topic 15: urinary system
1/112
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
113 Terms
Main function of the urinary system
Controls plasma composition (not just urine production)
What does the urinary system regulate?
Blood volume, blood pressure, electrolytes, pH, wastes
How much plasma do kidneys filter per day?
~180 L/day
Why isn’t all filtrate excreted?
Most is reabsorbed → only wastes/unneeded substances remain
What is the nephron?
Functional unit of kidney that controls plasma composition
4 processes of urine formation
Filtration, reabsorption, secretion, excretion
Hormones regulating kidney function
ADH, aldosterone, ANP
Role of ADH, aldosterone, ANP
Fine-tune water, BP, and electrolyte balance
Endocrine functions of kidneys
Produce erythropoietin and renin
Why is urinary physiology important?
Maintains homeostasis and connects multiple body systems
what does the urinary system consist of
kidneys - form urine and regulate the composition of blood plasma (contents are dropped off at the kidney and it dictates what is reabsorbed and excreted)
nephron - function unit
structure that transport urine - renal pelvis → ureters → urinary bladder → urethra
what are the functions of the kidneys?
maintain plasma volume ∴ maintain bp (MAP)
regulate [ion] + [H2O]
acid-base balance (movement of H+ ions)
eliminate waste (nitrogen), drugs, hormones
endocrine (partially endocrine organ)
renin (bp) (produced by kidney, angiotensin)
erythropoietin (rbc production)
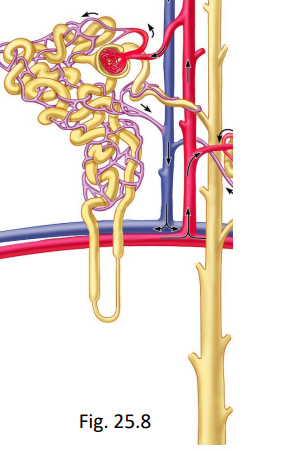
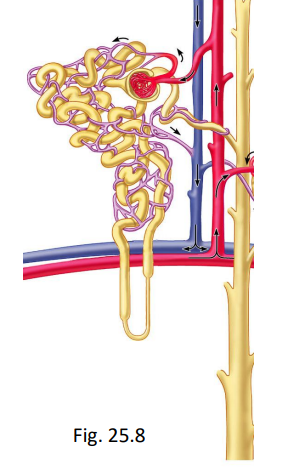
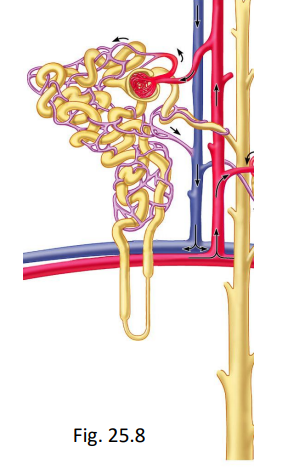
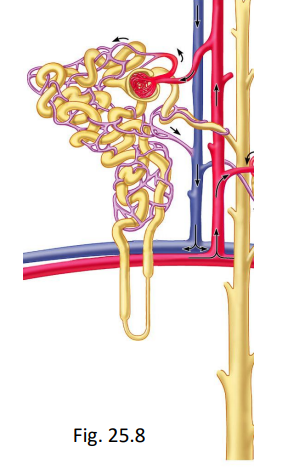
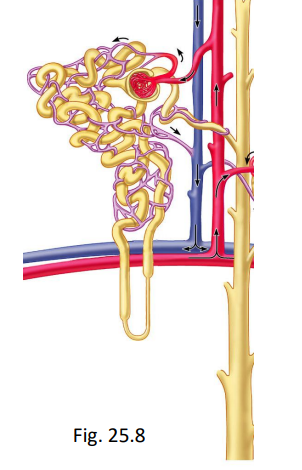
what is the nephron?
