Cerebral Vascular Accident (CVA)-Stroke
1/68
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
69 Terms

AVM (arteriovenous malformation): impaired blood flow; Pt suddenly collapse
Quicker you act, quicker recovery
may just have aphasia (cant speak), or may have paralysis & severe cognitive impairment
Cerebrovascular Accident (CVA) or Stroke
Brain requires blood to provide the oxygen and glucose
CVA = interruption of cerebral blood flow
Stroke occurs when
Functions are lost or impaired –can pt come back if perfusion and oxygen comes back thats why time is crucial
Severity of loss of
function varies according to the location and extent of the brain involved.
Time = Brain–cerebral spinal fluid, brain matter, and — the skull cannot take any additional of anything else bc then parts of the brain will start to die off
Risk Factors: Nonmodifiable
Age (doubles each decade >55 years of age)
Gender (Male)
Race (African American)
Ethnicity
Heredity/family history of stroke (prior transient ischemic attack, or a prior stroke)
Modifiable risk factors
HTN and Heart disease
Metabolic syndrome
Serum cholesterol→ platelet aggregation on top of cholesterol
Heavy alcohol consumption and Drug abuse and Smoking
Poor diet and Obesity
Sleep apnea
Physical inactivity
Diabetes→ can be both non-modifiable and modifiable; once Dx you cannot cure
Transient Ischemic Attack (TIA)
Transient dysfunction
Not permanent
High risk for CVA
Symptoms last <1 hour
Transient Ischemic Attack (TIA): clinical manifestations
hemiparesis
inability to speak, diplopia, transient weakness,
numbness, loss of sensation,
vertigo and Vision difficulty
aphasia (understand or express speech),
dysarthria (impairment of speaking muscles),
dysphagia (swallowing),
ataxia (loss of muscle coordination ie. Gait
difference between TIA and stroke
all these things are seen in a regular stroke except it last less than 1hr and if someone doesn’t rec it they are then at high risk of stroke if TIA goes away, essentially a precursor to a stroke down the road
Transient Ischemic Attack (TIA) tx
platelet inhibitor (ASA, clopidogrel), anticoagulants
Platelet inhibitors return brain back to normal function
Ischemic stroke
Inadequate blood flow
May progress in the first 72 hours related to growing edema
80% of all strokes are ischemic strokes.
Ischemic stroke: 2 types
Thrombotic→ plaque in artery and then clot occludes
Embolic→ embolism completely occluded
Small chances for survival and difficult for patient to remain fully functioning (both ischemic and hemorrhagic)
Hemorrhagic stroke
Bleeding in skull–vessel in the brain broke and blood in places where it should not be, extra blood is destroying other cells and brain matter
HTN most common cause
Sudden onset, rapid deterioration
“Worst headache of my life” blood puts extra pressure on parts of the brain and thus die off
Thrombotic stroke
plaque builds up on the side of vessel (narrows) and then everything builds up (causing a partial-complete blockage)
Embolic stroke
can be vegetative bacteria, A-fib, right atrial clots, DVT
Something breaking off, rather than “dam effect” of building up
Ischemic stroke
no oxygen or nutrients
nursing assessment
ABC
Time of Onset
Rapid glucose check
Vitals
Comprehensive neuro examination
Level of consciousness
Including NIHSS stroke scale–don’tmemorize it just know it’s a part of the assessment
Glasgow Coma Scale
Motor abilities and Sensation
Proprioception (ability to sense movement)
Cerebellar function–romberg
