anatomic path final
1/108
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
109 Terms
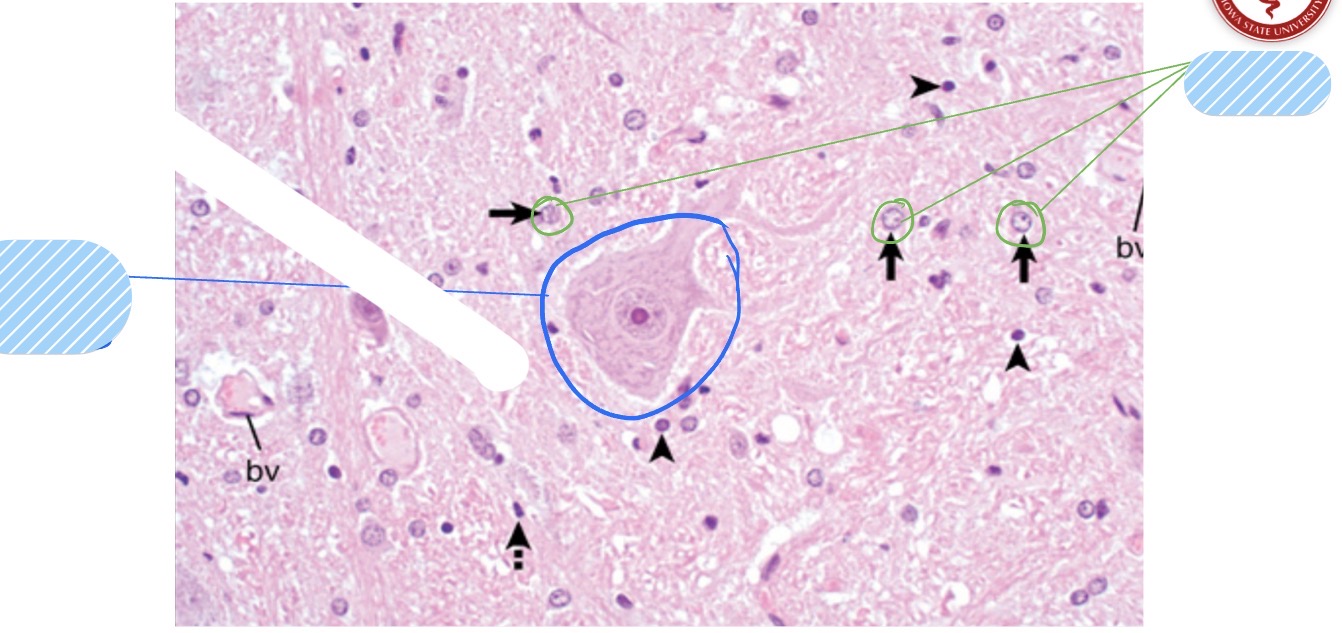
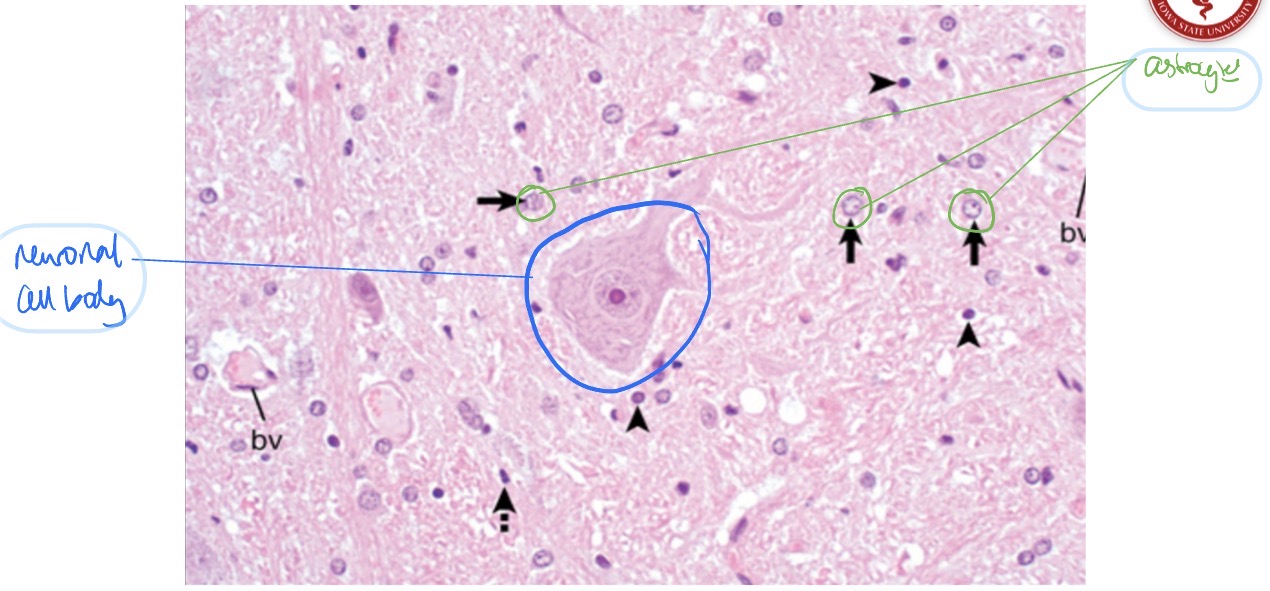
Most important neuroectodermal cells?
neurons
astrocytes
oligodendrocytes
schwann cells
ependymal cells
Most important mesenchymal cells of the CNS?
microglia
cells that make up the meninges
What is the functional unit of the nervous system?
neurons
Neurons are very hungry for ______ + ______, making them very ______ to physiological changes.They are ______-lived and have a _____ _____ of morphologies.
Neurons are very hungry for glucose + oxygen, making them very sensitive to physiological changes.
They are long-lived and have wide variety of morphologies
What is the most numerous glial cell type in the CNS? What are its fxns?
astrocytes
fxns
maintain extracellular environment
interconnect w/ other astrocytes to form a monitoring system
participate in the formation of the blood-brain barrier
remove excess NTs
participate in the CSF-brain barrier
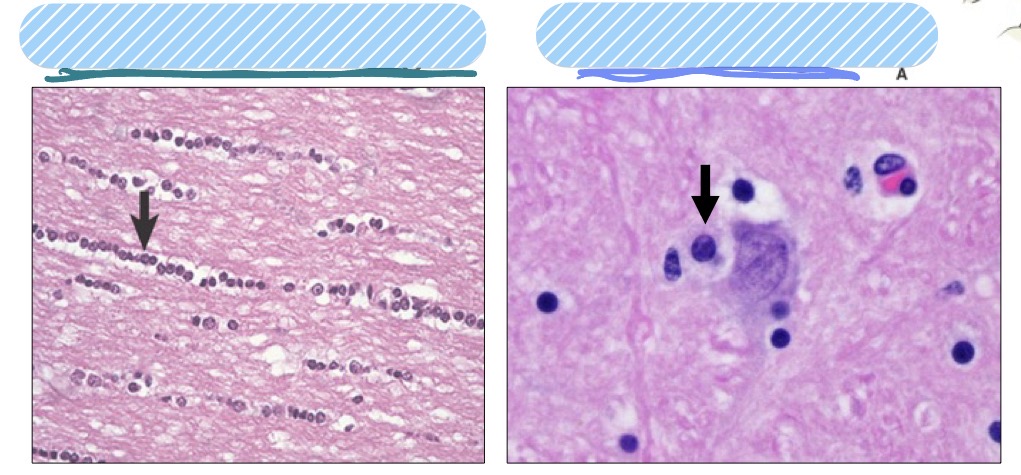
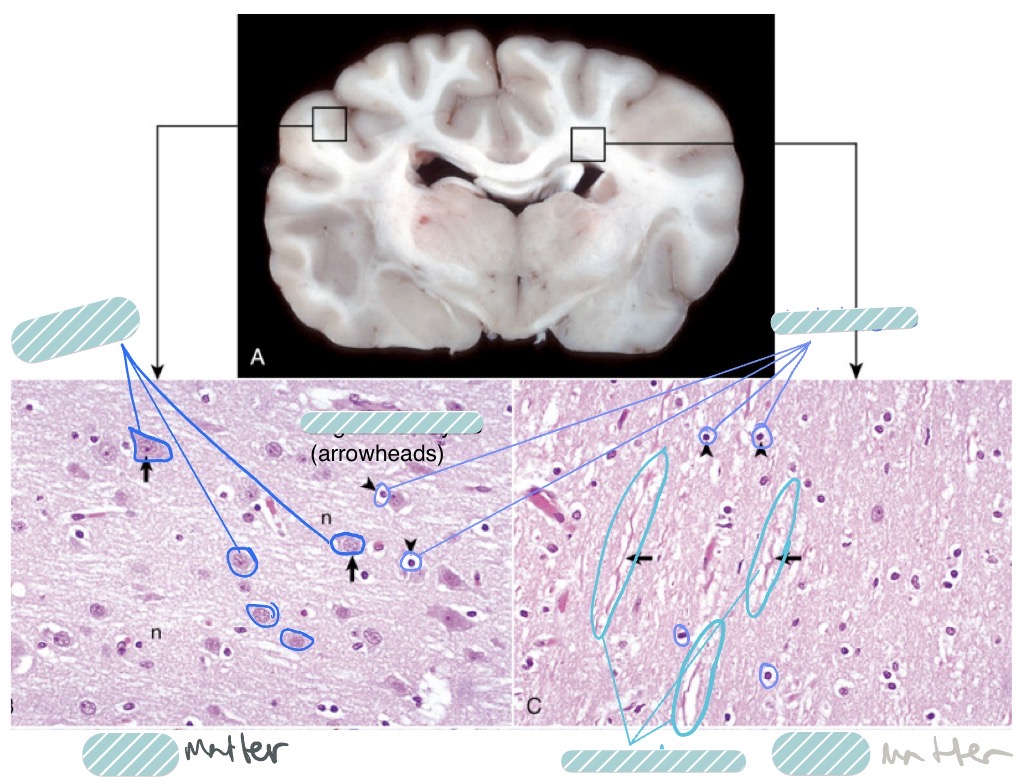
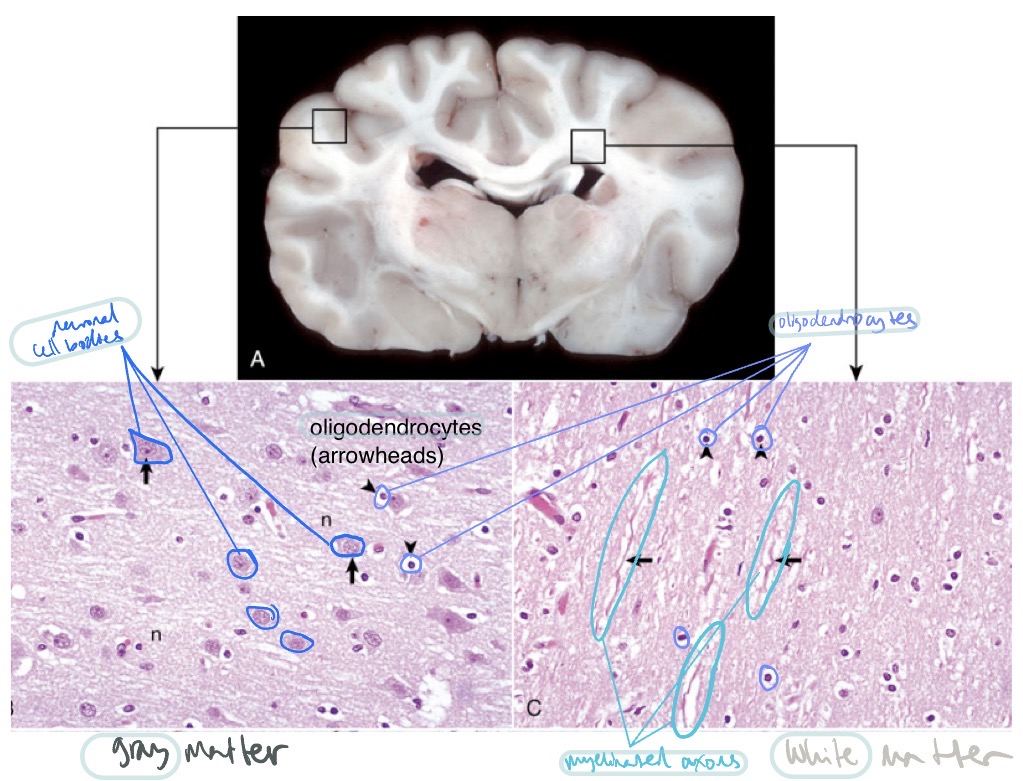
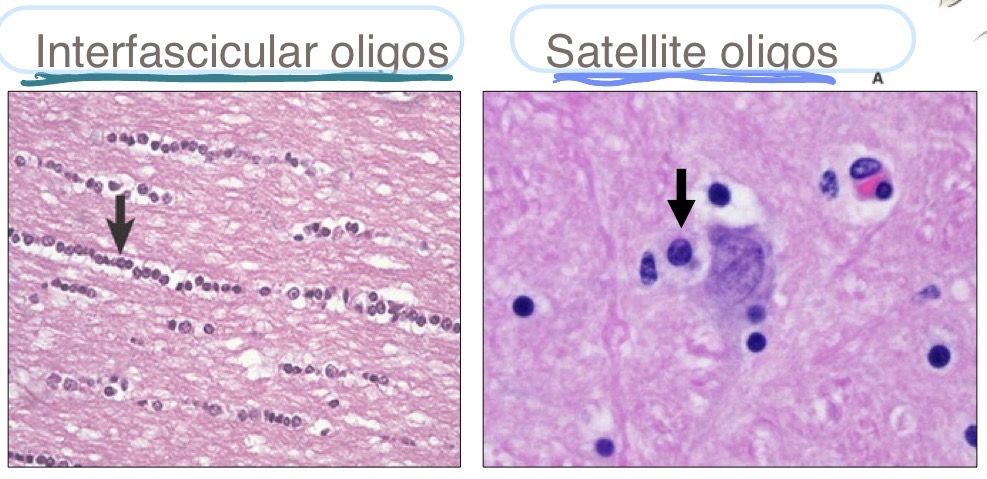
What are the 2 different types of oligodendrocytes, where are they found, and what do they do?