functional unit of the kidney
includes renal corpuscle (glomerulus with renal capsule) and the tubule ((1st)proximal convoluted tubule, descending and ascending Nephron Loop, (2nd) distal convoluted, collecting duct)
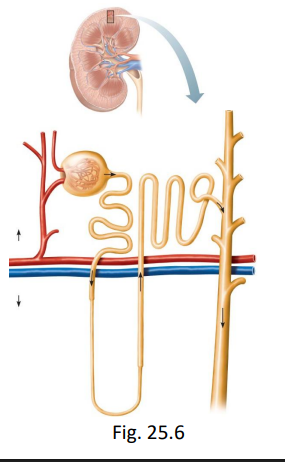
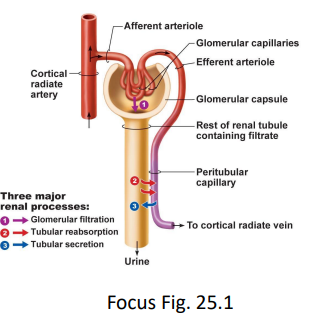
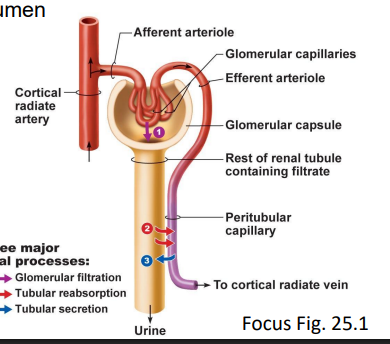
what are the processes in the nephron that lead to urine formation?
glomerular filtration
tubular reabsorption
tubular secretion
what is the glomerular filtration process?
process by which water and small solute are forced out of the blood in the glomerulus and into the Bowman’s capsule due to pressure differences across the filtration membrane
bulk flow and osmotic pressure
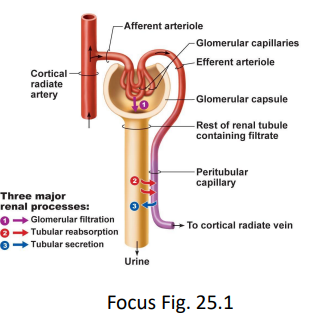
what is the process of tubular reabsorption?
process by which valuable substances like water, glucose, and ions are transported from the filtrate in the nephron back into the bloodstream
glucose and Na+ transporter
H2O - osmosis
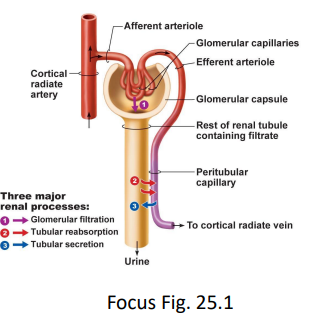
what is the process of tubular secretion?
process by which additional waste products and excess ions are actively transported from peritubular capillaries into the lumen of nephron tubules to be excreted as urine
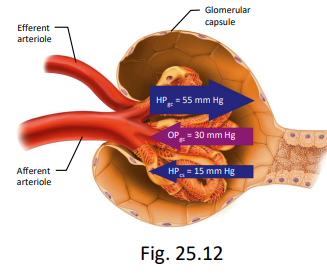
what is glomerular filtration?
20% of plasma in glomerulus is filtered into Bowman’s capsule via bulk flow (ΔP) across the filtration membrane
what does the filtration membrane consist of?
fenestrated endothelium (glomerulus)
fused basement membranes
podocytes (layer of Bowman’s capsule) with filtration slits between
should not dump big molecules like proteins

explain the filtrate from glomerular filtration
identical to plasma minus large proteins
H2O, glucose, amino acids, vitamins, ions, urea, some small proteins (stuff that typically doesn’t cross the membrane will cross the glomerulus)
~7.45 (neutral, pH decreases when ejected)
net filtration pressure
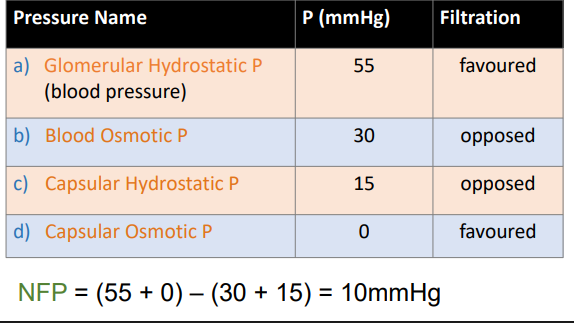
glomerular hydrostatic P
55 p (mmHg)
filtration: favored (push things out of glomerulus)
blood osmotic pressure
30 mmHg
filtration: opposed (pulls water back into blood)
capsular hydrostatic pressure
15 mmHg
filtration: opposed (pushes fluid back into blood)
capsular osmotic pressure
0 mmHg
filtration: favored (bowman’s capsule) (no capsular osmotic pressure)
glomerular filtration rate (GFR)
at this NFP, ~180 L/day filtrate (both kidneys) = 125 ml/min (so the entire plasma volume filtered ~65 times per day) not all will become urine
however, <1% of filtered volume remains at the end of collecting duct (reabsorption)
eliminate some stuff
What does a net filtration pressure (NFP) of +10 mmHg mean?
