Blood sampling and assays
1/100
Earn XP
Description and Tags
Weeks two ENI - monday content
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
101 Terms
What is the difference between plasma and serum?
serum is blood that’s been allowed to coagulate, then centrifuged
plasma is blood that we’ve added an anti-coagulant to, then centrifuged
Why may we use serum for a blood sample - 3 reasons
chemical constituents in the circulation can be measured
no clotting factors
antibodies - serology
How do we collect a serum sample?
leg coagulation take place
centrifuge
remove liquid supernatant
use plain glass/plastic tube OR
ones with clot activators/gel that forms a barrier between cells and serum (no need for an additonal transfer tube)
Why may we use tubes containing gel for a sample?
serum/plasma - when centrifuged allowed a barrier between cells and serum/plasma so we don’t need an additonal tube for testing/transfer
Why may use use a whole blood sample?
counting cells - haematology
certain cellular chemistry - GSH-Px
How do we collect a whole blood sample?
tube that contains anticoagulant to stop blood clotting
anticoagulant is either dry powder coating/liquid (beware of dilution)
Why may we use a plasma sample?
test chemcial constituents in circulation e.g. fibrinogen
How do we obtain a plasma sample?
use a tube with an anticoagulant (with desired effect)
anticoagulant either a powder/liquid (beware dilution)
centrifuge and remove liquid supernatant from cells
others:
tubes with beads to help mix anticoagulant
tubes with gel that forms a sealant barrier b/w cells and plasma

What are the 3 layers in this sample, is this plasma or serum?
plasma, buffy coat, rbcs
PLASMA sample

What are the three layers here
serum
gel
blood clot
How do (in vitro) anticoagulants work?
calcium binding
heparin through anti-thrombin
How does calcium exist in blood?
ionised (iCa)
Albumin bound
complexed
What is EDTA
Calcium chelator (grabber)
irreversibly binds to calcium
How does citrate act as a calcium chelator
forms ionic complexes with iCa
reduced iCa below that needed for coagulation cascade
reversible
Give an example of when we use citrate as an anticoagulant
transfusion - along with glucose and adenine to support RBCs
How can we reverse the effects of citrate?
add Ca back to sample
How is citrate often found in tubes, what do we therefore need to consider with our sample?
liquid
dilution correction factor
How does oxalate work as a calcium chelator?
most commonly found mixed with fluoride
traps Na and K - therefore can’t use this anti-coagulant if we want to sample these ions
Outline fluoride as a calcium chelator
usually with oxalate as the Ca binding anticoagulant
inhibits glycolysis
preserves glucose in sample if posting
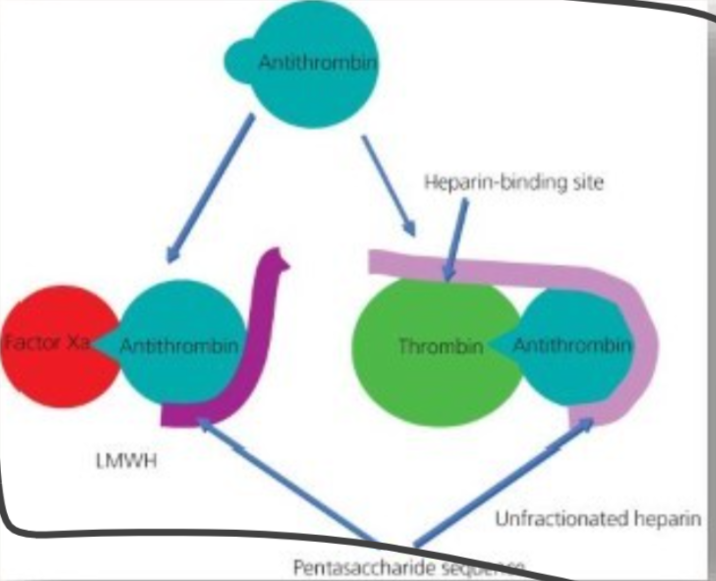
How does heparin work as an anticoagulant
indirect anticoagulation
depends on presence of: anti-thrombin III (AT)
promotes AT ability to bind Factor Xa
locks AT and thrombin (IIa) together
Why is heparin often used in blood samples?
