Health behaviour and the COM-B model
1/29
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
30 Terms
What is health?
People with chronic health conditions can still manage to have a good quality of life thanks to advancements in medicine
Health is not a binary state → health on a sepectrum
WHO definition out of date and not fit for purpose due to ageing population and ability to manage chronic health conditions
Huber et al (2011) propose shifting the emphasis of health towards the ability to adapt and self manage in the face of social, physical and emotional challenges
Cause of death
In the 1900’s
Pneumonia / flu
TB
Diarrhoea
Heart disease
Intracranial lesions (vasc.)
Nephritis
Accidents
Cancer
Senility
Diphtheria
% of deaths from major causes in UK 2006 (Allender et al, 2008)
All cardiovasular diseases
men - 35%
women - 34%
All cancers
men - 29%
women - 26%
Respiratory disease
men - 13%
women - 14%
Accidents and injuries
men - 5%
women - 3%
Other causes
men - 18%
women - 23%
Just diseases of older age?
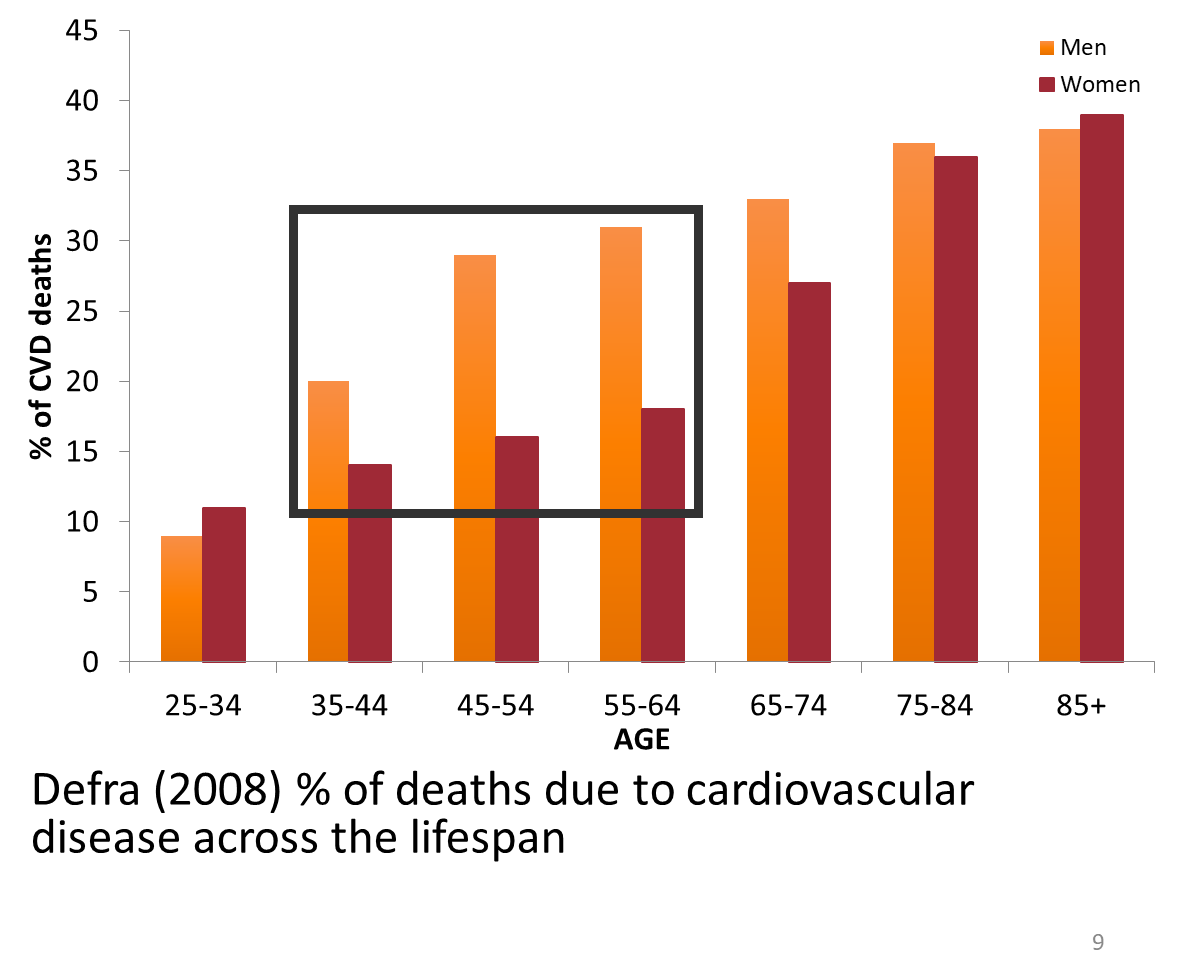
Summaries of the causes of death across the adult age group shows that it is not the case of being diseases of older age
We see peaks in the 35 - 64 age groups
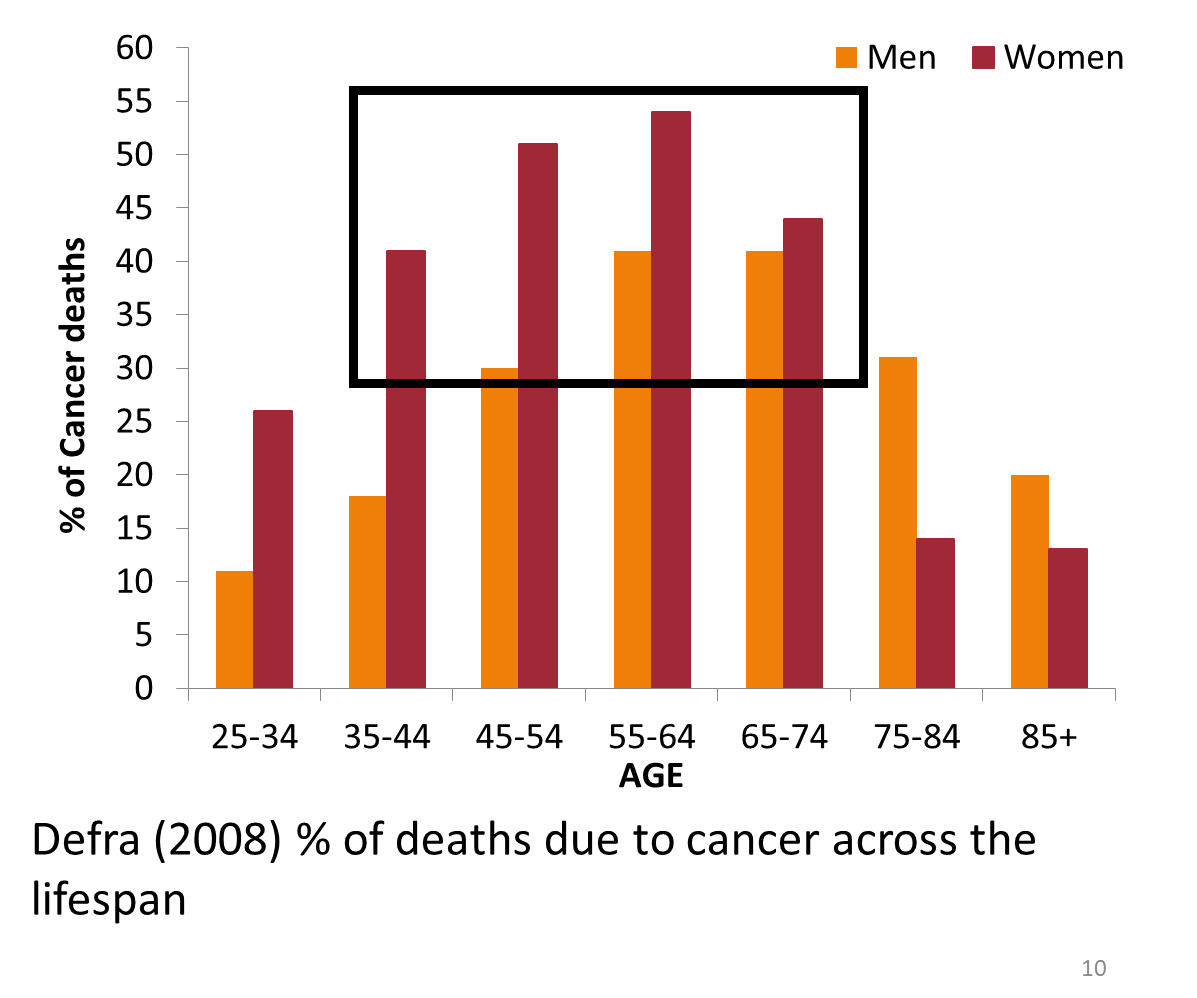
Younger people are dying of preventable causes
More apparent in cancer that is not just a disease of older age
Explaining these health outcomes
Over the past half century, it has been realised that behaviours such as smoking, dietary choice, alcohol consumption and regular physical activity play an important role in health outcomes
Adler et al, 1999
Behavioural factors account for around 50% fo premature deaths from the 10 leading causes
Gruman & Follick, 1998
The modern concept of health behaviour can be dated back to the Doll & Hill (1964) who studied British doctors in the 1950’s and found smoking was a major precursor of premature mortality
What are health behaviours?
Health behaviour - any activity undertaken for the purpose of preventing or detecting disease or for improving health / well being (Conner & Norman, 1996)
BUT health behaviours can have positive and negative health effects (Steptoe, Gardner & Wardle, 2010)
Positive (protective) health behaviour can be defined as ‘activities that may help to prevent disease, detect disease and disability at an early stage, promote and enhance health, or protect from risk or injury’
Negative (risky) health behaviour can be defined as ‘activities undertaken by people with a frequency of intensity that increases risk of disease or injury’
Broadest sense health behaviours - behaviours individuals engage in that affect their health
Measuring health behaviours
Behaviour is the currency of research into health behaviours
ie. it is often the dependent variable
But behaviour is notoriously hard to measure
Typically measured using categorical or continuous measurements using self report questionnaires
Eg. categorical - do you smoke? yes / no
Eg. continuous - how many cigarettes do you smoke a day?