Filtration is favoured
→ Net force pushing fluid out of blood into Bowman’s capsule
→ Normal urine formation is occurring
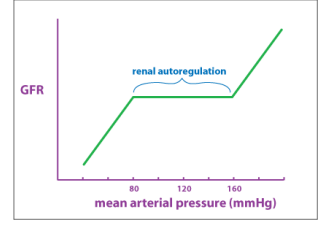
what is regulation of GFR?
regulated to ensure that the kidneys filter blood a consistent and appropriate rate for the conditions the body and helps to maintain a constant pressure in the glomerulus despite changes in system blood pressure
keeps GFR from changing when systemic blood pressure changes - if not, ⇑ MAP = ⇑ GFR (and vice versa)
what happens if GFR is too high?
valuable nutrients and water may be lost in the urine (filtrate passes through too quickly for proper reabsorption)
what happens if GFR is too low?
yhe blood is not being filtered fast enough and wastes may accumulate in the blood
how does regulation help keep GFR?
from changing when blood pressure changes - if not ⇑ MAP = ⇑ GFR (and vice versa)
what are the processes of regulation of GFR?
intrinsic regulation
extrinsic regulation
intrinsic regulation (autoregulation) of GFR
for BPs in resting to moderate exercise range
myogenic
juxtaglomerular apparatus
intrinsic regulation (autoregulation) of GFR: myogenic
⇑ MAP ⇒ stretch ⇒ afferent arteriole smooth muscle contracts ⇒ prevents ⇑ bp in glomerular capillaries (and vice versa)
intrinsic regulation (autoregulation) of GFR: juxtaglomerular apparatus
⇓ BP ⇒ ⇓ GFR ⇒ flow of filtrate past macula densa ⇓ - causes release of local factors ⇒ afferent arteriole dilates ⇒
⇑ GFR to resting
NOTE: macula densa monitors [NaCl] in filtrate flowing past it
juxtaglomerular complex (apparatus): if filtrate flow (∴ GFR)
= high → reabsorption may be inadequate ∴ [NaCl] high; if filtrate flow = low → too much reabsorption ∴ [NaCl] low
juxtaglomerular complex (apparatus): if bp ⇑ (in glomerular capillaries)
GFR ⇑ ⇒ ⇑ [NaCl] in filtrate at macula densa ⇒ triggers local release of vasoconstrictor ⇒ afferent arteriole constricts ⇒ GFR ⇓ to resting
extrinsic regulation of GFR
primarily SNS → arteriolar vasoconstriction (both arterioles):
afferent: ⇓ flow into glomerulus
efferent: blood backs up in glomerulus
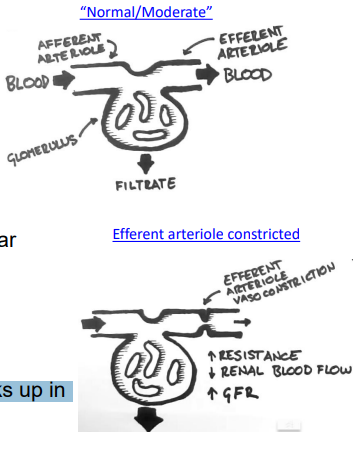
moderate SNS activation in extrinsic regulation of GFR
constriction of the afferent and efferent arteriolar is balanced → GFFR doesn’t change much
extrinsic regulation of GFR: during extreme stress
(e.g. heavy excersie, hemorrhage - losing fluids) there is more vasoconstriction of the afferent arteriole (than efferent) which causes ⇓ GFR to ( which helps the body conserve fluid and redirect blood to critical organs)
what can NFP change?
