Safe injecting and anaphlaxis
1/53
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
54 Terms
What are injections?
Injections are sterile solutions or occasionally emulsions. They are prepared by dissolving, emulsifying or suspending the active ingredient in water for injection or a suitable diluent liquid
Key principles of safe injection
Injections are invasive and strict aseptic technique is required during preparation and administration. Good injection technique makes the experience less painful and invasive for the patient
Before you start preparing a prescribed injectable drug, what should be checked?
Ask the patient their name and DOB
Do they have any allergies
Check against prescription chart
Check details about the indication of the drug
Check dose
Check route
check expiry date
Check contraindications with the BNF
Make sure the date and time of administration is correct
What are the 5 R’s?
R-Right patient
R-Right drug
R-Right dose
R-Right time
R-Right route
What must be worn by the person administering the injection?
staff should wear gloves for the preperation of drugs and during the injection procedure to avoid cross contamination by bacteria
gloves will protect adminstrator from absorption of medication via the skin but will not protect against sharps injury.
Reconstitution of Powdered Medicine & Sharp Safety – Key Steps
Use a clean treatment room and confirm prescription and drug information. Read labels carefully and gather equipment (sharps bin, ampoules, diluent, syringe, needles, gloves, tray). Remove caps; open glass ampoules safely. Clean diluent top. Draw up required diluent with a green needle, inject into vial, and agitate to mix. Draw up the reconstituted drug while keeping the needle tip submerged to avoid air. Dispose of the drawing‑up needle and attach a fresh needle for SC or IM injection. After administration, place the entire used needle‑and‑syringe unit directly into the sharps bin without separating.
When is the only time you can remove a needle from a syringe?
When they are UNUSED. When a drug has been administered, the needle and syringe are placed straight into the sharps box unseperated
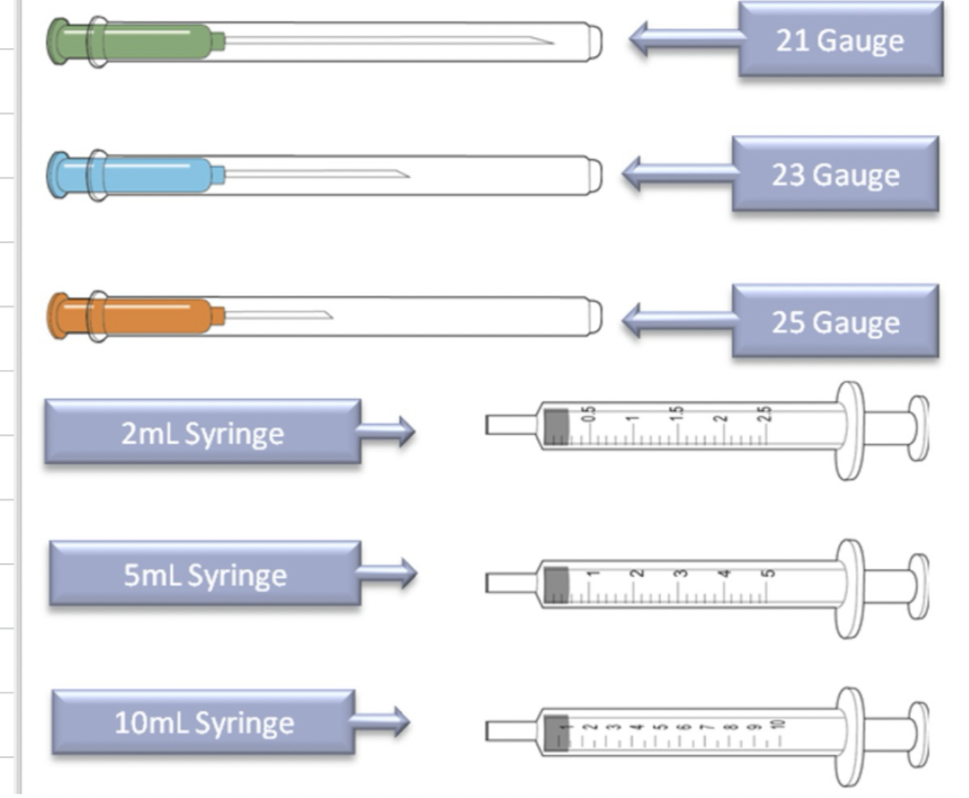
What colour needle do we use for SC injection?