x - social desirability bias (under or over reporting)
x - subject to recall bias
Other measures include observation
Eg. CCTV cameras to observe mask wearing in supermarkets
Or proxy measures
Blood tests, step counters, pill counters
BUT proxy measures not always accurate
Blood tests results can depend on metabolic rate
Pill counters rely on pills actually being taken out of a bottle
Step counters - errors in measurement, can be falsified
Number of health behaviours
Alameda county study (Belloc, 1973)
~ 7000 adults
Baseline postal questionnaire in 1965 followed by regular surveys of death and illness
7 baseline negative health behaviours predicted mortality
Lack of exercise
Snacking between meals
Smoking
Sleep (more than 8 hrs, less than 7)
Skipping breakfast
Regularly drinking more than 5 units of alcohol
Over / underweight
7 features of a health lifestyle
Non-smoking
Moderate alcohol intake
7 - 8 hours per night sleep
Exercise regularly
Maintain a healthy body weight
Avoid high calorie snacks
Eat breakfast regularly
Belloc (1973) The relationship was so strong that they proposed that people aged over 75 years who carried out all 7 of the behaviours had health that was comparable to those aged 35-44 who did less than 3
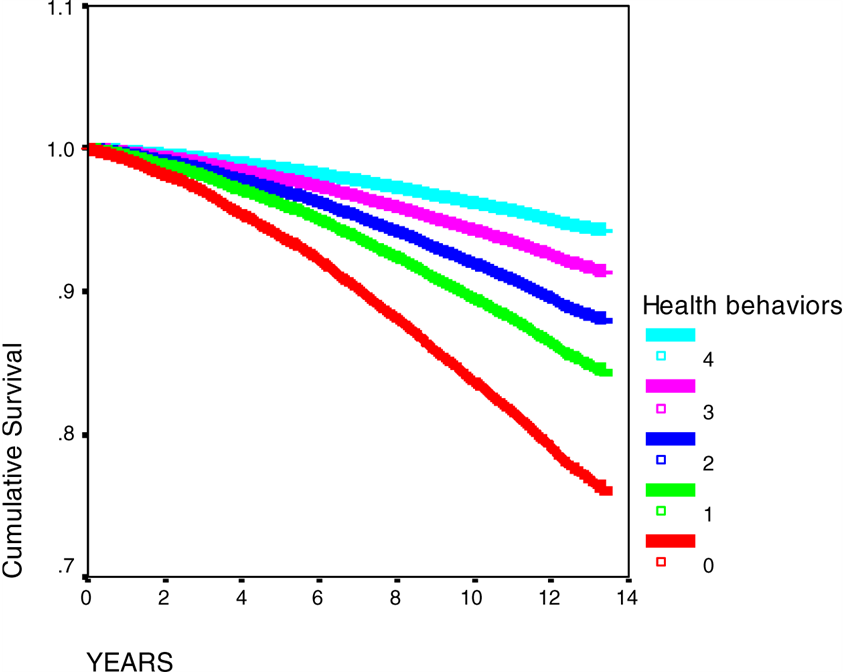
Khaw et al (2008)
Analysed data from EPIC Norfolk longitudinal study of 20,000 men and women
Baseline no known CVD / cancer, aged 45 - 79
Followed up over 14 years
Survival was associated with four health behaviours
not smoking
being physically active
drinking moderately
eating 5 or more servings of fruit and veg a day
The fewer of these behaviours performed the greater risk of death
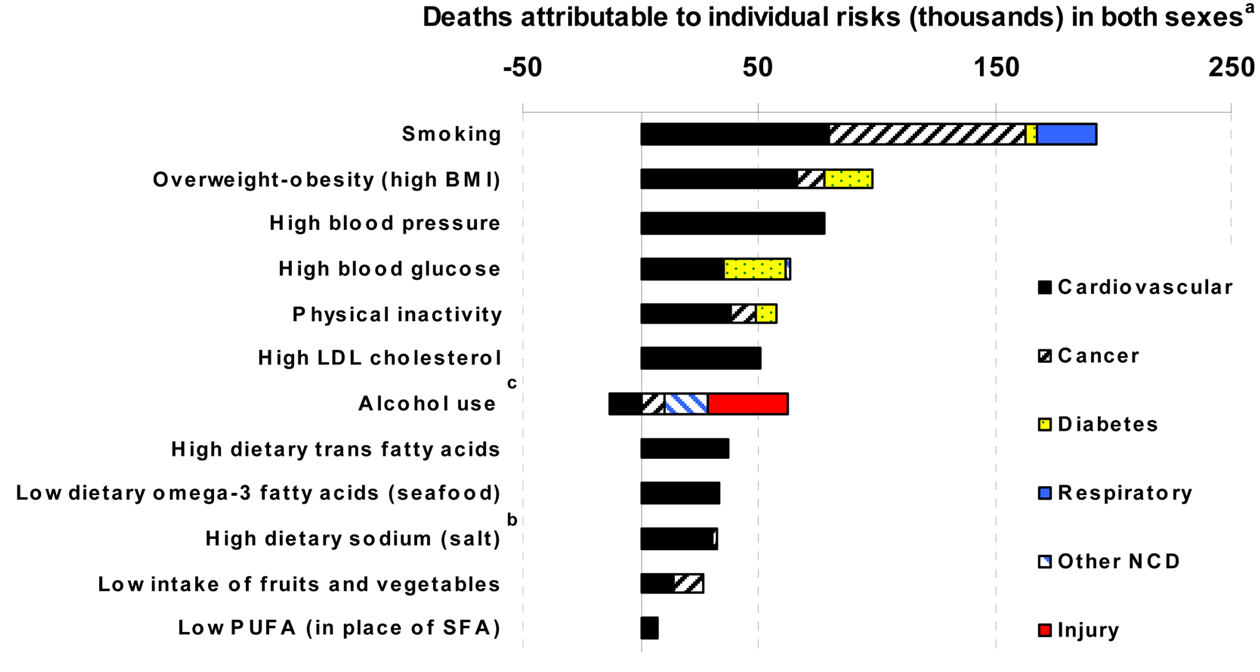
Preventable causes of death by health behaviour
Danaei et al (2009)
Investigation of deaths in the USA
Health behaviours can be lihnked to range of different causes of death
Eg. smoking atributable to CVD, cancer, diabetes and respiratory diseases
Health behaviours in the modern world
Several points emerge from the defintions of health behaviour and it’s study
