize VS and airway
(2) Large bore IV access
(3) Neuro, disability, physical trauma assessment
(4) Exposure assessment (remove clothing)
Emergent Phase concerns
(72 hours)
Concerns are hypovolemic shock and edema formation
(1) Hypovolemic Shock: shift of fluids out of blood vessels + increased capillary permeability -> decreased intravascular volume -> decreased preload, blood becomes viscous (increased Hct), K and Na imbalance, hemolyzed RBCs release into circulation (increased Hbg and myoglobin block renal tubules and cause AKI)
(1) Also concerned about infection risk d/t skin loss
S/S of Emergent Phase
(1) Hypoxia (decreased LOC or can be AO4 before intubated)
(2) Fall/trauma
(3) Anxious
(4) Shivering
(5) Pain (unless full thickness)
Complications of Emergent Phase
Respiratory
Cardiovascular
Renal
Respiratory Complication
Inhalation Injury
(a) Upper is above the glottis: mucosal edema
(b) Lower: airway inflammation + edema = PNA and atelectasis
Smoke Inhalation: Sx and Tx
(a) SMOKE INHALATION IS BIG PREDICTOR OF MORTAILITY AND IS A PRIORITY
(i) Sputum, respiratory distress (agitation and anxiety), bright cherry red
(ii) Provide 100% humidified oxygen
Cardiovascular Complications
Decreased CO and perfusion + VTE risk + Dysrhythmias
(a) Tx: Escharotomy to cut through eschar to restore circulation to compromised extremities
(b) VTE risk= heparin and lovenox
Renal Complications
AKI
(a) Pre-renal d/t hypovolemia
(b) Intra-renal d/t myoglobin and hgb blocking renal tubules
Emergent Nursing Management
- AIRWAY #1
- F/E Balance
- Wound Care
- Drug Therapy
- Nutrition
AIRWAY: Emergent Phase
(a) AIRWAY #1: high fowlers, 100% O2, early intubation and ventilatory support, ABGs
(i) If face/neck burns are present intubation may be delayed 1-2 hours
(ii) Extubate once facial/neck edema gone
F/E Balance : Emergent Phase
>20% burns = 2 large bore IV or central line FAST
- Parkland Baxter
- Foley with hourly UO + watching for fluid overload
- Will always have arterial line, not BP cuff
**Electrical burns have increased fluid needs to prevent AKI (mannitol to increase OU and continuous dialysis needed) -> want 75-100mL/hr
Wound Care : Emergent Phase
(i) Trolley bath, 85 degree rooms, PPE for infection risk, mild cleansers and cloths for debridment
Drug Therapy: Emergent Phase
1. Analgesics (multimodal long and short acting)
2. Sedative and antianxiety
3. Music distraction
Nutrition: Emergent Phase
(i) Increased proteins and calories d/t hypermetabolic state
(ii) Always use enteral when you can
Acute Phase
i) Begins with fluid mobilization and subsequent diuresis and continues until wounds are nearly healed
Acute Phase S/S
(1) Wounds starting to heal
(2) More pain d/t therapy and dressing changes
(3) Fatigued
(4) F/E balancing
Acute Phase Complications
(1) INFECTION! -> sepsis is leading cause of death
Acute Phase Nursing Managment
(1) Wound care: cleaning and debriding, decrease infection risk, graft care
(2) Excision and Grafting: abd and thigh most common donor sites
(3) Pain management: premedicate, multimodal
(4) PT/OT: prevents contractions
(5) Nutrition: increase calories and protein, daily calorie count, I&O
Rehabilitation Phase
i) Wounds have nearly healed, patient engaging in some level of care
ii) Goals: work toward resuming a functional role in society and rehabilitate from and functional or cosmetic post-burn surgeries and procedures
S/S of Rehabilitation
(1) Wounds heal spontaneously from surgery
(2) Scarring
(3) Sensitive to temp, blisters, skin tears
Complications of Rehabilitation
(1) Contractures: good positioning and exercise
(2) Hypertrophic scarring
Rehabilitation Nursing Managment
(1) Involve caregivers in wound care
(2) Instruct when to contact burn team
(3) Emotional and physical support
Rule of Nine's
a) Used to determine EXTENT of burn
i) Head: 4.5% (front and back)
ii) Torso (Chest/Abd/Back): 18%
iii) Arms: 4.5% each (front and back)
iv) Legs: 9% each (front and back)
v) Genitals: 1% (front only)
Parkland (Baxter) Formula
a) 2mL LR per kg per %TBSA = total fluid requirments in first 24 hours
b) ½ of the total first 8 hours, ¼ of total in second 8 hours, ¼ total in third 8 hours