Orange/25 guage - short needle unlikely to penetrate muscle layer
How much volume is injected via SC route? What syringe would we use?
1-2ml is injected via SC route, use 5ml syringe.
What colour needle is used for intramuscular injection?
Green (21 guage) or blue (23 guage)
Longer to penetrate the mucle but still allow a quarter of the needle to remain external to the skin.
When is it preferrable to use a blue needle for intramusclar injection?
for children (23 guage) so smaller
Before administrating injection, how do we prep the skin?
if skin disinfecting is practiced then the skin should be cleansed with alcohol swab for 30 seconds and allowed to dry for 30 seconds.
What drugs are administered via subcutaneous injection?
insulins
anticoagulants
typically slow sustained absorption medications
relatively pain-free and sites are often suitable for frequent injections
What sites are recommended for S/C injection?
Upper arms are a favourable choice - they do not cause discomfort to the patient. Avoid areas of bruising, tenderness, hardness, infection or inflammation
Why must care be taken in particular when administering insulin?
care must be taken when administering insulin because…
It should not enter the muscle as this could cause rapid absorption and hypoglycaemia
At what angle should S/C injection be administered?
90 degrees
True or false: you should aspirate the needle following SC injection
False: do not aspirate the needle
This means drawing blood from the body into the needle
What volume of liquid is injected intramuscularly in the deltoid?
1ml is injected into the deltoid
What volume is injected intramuscularly into the ventrogluteal site
5ml can be injected into the ventrogluteal site
What must we do before delivering medication to elderly frail patients via intramuscular route?
Ensure you ‘bunch up’ the muscle to ensure adequate bulk before injecting
Where would you inject intramuscular injection going into the deltoid muscle?
About 2 finger widths below the acromial process
At what angle do you inject intramuscular injections?
90 degrees
When is the only time it would be recommended to aspirate an IM injection?
when injecting into the ventrogluteal route
Before delivering SC injection what should you do?
stretch the skin
What is anaphylaxis?
A severe life threatening generalised or systemic hypersensitivity reaction
How is anaphylaxis characterised?
Rapidly developing, life threatening airway and / or breathing and or circulation problems
usually with skin or mucosal changes
Who gets anaphylaxis?
mainly children and young adults
Common in females
Incidence seems to be increasing
What causes anaphylaxis?
bee sting, wasp sting
nuts
food e.g. milk, fish, chickpea, banna, snail
antibiotics e.g. penicillin, cephalosproin, vancomycin
anaesthetic drugs - suxamethonium
other drugs - NSAIDs, ACEi, gelatins, protamine, vitamin K, diamorphine
Contrast media
Latex, hair dye,
How is anaphylaxis recognised?
ABCDE approach
A – Airway
Look for airway swelling: hoarse voice, stridor, tongue/lip swelling, difficulty speaking.
Treat immediately with high‑flow oxygen. Call for senior help early.
Airway obstruction is life‑threatening and must be managed first.
B – Breathing
Assess respiratory rate, work of breathing, wheeze, cyanosis, reduced air entry.
Give high‑concentration oxygen (15 L/min via non‑rebreather).
Be alert for bronchospasm → treat with adrenaline IM (first‑line for anaphylaxis).
C – Circulation
Check pulse, blood pressure, capillary refill, signs of shock (pale, clammy, weak pulse).
Anaphylaxis can cause rapid circulatory collapse.
Lay patient flat, elevate legs, give IM adrenaline immediately.
Prepare for IV fluids if hypotensive.
D – Disability
Assess consciousness (AVPU), agitation, confusion.
Hypoxia and hypotension can cause reduced GCS.
Check glucose if possible.
E – Exposure
Look for urticaria, flushing, angio‑oedema, abdominal symptoms.
Remove allergen if still present (e.g., stop infusion).
Maintain dignity and prevent heat loss.