blood OP (proteins)
e.g. dehydration - ⇑ BOP = ⇓ GFR
e.g. burns, nephrotic syndrome (proteins filtered) - ⇓ BOP = ⇑ GFR (nephrotic syndrome, proteins filtered)
capsular HP
urinary tract obstruction (kidney stones, inflammation, prostate enlargement) - ⇑ CHP = ⇓ GFR
⇑ hydrostatic p → things wont filter properly - opposes filtration
what is tubular absorption?
1 - 1.5 L/day urine but 180 L/day filtered ∴ 99% of filtrate reabsorbed
may be active and passive
active tubular reabsorption
required energy (move things across membrane)
Na+, other ions, glucose, amino acids (wan to retain, actively move back into bloods)
passive tubular reabsorption
no energy
Cl-, H2O, urea (flow along concentration gradient until equilibrium)
reabsorption in the proximal convoluted tubule - unregulated?
i. glucose, amino acids – 100% reabsorbed via active transport (small amount amino acids in urine naturally but never should have glucose)
ii. Na+ - 65% - reabsorbed via active transport (some will be eliminated with urine, helps dilute urine in loop of henle)
iii. small proteins (endocytosis into tubule cell ⇒ amino acids ⇒ blood)
iv. vitamins v. obligatory (unregulated) reabsorption of H2O (osmosis – follows solutes)
what is the result of reabsorption in the proximal convoluted tubule?
large amount of solute removed and the volume of the filtrate is reduced (decreased) taken back → takes H2O with it
filtrate is now isotonic to plasma = 300 mOsmoles/L (atp. not actively moving H2O)
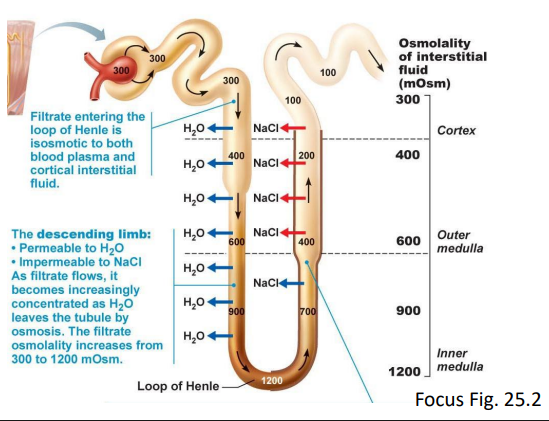
reabsorption in the Loop of Henle - (reabsorbs - into vasa recta)
descending limb (DL) = unregulated (obligatory) reabsorption of H2O only
ascending limb (AL) - impermeable to water, but get active transport of Na+, Cl- (excretes salt)
reabsorption in the distal convoluted tubule (DCT)
reabsorbs Na+, Cl-, Ca2+ (ejected lots in L of H to make concentration, reabsorbed some
impermeable to H2O (helps determine concentration of urine with L of H
reabsorption in the late distal convoluted tubule and collecting duct
important to maintaining homeostasis
reabsorbs Na+
aldosterone ⇑ Na+ reabsorption
ANP ↓ Na+ reabsorption
facultative (regulated) reabsorption of H2O (permeable to H2O)
ADH ⇑ (ANP inhibits ADH)
what do the nephrons normally reabsorb?
99% of filtered H2O (eliminate in urine)
99.5% of filtered NaCl
100% of filtered glucose (unless there is diabetes)
50% of filtered urea (transporters exist, try to get rid of as nitrogenous waste; reaches equilibrium)
what may filtrate normally contain?
trace amino acids and small proteins (depends on diet) but no glucose or blood
what is tubular secretion?
movement of substances from peritubular blood into filtrate in nephron lumen
what are the main substances secreted in tubular secretion?
