Neuromuscular Disorder (MG, MS, ALS)
1/84
Earn XP
Description and Tags
syds quizlet
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
85 Terms
What is the underlying pathophysiology of Myasthenia Gravis?
An autoimmune attack on the neuromuscular junction, leading to a decrement in acetylcholine (ACh) binding to receptors on the motor end plate.
What are the risk factors for ocular myasthenia gravis?
prepubertal juvenile MG and men with late-onset MG
What are the risk factors for MuSK MG gravis?
younger women and possibly nonwhite population
What is the hallmark clinical feature of Myasthenia Gravis?
Fatigable weakness symmetrically affecting proximal > distal muscles after multiple reps
What are the ocular symptoms of MG?
ptosis (worse with sustained upgaze, improved with ice), diplopia, blurred vision, and ophthalmoplegia
How does bulbar weakness present in MG?
drooling, facial weakness, dysarthria, and dysphagia
What is 'myasthenic crisis'?
A serious complication of MG involving respiratory muscle weakness that can lead to respiratory failure.
What respiratory assessment can be used to evaluate a patient's ability to speak in sentences?
Forced breath counting; > 20 means significant respiratory involvement unlikely
What physical exam finding is a good surrogate for assessing diaphragmatic weakness?
Neck flexion and extension strength.
What type of gait may be associated with MG?
Difficulty getting out of a chair and head drop with ambulation.
What red flag signs may indicate a condition other than MG?
fatigue without fatigable weakness, symmetric weakness without fatigability (myopathy), upper and lower motor signs (ALS)
What laboratory findings may help to diagnose MG?
Acetylcholine receptor antibodies (AChR +), MuSK (generalized MG who are AChR negative), LRP4 (much less common). Do not suggest severity or are serially monitored
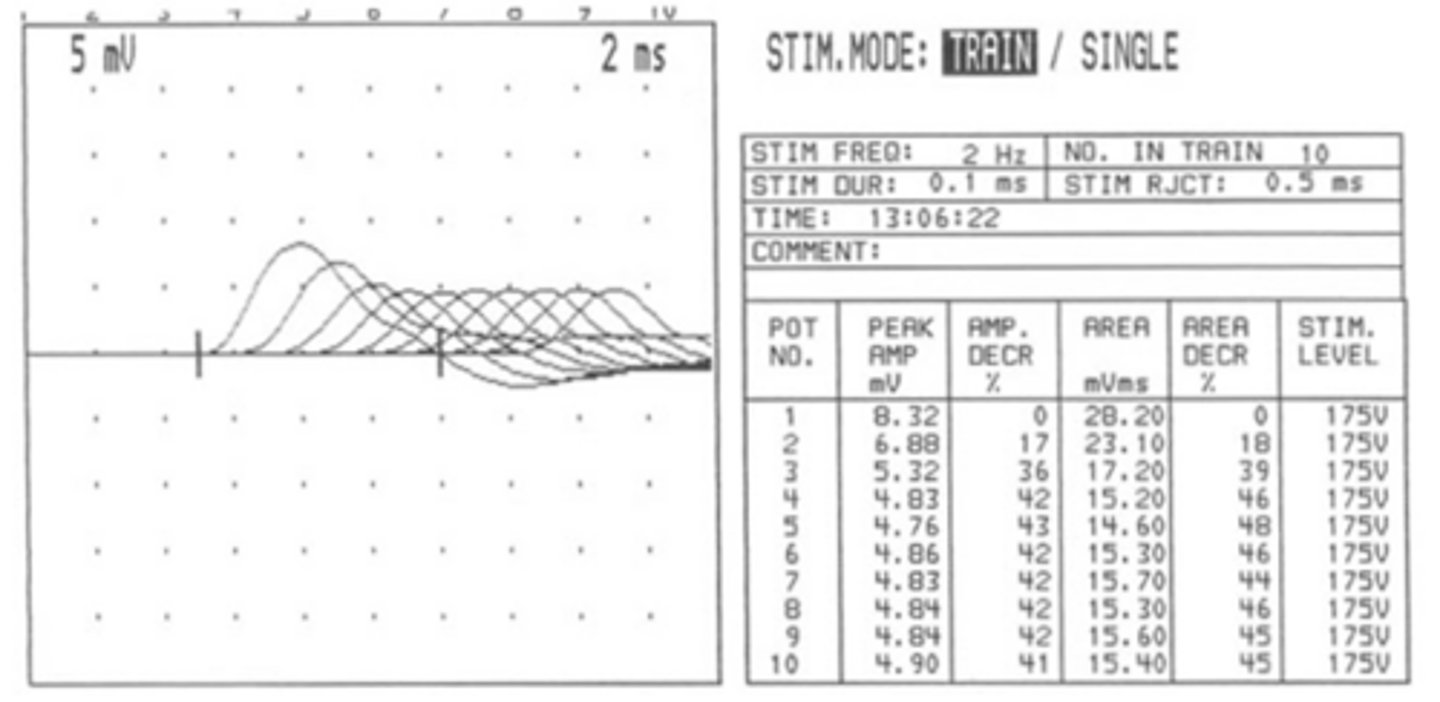
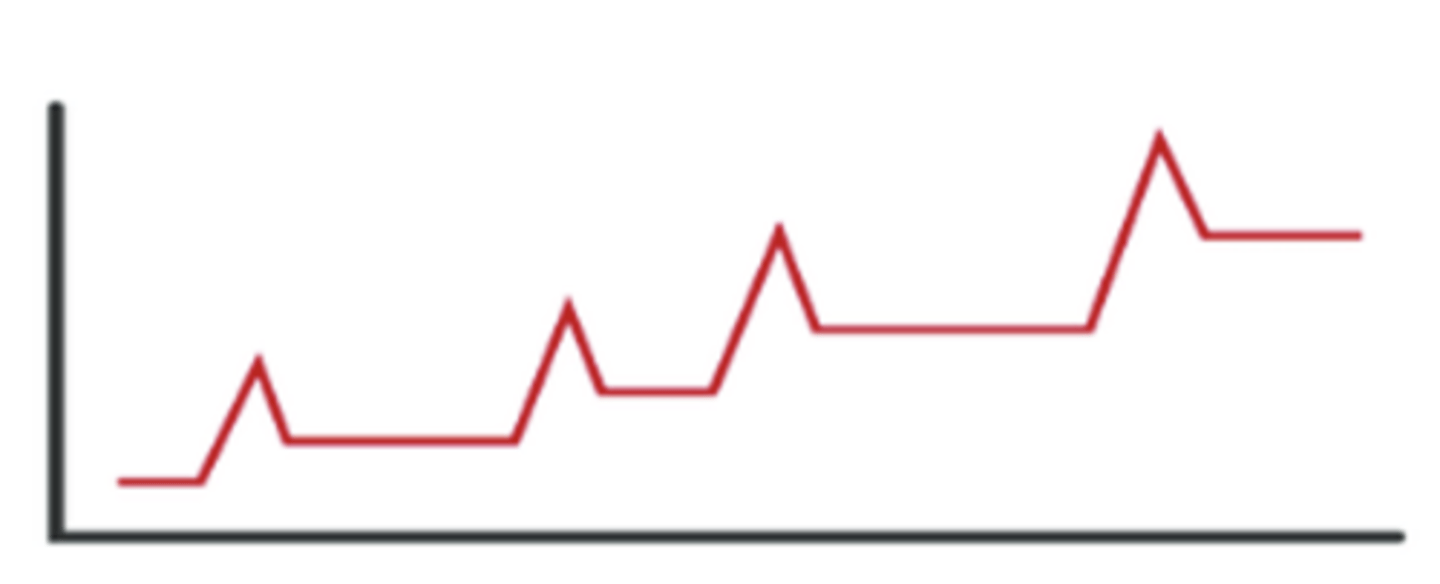
What electrodiagnostic is used for MG?
Electromyography (EMG) with Repetitive nerve stimulation (RNS) showing decrement
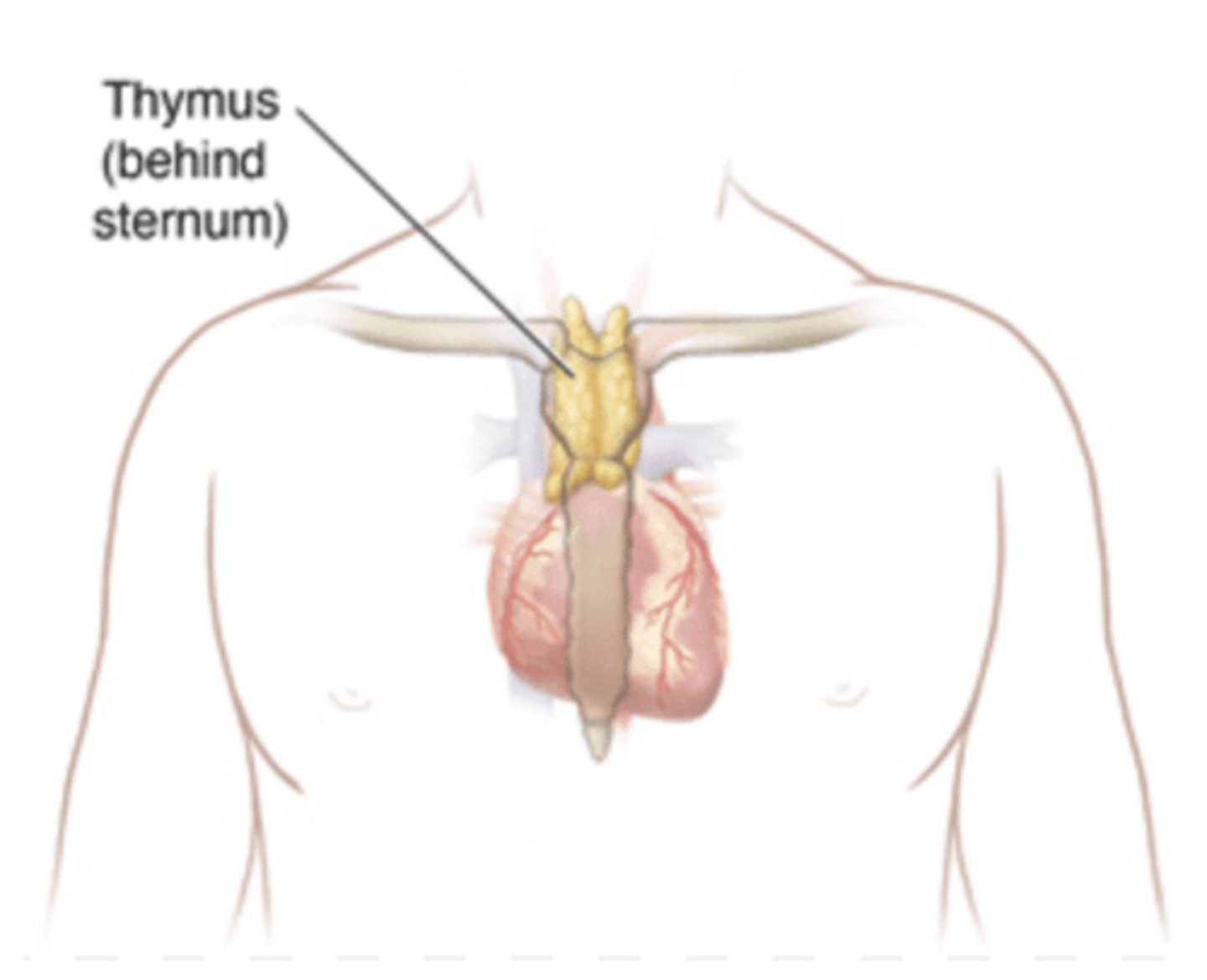
Why is a chest CT scan indicated in the initial evaluation of Myasthenia Gravis?