Pupil check
Common Deficits Following Stroke: Contralateral
ex. right brain stroke produces effects on left side (L hemiplegia)
Common Deficits Following Stroke:Hemiparesis→
weakness on one side
Common Deficits Following Stroke: Hemiplegia→
the inability to move a group of muscles on one side (paralysis)
Pt may or may not know their limb is present
no movement at all
Akinesia –
loss of skilled voluntary movement
common deficits following stroke: facial droop, ptosis
ptosis is the eyelid drooping
Swallowing and speech deficits Following Stroke: Dysphagia→
impaired muscles of swallowing
Speech therapy consult and swallowin eval
Swallowing and speech deficits Following Stroke: Diminished Sensation and Gag reflex
Assessed by speech pathologist; ensure gag reflex before anything PO
May need to ask them to swallow twice or rinse with water to fully swallow and clear mouth
Swallowing and speech deficits Following Stroke: Aphasia→
communication dysfunction
Expressive (Broca’s) Aphasia (slow speech, takes effort)
Loss of speech production can’t tell you the answer bc it isn’t coming out that way
Receptive (Wernicke’s) Aphasia
Loss of speech comprehension doesn’t understand what youre saying
Global: Both gestures, communication boards,
Sensory and perceptual deficits following Stroke: Dysarthria
impaired muscles of speech. Slurred speech
Does NOT affect the comprehension of language/ communication the motor of the mouth doesn’t let em speak
Sensory and perceptual deficits:
Blindness in same half of each visual field
Other visual problems
Diplopia (double vision)
Neglect of affected side –usually dt hemianopsia
Agnosia: inability to recognize objects or stimuli using senses –or name objects in their hands
Apraxia: inability to perform learned, purposeful movements (know how to do it, but can’t physcially do it)
Blindness in same half of each visual field
Known as Homonymous Hemianopsia–can only see from half of their eye and sees the same thing, tell em to turn their head to scan the room
Right side stroke-left hemiplegia-left side of both eyes
Emotional and cognitive changes
Frustration
Depression
Anxiety
Impulsive, Impaired judgement
Impatient
Memory problems
Diagnostic studies
Noncontrast Cat Scan (CT) the gold standard or MRI
Indicate the size and location of the lesion
Differentiate between ischemic and hemorrhagic stroke–since both are treated differently, white stuff is blood
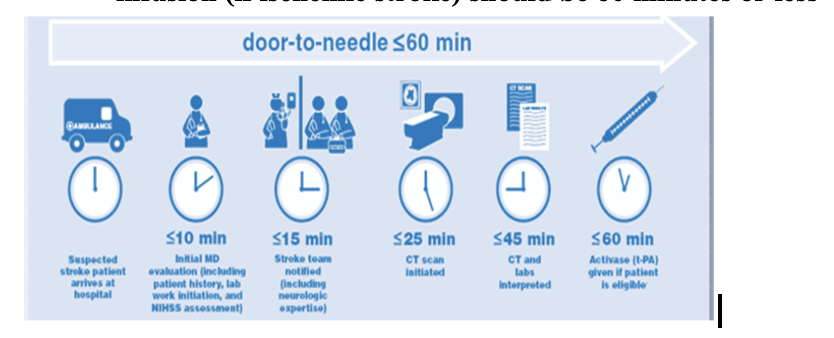
Ischemic: treatment must be given in <4.5 hrs
Don’t treat ischemic stroke if you don’t know when it started
Done within 25 minutes of ED arrival
initial nursing Interventions
Ensure patent airway and breathing
Call Stroke Alert
Maintain adequate oxygenation
Obtain IV access (2 IV access), give normal saline
Obtain CT scan immediately
Baseline laboratory tests
Vital signs (high BP is fine, but should be crazy high)
most important point from patient history is
Time of onset. About 25% of patients will worsen in the first 24 to 48 hours.
Maintain BP according to guidelines:
Elevated BP is common immediately after a stroke.
Body’s attempt to maintain cerebral perfusion
Use of drugs to lower BP is recommended only if BP is markedly increased (mean arterial pressure [MAP] greater than 130 mm Hg or systolic pressure greater than 220 mm Hg).
In the case of an acute stroke,
IV antihypertensives such as metoprolol are preferred.
Although low BP immediately following a stroke is uncommon, hypotension and hypovolemia should be corrected.