wastes e.g. urea, uric acid, some hormones
K+ (⇑ by aldosterone)
H+ or NH4+ → maintains blood plasma pH (active secretion)
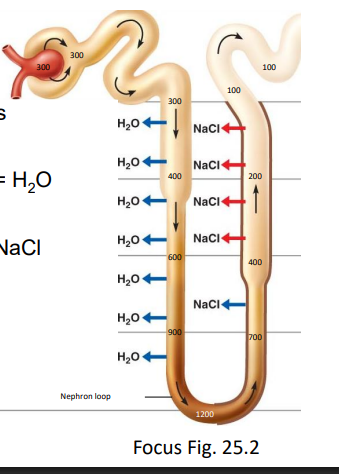
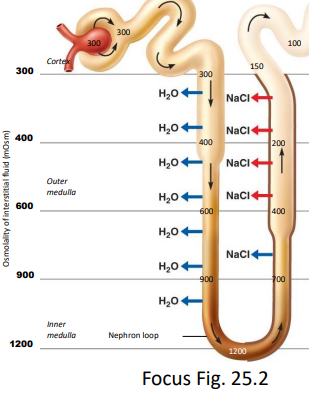
countercurrent multiplier mechanism
what is the purpose of the Countercurrent Multiplier Mechanism
Creates a medullary concentration gradient by:
Ascending limb → NaCl out (no water)
Descending limb → water out (no salt)
Allows kidneys to produce dilute or concentrated urine
(≈ 100–1200 mOsm/L)
what does the gradient established from the countercurrent multiplier mechanisms allow?
allows the kidney to produce urine that is either concentrated of dilute, helping regulate water balance and blood pressure
what does the nephron loops of juxtamedullary nephrons produce and maintain?
vertical osmotic gradient
i.e. a progressive increase in [solute] in the ISF as you move deeper into the medulla
the countercurrent multiplier mechanism within the Loop of Henle
a. fluid flows in parallel tubes (descending and ascending limbs of the nephron loop) in opposite directions
b. descending limb - permeable to H2O, impermeable to NaCl
c. ascending limb - impermeable to H2O, permeable to NaCl
active NaCl pump (from filtrate →ISF)
d. as filtrate moves down the descending limb - H2O moves into the ISF (osmosis, and the filtrate becomes more and more concentrated)
e. highly concentrated filtrate enters the ascending limb where
NaCl pumped out against its concentration gradient (200 mOsm/L gradient, change in osmotic balance, increase difference)
f. when the filtrate leaves the ascending limb (=150 mOsm/L; urine should get more dilute) it has lower osmolarity than plasma due to
ascending limb being impermeable to H2O
ascending limb actively transporting NaCl out into the ISF
the countercurrent multiplier mechanism within the early DCT
more salt removed from filtrate (reabsorbed), no H2O removed, therefore ~100 mOsm/L when enters late DCT
urine production
filtrate (100 mOsm/L) enters late DCT, CD
average = 1-1.5L/day
urine may be?
concentrated
dilute
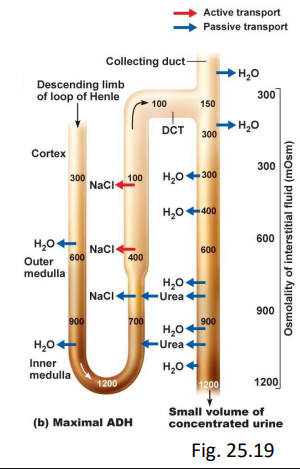
characteristics of concentrated urine
dehydrated, low bp
in late DCT, CD:
aldosterone ⇑ Na+ reabsorb
ADH ⇑ facultative H2O reabsorb (responds to need)
urine can be up to 1200 mOsm/L
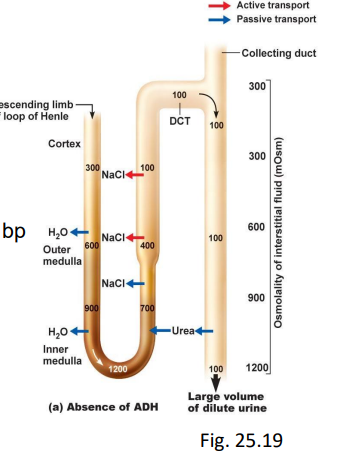
characteristics of dilute urine
excess plasma H2O, high bp
in late DCT, CD:
ANP inhibits ADH, aldosterone - impermeable to H2O, NaCl
what contributes to the regulation of urine?