To evaluate for the presence of thymoma or thymic hyperplasia.
What are the clinical characteristics of early-onset AChR+ Myasthenia Gravis?
Onset before age 50, association with thymic hyperplasia with response to thymectomy, female predominance (3:1), HLA-DR3 and HLA-B8
What are the clinical characteristics of late-onset AChR+ Myasthenia Gravis?
Onset after age 50, rare thymic hyperplasia, male predominance, and less response to thymectomy.
What is the typical clinical presentation of MuSK-associated Myasthenia Gravis?
Predominantly cranial and bulbar muscle involvement, usually in adults, with no thymus changes.
What is the first-line treatment for MuSK-associated Myasthenia Gravis?
Rituximab
What is the recommended treatment for generalized MG?
Cholinesterase inhibitor (Pyridostigmine and neostigmine), steroids, chronic immunotherapy (azathioprine, mycophenolate mofetil, cyclosporine)
What are the primary risks associated with Azathioprine therapy?
Leukopenia and hepatotoxicity.
What medications can unmask or exacerbate MG?
High: Magnesium, Penicillamine, Telithromycin, Botulinum toxin
Moderate: Aminoglycosides, macrolides, and fluoroquinolones
Low: Statins, Beta-blockers, iodine contrast, quinines
What are the common precipitating factors for myasthenic exacerbations?
Infection, surgery, pregnancy/childbirth, tapering immunosuppressive medications, or certain medications.
What is the management for myasthenic exacerbations?
Admit to ICU, frequent respiratory testing (VC and NIF), administer immunomodulating therapy (IVIG or PLEX)
What is the management for myasthenic crisis?
respiratory support with Bipap or intubation
What is the underlying pathophysiology of Lambert-Eaton Myasthenic Syndrome?
Antibodies against P/Q-type voltage-gated calcium channels leading to decreased ACh
What is a strong association with Lambert-Eaton Myasthenic Syndrome?
Small Cell Lung Cancer
What signs and symptoms are present in Lambert-Eaton Myasthenic Syndrome?
muscle weakness (mostly of the legs), oculobulbar symptoms,dry mouth, constipation, orthostatic dysfunction, respiratory/sensory symptoms
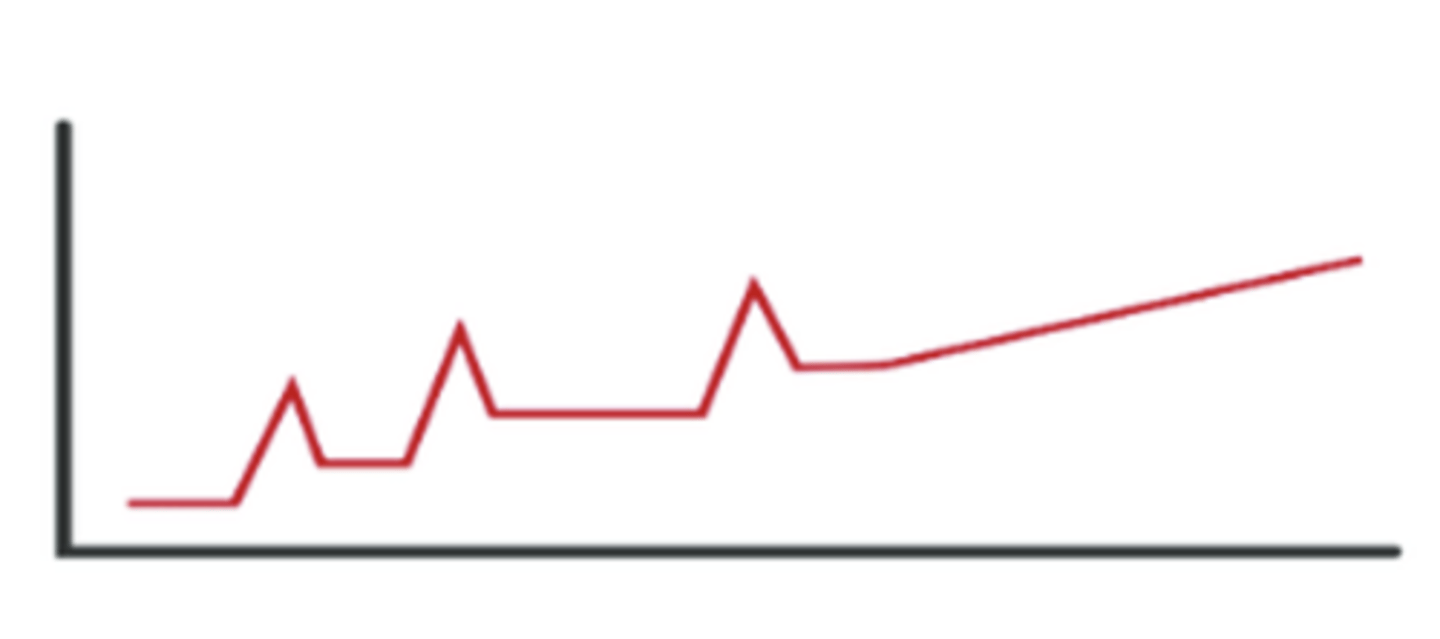
What physical exam findings are present with Lambert-Eaton Myasthenic Syndrome?