interfascicular oligodendrocytes
found b/t axons
fxn: make myelin
satellite oligodendrocytes
found surrounding neuronal cell bodies
fxn: regulate perineural microenvironment
What is the fxn of microglia?
resident macrophages of CNS
fxn: reactive proliferation, immunosurveillance, immunoregulation, and phagocytosis
Where are ependymal cells found + what is their fxn?
found as the epithelial cells lining the ventricular system
fxn:
produce CSF
circulate CSF
regulate flow of materials b/t CSF + CNS
What are the meninges + what is their fxn? Where is the subarachnoid space located + what stuff is inside of it?
meninges = layered membranes that surround the brain + spinal cord
fxns:
provide support
contain CSF
subarachnoid space is located b/t the arachnoid mater + pia mater (leptomeninges)
contains:
vasculature
nerves
CSF
List the cells of the CNS from most to least sensitive to injury
neurons > oligodendrocytes > astrocytes > microglia > blood vessels
The nervous system has _____ lymphatic vessels. Necrotic areas have _____ granulation tissue. This, combined w/ the fact that the nervous system is very _____, makes _____ necrosis followed by _____ common and demonstrates the unique way the nervous system responds to damage.
The nervous system has no lymphatic vessels.
makes it hard to drain fluid
Necrotic areas have no granulation tissue
meaning no fibroblasts depositing collagen
This, combined w/ the fact that the nervous system is very fatty, makes liquefactive necrosis followed by cavitation common and demonstrates the unique way the nervous system responds to damage.
Why is malacia a common sequelae of necrosis in the CNS?
high fat + macrophages eat up dead tissue + no granulation tissue being laid down (fibrosis) → loss of tissue → softening = malacia
What are the main glial cells that respond to dmg in the CNS? What do they do?