usually Li heparin
therefore doesn’t affect ability to measure Na or K without interference
also recommended for bird/reptile haematology too
What are 3 tube types that promote coagulation
plain glass/Z serum
clot activator tube (CAT)
serum separation tube with gel (SST)
What are 4 tubes that impede coagulation?
sodium citrate (fill to line)
EDTA (K2/K3)
Na/Li heparin
NaF - K oxalate
For each of these tube types, why is tube fill important?
EDTA
Citrate
Liquid anticoagulants
osmotic effects, under-filled tubes → cell shrinkage
need to know how much calcium required to overcome clotting. Citrate in concentration needs to be known precisely. Depends on filling volume expected
anti-coagulant solution as a liquid, need to know vol for dilution factors
which sample do we always do last?
EDTA
what are doughnuts/beads used for in blood sampling?
mixing/even distribution of additives
How do we ensure our sample is mixed properly?
gentle tipping back and forth - don’t want to cause haemolysis
What sample can’t be analysed by a cell counter?
clotted haematology
What coagulation sample can’t be analysed?
clotted citrate coagulation
What anticoagulant/sample do we want to use for:
most clinical chemistry
haematology of whole blood
glucose by mail/delayed analysis
coagulation?
serum and LiHep
EDTA
OxF
citrate
For each species, what size needle to we tend to use?
cat
dog
horse
23-21G, 5/8 inch
21G - 5/8 or 1 inch long
18-20G - 1 inch
How do we prepare a site for blood withdrawal?
clip the area
clean with chlorohexidine 4% (hibi scrub)/10% povidone iodine solution
squirt 70% surgical spirit onto the site
use cotton wool/gauze swabs
may use gloves (re-sterilise site each time you touch without gloves)
What are the 3 veins we can use for a blood sample?
jugular
cephalic
saphenous
How do we take a cephalic blood sample?
clip fur
restrain foot
hibiscrub with cotton wool - check to see if dirty
surgical spirit
feel vein and occlude
clean again
angle the syringe at 35 degrees, bevel pointed dorsally
check blood has entered the needle, then draw back gently
place lid back on needle, remove into sharps bin
place droplets into each bood sample tube (prevents contamination of any coagulants, therefore affecting future tests)
What angle do we want to enter the jugular at?
30 degrees upwards
How do we make the saphenous vein obvious?
cusp behind the knee and apply downwards pressure - keep leg off ground
vein should occlude and become visible
For vacutainer collection for a horse:
what vacutainer needle size
other equipment
how does it work?
18-20G
needle holder and appropriate vacutainer
Method:
attach needle to the vacutainer (has an internal and external bit)
hold the vacutainer by the flange with the selected tube
insert the needle as usual, once blood shows in the vacutainer, click the tube in place and take sample.
What equipment is needed for a blood sample in horses?
20G needle
10-30ml (usually) syringe
appropriate sampling tube/vacutainer
How do we perform a jugular blood sample?
locate the jugular groove between the brachiocephalicus and sternocephalicus
occlude more caudally
avoid the lower third of the area (the carotid artery is also present)
enter at a 30 degree angle upwards
Where do we take a blood sample from a cow?
jugular - in a crush, either with a halter on or nosing
tail vein
How do we take a blood sample from the tail vein?
raise tail up (supporting ventrally with hand in a V-shape)
palpate the vein in the tail groove
insert needle perpendicular to the tail
once blood present in needle head, draw back/click tube into vacutainer
When do we recap a needle when taking a sample from a cow?
at a safe distance
Where can we identify the jugular vein in a fully wooled sheep?
look for the wool break
what is the grey bit present on some needles?
haemoguard
what do we need to consider when taking a blood sample, relating to obtaining relevant data?
