Internal exam (endocrinology)
1/7
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
8 Terms
E-1. Pathogenetic classification of diabetes mellitus
Type 1 DM: autoimmune destruction of pancreatic β-cells → absolute insulin deficiency
Type 2 DM: insulin resistance + impaired β-cell insulin secretion → relative insulin deficiency
Gestational DM: impaired glucose tolerance first diagnosed during pregnancy
Genetic defects:
β-cell function defect → MODY
insulin synthesis defect
Pancreatogenic DM: destruction/removal of pancreas or islets
chronic pancreatitis, pancreatic cancer, pancreatectomy
Endocrinopathies: Cushing syndrome, acromegaly
Drug-induced DM: especially corticosteroids
Infections: e.g. congenital rubella
Rare immune causes: stiff-person syndrome
E-2. Diabetes diagnostic and metabolic compensation criteria
Diagnostic criteria for diabetes:
Classic symptoms: polyuria, polydipsia, polyphagia, weight loss, poor wound healing
*Random plasma glucose ≥11.1 mmol/L with symptoms
*Fasting plasma glucose ≥7.0 mmol/L
*OGTT: 75 g glucose → 2h plasma glucose ≥11.1 mmol/L
*HbA1c ≥6.5%
Good metabolic compensation:
HbA1c <6.5%
Fasting glucose 4.4–6.7 mmol/L
No glucosuria
TAG <1.7 mmol/L
Total cholesterol <5.0 mmol/L
BMI: male <25, female <24
BP <135/85 mmHg
can be divided into good, sufficient, and insufficient
E-3. Type 1 and type 2 DM differences: pathogenesis, clinical picture, therapy strategy
Type 1 DM
Pathogenesis: genetic/environmental factors → autoimmune β-cell destruction → absolute insulin deficiency
Clinical picture: usually <20 years, sudden onset, often thin, ketoacidosis common
Symptoms: polyuria, polydipsia, polyphagia, weight loss, poor wound healing, visual disturbances
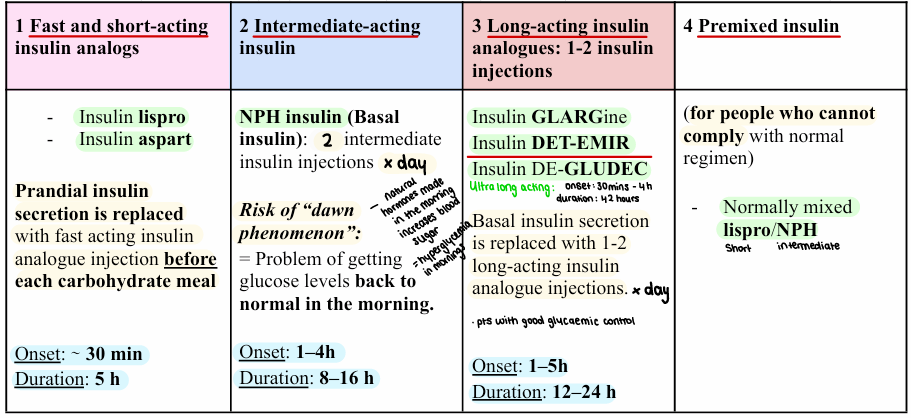
Therapy: lifelong insulin therapy
basal insulin + prandial insulin or insulin pump
regular glucose/HbA1c monitoring
diet, exercise, cardiovascular risk control
Type 2 DM
Pathogenesis: insulin resistance + progressive β-cell dysfunction → relative insulin deficiency
Risk factors: obesity, glucotoxicity, lipotoxicity, genetic/environmental factors
Clinical picture: usually >30 years, gradual onset, often obese, initially asymptomatic, ketoacidosis uncommon
Therapy: lifestyle + oral antidiabetics
metformin first-line, SGLT2 inhibitors etc.
insulin if decompensated
BP/statins/smoking control
E-4. Late complications of diabetes: pathogenesis, types, therapy principles
Microvascular complications:
Pathogenesis: Chronic hyperglycemia → glycation of proteins/lipids → basement membrane thickening + vascular/tissue damage
Diabetic nephropathy: glucose + BP control, ACEi/ARB for proteinuria, lifestyle, RRT if end-stage
Diabetic retinopathy: non-proliferative/proliferative/macular edema; glucose + BP control, laser photocoagulation, anti-VEGF
Diabetic neuropathy: glucose + BP control, pain control e.g. gabapentin
Macrovascular complications = accelerated atherosclerosis:
Pathogenesis: Metabolic risk factors (obesity, dyslipidemia, and arterial hypertension)
Coronary artery disease - MI
Cerebrovascular disease - Stroke
Peripheral artery disease - Peripheral occlusions
Therapy/prevention:
Strict glucose and BP control
Statins
Antiplatelet therapy/aspirin when indicated
Smoking cessation, weight control, physical activity
Treat metabolic risks: weigh control, lipid control, AH control
E-5. Diabetic sensorimotor polyneuropathy: symptoms, diagnosis, therapy principles
Diabetic neuropathy can be peripheral + autonomic.