The concept of health behaviours is fluid, and behaviours that are included can change as medical knowledge develops
Health behaviours are not uniformly important, but vary in their influence across time and across different populations
The strength of the evidence relatign behaviours with health outcomes is variable
Case control, prospective, experimental, cross-sectional (but association DOES NOT equal causation)
But consistent results with different samples and study designs, and a clear biological mechanism - stronger evidence
Behaviours may be done for non-health purposes, eg. limiting fat in the diet, going to the gym may be motivated by concern for appearance rather than health
Health psychologists need to view behaviour in a broad context and recognise that health motivations and cognitions are part of a wider set of infleunces on health behaviour
Important health behaviours in the modern world
Diet
In 2018 only 28% of adults eating 5+ servings of fruit / veg a day (NHS, 2020)
Physical activity
More than 80% of adolescents and 27% of adults do not meet WHO’s recomended levels of physical activity (WHO, 2022)
Smoking
Rates declined over the last decade, but ~ 8 million adults in the UK smoke (ONS, 2021)
Highest rate amoung 25 - 34 year old (ONS, 2021)
Sexual behaviour
47% of sexually active young people do not use a condom when sleeping with someone for the first time (YouGov Poll, 2017)
Alcohol
25 - 28% of adult drinkers in UK binge on alcohol on their heaviest drinking day (ONS, 2017)
Types of behaviour change
Different kinds of behaviour change
Initiate a new behaviour
Eg. starting to recycle, wearing face masks
Stopping an existing behaviour
Eg. stopping smoking, stop hugging friends / family
How a behaviour is performed
Eg. changing frequency, intesnity, duration of a behaviour (exercising more, eating less)
Changing behaviour - what do we need to consider?
Our primary motivational concerns in life are the same for humans as they are for most animals (food, water, air, reproduction, etc)
Challenging these behaviours that are motivated by these systems can be difficult, for example
