Ch 19 LO: Renal physiology
1/19
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
20 Terms
19.1.1 What are the 6 functions of the kidney?
Regulation of MAP and blood volume
Work with CVS to maintain ECF volume
Regulation of osmolarity
Tied to behavioral drives, including thirst
Ion balance
Balance dietary intake with urinary loss (Na+, K+ and Ca2+)
pH homeostasis
Excretes H+ or HCO3- to maintain stable plasma pH
Excretion of wastes
Excrete metabolic wastes, or foreign substances (xenobiotics) Creatine, urea, uric acid
Production of hormones
Synthesizes erythropoietin (RBC production), renin (RAAS system), and vitamin D conversion
19.2.1 What is the anatomical path of a drop of water from Bowman’s capsule to urine leaving the body?
Bowman’s capsule →
Proximal tubule →
Loop of Henle (descending → ascending) →
Distal tubule →
Collecting duct →
Renal pelvis →
Ureter →
Bladder →
Urethra → Outside body
19.2.2 how do you trace a drop of blood from the renal artery to the renal vein?
Renal artery →
Segmental arteries →
Interlobar arteries →
Arcuate arteries →
Cortical radiate arteries →
Afferent arteriole →
Glomerulus →
Efferent arteriole →
Peritubular capillaries / vasa recta →
Venules →
Renal vein
19.2.3 what is the anatomical relationship between the vascular and tubular elements of a nephron? (diagram)
Blood vessels wrap around tubules → allows exchange (reabsorption & secretion)
19.3.1 What are the three processes of the nephron.
Filtration
Blood → tubule (Bowman’s capsule)Reabsorption
Tubule → blood (keeps useful stuff)Secretion
Blood → tubule (adds wastes)