The time a suspected stroke patient arrives in the ED to the start of the
thrombolytic infusion (if ischemic stroke) should be 60 minutes or less
Medications
Antiplatelet drugs. Aspirin, clopidogrel
Anticoagulant therapy
Platelet inhibitors and anticoagulants are Contraindicated for patients with hemorrhagic stroke
Only for ischemic stroke
Not until after CT scan
Anticipate thrombolytic therapy for ischemic stroke
Statins
Monitor for SE of meds
Management of hypertension
Seizure prophylaxis-specific after hemorrhagic stroke
Thrombolytics–recombinant tissue plasminogen activator (ends in -ase)
Acts directly on clot to cause lysis. Converts plasminogen to plasmin, which digests fibrin and dissolves clot
*Within 30 minutes of arrival to ED, not usually after 4.5 hours after symptoms (Average 4.5 hours)
Before tPA→do all invasive procedures (draw labs, start 2 or 3 IV lines, foley)
Contraindications (Bleeding, BP etc. See MI PPT)
Role of the RN in rtPA administration
Assess for exclusions to therapy
Monitor baseline coagulation studies
Insert foley, nasogastric tube and multiple IV’s before rtPA administration
Monitor level of consciousness (bleeding), for symptoms of cerebral hemorrhage
May have bleeding gums, IV sites-small amount ok. Concerns if frank bleeding; change in LOC
After start of rtPA-
no IV starts, IMs, Invasive procedures or foley insertions for 24 hours
Teach patient about increased risk of bleeding
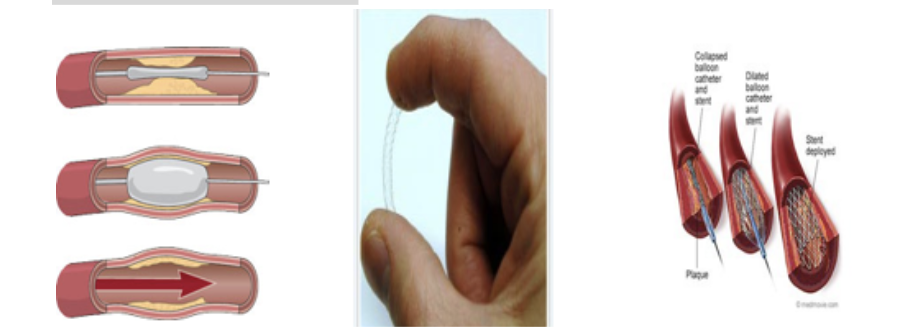
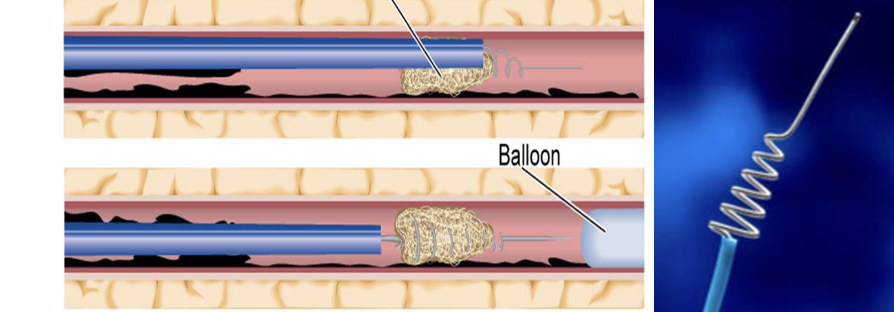
Ischemic surgical care
Angioplasty
Stenting
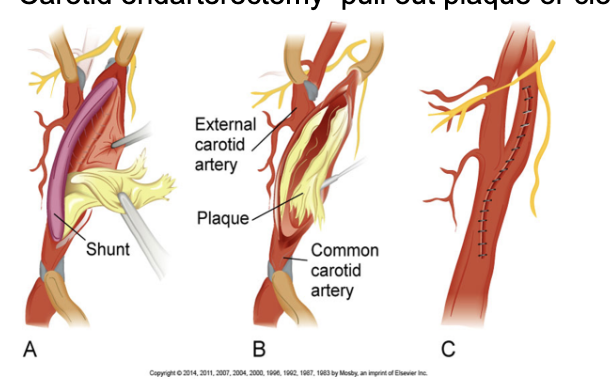
Carotid endarterectomy
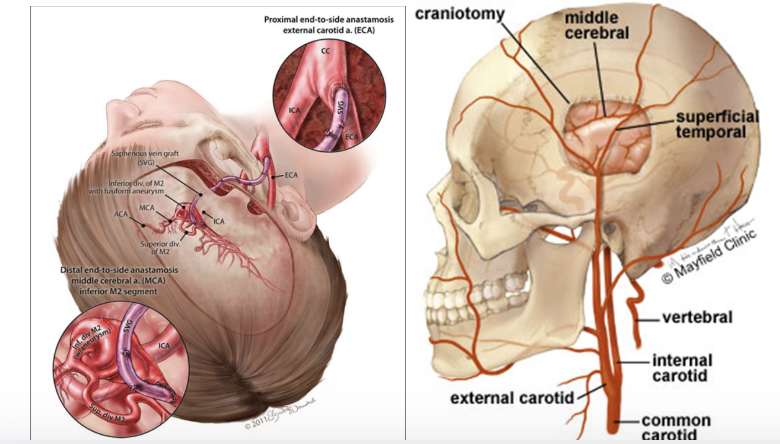
Extracranial-intracranial bypass
Stent retriever
MERCI
Hemorrhagic stroke surgical care
Resection (clips off vessels feeding area)
Clipping of aneurysm
Coiling
Angioplasty and stenting
–if clot of plaque
Carotid endarterectomy