Peripheral sensorimotor neuropathy
Common DM complication → neuropathic pain + ↑ risk of foot ulceration.
Symptoms: distal symmetric sensory loss with proximal progression, numbness, tingling, burning, sharp/shooting pain in feet or legs, hyperalgesia, ↓ vibration sense, ↓ reflexes, late: ↓ pain + temperature sensation, motor weakness, ataxia/balance problems, foot deformity/ulcers
Autonomic neuropathy
Small-fiber autonomic nerve damage → many organ systems affected.
Symptoms: gastropathy, sweating abnormalities, constipation, cardiopathy, urinary retention, erectile dysfunction, hypoglycemia unawareness
Diagnosis
Symptoms + known DM
Physical exam:
tuning fork vibration test
5-point measurement
reflexes
pain + temperature sensation
EMG / MRI neurography / neurometry if needed
Treatment
First line: optimal glycemic control
Foot care: daily self-checks, proper footwear, treat ulcers
Pain management: gabapentin; also anticonvulsants, antidepressants/SNRIs, opioids if needed
B vitamins: B1, B6, B12
Antioxidants
TENS
Physiotherapy: strength, balance, coordination
E-6. Diabetic macroangiopathy: symptoms and diagnostic principles
Definition: accelerated large-vessel atherosclerosis development in DM → CAD, cerebrovascular disease, PAD.
CAD: chest pain, dyspnea, MI/HF; dx ECG, echo, coronary angiography.
Cerebrovascular: speech disturbance, confusion, facial signs, poor balance, hemiparesis; dx CT/CT Angiography/MRI.
Peripheral Artery Disease: claudication (muscle pain due to lack of O2), cold leg, ulcers/gangrene/necrosis; dx ABI ≤0.9, MR angiography if revascularization planned.
Core idea: macroangiopathy = atherosclerotic complications, main morbidity/mortality risk in diabetes.
E-7. Basic groups of insulin preparations (with examples and pharmacokinetic differences)
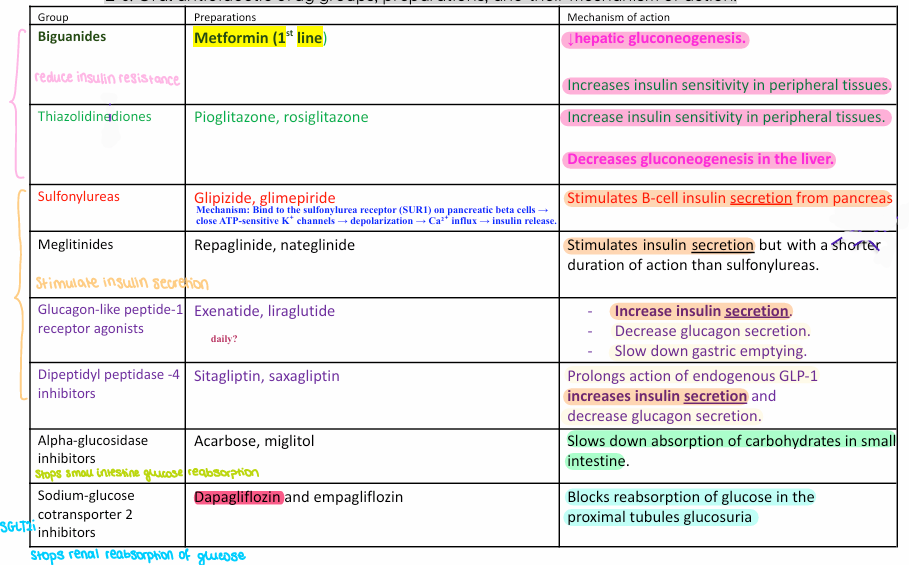
E-8. Oral antidiabetic drug groups, preparations, and their mechanism of action.
Biguanides: metformin → ↓ hepatic gluconeogenesis + ↑ insulin sensitivity; 1st line.
Thiazolidinediones: pioglitazone, rosiglitazone → ↑ peripheral insulin sensitivity, ↓ hepatic gluconeogenesis.
Sulfonylureas: glipizide, glimepiride → ↑ β-cell insulin secretion via SUR1/KATP closure; hypoglycemia risk.
Meglitinides: repaglinide, nateglinide → ↑ insulin secretion, shorter acting than sulfonylureas.
GLP-1 agonists: exenatide, liraglutide/semaglutide → ↑ insulin, ↓ glucagon, slow gastric emptying.
DPP-4 inhibitors: sitagliptin, saxagliptin → prolong GLP-1 → ↑ insulin, ↓ glucagon.
α-glucosidase inhibitors: acarbose, miglitol → ↓ intestinal carbohydrate absorption.
SGLT2 inhibitors: dapagliflozin, empagliflozin → ↓ renal glucose reabsorption → glucosuria.