microgliosis + recruitment of blood monocytes
microglia + peripheral macrophages → become gitter cells and eat up dead tissue
astrocytosis
activated astrocytes hypertrophy, recruit other cells, try to fill in gaps in tissue
proliferative astrocytes are the CNS’s way of trying to copy fibroblasts
satellitosis
when activated astrocytes ± oligodendrocytes surround neurons
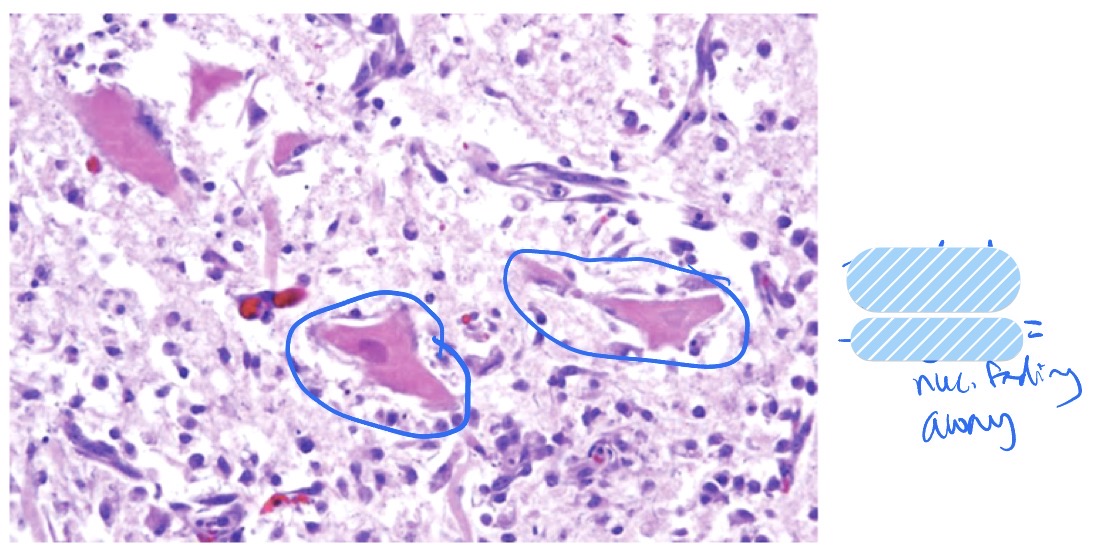
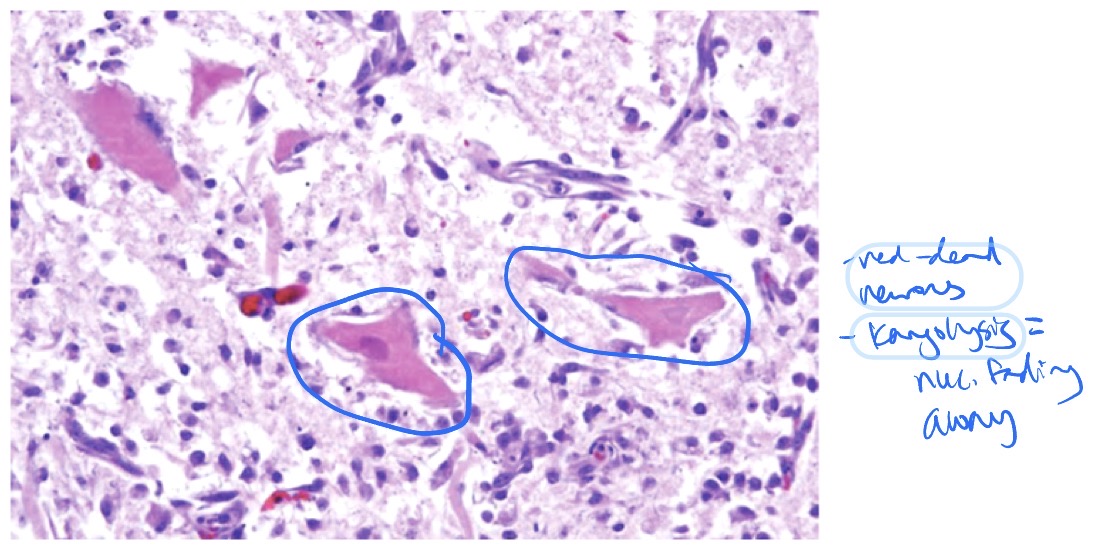
What is neuronal necrosis? What does it look like? What are the causes + outcomes?
neuronal necrosis = necrosis of neurons
appearance:
shrunken, hypereosinophilic, red = dead
astrocytosis + satellitosis
neuronophagia
causes:
hypoxia/ischemia
toxins
excitotoxins (excessive NTs can stimulate neurons to death)
viruses
outcomes:
lost neurons are not replaced bc they are terminally differentiated cells
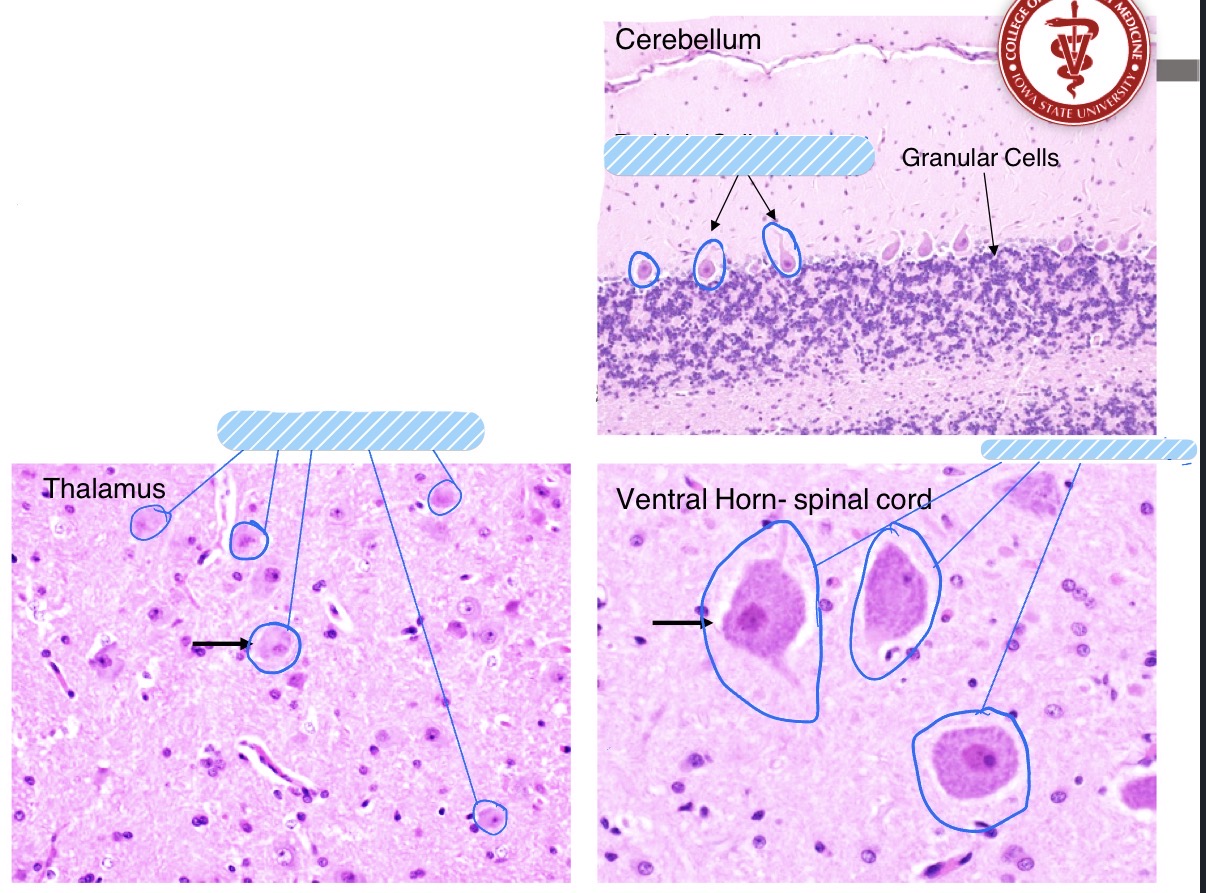
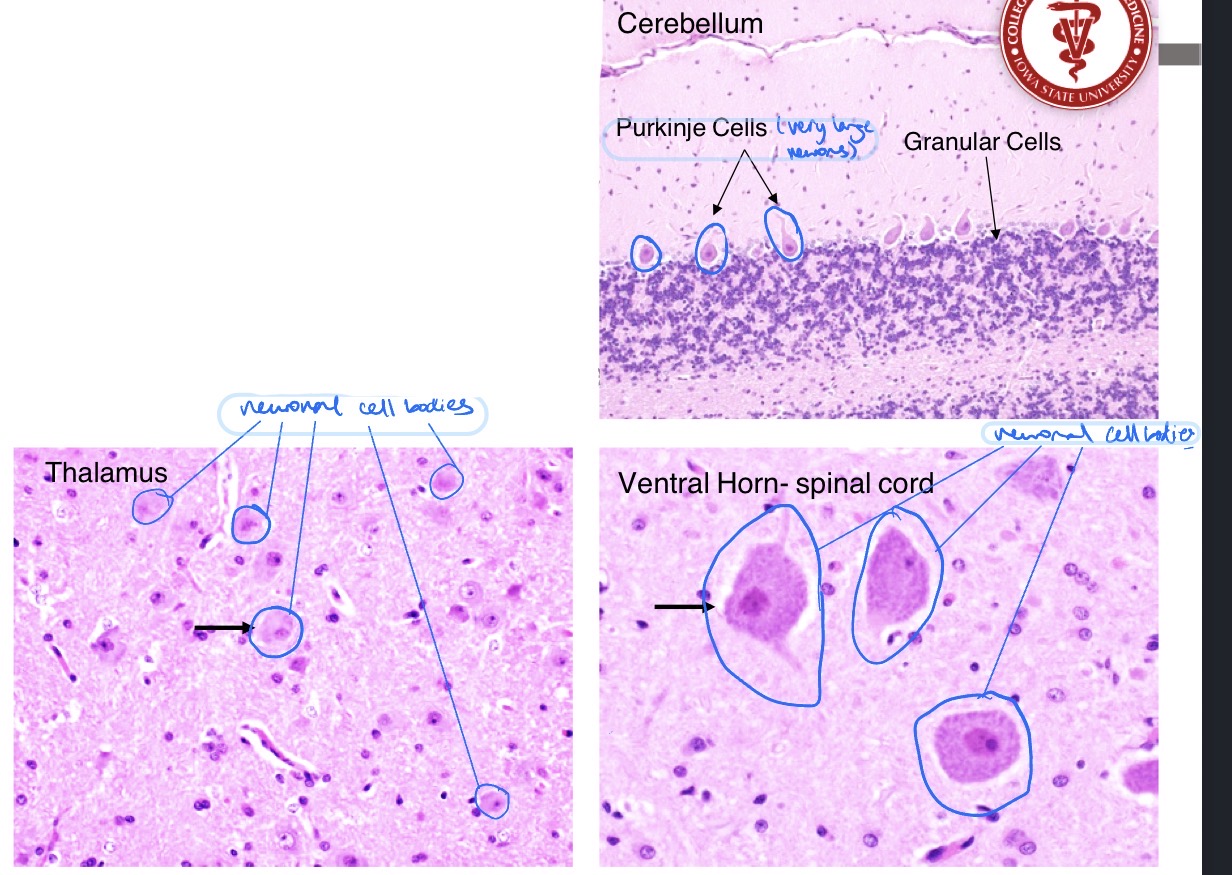
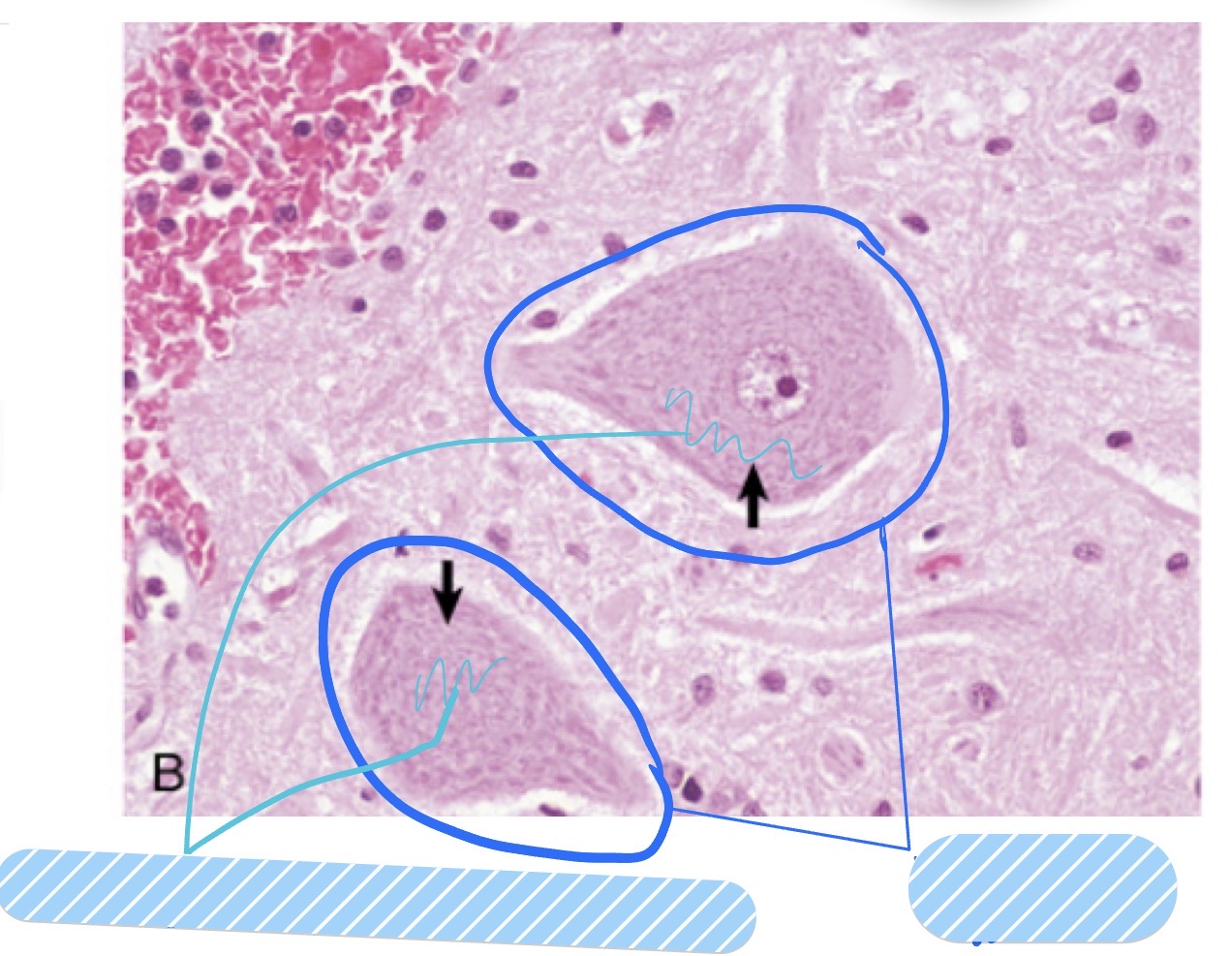
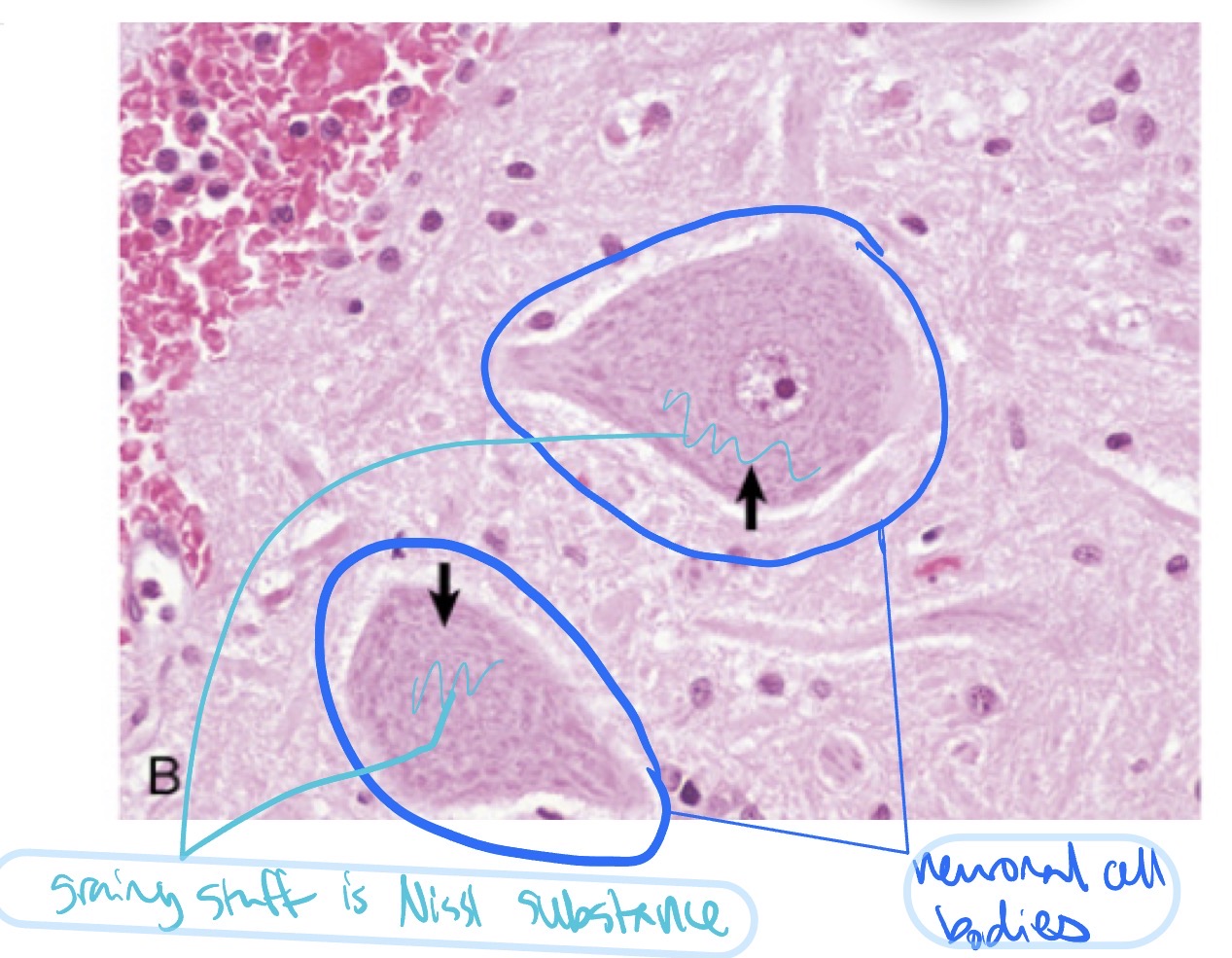
What is central chromatolysis? What does it look like? Causes?
reversible, sublethal change in neurons
appearance:
swollen cell bodies
loss of Nissl substance
causes:
axonal dmg
caused by: viruses, metabolic disturbances, toxins, nutritional deficiencies, infarctions, neuronal degen.
Where do bacterial hematogenous CNS diseases often occur?
Bacterial hematogenous CNS diseases often occur at the interface b/t gray + white matter in the brain bc of the abrupt change in vascular flow/luminal diameter
What happens in rapid vs slow ischemia in the CNS?
infarction = necrosis d/t ischemia
rapid ischemia → neurons die w/i minutes
slow ischemia → blood supply can adapt by anastomosing + compensating
What sequence of events led to this lesion? This cat also had bronchoalveolar carcinoma, is this lesion linked to the cancer?