In the common carotid artery or internal carotid artery, Endarterectomy is the removal of material on the inside of the artery.
Extracranial-intracranial bypass–
takes vessel from another part of the body and bypasses the clot
Common vessels used as a graft are the saphenous vein in the leg or the radial or ulnar arteries in the arm
Clot retrievers
Stent retrievers (Solitaire) 2015–se: if it doesn’t get all the clot it’ll break off a piece and send it somewhere else
MERCI Clot retriever catheter
Treatments for hemorrhagic strokes
clipping, clipping with bypass, coiling
Nursing management–priority problems
Risk for ineffective cerebral tissue perfusion– nutrients, glucose
Ineffective airway clearance
Impaired physical mobility
Unilateral neglect
Safety…fall precautions –hemiplesia
Impaired verbal communication
Impaired urinary elimination
Impaired swallowing…aspiration precautions, swallowing screen
Mobility, Skin Integrity
Situational low self-esteem
Nursing management: musculoskeletal: In the acute phase,
range-of-motion exercises and positioning are important. 1-2x a week
Paralyzed or weak side needs
special attention when positioned.
To move pt, place chair/wc on strong side–so this way they can do it emselves, pt may have contractures which we can put a brace or a wash cloth/something so the hand won’t close
Nursing management: musculoskeletal
Trochanter roll at hip to prevent external rotation
Hand cones to prevent hand contractures
Arm supports with slings and lap boards to prevent shoulder displacement
Avoidance of pulling the patient by the arm to avoid shoulder displacement or hurtin em
Posterior leg splints, footboards, or high-topped tennis shoes to prevent foot drop
Hand splints to reduce
spasticity but not all the time so they don’t have a contracture
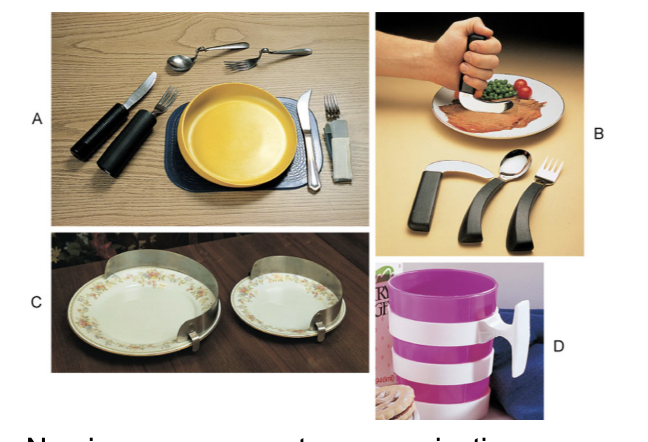
Nursing managements: assistive devices for eating
Nursing management: communication
Anxiety producing
Assess patient for both the ability to speak and the ability to understand.
