Cystic Fibrosis Study Terms & Definitions | Medical Lecture 50
1/41
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
42 Terms
Cystic Fibrosis
An inherited chronic, progressive multisystem genetic disorder:
• Chronic, progressive, obstructive lung disease
• Pancreatic insufficiency
• CF related Diabetes
• Malabsorption
• Liver disease and cirrhosis
CFTR
gene associated with Cystic Fibrosis
CFTR
-encodes for cystic fibrosis transmembrane
conductance regulator protein
CFTR
• Expressed largely in epithelial cells of airways, GI tract, sweat glands, and GU system
• Causes chloride and sodium transport dysfunction
F508del
-most common mutation assoc with cystic fibrosis
-Absence of phenylalanine @ 508 position
Maintain appropriate composition of secretions
goal of Na+/Cl- channels
Sweat Glands
-draws Cl- into cells from lumen of sweat duct, ENaC brings Na+
Airway (and Gut) Epithelium
-pumps chloride from cells to airways in lungs, ENaC still brings sodium in
-Thick secretions lead to mucus plugging leading to airway inflammation and bacterial colonization
What is the main pathogenesis of CF effects on lung
-Thick secretions cause impaired flow of bile and pancreatic secretions
-Cholestasis and Malabsorption of fat and protein, as well as liver and pancreatic disease
What is the main pathogenesis of CF effects on GI
Cystic Fibrosis
• Recurrent sinopulmonary
infections
• Steatorrhea
• Failure to thrive
Chronic Bronchiectasis
• Bronchioles become widened thinned and scarred
• Typically caused by conditions that prevent mucous clearance from the airways
• Leads to decreased airway clearance and increased infections leading to more damage and decreased airway function
Bronchiectasis
irreversible, abnormal dilation and anatomic distortion of the bronchial tree
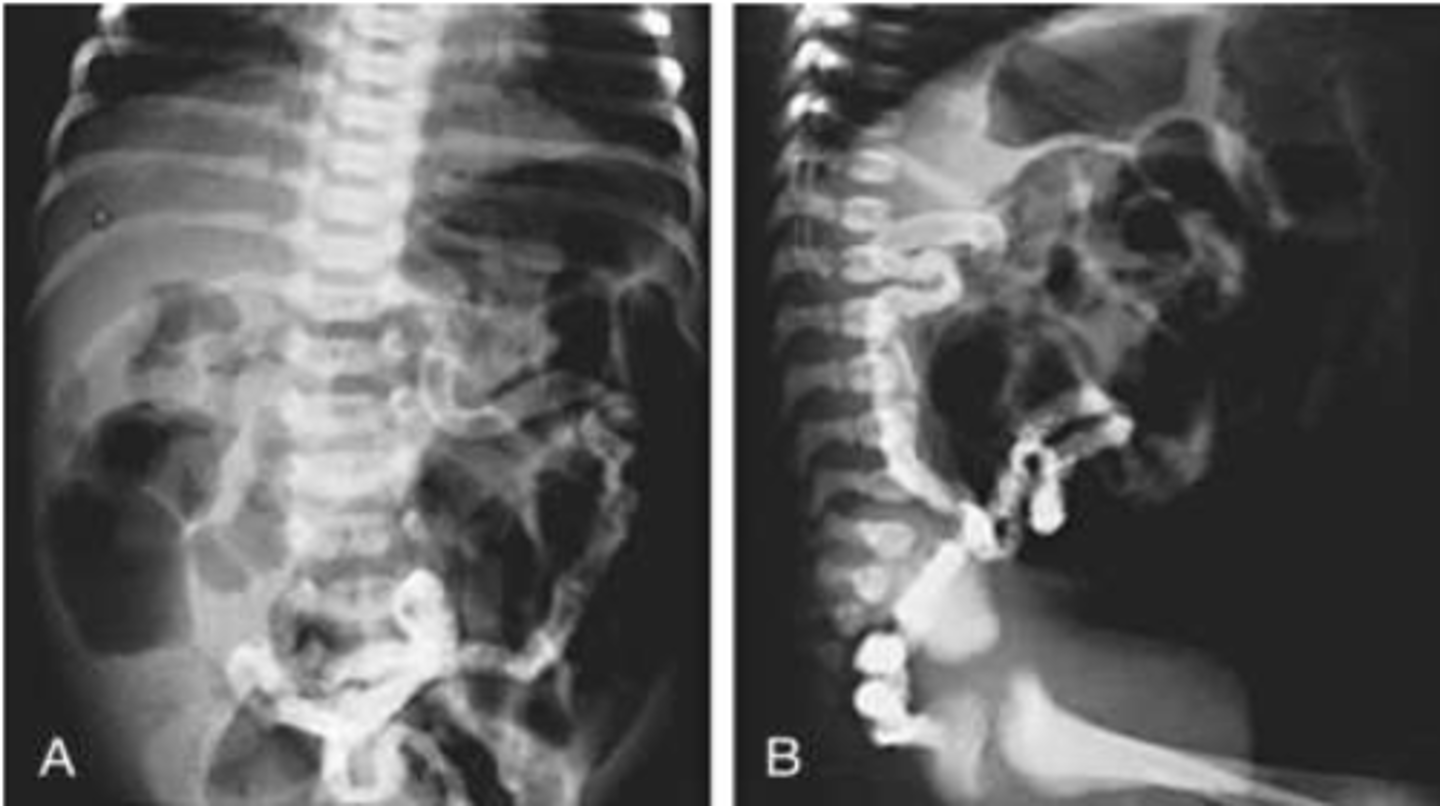
Meconium Ileus
• Obstruction of bowel by meconium in infants
• Abdominal distension, emesis, and failure to pass meconium presents in first 24-48 hours of life
• Is complicated by perforation and peritonitis 50% of the time
Meconium Ileus
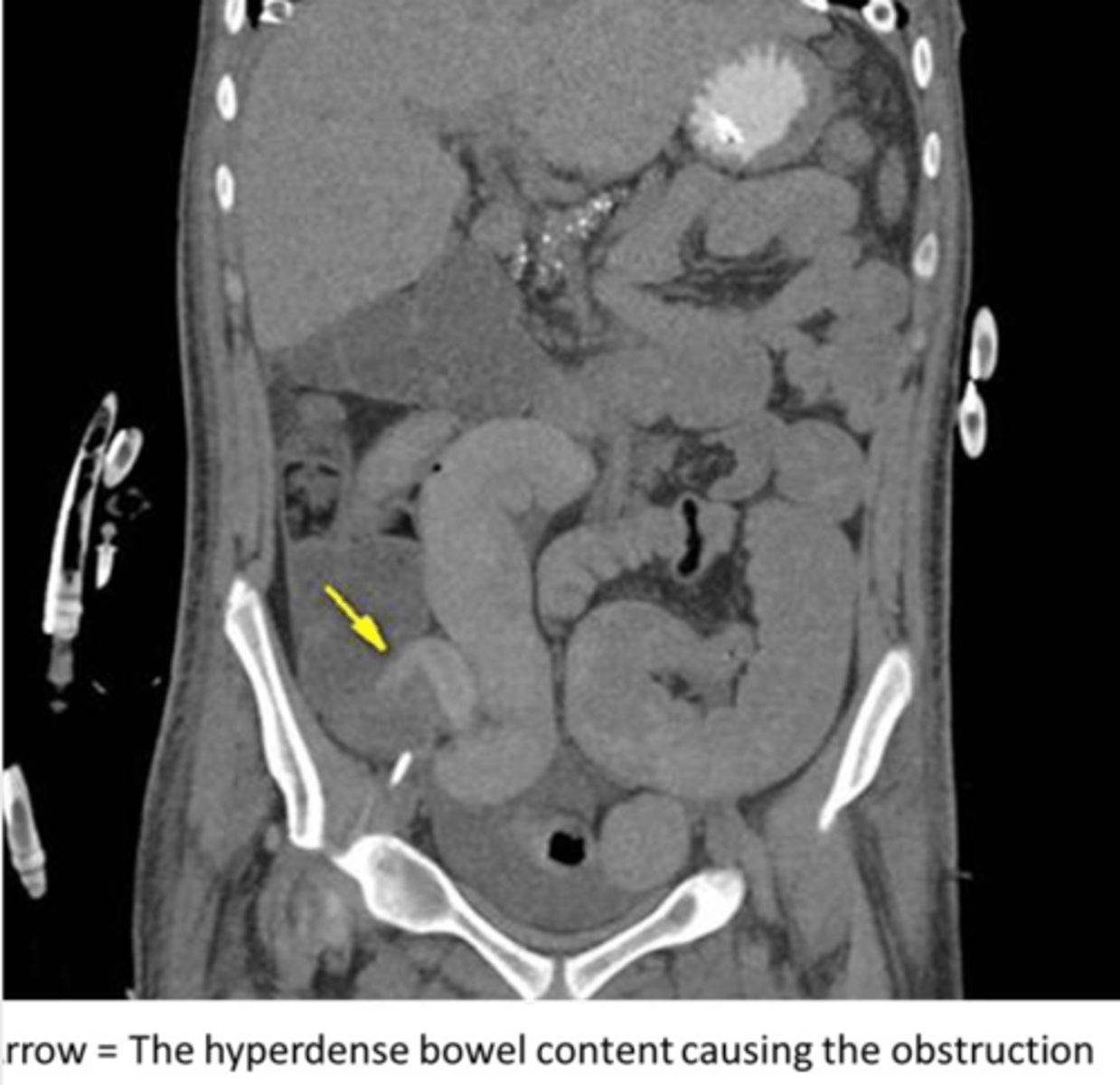
Distal Intestinal Obstructive Syndrome (DIOS)
-blockage of the intestine by thickened stool