vascular occlusion → ischemia → infarction → malacia
bronchoalveolar carcinoma metastasized to brain → cut off blood supply by occluding vasculature
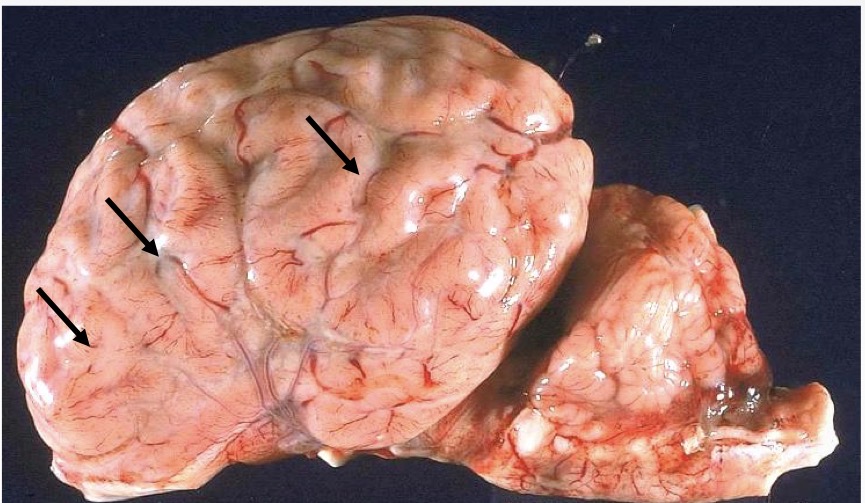
Name the lesion + observations that support that diagnosis
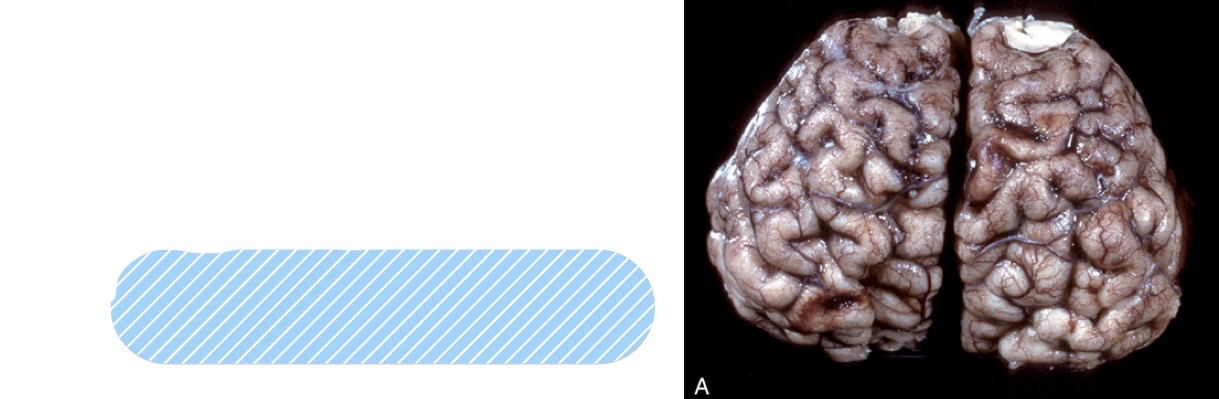
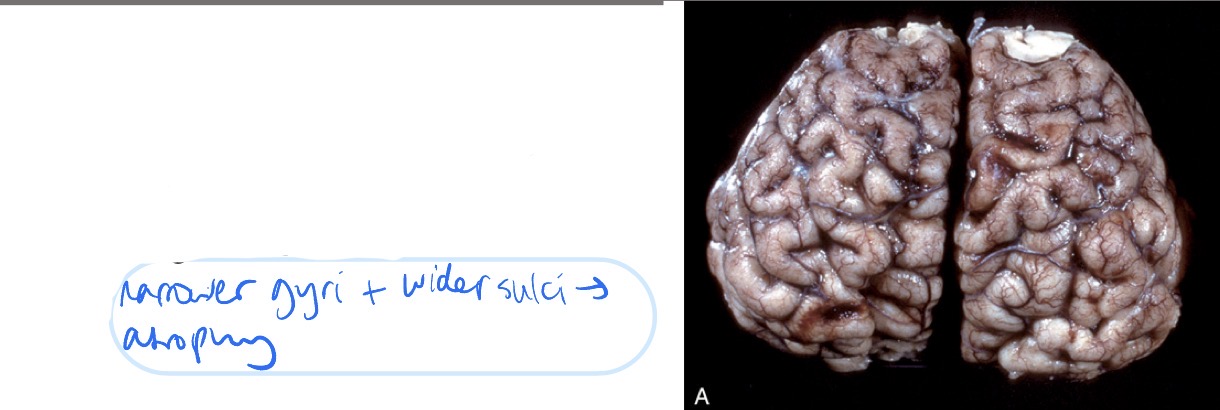
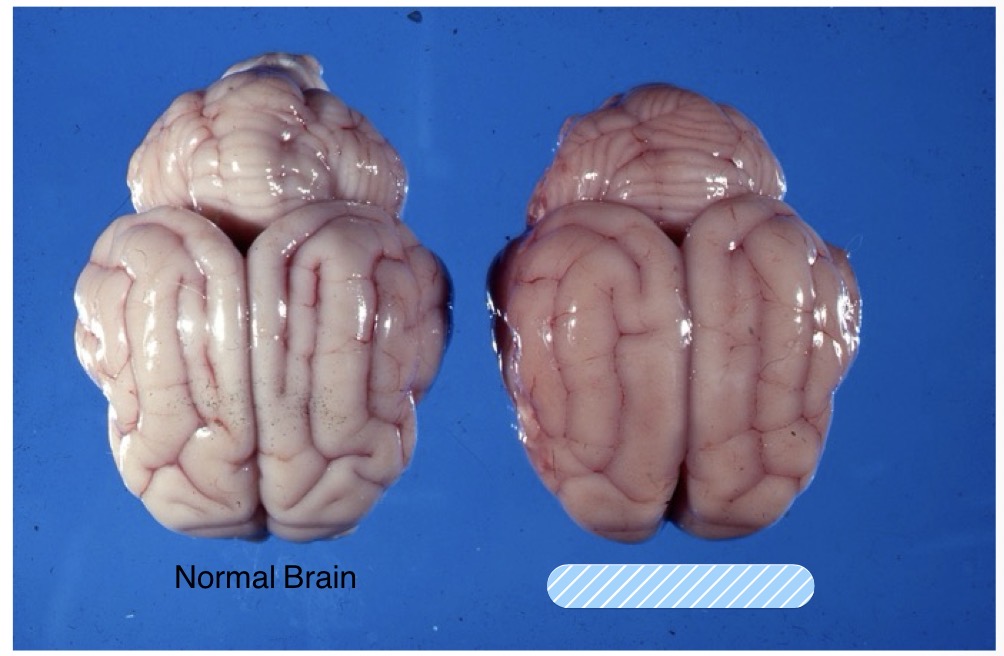
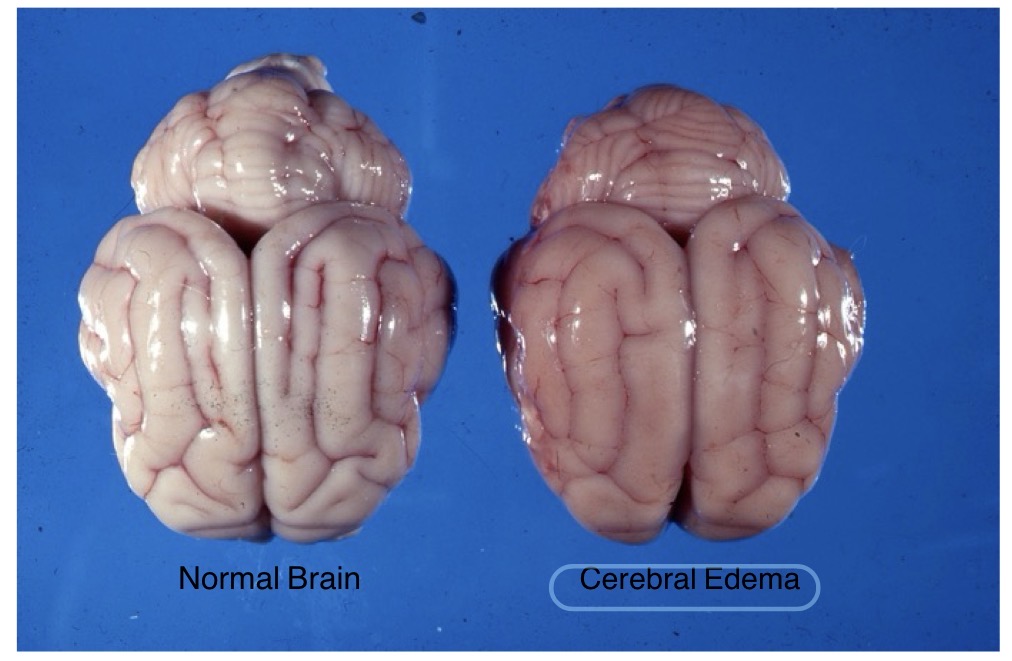
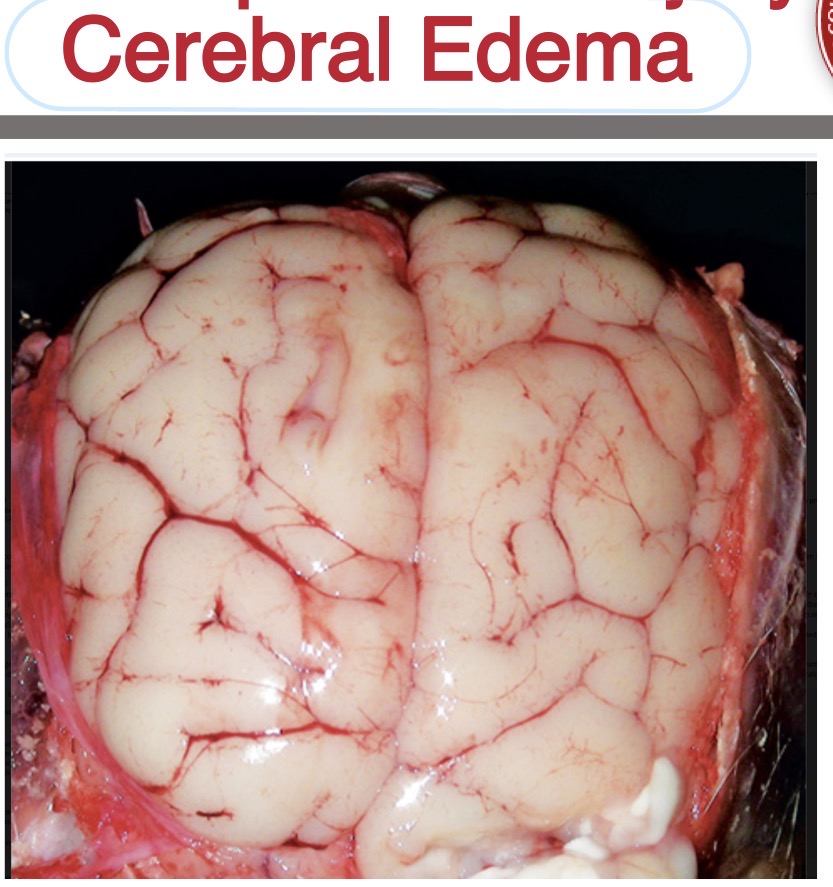
lesion: cerebral edema
observations:
widened gyri
less apparent sulci
diffusely swollen appearance
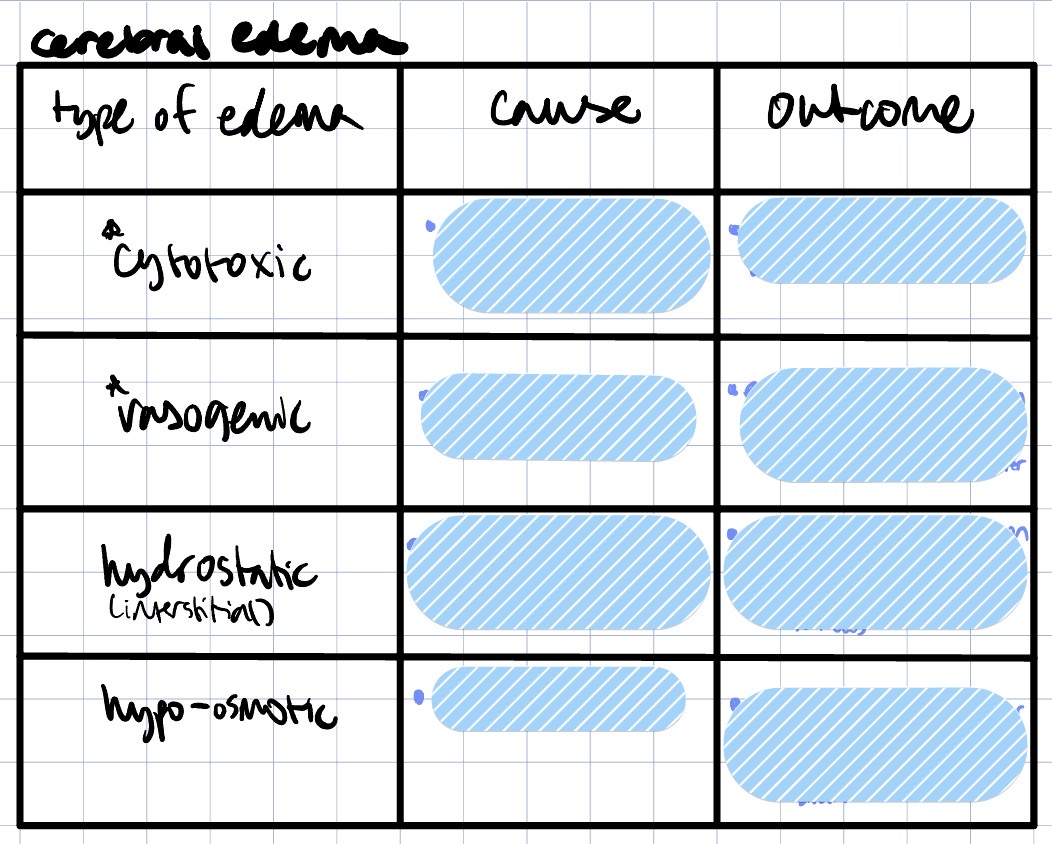
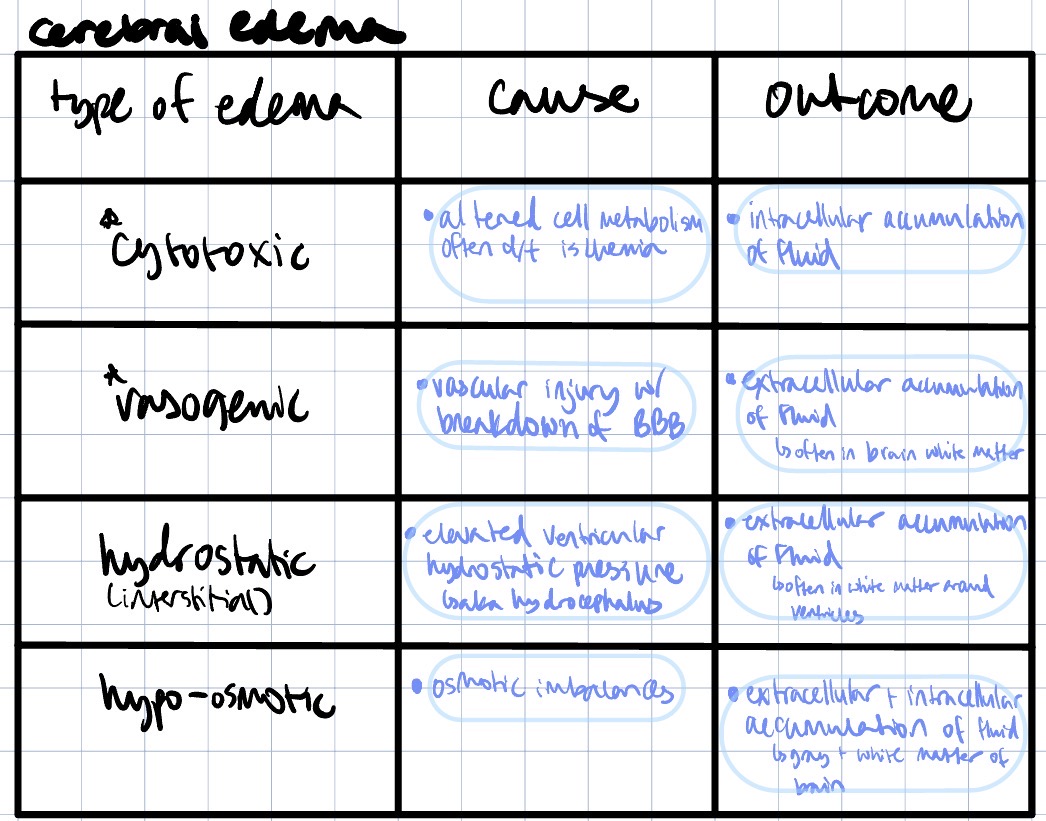
Which type is associated w/ hydropic degen? Which is associated w/ increased vascular permeability + inflammation?