Sexual behaviour - eg. condom use
Energy seeking behaviour - eg. eating habits
Energy conservation behaviour - eg. exercise levels
We need to first understand behaviour in order to change it, this requires adopting a biopsychological appeach to health
Understanding, and therefore attempting to change behaviour requires an appreciation of the evolutionary / biological, psychological and social contexts in which it takes place
Determinants of health behaviour - biopsychosocial approach
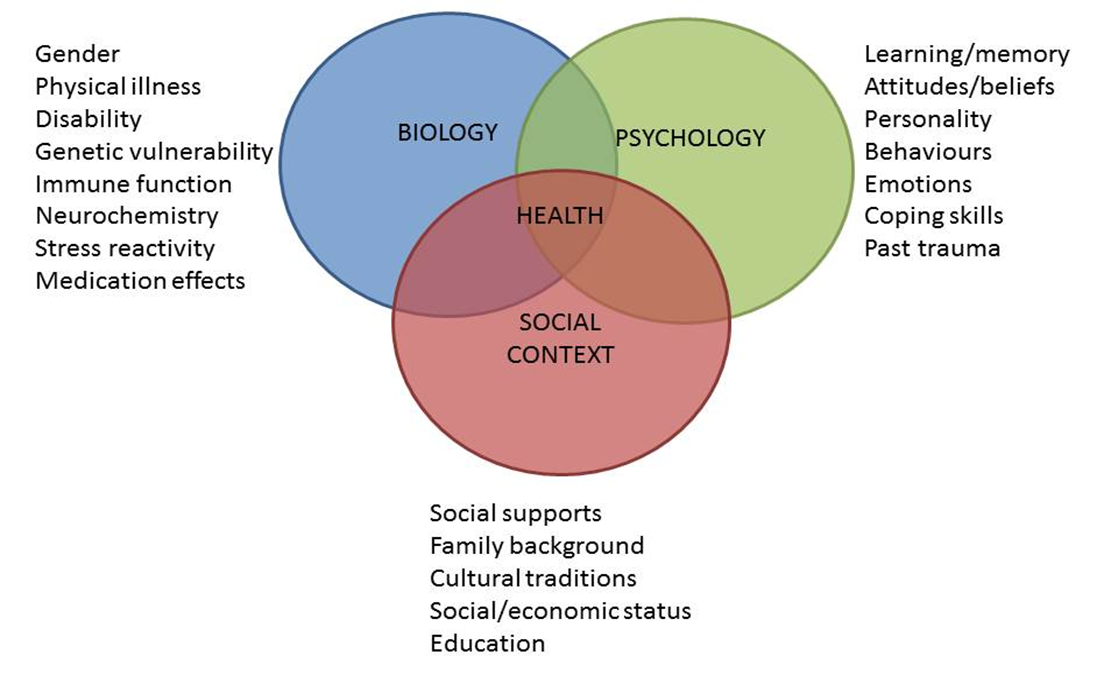
Biological determinants of health behaviour
Evidence from twin studies suggest there is a heritable component to smoking initiation, nicotine addiction as well as body weight and obesity (Plomin et al., 2000)
Some health behaviours have a physiological response (smoking, drinking, eating, exercising) releasing dopamine, endorphines which can reinforce the behaviour
The ability to carryout many health behavours is affected by personal
Disabilities may impact ability to carry out physical activity
Symptoms can act as cues to change or stop behaviour (eg. smoking, adherence to medications etc)
Social determinants of health behaviour
Health behaviours are strongly affected by peer group infleunces, family habits and social networks (Baranowski, 1997)
Early socialisation (observational learning) → health habits eg. brushing your teeth, smoking
Culturally valued or discouraged behaviour (eg. alcohol consumption in some religions)
Peer pressure in adolescence = origin og many risk behaviours
Socioeconomic status (Pampel, Krueger, Denney, 2010)
Financial barriers to health behaviours, lack of available resource, lower education
Legislative law (DeJong & Hingson, 1998)
Eg. seat belt use, drink driving
Psychological determinants of health behaviour
Emotion (Ferrer & Mendes, 2018)
Stress - smoking, drinking, overeating and exercise
Fear - avoidance of health care → eg. dental, delay in reponse to symptoms, screening etc)
Disgust - fear avoidance → blood test, cervical screening
Cognition (Armitage & Conner, 2000)