TYPE OF DETECTON METHOD USED
where to get it tested - lab/in house
what are 4 detection methods for assays?
colourmetric - measure colour change
turbidometric - measure cloudiness
fluorometric - light excitement
immunoassay - antibody/antigen, RIA/ELISA
How do we ensure we measure the correct substrate in a reaction e.g. A +B → C + D and required E and F (enzyme and cofactor)
ensure what is being measured is the limiting reagent
everything else must be in excess
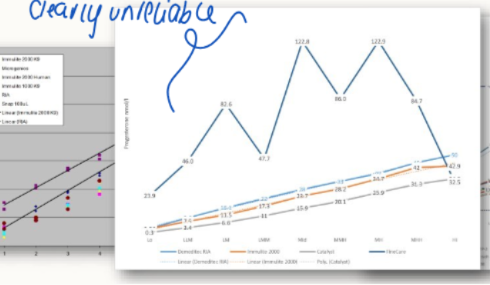
For most routine chemsitries how many calibration points are there?
Are there any concerns with this?
1
yes, not necessarily reliable (if calibration goes wrong, results will be wrong).
DOESNT WORK FOR HOMRONE
What are 4 components of immunoassays
antibodies
tracer
detection systems
separation
what antibodies are used in immunoassays?
Polyclonal or monoclonal
needs to react with hormone in species of interest
what is a tracer in an immunoassay?
an enzyme/radioactive tag on molecule/antibody
What separation is needed in immunoassays?
need tracer signal that’s reacted with hormone separated from which hasn’t
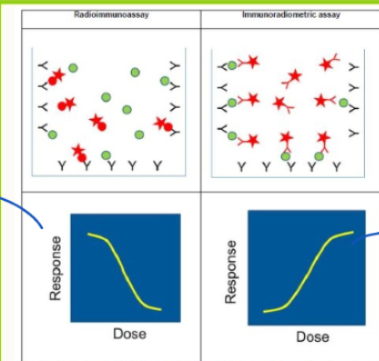
What is the dose/response curve for:
Radioimmunoassays
others e.g. ELISA
-ve response curve - inverse relationship
+ve response curve
Why may we choose to use an ELISA over an RIA?
ELISA avoids complexities of handling radiation
What is chemiluminescence?
enzyme induced light emission
causes a light induced reaction rather than colour change => non-specialist lab common practice
How many calibration points do there tend to be in reference lab results? Is this good/bad?
multiple
improves performance of the test, good thing
How do we know that it’s okay to use results?
validation
imprecision (how closely results match if we keep repeating the test)
accuracy (how far away from real result, ours is)
species differences
quality control

How do we measure imprecision?
Coefficient of variation (CV%) = %SD/mean
varies across range of concentrations
How does the imprecision of immunoassays compare to colouimetry?
Immunoassays - 3-10% (hormone results just less precise)
Colourimetry: creatinine <2%, electrochemistry for K+, <1%!
What can we use accuracy to compare?
different results of different methods
harder to compare against true gold standard
State advantages and disadvantages of reference lab testing
quality assurance and QC taken care of
daily or more frequent → cheaper?
slower (next day)
validated precise and accurate methods
inspected annually if accredited
State advantages and disadvantages of in-clinic lab
validation check responsible by in-clinic lab
may be less precise/accurate
QC responsibility
interpret, spot errors and understand results yourself
quicker
more expensive ??
Rules of shipping blood samples?
less than 50ml
primary receptacle - leak proof
secondary packaging - leak proof
absorbent material b/w primary and secondary (must be able to absorb contents in whole)
outer packing
must pass 1.2m drop test
not smaller than 100mm by 100mm
what paperwork should be included with a blood sample?