hydropic degen → cytotoxic edema
increased vascular permeability + inflammation → vasogenic edema
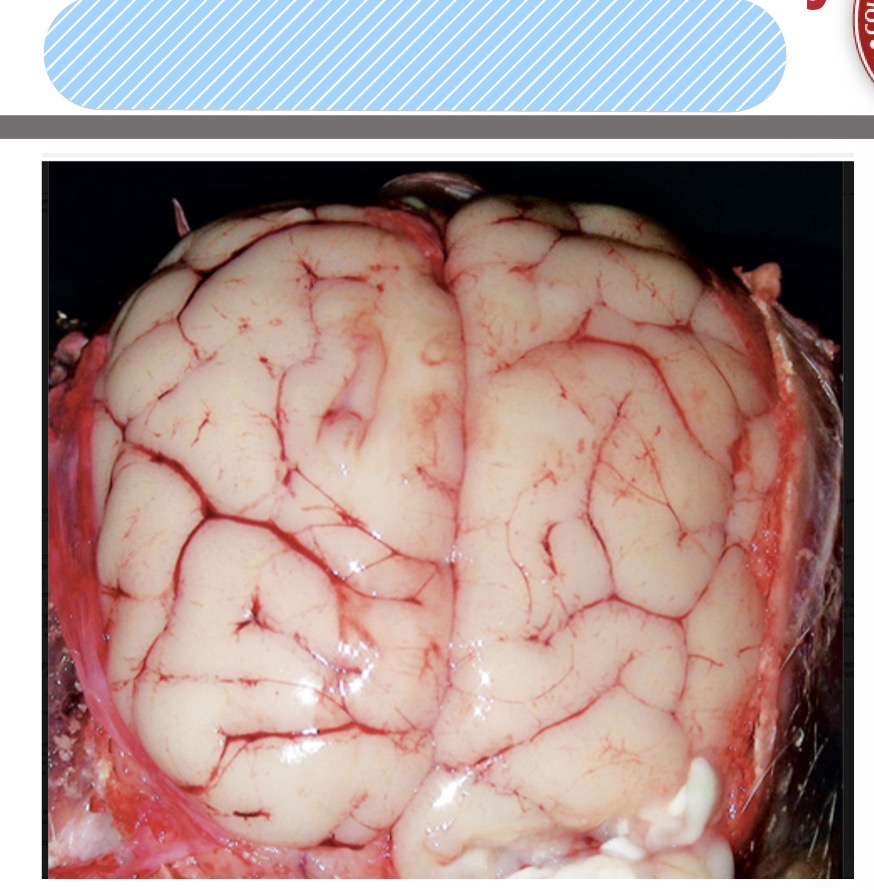
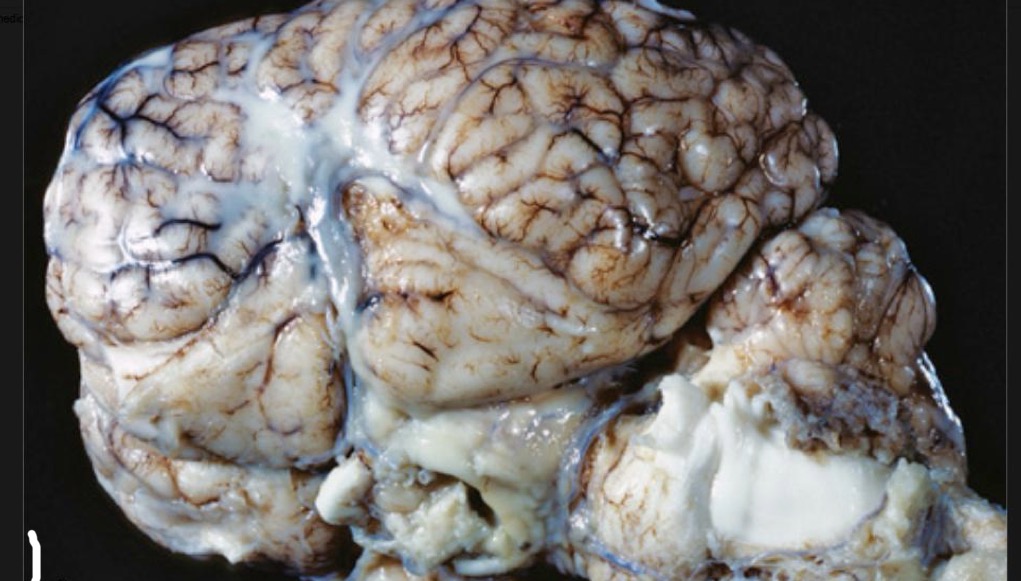
Name the lesion
brain, cerebral edema
4 portals of entry/pathways of spread into CNS + which is most common
direct extension
penetrating trauma, extensional infxns
ex) HBC, gunshot, etc
hematogenous = bloodstream
most common
leukocyte trafficking = agents hitch a ride on macrophages + lymphocytes
ex) bac, viruses, protozoa
retrograde axonal transport = agents invade via peripheral nerves + axons
ex) rabies, Listeria
5 defense mechanisms/barrier systems of the CNS + what they’re composed of
blood-brain barrier
endothelial cells + BM + astrocytic endfeet
glia limitans
astrocytic endfeet + pia mater
blood-CSF barrier
choroid plexus + arachnoid
CSF-brain barrier (ependymal barrier)
ependymal epithelial cells + astrocytic endfeet
innate + adaptive immune system
For patterns of inflammation in the CNS:
serous to suppurative/purulent responses can be the result of _____ _____.
eosinophil responses occur in _____ _____ of pigs and in _____ _____ _____.
lymphoplasmacytic + histiocytic responses can be caused by _____ + _____
granulomatous inflammation can be the result of infection by _____, ______. and some _____ species like ______.
serous to suppurative/purulent responses can be the result of bacterial infection.
eosinophil responses occur in salt poisoning of pigs and in parasitic larval migration.
lymphoplasmacytic + histiocytic responses can be caused by viruses + protozoa.
granulomatous inflammation can be the result of infection by fungi, protozoa, and some bacteria species like Mycobacterium.
Define hydrocephalus vs hydranencephaly. List causes for each
hydrocephalus = dilation of the ventricular system d/t CSF accumulation in the ventricles or subarachnoid space
lined by ependymal cells
brain tissue compressed
causes: in utero viral infxn, developmental abnormality of the ependymal cells/ventricular system, breed disposition
hydranencephaly = a CSF-filled cavity replacing the cerebral hemispheres
cavity not lined by ependymal cells
little/no cerebrum
causes: teratogenic viral infxns, toxin exposure, nutrient deficiencies
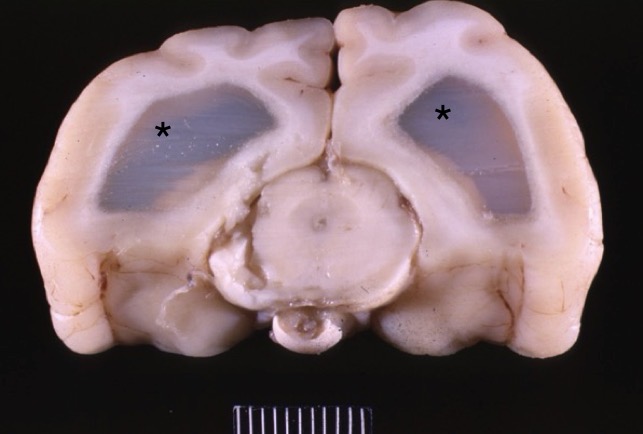
Name lesion + supporting observations
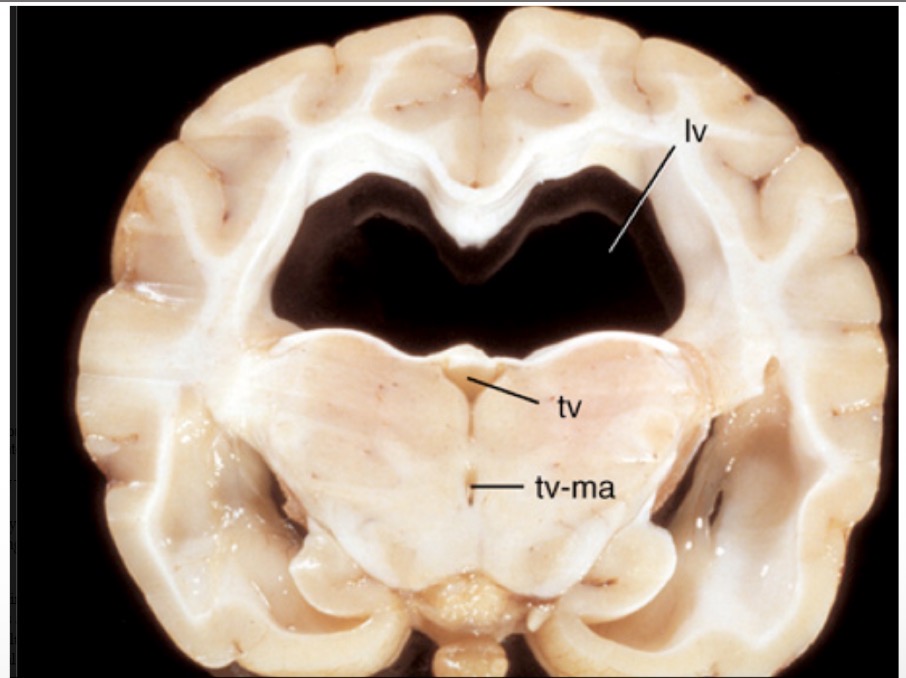
lesion: hydrocephalus
observations:
bilateral dilation of lateral ventricles
Name it
brain hydranencephaly
Name the lesion in this calf + provide a possible pathogenesis. What kind of developmental disturbance would it be?
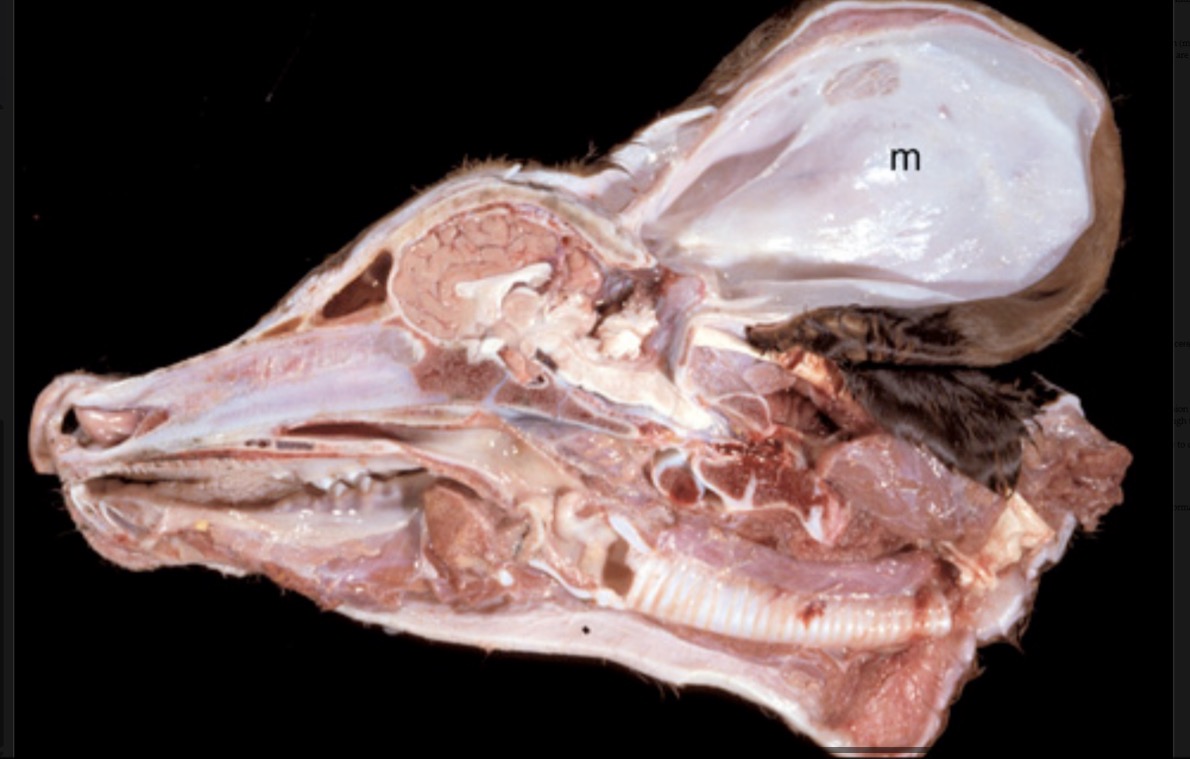
brain: meningocele
pathogenesis: congenital defect in caudodorsal aspect of skulll allowed meninges to herniate into a large pouch only covered by skin
developmental disturbance: dysplasia
What is an abscess? What portals of entry usually cause cerebral abscesses to occur? What is the exudate called?