Attitudes and beliefs
Social cognition models (eg. Theory of Planned behaviour - Ajzen, 1991)
Interventions based on theory of planned behaviour to improve health behaviour
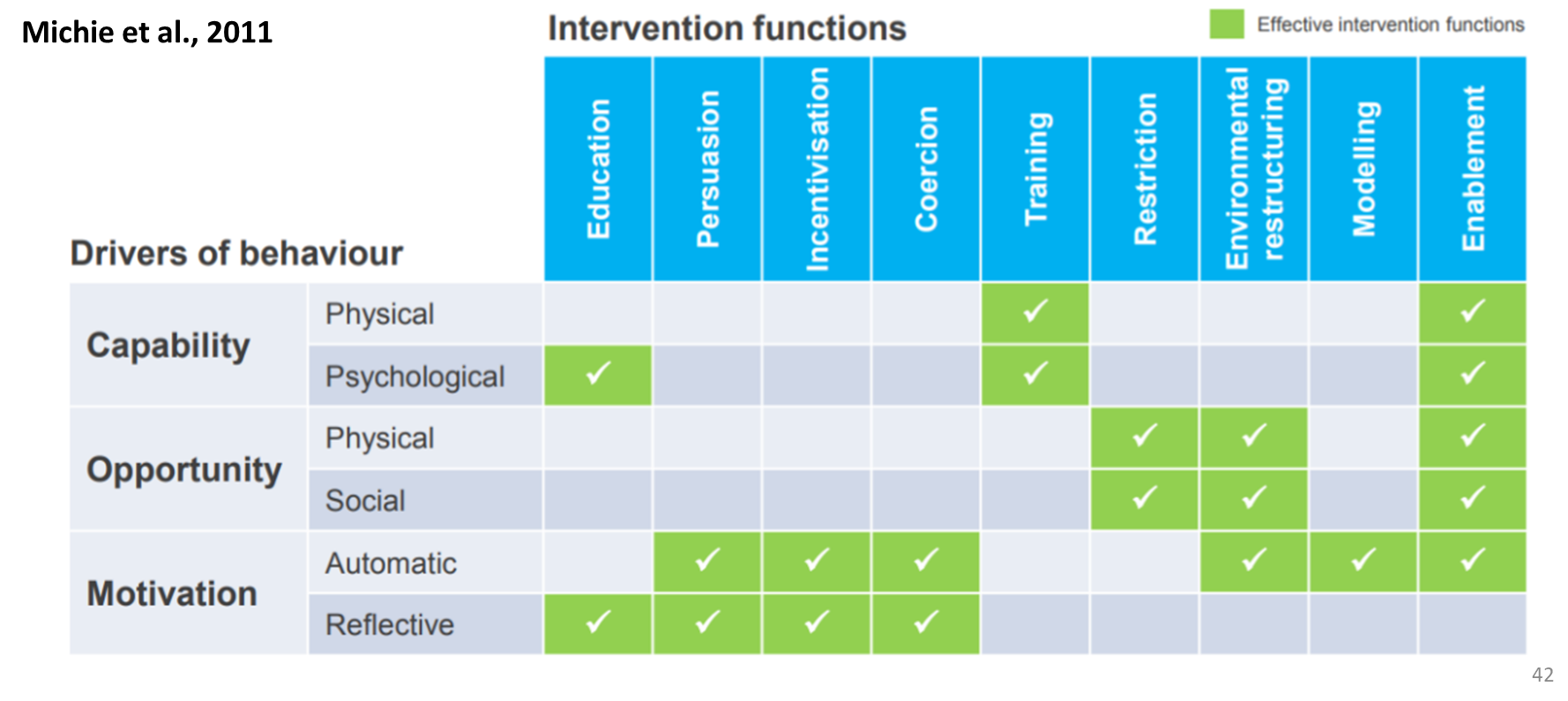
COM-B model
Michie et al (2011)
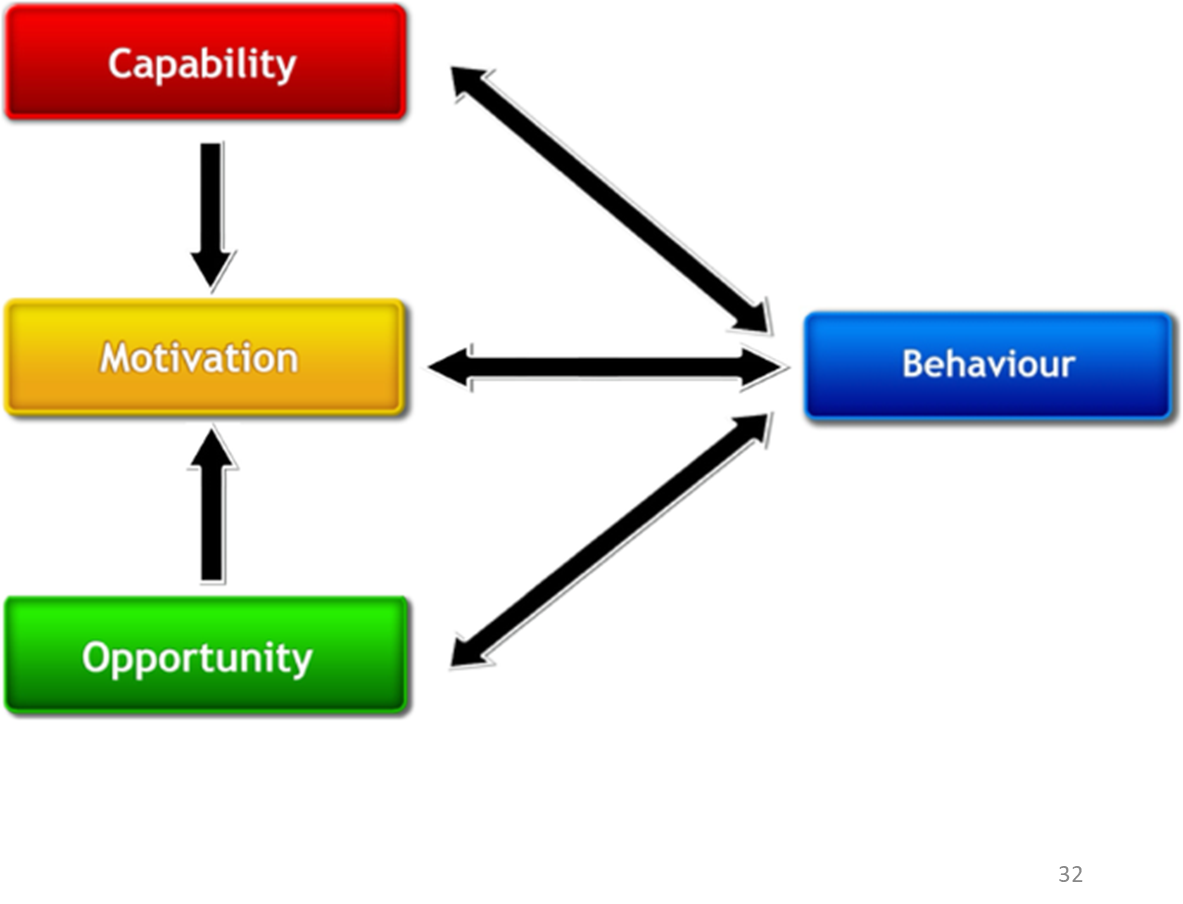
COM-B - capability
The ability to enact behaviour
Made up of physical and psychological capability
Physical capability
Physical skill / strength to perform the behaviour
Eg. ride a bike, lift a 20kg weight
Psychological capability
Capacity to engage in nencessary thoughts processes - knowledge, reasoning
Eg. Knowledge of COVID-19 transmission and how to avoid it
COM-B - opportunity
Environment that enables behaviour
Made up of physcial and social opportunity
Physical opportunity
Opportunity afforded by the environment
Eg. close proximity to a gym, availability of cycle lane
Social opportunity
Opportunity afforded by social / cultural norms
Eg. people around you enjoy engaging in behaviour, reminders to do something, having support from people around you
Eg. Being able to smoke in the house of another smoker vs work meeting
COM-B - motivation
Mechanisms that activate or inhibit behaviour
Made up of reflective and automatic motivation
Reflective motivation
Evaluations (beliefs about what is good or bad), plan (intentions)
Eg. drinking responsibly is a good thing to do
Eg. planning to wake up early to go to the gym
Automatic motivation
Emotional reactions, desires (wants and needs), impulses, inhibitions
Anticipated pleasure at the prospect of eating piece of cake
Methods to collect data using COM-B
Questionnaires
Specific questions about their capability / opportunity / motivation
Reach larger groups of people
Interview / focus groups
In depth qualitative data
Ask open ended questiosn about capability / opportunity / motivation, barriers / facilitators of engaging in the desired behaviour
Smaller samples
Observation
Self report data questionnaires / interviews may be far away from the truth, observations useful tool to see what actual happens
How well can the COM-B explain behaviour?