Submission form:
- who you are
contact details
address/contact
desired tests
animal ID, species, age, breed
sample type
client ID
dates taken and postedmaybe some history/reason for sampling
may able to be an electronic transfer of information
What should we use to write on our samples?
ideally a waterproof marker, easy to read
what is the UN3373 label?
not known to have hazardous agents in them
used for transporting blood - P650
what is the number for infectious category A substance?
UN2814 (affect humans) or UN2900 (affects animals)
How do we use lab tests to define a diagnosis?
reference intervals
interpretative thresholds (diagnostic cut-offs)
+ve/-ve tests
what is a false-negative
a test restuls for a patient that is actually ill, however their measured level of xyz is low enough to clash with healthy levels
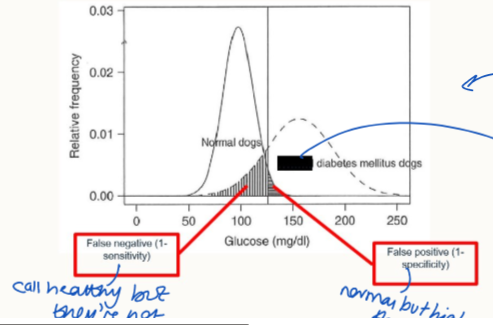
What is a false positive result?
a result where a healthy patient has a naturally higher level of xyz, but is not unwell. Found within the range considered diseased, but not.
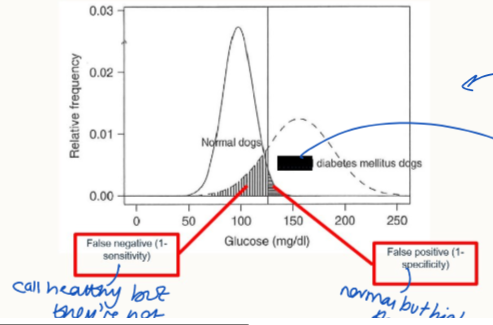
What is sensitivity?
proportion of animals with a disease that yield a positive test result
ability to identify diseased individuals
high sensitivity = minimise false negatives
What is specificity?
proportion of animals that don’t have the disease that yield a negative result
ability of a test to identify individuals without disease
high specificity = good confirmatory test
How are cut-offs determined?
balance between specificity and sensitivity
often sacrifice one for the other
How is specificity and sensitivity determined?
one must have the condition - diseased = need a gold standard test to determine SENSITIVITY
one group must not have the condition = healthy = needs similar age and presenting features to diseased group = SPECIFICITY
need lots of animals in the group = more reliable results.
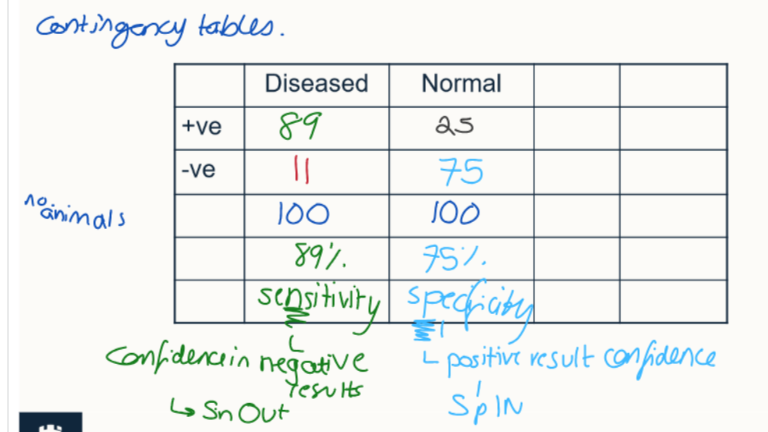
Outline how contigency tables work
show diseased vs normal animals
+ve and -ve results for the test
helps determine specificity and sensitivity
What is a screening test
apply to a large population for some who may have mild signs/asymptomatic
don’t mind a few false positives - check further to ensure they do have it
there’s a HIGH SENSITIVITY (LOW FALSE NEGATIVE RATE)
What is a confirmatory test?