abscess = localized collection of pus w/i a fibrous capsule
common portals of entry:
direct extension
hematogenous
exudate: purulent/suppurative
morph it
brain: severe, acute, multifocal, necrosuppurative/purulent encephalitis
lesion: cerebral abscess
What is meningitis? What is the most common pathogenesis in domestic animal species?
meningitis = inflammation of the meninges
most commonly caused by bacteria like E. coli + Streptococcus infiltrating leptomeninges + subarachnoid space hematogenously in domestic animal species
morph this tissue from a calf
meninges: severe, acute, diffuse fibrinopurulent meningitis
morph this tissue from a horse
meninges: severe, acute, diffuse fibrinopurulent meningitis
Lymphocytic inflammation in the CNS is often indicative of what kind of infection?
viral
What are the 3 classifications of mycoses?
systemic/deep mycoses = systemic spread throughout body + internal organs
angioinvasive fungi = invade blood vessel walls
superficial mycoses = infxn limited to just surfaces of skin, hair, etc
What are the 4 major systemic mycoses?
histoplasmosis
cryptococcosis
blastomycosis
coccidioidomycosis
Granulomatous inflammation in the CNS is often caused by infection of what?
fungi
protozoa
some bacteria like Mycobacterium
What are the 3 major viral neurological diseases in the horse?
rabies
arboviral encephalomyelitis
equine herpesvirus 1
What is the pathogenesis of equine protozoal myelitis?
sporocysts of Sarcocystis neurona passed in feces of opossum (definitive host) → horse ingests contaminated feed/water → virus enters CNS via leukocyte trafficking → parasite activates + replicates in CNS → lymphoplasmacytic inflammation + necrosis
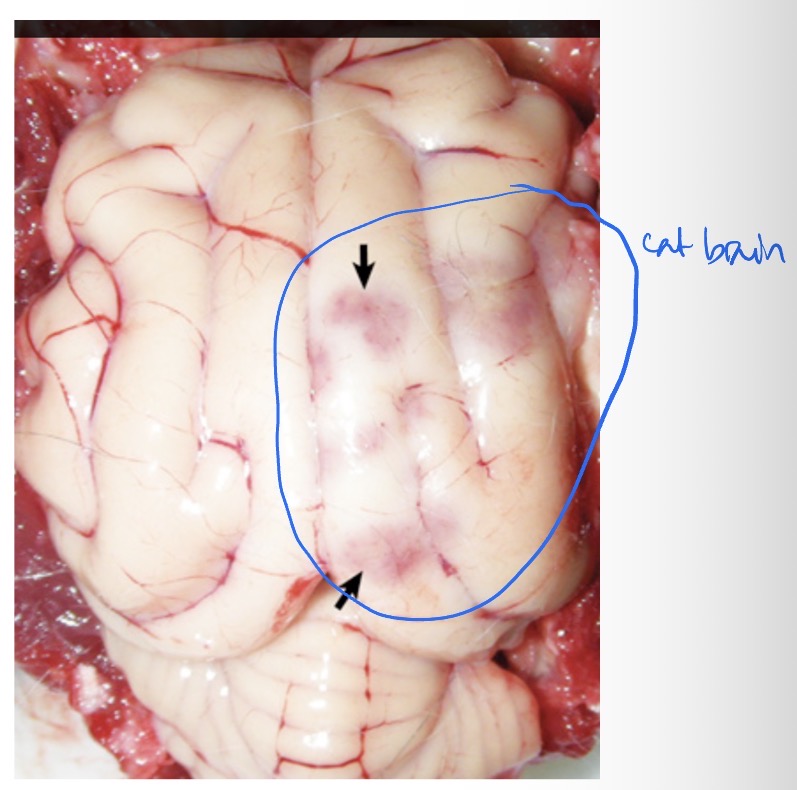
What is this lesion?
equine protozoal myelitis causing a focal area of hemorrhage
What is this lesion in this horse? What is it likely caused by?
brain: verminous encephalitis
likely caused by aberrant migration + hematogenous spread of nematode parasites
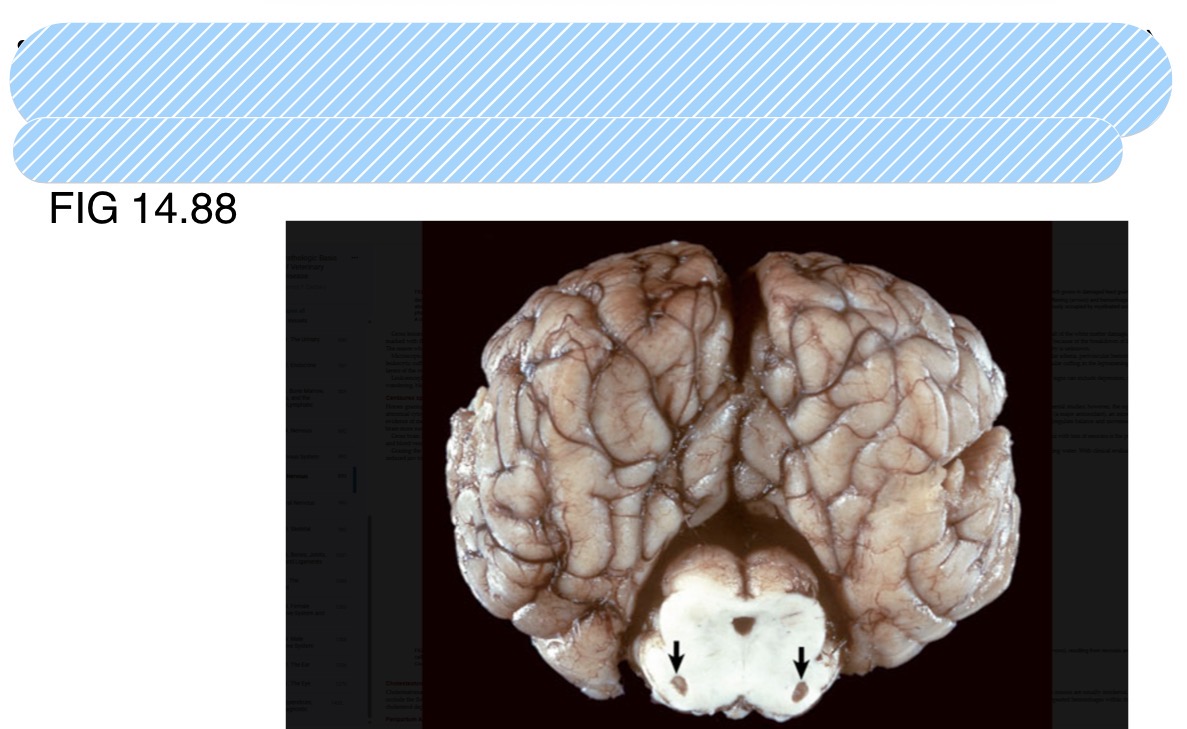
What is this lesion in a horse + what is it caused by?
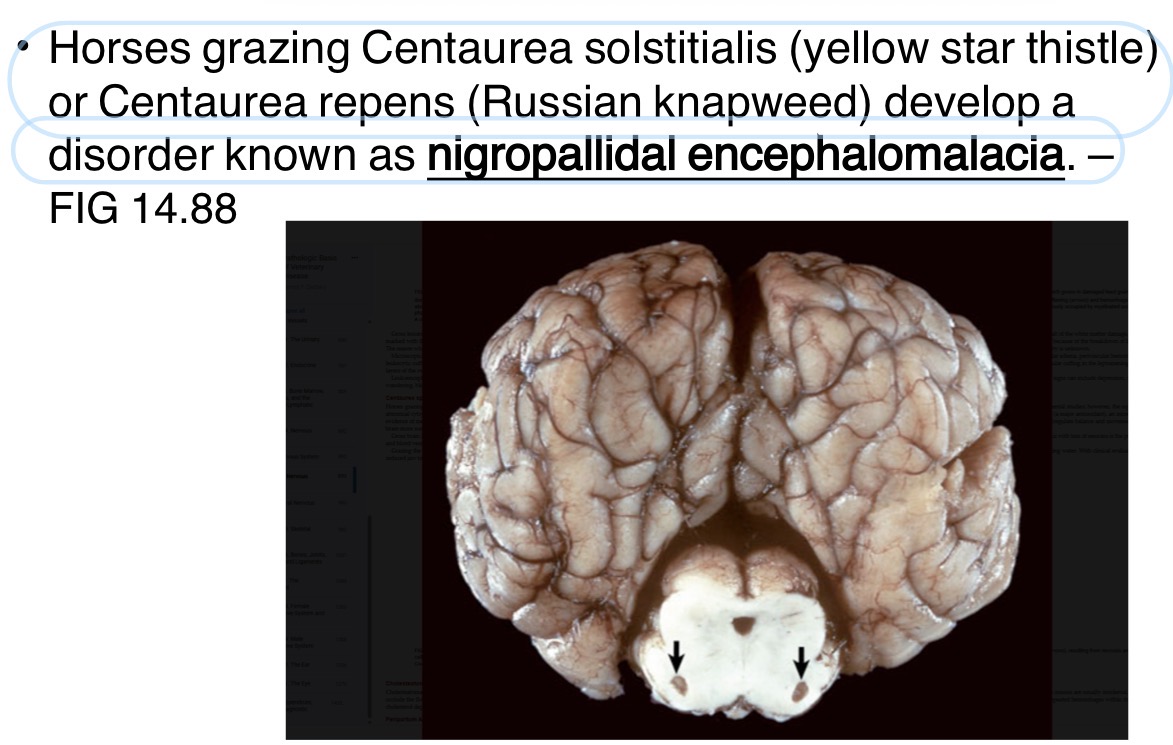
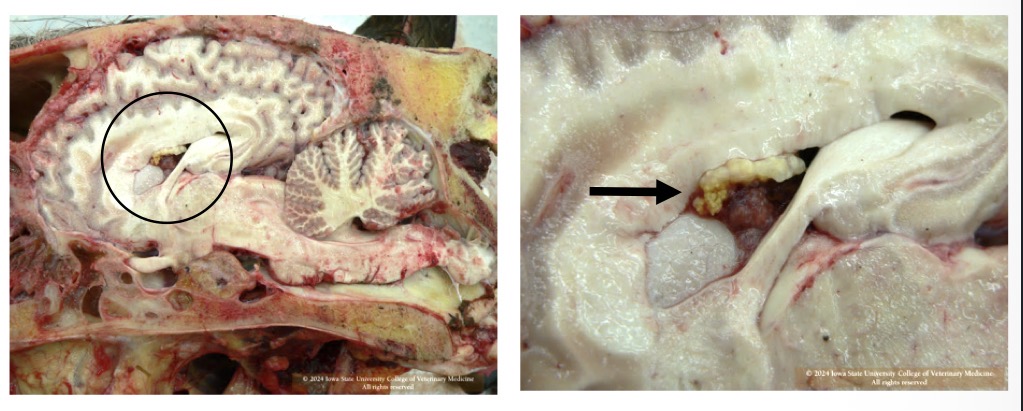
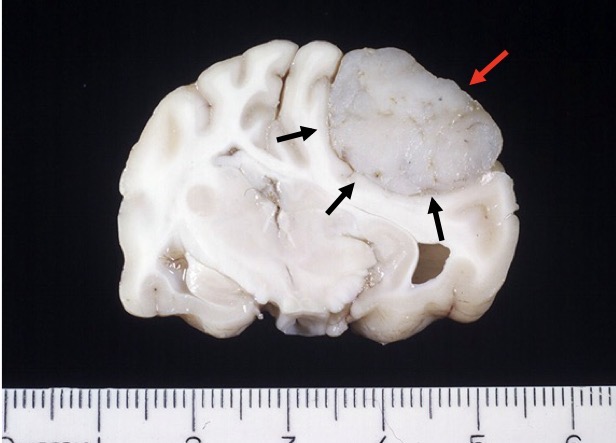
What is the black arrow pointing at in this horse? Is it likely malignant or benign? What is a possible sequelae of this mass?
lateral + 4th ventricles choroid plexus: cholesteatoma
concurrent pituitary adenoma
benign
can possibly cause occlude drainage in ventricular system → cause hydrocephalus
What are the 7 major neurological diseases of the ox?