Willmott et al (2021) - COM-B and physical activity
A cross sectional survey
Used validated measures to capture COM constructs and physical activity behaviour
Administered online to a sample of young adults aged 18 - 35 years
N = 582 (mean age = 22.8 years; 80.3% female)
The COM-B model explained 31% of variance in physical activity
Capability and opportunity were found to be assoicated with behaviour through the mediating effect of motivation
Increased capability + opportunity → increased motivation → increased physical activity
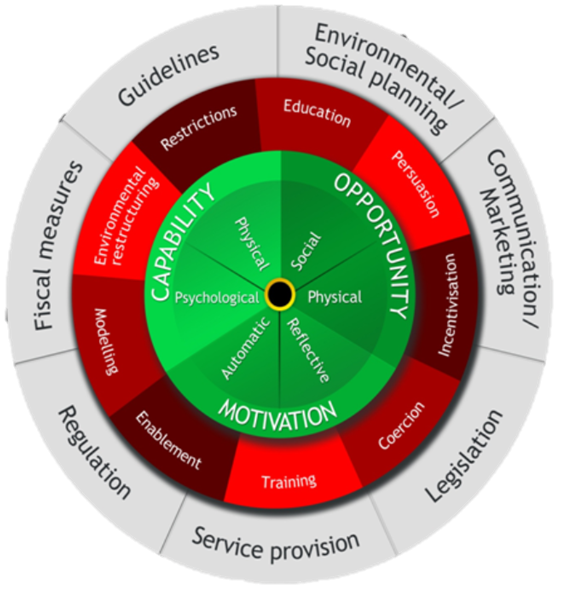
Designing interventions for behaviour change
Once you have considered behaviour in context (eg. collected data using the COM-B model) and understand what drives it you can begin to consider options for interventions
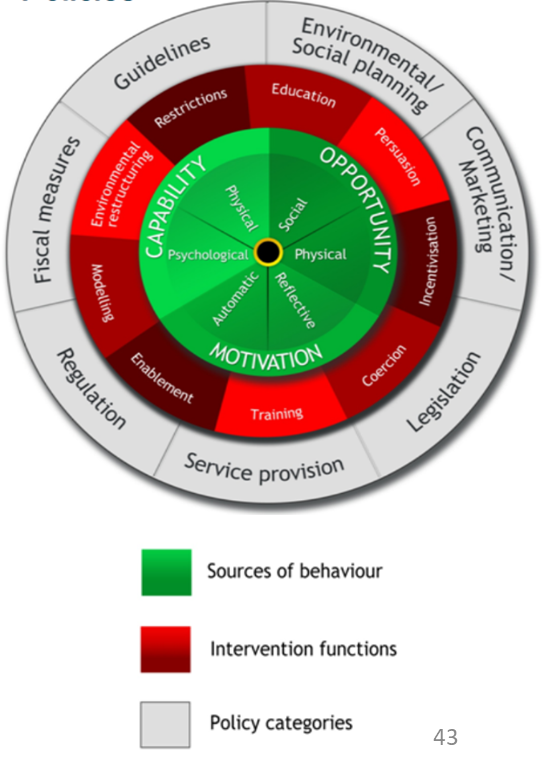
Michie et al (2011) developed a synthesis of 19 frameworks of behaviour change interventions to help with this - the behaviour change wheel (BCW)
Comprehensive
Coherent
Linked to model of behaviour (COM-B)
Identified 9 intervention functions and 7 policy categories that could enable or support these interventions to occur
BCW - intervention functions
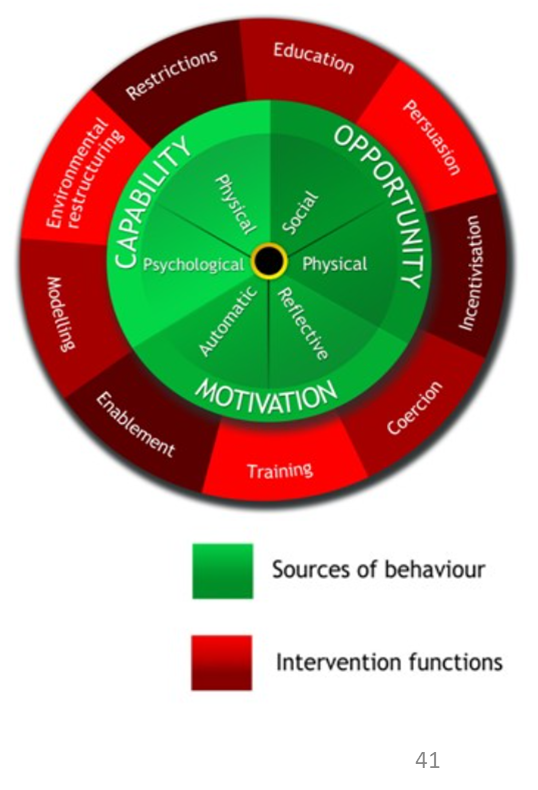
Michie et al (2011)
Intervention functions are activities to change behaviour
Behavioural diagnosis → aspects of COM-B that need addressing → intervention functions to change the behaviour
Education - increasing people’s knowledge
Persuasion - using communication to induce possitive or negative feelings
Incentivisation - creating an expectation of reward
Coercion - creating an expectation of cost or punishment
Training - helping people to develop skills
Enablement - giving people means to engage in behaviour or reduce barriers
Modelling - providing an example for people to aspire to or emulate
Environmental restructuring - changing the physical or social context
Restrictions - using rules to reduce opportunity to engage in target behaviour
Matching intervention functions to COM-B
BCW - policy categories
Michie et al (2011)
Policies - decisions made by authorities interventions
Policy categories
Environmental / social planning - designing and controlling the social environment (eg. creating cycle paths, parks)
Communication & marketing - print, electronic media, broadcasting (eg. adverts about COVID vaccines or washing hands)
Legislation - changing laws (eg. prohibiting sale or use of drugs
Service provision - delivering a service (eg. cancer screening services)