Decreased/absent DTRs and post-exercise facilitation
How is Lambert-Eaton Myasthenic Syndrome diagnosed?
antibody test and EMG with repetitive nerve stimulation
What is the definition of Amyotrophic Lateral Sclerosis (ALS)?
A neurodegenerative condition characterized by the degeneration of upper and lower motor neurons in the brain and spinal cord.
What is the typical life expectancy after an ALS diagnosis?
3-4 years on average
Which areas of the central nervous system undergo degeneration in ALS?
The motor cortex, brainstem, and spinal cord.
What symptoms are present in ALS?
weakness, gait instability, dysarthria, dysphagia, atrophy, and cramping
What are the classic physical exam findings of Upper Motor Neuron (UMN) involvement in ALS?
Spasticity, rigidity, hyperreflexia (babinski, hoffman, and clonus)
What are the classic physical exam findings of Lower Motor Neuron (LMN) involvement in ALS?
atrophy, flaccidity, fasciculations, and decreased reflexes

What sensory or cognitive functions typically remain intact in later stages of ALS?
Sensory, bowel, bladder, and visual functions often remain relatively intact.
What clinical criteria according to El Escorial and Awaji is clinically definite ALS?
clinical/EMG evidence of lower and upper motor neuron signs in > 3 regions (likelihood decreases wtih less regions involved)
What is the primary diagnostic tool used to exclude other conditions in suspected ALS?
MRI of the brain and spinal cord, along with EMG.
What is the role of Riluzole in ALS management?
Glutamate blocker delaying ventilator/tracheostomy need. May extend life by 2-3 months
What is the role of Edavarone in ALS management?
Antioxidant delaying functional decline
What ALS medication treats pseudobulbar affect?
dextromethorphan/quinidine-sulfate
What is the role of Tofersen in ALS managment?
An intrathecal injection targeting superoxide dismutase 1 used to decrease signs of disease and may provide some delay in functional decline
What supportive therapy is used in ALS?
PT/OT/SLP. Respiratory therapy (BiPAP, Trach), nutrition (PEG), social work, palliative care
What are the major complications of ALS?
aspiration and respiratory failure
How is Multiple Sclerosis (MS) defined in terms of its pathology?
It is a chronic demyelinating and degenerative CNS condition primarily affecting the white matter, characterized as an immune-mediated disorder
What are the risk factors for developing MS?
Low vitamin D, smoking, obesity, genetics
What immunologic/genetic factors are linked with MS?
CNS immunoglobulin production, Alteration of T lymphocyte activity, IgG and IgM oligoclonal bands seen in the CSF, Viral infections (EBV & VZV), HLA Dr2 and DR4
What type of MS is asymptomatic?
Radiographically isolated syndrome
How is clinically isolated syndrome (CIS) characterized?
Represents first attack of MS with typical symptom + imaging findings (30-70% change of development)
What is the most common form of MS?
Relapsing-remitting MS (RRMS), accounting for 85-90% of cases.
How is Relapsing-remitting MS defined?
Unpredictable attacks which may or may not leave permanent deficits followed by periods of remission
What is secondary progressive MS?
Initial relapsing-remitting MS followed by gradual worsening with or without occasional relapses, minor remissions, and plateaus 10-20 years after disease onset
What is primary progressive MS?
Steady increase in disability from onset without attacks
How do MS relapses (attacks) present?
Neuro symptoms progressive over 24-48 hours lasting for days to weeks. Gradually improve but may not return to baseline
What are the classic symptoms of unilateral optic neuritis in MS?
Pain with eye movements, monocular vision loss with central blurring or scotoma, and vision color changes.

Describe the ocular findings in intranuclear ophthalmoplegia (INO).
Abnormal horizontal ocular movements with lost or delayed adduction and horizontal nystagmus of the abducting eye.
What other physical exam findings are typical in a MS attacks?
dysarthria, dysphagia, sixth nerve palsy, facial numbness, trigeminal nerve pain, vertigo
What CNS symptoms are typical in MS attacks?
weakness, numbness, bowel.bladder dysfunction, band-like sensation (MS hug), hemibody sensory changes

What is the Uhthoff phenomenon?