hormonal
SNS
hormonal regulation of urine
renin-angiotensin system
ADH
aldosterone
ANP
hormonal regulation of urine: renin-angiotensin system
renin from juxtaglomerular cells
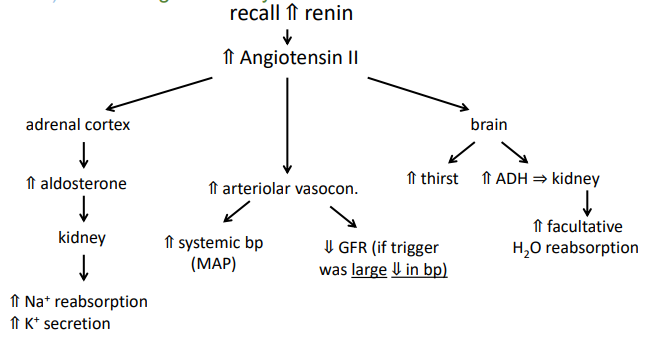
renin-angiotensin system: get ⇑ renin when:
i. ⇓ stretch of juxtaglomerular cells (i.e. ⇓ bp or blood volume)
ii. ⇑ SNS activity (systemic vasoconstriction)
iii. ⇓ NaCl in filtrate (detected at macula densa)
renin-angiotensin system: get ⇓ renin when:
i. ⇑ stretch of juxtaglomerular cells (i.e. ⇑ bp or blood volume)
ii. ⇑ ADH, angiotensin II
iii. ⇑ NaCl in filtrate iv. ⇓ SNS activity
hormonal regulation of urine: ADH
⇑ facultative reabsorption H2O (late DCT, CD)
hormonal regulation of urine: ADH ⇑ if
low bp volume
⇑ plasma osmolarity (concentration) reabsorbed H2O
⇑ angiotensin II
nicotine, nausea (can dilute urine)
maintain blood volume
hormonal regulation of urine: ADH ⇓ if
increased blood volume
⇓ plasma osmolarity
⇓ angiotensin II
⇑ ANP
alcohol (reabsorbing LESS H2O and excreting more)
what is diabetes insipidus?
body does not produce ADH or kidneys do not respond to ADH
result = large amounts of dilute urine and increased thirst
don’t produce ADH because do not have ADH receptors
can’t produce concentrate urine
hormonal regulation of urine: aldosterone (= steroid hormone)
⇑ aldosterone when ⇑ angiotensin II or high plasma K+
turns on genes that ⇑ number of Na+ /K+ - ATPase in late DCT, CD
⇑ Na+ reabsorption in late DCT, CD ∴ H2O follows (osmosis, Cl- follows (charge)
⇑ K+ secretion (Na+/K+ ATPase)
hormonal regulation of urine: ANP
⇑ blood pressure causes the release of ANP. effects of ANP include:
⇓ renin
⇓ ADH (inhibit function by preventing permeability of H2O after Na+/K+ exchange
⇓ aldosterone
⇓ vasoconstriction (cause vasodilation to decrease bp)
all of the above lead to ⇑ urine volume (more water out, reduces blood pressure) -ve
regulation of urine: SNS (no PSNS)
⇑ SNS impulses ⇒ afferent and efferent arterioles constrict
⇓ SNS impulses ⇒ afferent and efferent arterioles relax
Effect of SNS on kidney arterioles
↑ SNS → vasoconstriction (afferent + efferent) → ↓ GFR
↓ SNS → vasodilation → ↑ GFR
What happens to GFR when MAP increases?
Kidney auto-regulates
→ Afferent arteriole constricts
→ GFR returns to normal (constant)
Why is GFR kept constant despite BP changes?
Intrinsic mechanisms (myogenic response) override hormones/SNS
→ keeps filtration stable
What happens when BP/volume drops significantly?
Strong SNS + hormones → vasoconstriction
→ ↓ GFR to conserve fluid
What happens without ADH and aldosterone?