Regulation - establishing rules or principles of behaviour (eg. voluntary agreements on gambling / alcohol advertisement)
Fiscal measures - using the tax system to increase cost (eg. sugar levy / alcohol tax
Guidelines - creating documents that recommend or mandate a certain practice (eg. govt drinking guidelines or NHS physical activity guidelines)
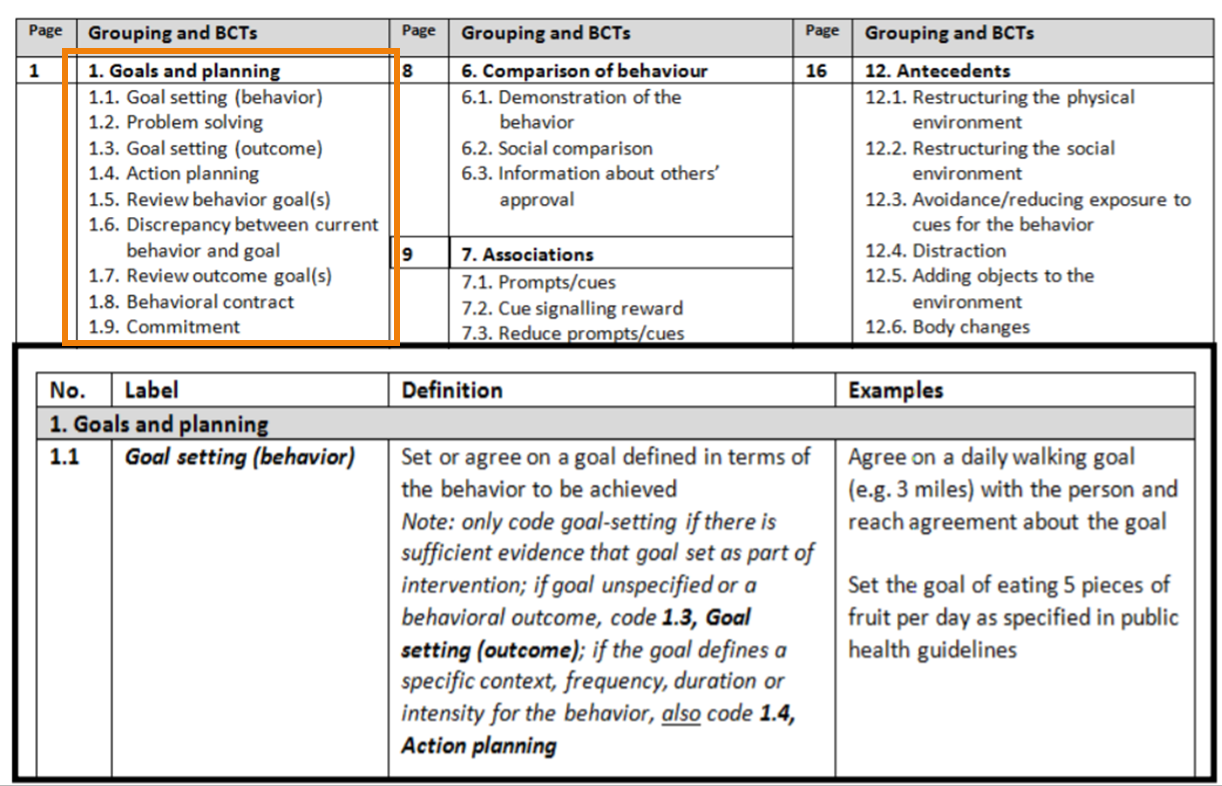
Behaviour change techniques
Michie et al (2013)
Intervention functions are delivered by behaviour change techniques
Created a taxonomy of behaviour change techniques to help specify interventions and their active ingredients in more detail
Active ingredients within the intervention designed to change behaviour
Observable
Replicable
Irreducible components of an intervention
Can be used alone or in communication
COM-B and the BCW in practice
Munir et al (2018)
Using BCW to develop an intervention to reduce sitting time at work
Focus group discussions with 39 NHS office workers based on COM-B model
Identified barriers / enablers related to
Psychological capability (eg. knowledge of health risks of prolonged sitting
Social opportunity (eg. social norms)
Physical opportunity (eg. to have height adjustable desk)
Automatic motivation (eg. need automatic reinforcement to change habit
Reflective motivation (eg. beliefs about positive consequences of standing)
Used BCW intervention functions, policy categories and BCTs to identify appropriate strategies
Findings
Physical opportunities - don’t have height adjustable desks
Intervention functions - environemntal restructuring, enablement
BCTs - restructuring the physcial environment, adding objects (provide height adjustable workstations)
Social opportunities - social norms made it difficult to stand at a desk and work
Intervention functions - modelling, enablement
BCTs - demonstration of behaviour, social support
Psychological capability - limited knowledge of health risks of prolonged sitting
Intervention functions - education
BCTs - info about health consequences via seminars, instruction booklets
Reflective motivation - beliefs about positive consequences of standing were low
Intervention functions - education, persuasion
BCTs - info about health consequences via seminars, coaching session, feedback on outcomes of behaviour
Automatic motivation - staff need simple automatic reinforcement to change habit
Intervention functions - environmental restructuring, incentivisation
BCTs - prompts and cues (via the use of an app), self monitoring usign a diary of daily sitting and standing time