Yes or No questions
Gestures may be used to support verbal cues.
Allow time for thought completion and speech
nurse should speak
Speak slowly and calmly, using simple words/directions or short sentences.
For pts with aphasia:
look at pt when speaking to them, use simple words and sentences, ask yes or no questions
Nursing management: sensory-perceptual alterations
Scan
Exercise
Eye patch
Ptosis eye exercises
Homonymous hemianopsia (food on the left side is not seen)
Diplopia have an eye patch
Nursing management: coping
Family members must cope aspects of patient’s behavior.
Behaviors that may have been reinforced during the early stages of stroke as continued dependency
Encourage Stroke Support Groups for patient and family resped so the family can take a break from pt
Rehabilitation
After stroke pt has stabilized for 12 to 24 hours, collaborative care shifts from preserving life to lessening disability and attaining optimal functioning.
PT, OT, ST
Patients may be transferred to a rehabilitation unit, outpatient therapy, or home care–based rehabilitation.
What were his risk factors for a stroke?
A 60-year-old male suffered a left cerebral hemispheric stroke involving the middle cerebral artery.
Transcranial Doppler ultrasonography demonstrated 80% stenosis bilaterally.
He was advised to undergo bilateral carotid endarterectomy.
He has a history of hypertension, MI 2 years previous, COPD, and rheumatic arthritis.
He has a 40-year history of smoking, hyperglycemia, hypercholesterolemia, and steroid dependency secondary to treatment of RA.
5 days after his stroke, he is discharged from the hospital to recuperate.
The client is diagnosed with a thrombotic stroke. Over the next 72 hours, you plan care with the knowledge that he
is ready for aggressive rehabilitation.
will show gradual improvement of the initial neurologic deficits.
may show signs of deteriorating neurologic function as cerebral edema increases.
should not be turned or exercised to prevent extension of the thrombus and increased neurologic deficits.
The client also has dysphagia. Before allowing him to eat, which action should you take first?
Check the patient’s gag reflex.
Request a soft diet with no liquids.
Place the patient in high-Fowler’s position.
Test the patient’s ability to swallow with a small amount of water.
Which clinical indicator does the nurse identify when assessing a patient with hemiplegia?
Paralysis of both lower extremities.
Paralysis of one side of the body.
Weakness of both upper extremities.
Weakness of the upper and lower extremities.
A patient who has had a CVA is receiving continuous nasogastric tube feedings. Which of the following should the nurse implement to prevent aspiration pneumonia. Select all that apply.
HOB up at least 45 degrees at all times
Perform oral hygiene at least once a shift
Verify tube placement at the beginning of each shift.
Offer bedpan every 4 hours.
Allow the client to lie on the left side periodically.
The nurse is caring for a patient with expressive aphasia. Which should the nurse include as part of long-range planning for the patient?
Provide positive feedback when the patient uses a word correctly.
Suggest that the patient get assistance at home because the disability is permanent.
Communicate with “yes” and “no” questions only.
Support the family to accept the fact that the patient cannot participate in verbal communication.
The wife of a patient admitted with a left-sided brain stroke must leave her husband’s bedside for 2 hours to pick up their children. Which nursing action is appropriate to contribute to patient safety while she is gone?
Apply restraints to the patient’s wrists.
Maintain the bed in a low fowler position.
Sit with the patient until his wife returns.
Place the call light in the patient’s left hand
The spouse of a patient brought to the ED states that 6 hours ago her husband began having difficulty finding words. The patient has since become progressively worse. He has right hemiparesis. Upon assessing the patient, you note that he is lying flat in a supine position, is drooling, and has been incontinent of urine. Place in order of priority the interventions the nurse should take for this patient at this time?
Provide perineal care
Assess for gag reflex
Elevate the head of bed 45 degrees
Perform a linen and gown change
Can you answer these?
The patient from the previous question is admitted to the acute medical unit after 7 hours with a diagnosis of ischemic stroke. His wife asks if her husband will receive IV thrombolytic therapy. What is your best response?
Thirty minutes later, the wife asks for a glass of water or juice because her husband is thirsty. What is your best response?