A worsening of MS symptoms triggered by heat sensitivity.
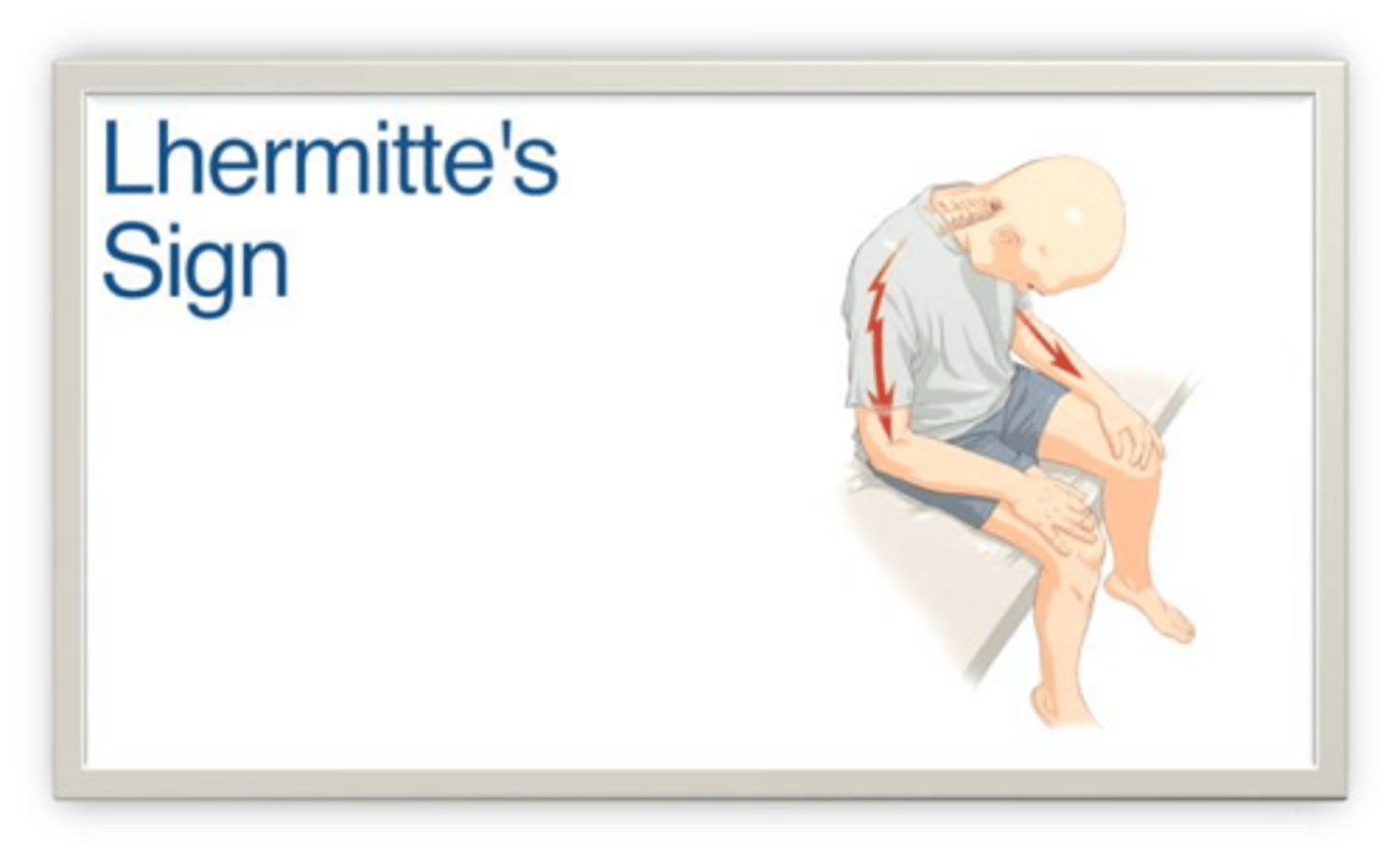
What is the Lhermitte sign?
A sudden electric shock sensation down the spine triggered by flexing the neck.
What reflexes may be present in MS?
Hoffman, Babinski, and Clonus
What gait may be associated with MS?