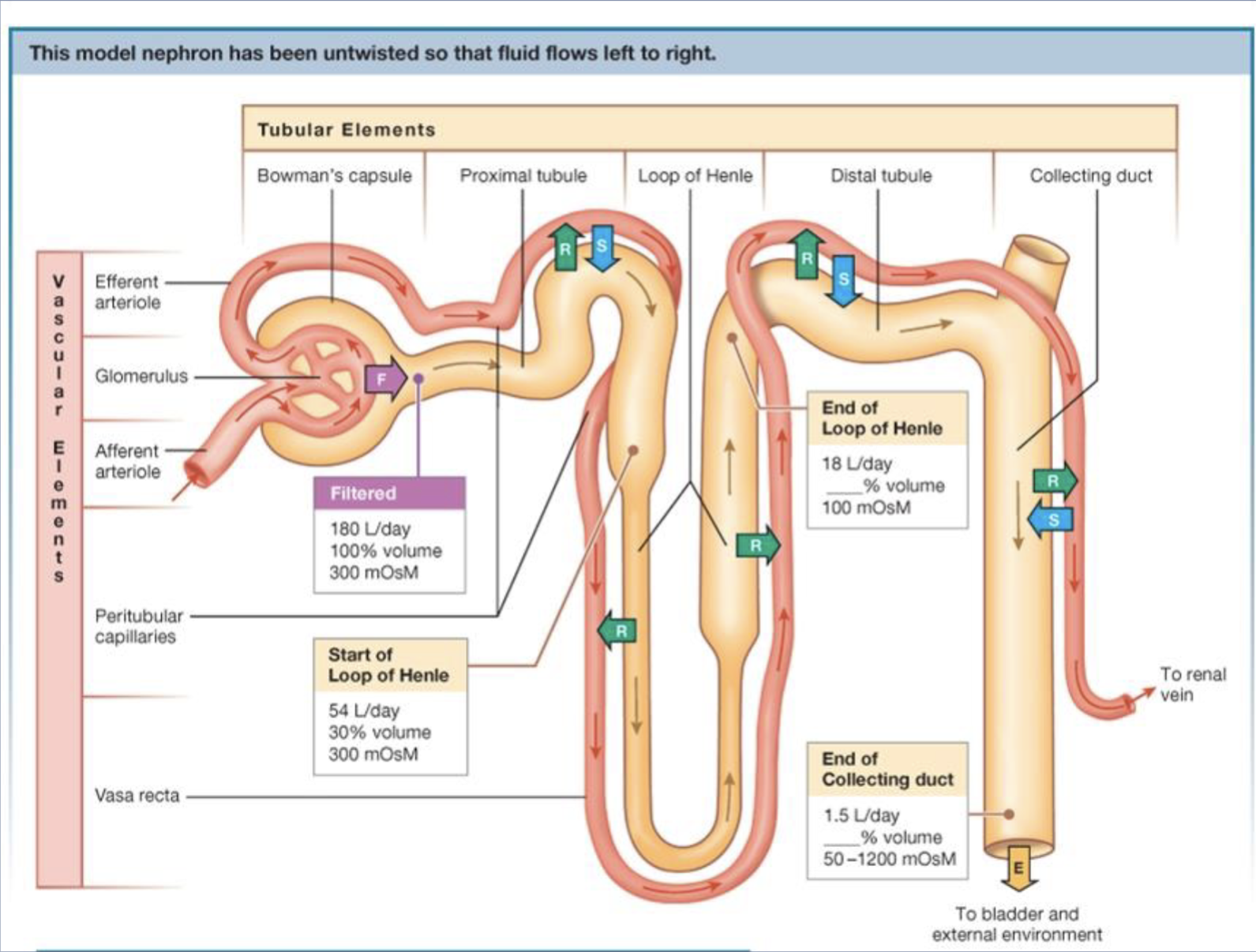
19.3.2 What is the volume and osmolarity changes of filtrate as it passes through each section of the nephron?
Bowman’s capsule:
~180 L/day, ~300 mOsm (isosmotic)Proximal tubule:
Volume ↓, still ~300 mOsmLoop of Henle:
Descending: water leaves → osmolarity ↑
Ascending: salt leaves → osmolarity ↓ (~100 mOsm)
Distal tubule & collecting duct:
Hormone-controlled → final urine (~1.5 L/day)
19.4.1 Describe the filtration barriers between the blood and the lumen of the nephron and explain how they can be modified to
control filtration
Three barriers to filtration:
Glomerular capillary endothelium
• Fenestrated capillaries
• Blood cells are not filtered
• Negatively charged surface repels most proteins
Basal lamina
• Extracellular matrix fibers act as a course sieve
(net)
• Blocks proteins
Podocytes
• Octopus-shaped cells wrap around glomerular
capillaries
19.4.2 Describe the pressures that promote and oppose glomerular filtration.
Promote filtration:
Glomerular hydrostatic pressure (~55 mmHg)
fluid pushing on the walls, primary force that pushes blood to filtrate (sets up filtrate).
Oppose filtration:
Osmotic pressure (~30 mmHg)
proteins in plasma promote reabsorption
Colloid capsule pressure (~15 mmHg)
bowman’s capsule hydrostatic pressure
👉 Net filtration ≈ 10 mmHg outward
19.4.3 Define glomerular filtration rate and give average values for GFR.
Glomerular Filtration Rate (GFR)
Volume of fluid that filters into the
GF pressure = hydrostatic pressure - colloid osmotic - capsule pressure
Bowman's capsule per unit of time
Average GFR is 125 mL/min (180 L/day)
indicator of kidney function
19.4.4 Explain how GFR can be influenced by local and reflex control mechanisms.
Local (autoregulation):
Myogenic autoregulation (afferent arteriole constriction in response to high MAP, strech)
Tubuloglomerular feedback (macula densa detects changes in filtration rate)
External:
Sympathetic nervous system (decreased GFR)
Hormones
angiotensin II - vasoconstrictor, especially of efferent arteriole
prostaglandins - vasodilator
19.5.1 – Distinguish between transcellular transport and paracellular pathways.