Treat life threatening problems, assess effects of treatment, call for help early, diagnosis not always obvious
Anaphylactic reaction is highly likely when the following 3 criteria are fulfilled…
sudden onset and rapid progression of symptoms
life threatening airway/ and or breathing and or circulation problems
skin and or mucosal changes such as uriticaria, angioedema, flushing
What helps support the diagnosis of anaphylaxis?
Exposure to a known allergen / trigger for the patient helps to support the diagnosis
True or false: skin or mucosal changes must be present for it to be anaphylaxis
False - subtle/absent in 20% of reactions
True or false: Anaphylaxis can cause GI symptoms
True - can cause vomiting, abdominal pain, incontinence etc
What are the airway problems which present in anaphylaxis?
Airway swelling e.g. throat, tongue swelling
Difficulty in breathing and swallowing
Sensation that the throat is closing up
Hoarse voice
stridor
What breathing problems present in anaphylaxis?
shortness of breath
increased respiratory rate
wheeze
patient becoming tired
confusion caused by hypoxia
cyanosis - appears blue - a late sign
respiratory arrest
What cardiac problems occur in anaphylaxis?
signs of shock - pale, clammy
increased pulse rate (tachycardia)
low blood pressure (hypotension)
decreased conscious level
myocardial ischaemia/angina
cardiac arrest
DO NOT STAND THE PATIENT UP
What Disability signs does anaphylaxis cause?
sense of impending doom
anxiety/ panic
decreased conscious level caused by airway, breathing or circulatory problems
Exposure in anaphylaxis - what do we look for?
skin changes are often the first feature
present in over 80% of anaphylactic reactions
skin mucosal or both skin and mucosal changes
erythema - a patchy or generalised rash
urticaria - also called hives, nettle rash, weals or welts anywhere on the body
angioedema - similar to urticaria but involves swelling of deeper tissues e.g. eyelids and lips, sometimes in the mouth and throat
What differential diagnosis must be made if someone has anaphylaxis?
are they have an asthma attack - can present as similar signs, especially in children
septic shock - hypotension with petechial / purpuric rash - bleeding under the skin as seen in meningitis
What non-threatening conditions present similarily to anaphylaxis?
panic attack
breath holding episode in children
vasovagal episode
How do we treat anaphylaxis?
Patient should lie flat and raise legs
Adrenaline should be administered / epinephrine
injected into the muscle - faster onset
Dose of adrenaline in adults and children over 12…
500mcg IM
Dose of adrenaline for children aged 6-12 years…
300 mcg
Dose of adrenaline for children 6months to 6 years
150 mcg
Dose of adrenaline for children less than 6 months
150mcg
Caution the use of adrenaline administered via the…
Intravenous route
Once patient has been admitted to hospital/ when skills and equipment are available and patient has recieved adrenaline, what is next step?
Administer high flow oxygen
Following introduction of high flow oxygen, what should we administer?
IV fluids - fluid challenge
used to treat shock and hypotension
500 - 1000mL IV bolus in adult
20mL/Kg in children
Monitor response - give further bolus as necessary
When adminsitering fluids, would we prefer to use a colloid or crystalcolloid?
Avoid colloids due to risks of allergic reactions and kidney dysfunction
crystalcolloid - small particles in an aqueous solution e.g. glucose and electrolytes whereas colloids have large particles such as proteins and starch
After giving fluids, what do we want to deliver? Second line drugs
Steroids, e.g. hydrocortisone
What do we deliver alongside hydrocortisone
Antihistamine e.g. chloramphenamine
How do we confirm if a patient has had anaphylaxis reaction?
Mast cell tryptase is an enzyme released from mast cells during anaphylaxis. Measuring its level in the blood helps confirm whether a patient has had a true anaphylactic reaction.
When is best time to sample for mast cell tryptase?
after initial resuscitation and feasible to do so,
They peak at 1–2 hours.
They return to baseline within 6–8 hours.
What are autoinjectors?
e.g. epipen/ Anapen
For self use by patients or carers
Should be prescribed by allergy specialist
For those with severe reactions and difficult to avoid triggers
ensure patient is well trained as to how to use the device