may be ataxic, wide-based, +/- leg circumduction
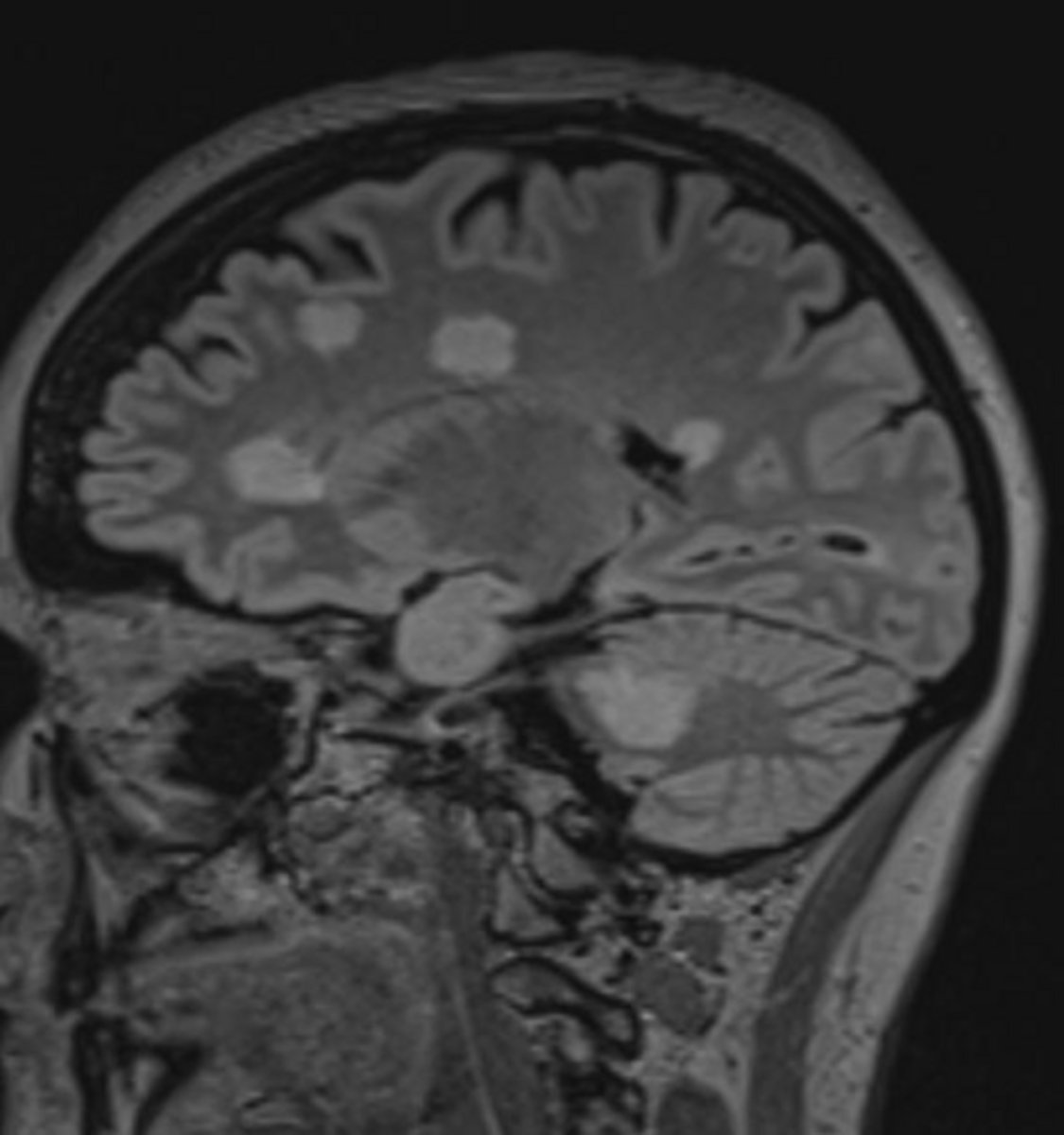
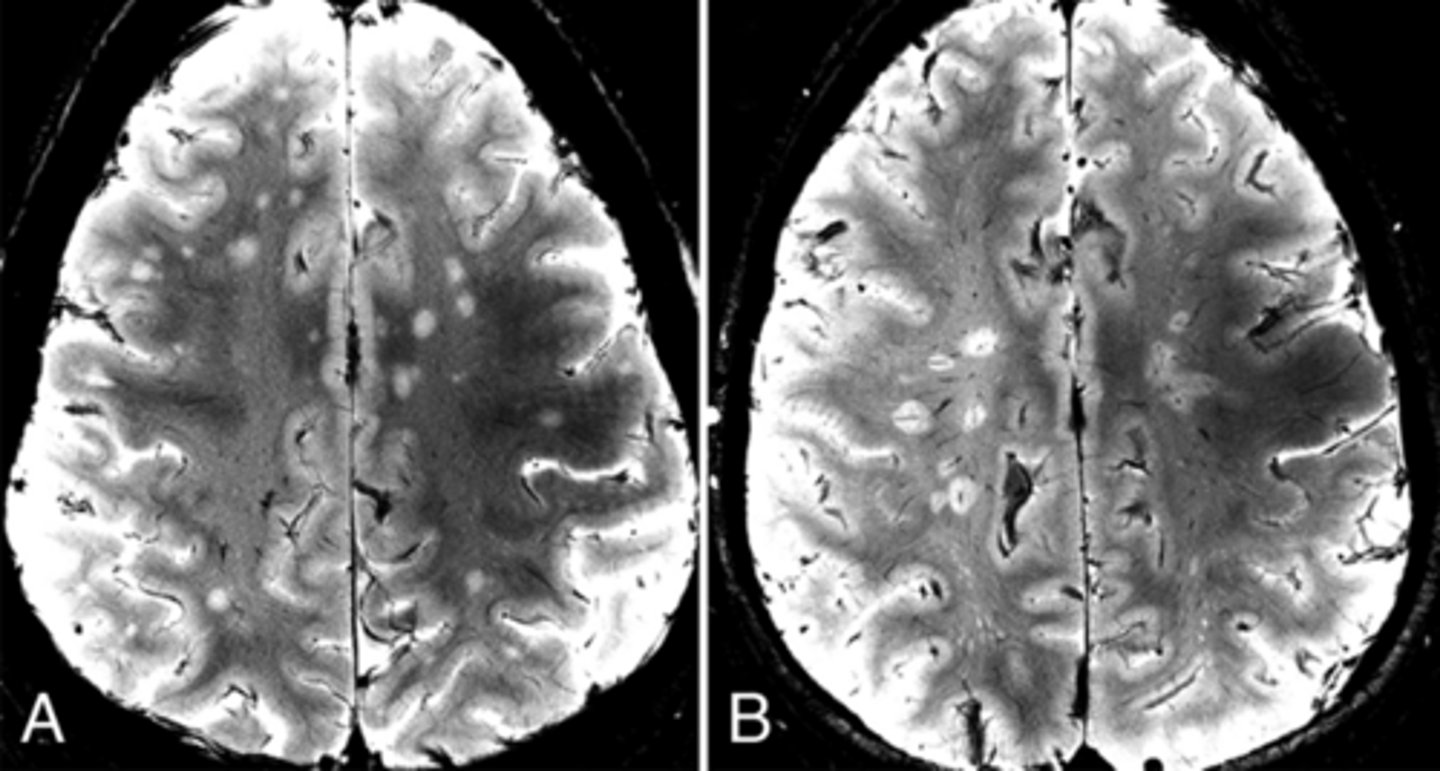
What are the typical MRI characteristics of MS lesions?