polioencephalomalacia
listeriosis
TEME
fibrinopurulent meningitis
bovine viral diarrhea
rabies
bovine spongiform encephalopathy
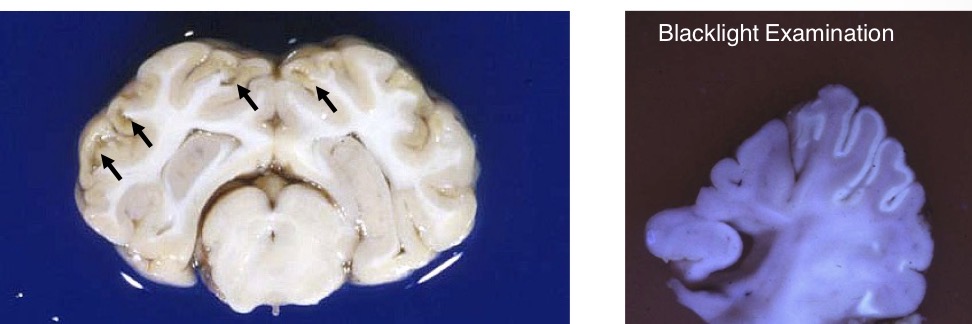
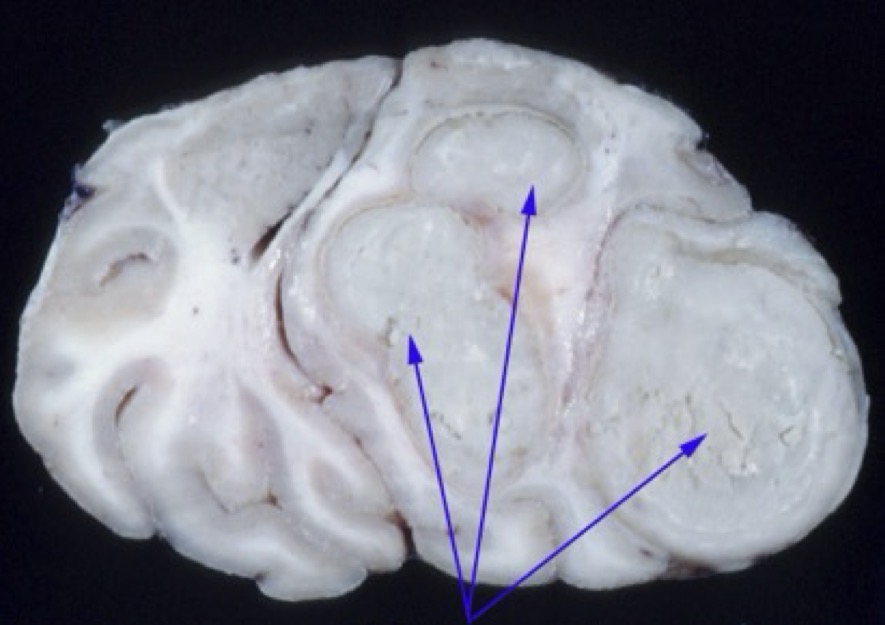
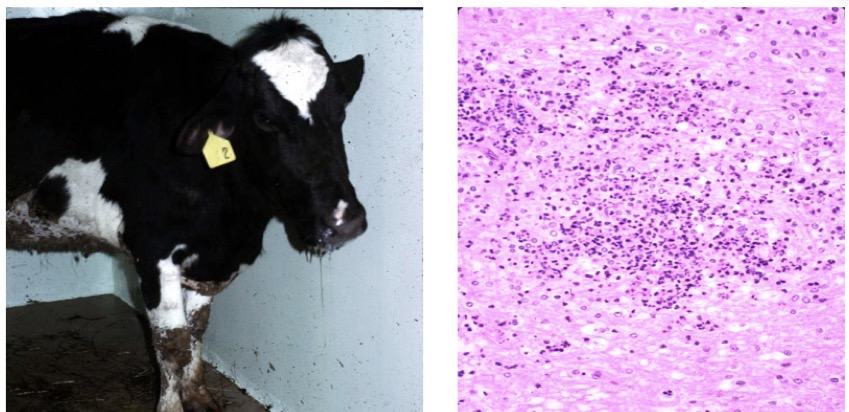
What is this lesion in this cow? What supporting observations do you see? What is it caused by?
polioencephalomalacia
cavitation/liquefactive necrosis in the gray matter
necrotic areas autofluoresce under blacklight
caused by thiamine deficiency OR sulfur toxicosis OR lead toxicosis
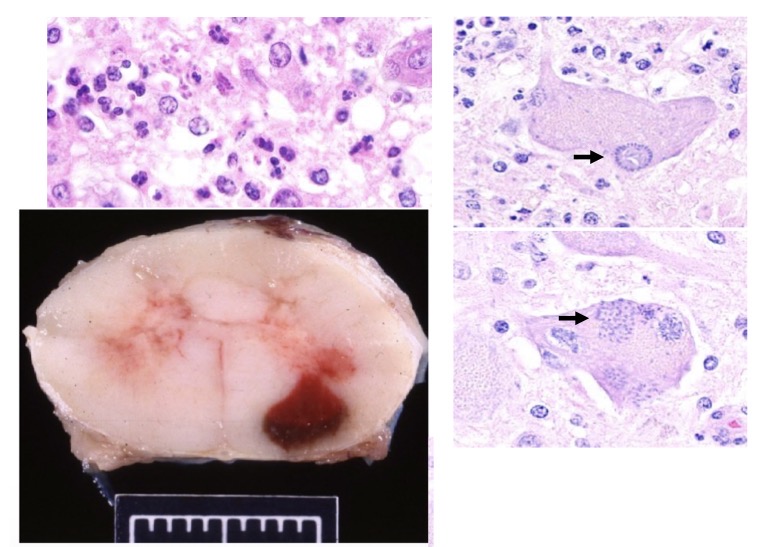
This cow was demonstrating facial paralysis, ear droop, excessive salivation, eyelid droop, and lack of menace response. No gross lesions were observed but this slide from her brainstem did show something. What is disease + lesion? What is the pathogenesis
listeriosis
can see microabscesses on the microscope slide
pathogenesis: Listeria bacteria invade thru wounds in oral mucosa → invade CN 5 → travel via retrograde axonal transport to the medulla oblongata + midbrain → invasion into adjacent cells → acute inflammation → necrosupparative meningoencephalitis w/ vasculitis
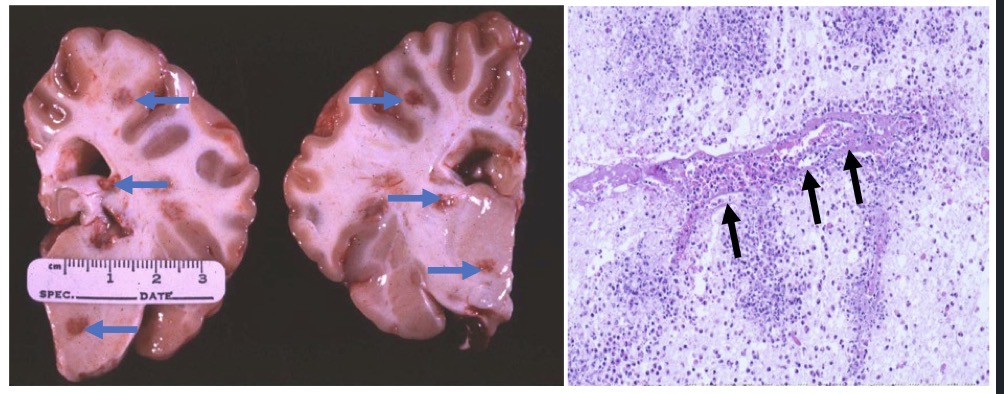
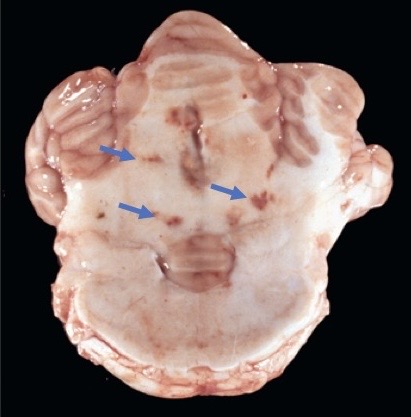
Tissue from a cow. What’s wrong? Pathogenesis?
histophilosis
multifocal areas of necrohemorrhagic + purulent encephalitis
pathogenesis: respiratory tract colonized by Histophilus somni → bacteria replicates locally → gets into bloodstream → septicemia → bacteria invades brain hematogenously and deposits at the gray + white matter interface → endothelial apoptosis/dmg → vasculitis + secondary thrombosis → ischemia → infarction

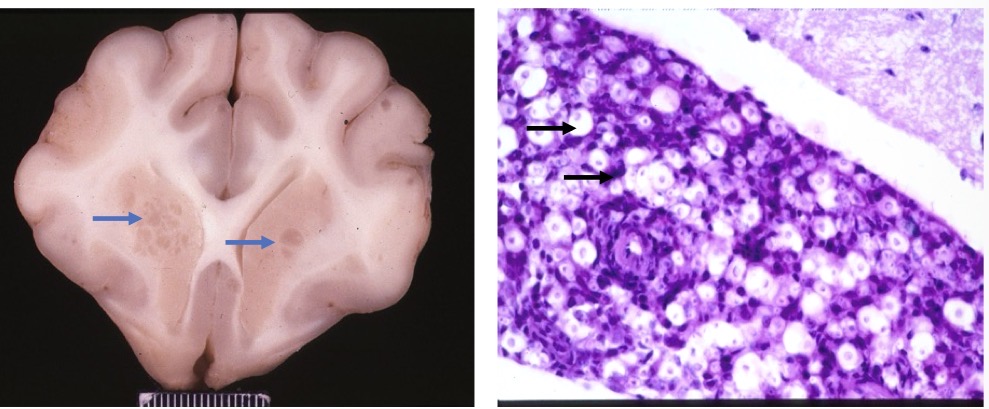
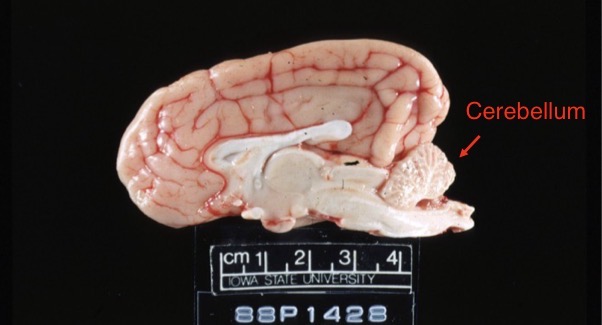
Name the lesion + 2 possible causes in this tissue from a calf.
cerebellar hypoplasia
caused by:
spontaneous congenital defect
teratogenic viral infection (often bovine viral diarrhea)
5 major neurological diseases in small ruminant
fibrinopurulent meningitis
listeriosis
scrapie
polioencephalomalacia
enterotoxemia
Pathogenesis of prion diseases?
animal picks up protease resistant prion protein from environment or ingestion → prion protein replicates in lymphoid tissue → prion invades CNS via leukocyte trafficking or retrograde axonal migration up cranial nerves
What are the 5 major neurological diseases in pigs?
fibrinopurulent meningitis
edema disease
pseudorabies, rabies, PRRSV
neurotropic enteroviruses (teschovirus, astrovirus, sapovirus)
water deprivation/sodium toxicosis
What are the 5 major neurological diseases in the dog?
hydrocephalus
canine distemper (morbillivirus)
rabies
ischemic myelopathy
secondary to IVDD or IV disc cartilage embolism
primary brain neoplasms
Name the lesion in this dog. Supporting observations?
lesion: hydrocephalus
observations:
severely dilated lateral ventricles
atrophy of the cerebrum
Morbilliviruses like CDV and measles can cause ______ ______, which is a condition in which the body forgets how to fight previously encountered pathogens. Morbilliviruses do that by preferentially infecting and depleting ______ _ and _ ______, which are responsible for long-term immune protection.
Morbilliviruses like CDV and measles can cause immune amnesia, which is a condition in which the body forgets how to fight previously encountered pathogens.
Morbilliviruses do that by preferentially infecting and depleting memory T and B lymphocytes which are responsible for long-term immune protection.
pathogenesis of rabies
bite wound from infected animal → rabies virus enters + replicates in muscle → rabies enters spinal cord via peripheral nerves → rabies travels via retrograde axonal transport to brain → rabies spreads to salivary glands + eye
results in rabies viral encephalitis
In rabies virus encephalitis, neurons can have intracytoplasmic viral inclusions called _____ _____
Negri Bodies
Spinal cord injuries in dogs:
_____ = inflammation of the spinal cord
_____ = inflammation of spinal cord gray matter
_____ = inflammation of spinal cord white matter
_____ = necrosis of the spinal cord
usually d/t _____ or _____
_____ ______ = pathology caused by traumatic injury like HBC
disc rupture vs protrusion
myelitis = inflammation of the spinal cord
poliomyelitis = inflammation of spinal cord gray matter
leukomyelitis = inflammation of spinal cord white matter
myelomalacia = necrosis of the spinal cord
usually d/t inflammation or ischemia
traumatic myelopathy = pathology caused by traumatic injury like HBC
type 1 IVDD herniation = disc rupture
associated w/ chondrodystrophic breeds
type 2 IVDD herniation = disc protrusion/bulging disc
associated w/ older dogs of any breed
5 major neurological diseases in the cat
FIP
cryptococcosis
cerebellar hypoplasia
secondary to feline panleukopenia virus infection in utero
meningioma
purulent otitis media/interna → meningitis
Lesion in this cat + cause
serofibrinous ventriculitis + hydrocephalus d/t FIP
Lesion in this cat + cause
meningoencephalitis w/ focal areas of gelatinous clumps d/t cryptoccosis
Lesion in this cat + pathogenesis
cerebellar hypoplasia
pathogenesis: intrauterine infection w/ feline panleukopenia virus → virus infects Purkinje cells → viral-infected cells destroyed → decreased growth + differentiation of Purkinje cells → cerebellar hypoplasia
Name the lesion in this cat. Benign or malignant?
meningioma
technically benign
neoplasms of the brain:
astrocytes → ____
neurons/progenitor cells → ____/____
oligodendrocytes → ____
ependymal cells → ____
meninges → ____
metastatic lymphocytes → ____
metastatic endothelial cells → ____
astrocytes → astrocytoma
neurons/progenitor cells → neuroblastoma/medulloblastoma
oligodendrocytes → oligodendroglioma
ependymal cells → ependymoma
meninges → meningioma
metastatic lymphocytes → lymphosarcoma
metastatic endothelial cells → hemangiosarcoma
What is the fxnal subunit of the liver? What is the portal triad?
hepatic lobule = stacks of hepatocytes w/ portal triads at each corner arranged around central veins
portal triad:
hepatic a
hepatic portal v
bile duct
As blood drains from the portal triad to the central vein via the ____ → oxygen concentration ____ + hepatocytes get ____ metabolically active. This makes the ____ area hepatocytes more sensitive to hypoxic stress.