Transcellular: through cells (membranes)
Paracellular: between cells (tight junctions)
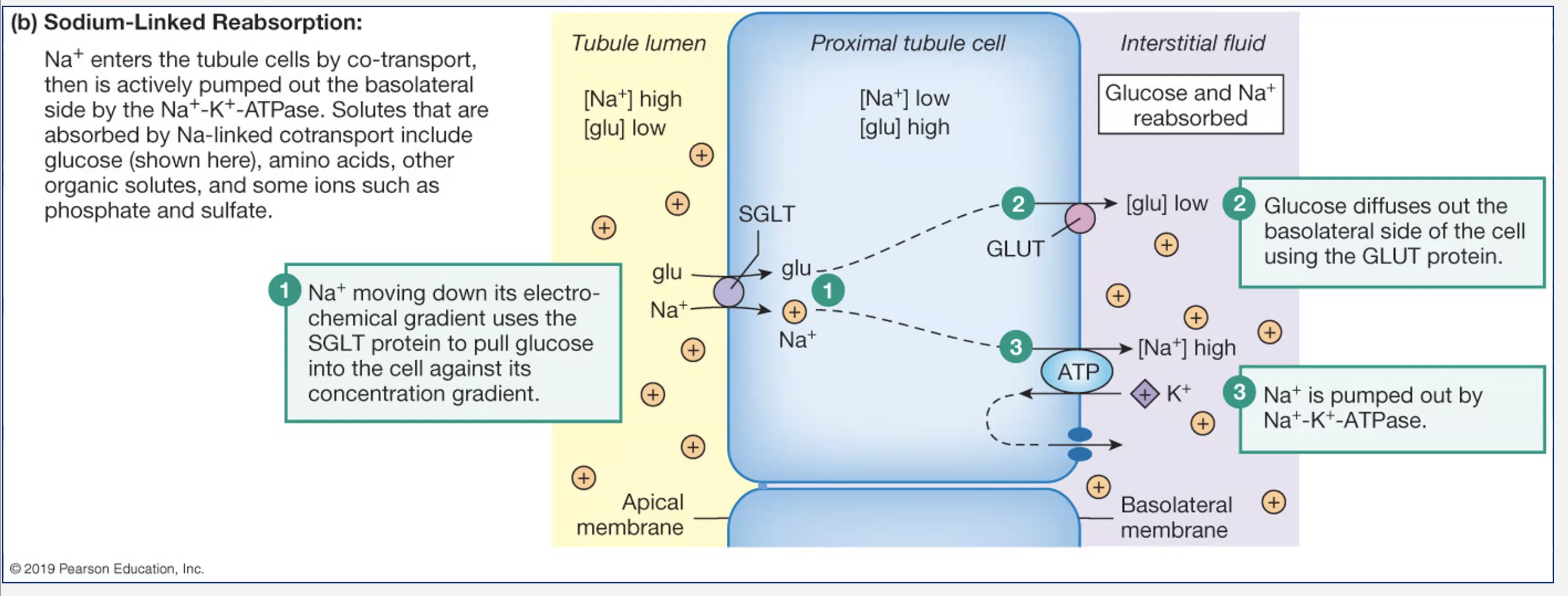
19.5.2 Describe and give examples of active and passive reabsorption in the proximal tubule.
Active:
Na⁺ (primary driver via Na⁺/K⁺ pump)
active because there is high Na+ on both sides
Glucose (SGLT transporters)
Passive:
anions (-) that move following the electrical gradient of sodium
Water (osmosis)
follows solute reabsorption to keep equilibrium
urea - passive diffusion, paracellular.
19.5.2.5 Sodium linked reabsorption in proximal tubule
LO 19.5.3 – Using glucose, create graphs to show filtration, transport maximum, and renal threshold of a substance reabsorbed by protein-mediated transport.
Type-1 diabetes and glucose transport illustrate reabsorption and saturation
• 100% glucose is filtered at glomerulus
• Normally, 100% glucose is reabsorbed in prox. tubule
Lack of insulin → high [glucose] in blood → high
[glucose] in filtrate
• Glucose transporters get saturated with glucose
• Glucose is excreted in urine instead
![<p>Type-1 diabetes and glucose transport illustrate reabsorption and saturation</p><p>• 100% glucose is filtered at glomerulus</p><p>• Normally, 100% glucose is reabsorbed in prox. tubule</p><p>Lack of insulin → high [glucose] in blood → high</p><p>[glucose] in filtrate</p><p>• Glucose transporters get saturated with glucose</p><p>• Glucose is excreted in urine instead</p><p></p>](https://assets.knowt.com/user-attachments/a43a52d5-3012-476b-8951-6baaecd4e00d.png)
LO 19.6.1 – Explain and give examples of the importance of tubular secretion in renal function.