↓ water reabsorption → dilute urine
→ ↓ blood volume → ↓ MAPhormones correct BP, and GFR is kept constant
what are normal urine constituents?
H2O
nitrogenous wastes
regulated substances e.g. ions
pH 4.5-8.0 (ave = 6.0)
what are the nitrogenous wastes?
urea - from amino acid metabolism ~50% reabsorbed
uric acid - from nucleic acid breakdown - secreted, ~10% reabsorbed
poorly water soluble - accumulation = gout (in joints) or kidney stones
creatinine - from breakdown of creatine in skeletal muscle (excersie)
production/excretion constant, no reabsorption (no transporters for it)
used to estimate GFR - can indicate kidney disease before symptoms occur
what are the abnormal urine consistuents?
proteins - proteinuria (aka albuminuria) - due to increased permeability of glomerulus
due to e.g. heavy metals, glomerulonephritis
larger proteins that are meant to stay, end up in urine
glucose - glycosuria
temporary e.g. IV glucose (put more glucose in system)
pathological e.g. diabetes mellitus - high blood glucose (no insulin, or receptors not responding)
too much glucose being dumped and it cannot transport it out fast enough
doesn’t affect tubular reabsorption → more issue that insulin doesn’t work
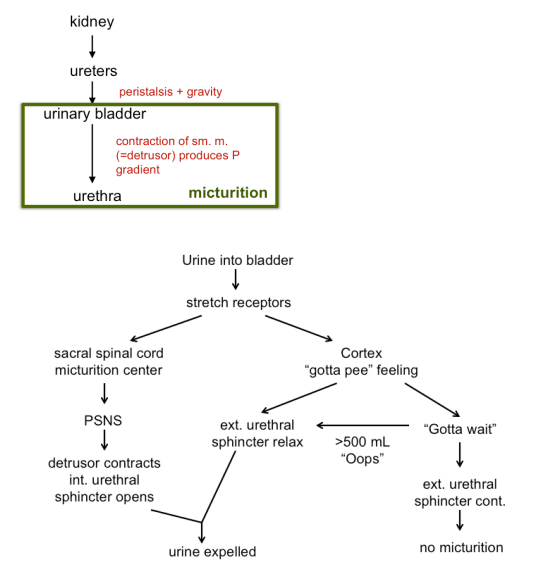
what is the micturition (bladder) reflex?
involuntary reflex in response to bladder stretching that causes the bladder to contract and internal urethral sphincter to relax, initiating the urge to urinate (peeing reflex)
what is renal plasma clearance?
volume of plasma from which the kidneys are able to completely remove a substance in one minuet (shows how efficiently the kidneys can eliminate that substance)
eliminated drug and hormones
What does renal plasma clearance indicate?
How efficiently the kidneys remove a substance
Why is renal plasma clearance important?
Estimates how long a substance (e.g. drug) stays in the blood
plasma clearance of substance

insulin can be used to estimate GFR
completely filtered but not reabsorbed, secreted or metabolized (comes out in urine)
therefore, amount of insulin in urine = amount filtered (should get 100% filtered but not reabsorbed)
what does it mean that inulin is “completely filtered”?
all inulin that enters the filtrate ends up in urine
→ nothing is added or removed along the nephron
how do you interpret plasma clearance (PC) vs GFR?
PC = GFR → no reabsorption or secretion
PC < GFR → substance is reabsorbed
PC > GFR → substance is secreted
examples of PC compared to GFR
PC < GFR → urea ~75 mL/min (50% reabsorption), glucose (100% reabsorption, PC = 0)
PC > GFR → penicillin, H+ (secretion)
e.g. if urine volume = 4mL/min; [inulin] in urine = 62.5g/L, and [inulin] in plasma = 2 g/L

what is acid-base balance
regulation of free H+ in ECF
H+ normally produced by metabolism
body pH

H+ buffered (to prevent change in pH) then eliminated by?
respiratory system (breathe out CO2)
renal system
what are buffer systems?
= pair of chemicals
balance of bases and acids minimize pH changes
what do bases take up?
H+ (remove them from solution) (-)
what do acids give up?
H+ (add them to solution) (+)
what is the major buffer in the blood?
bicarbonate system
can go both ways