As blood drains from the portal triad to the central vein via the sinusoids → oxygen concentration decreases + hepatocytes get more metabolically active.
This makes the centrilobular area hepatocytes more sensitive to hypoxic stress.
3 major portals of entry of insults to the liver
direct extension
ex) physical trauma
hematogenous
ex) portal v or systemic
biliary
retrograde biliary transport = agents coming up via common bile duct
3 defense mechanisms the liver has against insults
structural
like omentum
immunologic
like Kupffer cells (resident macrophages)
biochemical
think enzyme inhibitors that prevent premature activation of enzymes
What are some ways the liver responds to injury?
hepatocyte vacuolar degeneration
hepatocyte necrosis + apoptosis
atrophy of hepatocytes or entire liver
inflammation
fibrosis + hepatocellular regeneration + bile ductular proliferation = cirrhosis
neoplasia
3 types of vacuolar change in hepatocytes
hydropic → water accumulates inside vacuoles
glycogen → glycogen accumulates inside vacuoles
lipidosis → lipid accumulates
Most common causes of hydropic degeneration in hepatocytes?
hypoxia
certain toxins
infections
physical injury
nutritional deficiencies
metabolic
Hepatocyte vacuolar glycogen accumulation likes to happen in which species? Hepatic lipidosis likes to happen in which species?
glycogen accumulation → dogs
hepatic lipidosis → cats
3 different pathogenesis of glycogen degeneration? What is the most common one
hyperadrenocorticism (aka steroid hepatopathy) is most common
inc glucocorticoids → inc glycogen synthetase activity → inc hepatic storage of glycogen → severe hepatocellular swelling + degeneration
diabetes mellitus
pancreatic islet cell destruction → dec insulin → hyperglycemia → cells uptake glucose → convert glucose to glycogen → glycogen accumulation → hepatocellular swelling + degernation
glycogen storage disease
Prolonged exogenous prednisone administration → induction of ____ ____ → enhanced hepatic storage of ____ → severe hepatocellular ____ → steroid hepatopathy
Prolonged exogenous prednisone administration → induction of glycogen synthetase → enhanced hepatic storage of glycogen → severe hepatocellular vacuolation → steroid hepatopathy
What is hepatic lipidosis? Pathogenesis? 3 primary causes?
intracytoplasmic accumulation of TGs
pathogenesis: occurs when the rate of intrahepatic TG accumulation exceeds degradation/release as lipoproteins
3 primary causes
excessive delivery of FAs to liver
abnormal production
decreased oxidation of FAs
abnormal utilization
impaired lipoprotein synthesis/release
abnormal utilization/mobilization
3 causes of hepatocellular atrophy
apoptosis
inadequate caloric intake
d/t portosystemic shunts, starvation, etc
hepatic amyloidosis
4 patterns of hepatocellular degeneration/necrosis, what they look like, and common causes
random
multifocal, discrete, pale spots
hematogenous invasion of viruses, bac, protozoa
zonal
centrilobular
enhanced lobular pattern
hypoxic injury + toxic agents activated by cytochrome p450
midzonal
periportal
panlobular
entire hepatic nodules necrosed
massive necrosis = panlobular necrosis affecting most of the liver
commonly caused by blue green algae, torsion, vitamin e deficiency
bridging
hemorrhagic necrosis expanding from 1 centrilobular area to another
5 morphological classifications of inflammatory hepatobiliary disease
acute hepatitis
chronic hepatitis
cholangitis
cholangiohepatitis
interface hepatitis/piecemeal necrosis
The liver is ____ at regenerating lost hepatic mass. If there is loss of normal ECM scaffolding, then you’ll get ____ proliferation which produces _____ _____ w/ _____ bile flow. These act like ____.
The liver is good at regenerating lost hepatic mass. If there is loss of normal ECM scaffolding, then you’ll get nodular proliferation which produces regenerative nodules w/ abnormal bile flow. These act like shunts.
What is liver cirrhosis? What does it cause?
cirrhosis = fibrosis + nodular regeneration + biliary hyperplasia
causes end stage liver + compromised hepatic fxn
What is hepatic failure? What are the 2 types? What are some common consequences?
hepatic failure = liver can’t adequately perform normal fxns d/t insufficient fxnal hepatic mass
2 types
acute = abrupt loss of hepatic fxn (days)
chronic = progressive loss of hepatic fxn (months to years)
common consequences
hepatic encephalopathy
coagulopathy → hemorrhage
hypoalbuminemia which can cause decreased capillary oncotic pressure → causing edema + ascites
portosystemic shunts
icterus
photosensitization
What is cholestasis? What are the 2 types? What does it cause?
cholestasis = obstructed bile flow
2 types
intrahepatic
d/t hepatic canaliculi swelling
extrahepatic
d/t mass or cholelith
causes hyperbilirubinemia → icterus/jaundice
What are the 3 categories of causes for icterus?
pre-hepatic
overproduction of bilirubin
hepatic
impaired uptake, metabolism, or secretion of bilirubin
post-hepatic
cholestasis
What is hepatic passive congestion? What is it caused by? What are the 2 types?
fluid back-up in liver
almost always d/t cardiac dysfxn (especially R-sided heart failure
acute + chronic
What does acute passive congestion look like compared to chronic?
acute
slight hepatomegaly
dark red in color
blood flows freely from cut surface
chronic
significant hepatomegaly w/ very rounded edges
significantly enhanced lobular pattern especially on cut surface
What is a portosystemic shunt? What does it result in? What are the 3 types of congenital portosystemic shunts?
abnormal communication b/t portal vein + systemic circulation where the liver is bypassed
portosystemic shunt → reduced hepatic circulation →
decreased delivery of trophic factors to liver → microhepatica (abnormally small liver)
decreased removal of toxins, bacteria, and ammonia from systemic circulation → hepatic encephalopathy
3 types
intrahepatic
extrahepatic
hepatic microvascular dysplasia/portal vein hypoplasia
Difference b/t congenital extrahepatic shunts + hepatic microvascular dysplasia? What breed is associated w/ each?
extrahepatic = single shunt from main trunk of portal vein to systemic circulation vein, bypassing liver
commonly affects small breed dogs + cats
avg age at presentation: 6-18 months
hepatic microvascular dysplasia/portal vein hypoplasia = abnormal formation of liver microvasculature → altered lobular blood flow
commonly affects small breed dogs
avg age at presentation: 3 yrs
What is portal hypertension? 3 types + common causes?
increased pressure w/i hepatic portal vein
3 types:
prehepatic
portal vein thrombosis, embolism, obstructing mass
hepatic
fibrosis, amyloidosis, granulomatous inflammation
posthepatic
R-sided heart failure
Pathogenesis of hepatic amyloidosis? How does it cause portal hypertension?
chronic inflammatory state → persistently elevated serum-amyloid A → conversion of SAA to AA → too much AA being deposited into various organs → amyloidosis
excessive amyloid deposition in the liver can cause resistance to blood flow into or w/i the sinusoids → portal hypertension
3 common causes of hepatic copper accumulation? Why is copper accumulation bad?
primary defect in copper metabolism
cholestasis → defective biliary excretion of copper
excessive dietary intake of copper
excess copper → increased reactive oxygen species → lipid peroxidation
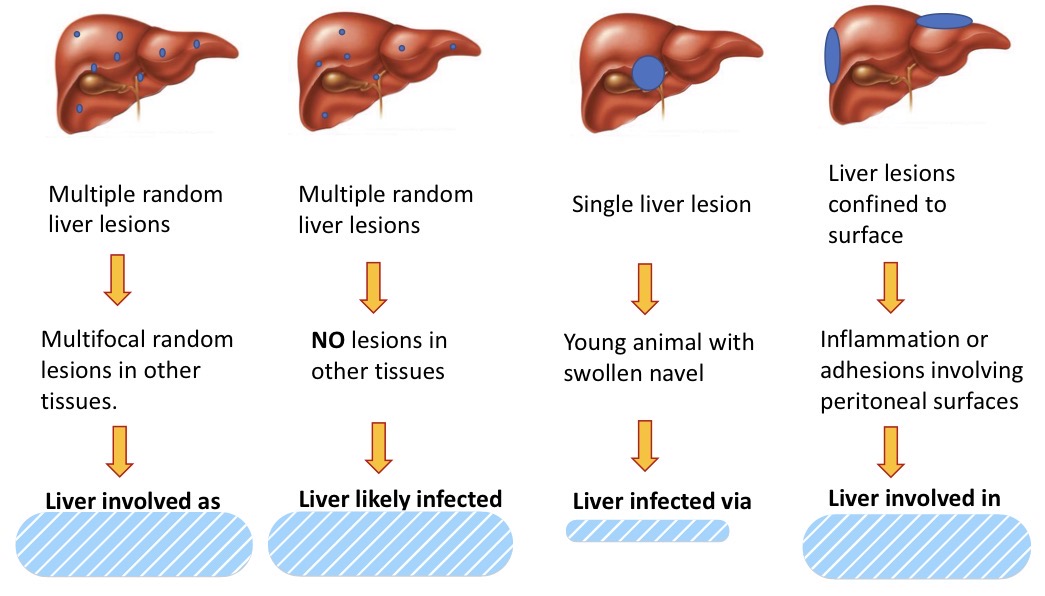
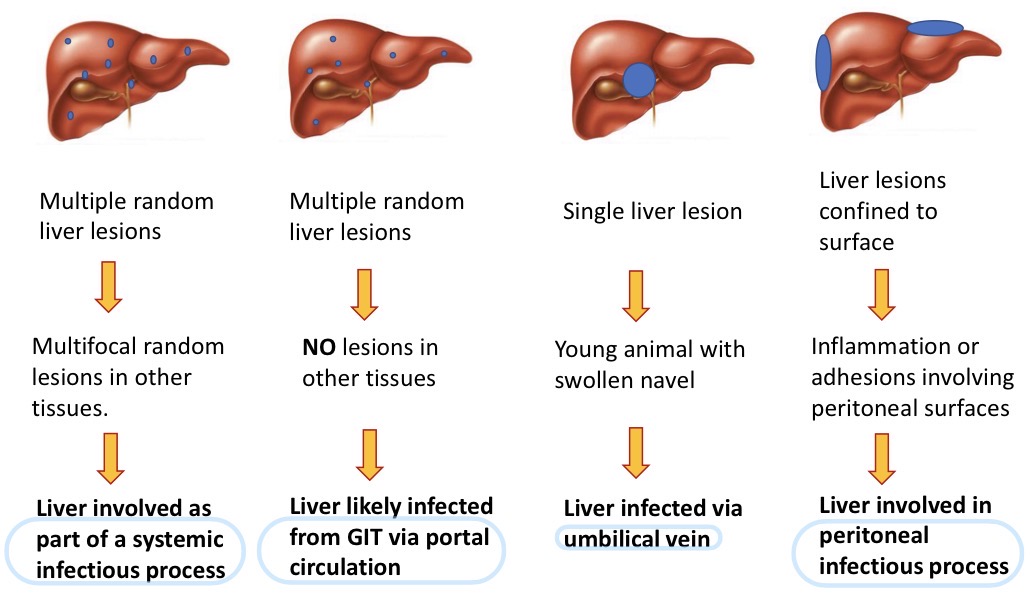
Gross patterns of liver infection + pathogenesis

Dx + pathogenesis in this liver from a feedlot steer
dx: multifocal hepatic necrosis
pathogenesis: Fusobacterium necrophorum present in rumen → ruminal acidosis d/t diet → loss of ruminal mucosal integrity → F. necrophorum enters portal circulation → F. necrophorum infects liver → liver necrosis
What are the 2 major types of hepatotoxins + their expected pattern of injury?
toxins that cause direct hepatocellular injury
expect periportal pattern
toxins transformed by liver to toxic metabolites by cytochrome p450
expect centrilobular pattern