-presents like an obstruction
-abdominal pain, distension, and vomiting
-treat with rehydration, osmotic laxatives, and enemas
Distal Intestinal Obstructive Syndrome (DIOS)
-recurrent sinopulmonary infections, steatorrhea, failure to thrive
-salt depletion syndrome
-prolonged jaundice
-malabsorption (acrodermatitis and enteropathica)
-hemorrhagic disease of the newborn (vitamin K deficiency)
Distal Intestinal Obstructive Syndrome (DIOS)
Distal Intestinal Obstructive Syndrome (DIOS)
Common presentations in older children and adults:
• Respiratory– Recurrent sinus and lung infections, uncontrolled asthma, Nasal polyps
• Gastrointestinal– Poor weight gain and growth, steatorrhea, rectal prolapse, constipation, pancreatitis, etc
Distal Intestinal Obstructive Syndrome (DIOS)
One of These Three
• > 1 Phenotypic feature of CF
• Chronic sinopulmonary disease
• Characteristic GI & nutritional abnormalities
• Salt loss syndromes
• Male urogenital abnormalities
• CF in sibling
• Positive newborn screen
Plus One of These Three
• Elevated sweat chloride concentration
• On 2 or more occasions
• Identification of mutation in both CFTR genes
• In vivo demonstration of characteristic abnormalities in ion transport across the nasal epithelium
• Newborn screen
• DNA or Genetic testing
• Sweat test
• Nasal Potential Difference Testing
Diagnostic Studies for CF
Immunoreactive Trypsinogen (IRT)
newborn screening for CF
Sweat Chloride Test
• Gold Standard test for CF
• Measures chloride in sweat (↑ in CF)
Pilocarpine Iontophoresis (sweat test)
• Pilocarpine is applied to the skin along with two electrodes to drive med into the skin and cause sweating
• A sweat collecting dressing is then placed
• 50 mg of sweat must be collected in 45 minutes for test to be valid
60
a positive sweat chloride test is > _________ mmol/L
2
diagnosis of CF requires _____ abnormal sweat tests
Genetic Testing
• Helpful if indeterminate sweat test
• Identifies about 95% of patients with CF
Nasal Potential Difference Testing
• Only done if sweat test and DNA testing are inconclusive
• Electrode is placed in nasal cavity
• Voltage measurements are taken at basal state