‘‘diagnostic test’’
ensure animals that test positive do have the disease
may be some false negatives but HIGH SPECIFICITY (LOW FALSE POSITIVE RATES)
Consequences of bad sensitivty?
higher false negatives
diagnosis missed
may re-present
outbreak may worsen in epidemic
costs (financial, life, welfare, emotional)
Consequences of bad specificity?
higher false positives
unnecessary lifelong therapy (e.g. endocrine)
unnecessary euthanasia
costs (financial, life, welfare, emotional)
What is prevalence?
proportion of animals in the tested population that have the condition
pre-test probability
How can we affect pre-test probability?
widespread healthy population screen for an infectious disease - low pre-test probability
only testing in animals for disease that have several relevant clinical circumstances - high pre-test probability
what is LDDST a test for?
— hyperadrenocorticism/Cushing’s
As prevalence increases what happens to:
POSITIVE predicted value
INCREASES - more likely that a positive result is truly positive
as prevalence falls what happens to negative predicted value?
increases
if the disease is rare in the tested group, negative more likely to be true
In terms of positive results:
what tells us if we can believe the result?
what has influence on PPV?
PPV of low specificity tests?
PPV of high specificity tests?
acronym?
PPV
specificity and prevalence
poor, except when prevalence is really high
good PPV even at low prevalence
sPin
In terms of negative results:
how do we know if we can trust the result
what has an influence on NPV
NPV of low sensitivity tests?
NPV of high sensitivity tests?
acronym?
look at NPV value
prevalence and sensitivity
poor except when prevalence is very low
good even with high prevalence
sNout
what kind of tests use:
sensitivity
specificity?
screening
confirmatory
Relevance of specifcity/sensitivity in endocrinology?
diagnostic tests are poor for endocrine diseases
booth physiological and pathological causes for lots of conditions, false positives are common (low specificity)
How can we mitigate problems of diagnostics in endocrinology?
look at response
we can stimulate xyz to produce more hormone
we can suppress using principle of negative feedback
we can monitor blood concentrations to see if they change to pathological levels
Case 1
A 15yo cat is brought into your practice, as her owners are worried that she has lost weight even though she has a ravenous appetite. They have also noticed her drinking more.
On physical examination she is underweight (BCS 2/5) and has an unkempt coat. She is tachycardic (HR 200 bpm) with a gallop rhythm noted on auscultation. The owner is happy for you to investigate further.
Your differential diagnoses at this stage include: Hyperthyroidism, diabetes mellitus, renal insufficiency/failure

From the information available and blood tubes on display
1. Select the appropriate blood tube for collection.
2. Select the needle and syringe to collect the sample.
3. Where would you take the sample from?
We want to assess biochemistry:
renal function: serum (plain/gel) or LiHep
glucose: FOx OR LiHep
Total T4: plain Z/serum gel
Haematology: EDTA
23G, 2ml syringe (look at condition of cat, poor, don’t want to take lots of blood from it)
jugular (preferred) or cephalic
Case 2
A 10yo FE Lab cross is brought

in by her owners as they are concerned about her increased drinking and bed wetting. She is overweight (BCS 4/5) making abdominal palpation difficult, but the owners say she has been losing weight recently and vomiting.
Clinical examination: You note bradycardia (HR 56) with weak peripheral pulses and that she is continuously panting. There is mild muscle atrophy, to which her owners say she has been slowing down but they think this is due to her age.