Focal hyperintensity on T2-weighted imaging, round to ovoid shape, 3mm to <1-2 cm in size, and generally asymmetric distribution.
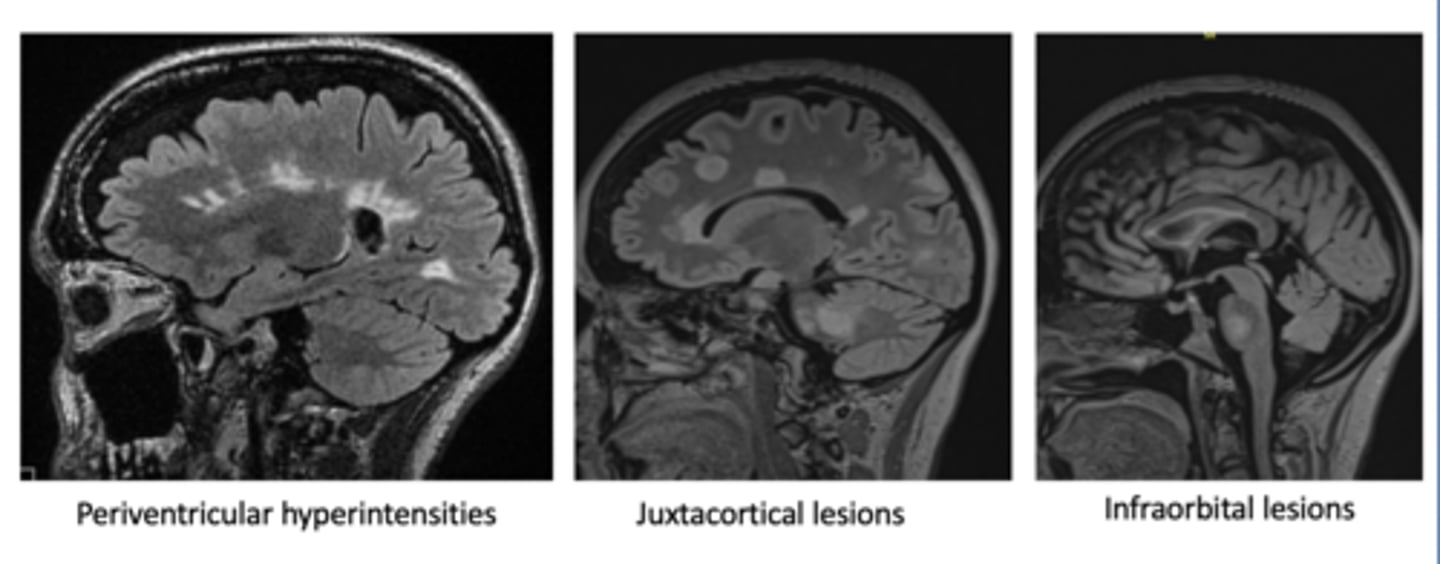
What types of lesions may be seen on imaging in MS?