• Measurements are repeated after the nasal mucosa is bathed in different solutions that predictably change the ion flow across the membrane
S. aureus
the most prevalent infectious CF bacterium in childhood
P. aeruginosa
the most prevalent bacteria for CF in adults
Pulmonary Clearance
-a treatment for CF
-leads to decreased secretions and bacteria which decreases freq of infection
-improves air exchange, reduced airway resistance and corrected V/Q mismatch
• Postural drainage
• Active cycle breathing
• Chest Physiotherapy/Percussion
• High frequency chest wall oscillation
• Positive expiratory pressure
• Exercise
-modalities used for pulmonary clearance in CF pts
-Pulmonary Clearance
-Anti-inflammatories
treatment for CF
-High dose ibuprofen
-PO Azithromycin (3x a week)
antiinflammatories for CF
Allergic Bronchopulmonary Aspergillosis
• An exaggerated immune response to Aspergillosis
• More common in patients with CF or Asthma
• Causes an inflammatory response of the airways that leads to bronchiectasis and scarring
-elevated IgE and eosinophils
Corticosteroids and Antifungals (Itraconazole)
treatment for Allergic Bronchopulmonary Aspergillosis
• Routine respiratory cultures
• Nebulized antibiotics
treatment for Chronic Pulmonary Infection
Pulmonary Exacerbation
Progressive airway obstruction and increased daily respiratory symptoms (cough, sputum production) and decreased lung function along with fatigue, decreased appetite, and weight loss
• Bronchodilators
• Increased frequency of Airway clearance treatments
• Sputum cultures are obtained to check for resistance
• Antibiotics (Typically IV)
Treatment for Pulmonary Exacerbation
-Replacement of pancreatic enzymes (lifelong)
-Replacement of ADEK
-Insulin
-Eat carbs, avoid simple sugars
treatment for pancreatic insufficiency in pts with CF
CFTR Modulator Ivacaftor
• Treats patients with G551D mutation
• Activates defective CFTR at the cell surface!
• Restores the functioning of mutant CF protein!!!
• Shown to decrease pulmonary exacerbations and improve lung function, weight, sweat chloride levels and quality of life
• Inactivated Influenza vaccine yearly
• Pneumococcal vaccine
• COVID-19
• Palivizumab-
vaccines that help prevent CF