Purpose:
eliminate drugs/toxins
regulate K⁺ and H⁺
Examples:
Enhances excretion of a given substance like:
• Xenobiotics
• K+ and H+
• Metabolites
• Organic anions
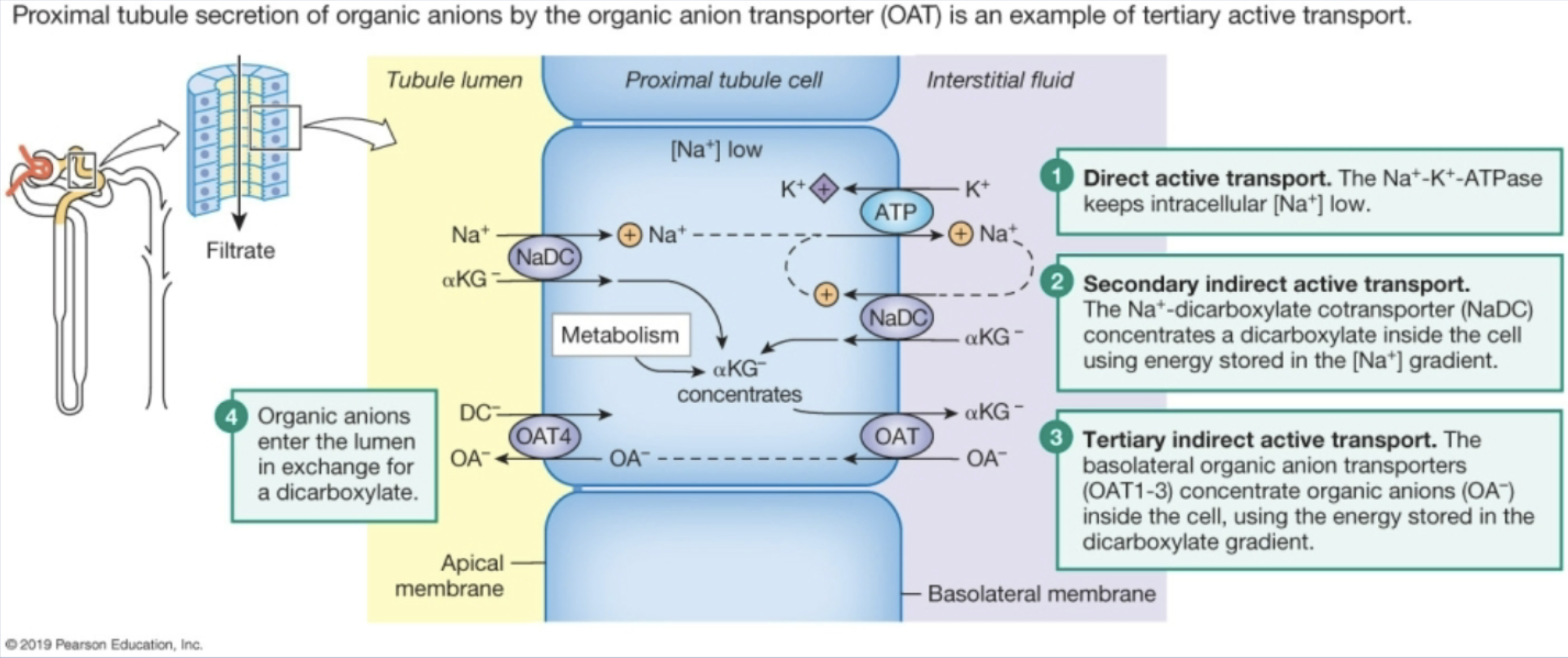
Diagram an example of tertiary active transport
Secretion of organic anions through OAT
sodium gradient moves along with dicarboxylates, creating dicarboxylate gradient in cell
OAT concentrates organic anions in the cell using energy from dicarboxylate gradient moving out.
LO 19.7.1 – Explain in words the relationship between the excretion of a solute and its renal clearance.
Relationship:
Excretion = Filtration − Reabsorption + Secretion
Clearance = how fast substance is removed from plasma
LO 19.7.2 – Explain how clearance can be used as an indirect indicator of renal handling of a solute.
Clearance = GFR → no reabsorption/secretion
Clearance < GFR → reabsorption
Clearance > GFR → secretion
Examples:
Inulin → GFR marker
Glucose → reabsorbed
Penicillin → secreted
what is the renal clearance formula?
Formula and variables:
C = (Ux x V)/Px
• C = renal clearance (mL/min)
• Ux = urine concentration of substance (mg/mL)
• V = volume of urine produced per minute (mL/min)
• Px = plasma concentration of substance (mg/mL)
what are important substance values for clearance?
creatinine & inulin - 100 % cleared bc freely filtered n none reabsorbed or secreted
glucose - 0% cleared because all gets reabsorbed to plasma
penicillin - 150% bc freely filtered AND half is secreted to urine as well