Periventricular (Dawson's Fingers), Juxtacortical, and Infraorbital lesions
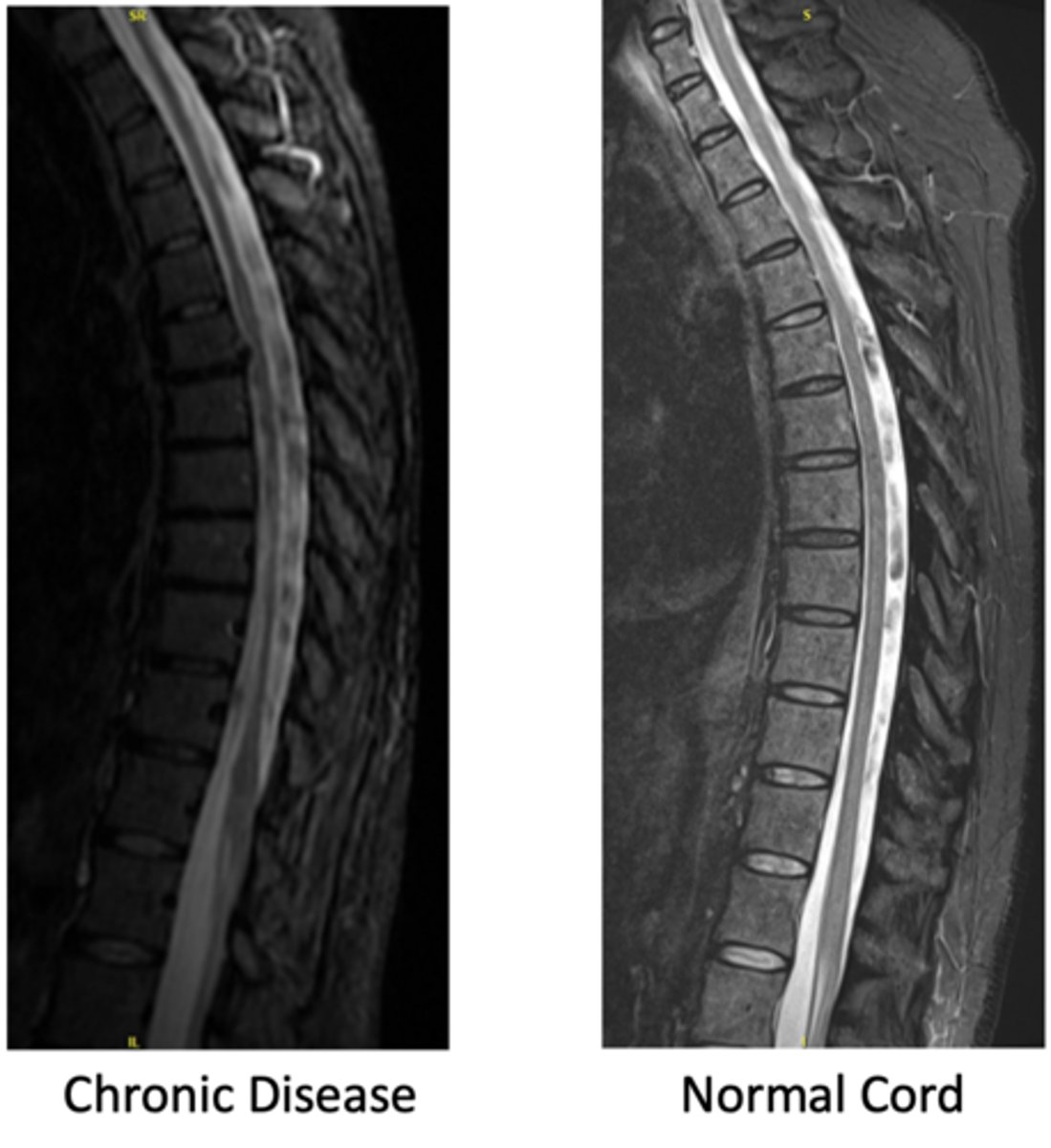
How does chronic MS appear in the spine?
decreased CSF with possible stenosis
What is the 'Central Vein Sign' in MS imaging?
A diagnostic imaging marker where a central vein is visible within a white matter lesion, helping to distinguish MS from other conditions.
What CSF findings are typically associated with MS?
oligoclonal bands or kappa free light chains, WBC < 30, proteins
What clinical presentation of MS does not require additional data for diagnosis via McDonald criteria?
>2 attacks and evidence of >2 lesions or 1 lesion with history of a lesion in a different location
Which serum autoantibodies should be tested to rule out MS mimics?
Aquaporin-4 (AQP4) IgG and myelin oligodendrocyte glycoprotein (MOG-IgG) autoantibodies.
What is the standard acute treatment for an MS relapse?
High-dose IV steroids (1000 mg IV) for 3-5 days and Plasma exchange therapy (PLEX; refractory with steroids)
What medications are used to manage pain in MS?
gabapentin, pregabalin, amitriptyline, AEDs (carbamazepine, lamotrigine, topiramate)
What medications are commonly used to treat MS-related fatigue?
Modafinil and methylphenidate.
What is a 'pseudo-exacerbation' in MS?
The recurrence of previous symptoms triggered by additional bodily stressors (e.g., infection, heat).
What is the primary cause of Neuromyelitis Optica (NMO)?
Antibodies to Aquaporin-4 water channels in the central nervous system.
What symptoms are associated with NMO?
bilateral optic neuritis, complete spinal cord syndrome
What is 'area postrema syndrome' in NMO?
intractable hiccups, nausea, and vomiting.
What is the management for acute attacks of NMO?
managed with IV Methylpredinisone (IVMP) and PLEX
What are the long-term maintenance therapies for NMO?
Eculizumab, inebilizumab, satralizumab, and rituximab.
What is the primary cause of MOG Antibody Disease (MOGAD)?
Antibodies to myelin oligodendrocyte glycoprotein (MOG) in myelin sheaths.
What is the clinical presentation of MOGAD?
Initially myelitis followed by optic neuritis
What is the management for acute attacks of MOGAD?
IVMP, IVIG, and PLEX
What are common long-term maintenance treatments for MOGAD?
Rituximab, mycophenolate mofetil, and azathioprine.
What is Acute Disseminated Encephalomyelitis (ADEM)?
A predominantly childhood demyelinating condition that typically occurs post-infection (measles, rubella, mumps, or vaccination)
What are common symptoms of ADEM?
Fever, vomiting, headache, gait changes, seizures, nystagmus, diplopia, and cranial nerve palsies.
How is ADEM managed?
high-dose steroids