Your differential diagnoses at this stage are:
· Hypercalcaemia
· Diabetes mellitus
· Diabetes insipidus
· Renal insufficiency/failure
· Cushing’s disease
· Addison’s disease
· Pyometra
· Liver disease
From the information available and blood tubes on display
1. Select the appropriate blood tube for collection.
2. Select the needle and syringe to collect the sample.
3. Where would you take the sample from?
Biochemistry:
renal and liver: serum or LiHep
glucose: FOx or LiHep
haematology: EDTA
21G needle and 5ml syringe
jugular, cephalic
1. Coughing horse
You are called to an equine livery yard where more than one horse has begun coughing over the past few days. You suspect equine influenza and decide to take acute serum samples for antibody detection from several horses on the yard.
which vacutainer tube will you use?
how long should you allow blood to clot for serum separation
how soon will you expect to return and collect a convalescent serum sample?
plain Z or CAT
at least 30 mins, the longer the better. Practically, takes longer than 30 mins to get from yard to lab anyway
10-14 days
2. Suspected Equine Pituitary Pars Intermedia Dysfunction (PPID)
You have been called to visit a pony that is suffering from laminitis. The owner has noticed that the pony has begun to drunk more water while it is stabled recently. You decide to check for endogenous ACTH.
Which of the tubes will you select in this case?
How will you process the sample?
EDTA plasma
centrifuge as soon as possible, transfer supernatant and discard red cells
What type of tests requires a citrated blood sample?
Coagulation test e.g. PT and aPTT
what are two things that are vital to do when collecting blood for a citrated sample?
fill to indicated mark or allow vacutainer to fill completely if no mark and mix tube after (gentle inversion 5-10x) collection
C. Farm animal blood sampling
Case 1
You visit a farm, the Holstein- Friesian Dairy cows have poor fertility as indicated by a declining conception rate. On inspection you notice the cows have a longer coat that expected with the black hair over the ribs in particular having a reddish hue, the cows also have some hair-loss around the eyes giving a spectacled appearance. You suspect that this could be a nutritional, mineral issue and wish to investigate further by taking a blood sample.
Please consult the given information and determine:
A) What sample(s) do you need to take?
B) which animals should we sample
C) how many should we sample?
D)what animals should we avoid sampling?
A) heparinised and serum sample. LiHep or CAT tube
B) representative proportion of the herd and across management groupings
C) at least 6 animals or 10% of herd - ideally 4 animals per management group
D) Ill animals
Why do we want to avoid measuring blood of ill animals in a farm sample, especially for copper?
caeruloplasmin (CP) is used to assess copper - it’s an acute phase protein
elevated during illness → false results
Case 2
You visit a farm, the Holstein- Friesian Dairy cows have a recent drop in milk yield and quality. They have recently changed from first cut to 2nd cut grass silage. You suspect that the energy of the 2nd cut silage is much lower than the first cut was and the formulated diet is deficient in energy. You have persuaded the farmer to send a sample of the silage off for analysis and the diet will be reformulated in light of this. However, this will take a while and you wish to confirm that this is indeed an energy issue and wish to investigate further by taking a blood sample.
Please consult the given information and determine:
A) What sample(s) do you need to take?
B) Which animals do we sample
C) How many animals?
D) what animals should we avoid sampling?
A) serum sample, (EDTA plasma could be used) plain Z or CAT tube
B) representative proportion across management groups
C) 4 per management group, 10% herd ideally, at least 6
D) ill animals - results will show response to illness not nutritional issue
D. Blood sampling problems - Consequences
Case 1. Sharpie’s Addison’s diagnosis
Results similar to these led to Sharpie being treated with the mineralocorticoid (Fludrocortisone acetate), initially at the recommended dose, due to suspected Addison’s disease. After 2 years of treatment he was referred to a specialist because the treatment appeared ineffective.
Why should alarm bells have rung when the vet received this result (or even before the lab issued the results)?
The specialist identified the problem as being selection of the wrong blood tube. Can you suggest what type of blood tube had been used by Sharpie’s vet and why this gave the wrong result for his potassium levels?
Which type of blood tube should have been used?
NOT EDTA TUBE - the anticoagulant IS Potassium!!!!!! This is why there is an elevated K+ level.