L6- The humoural response
1/17
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
18 Terms
what is another name for antibody
Immunoglobulin (Ig)
Parts of antibody
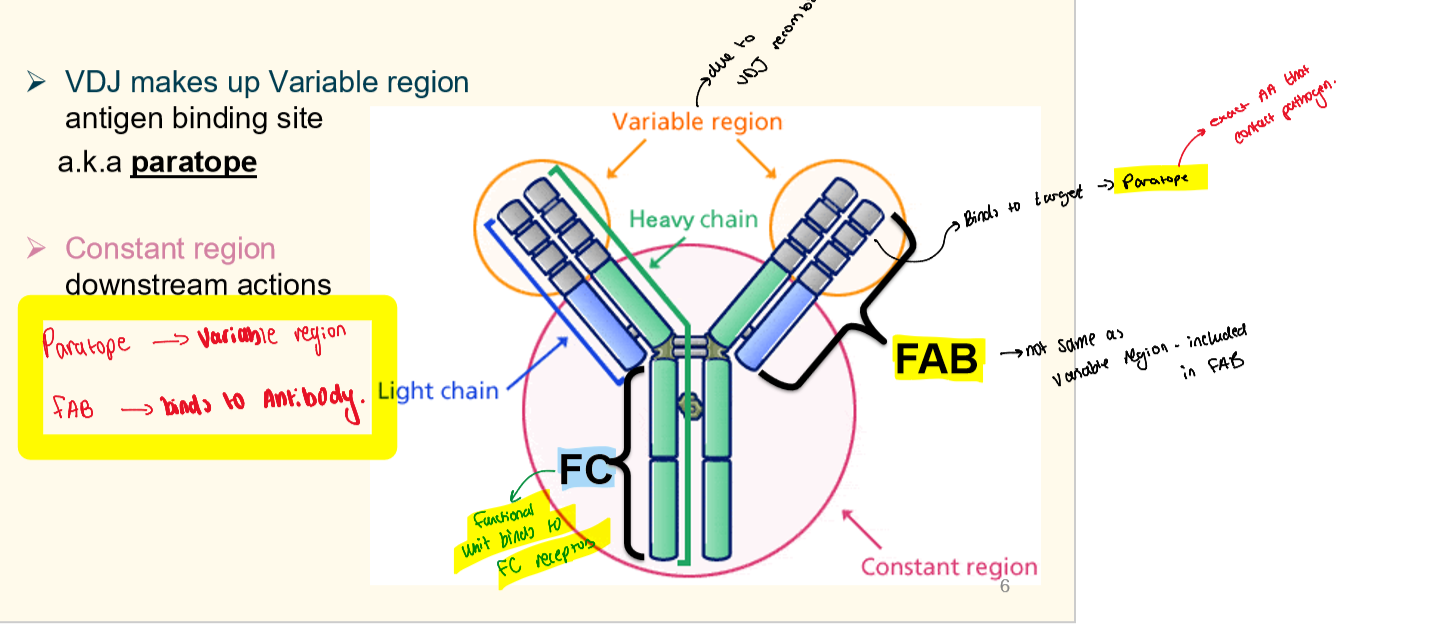
what is epitope
Epitope is on pathogen anitigen binds to partope on antibody
Differnce between BCR and antibody
Antibody is the secreated form of B cell reseptor - they are basically the same thing
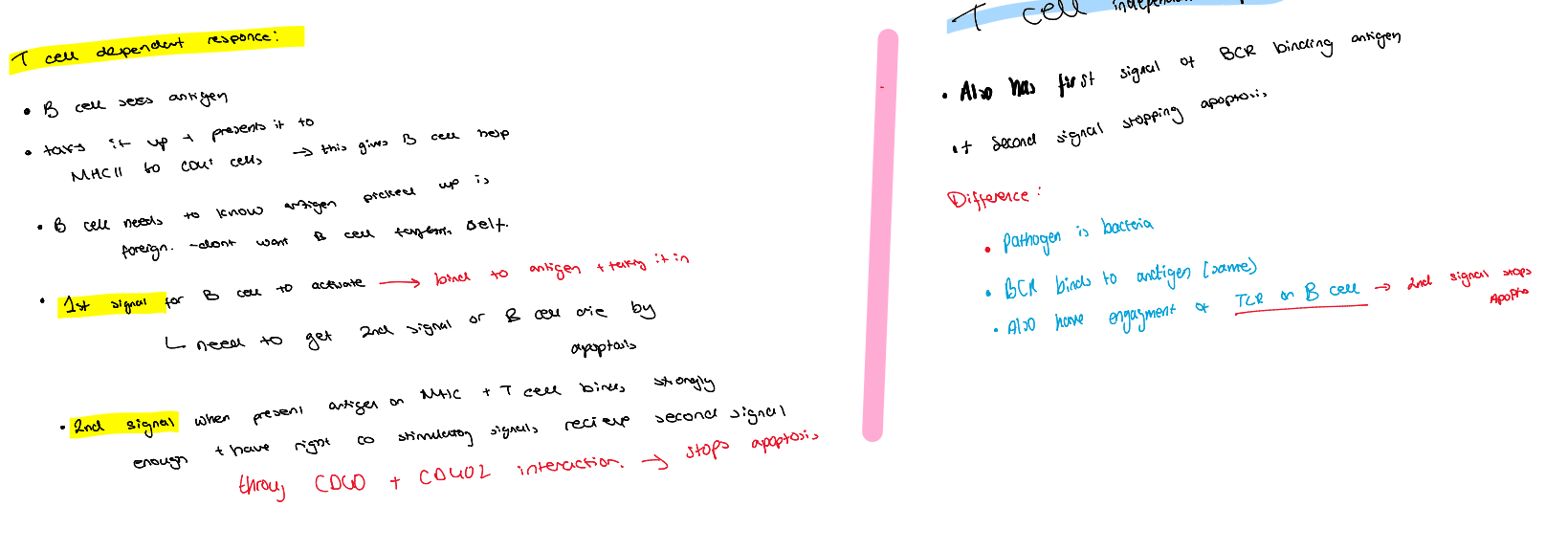
How do we get B cells actiavtion
T cell dependant response (More common)
Antigen binds to BCR → 1st activation signal
peptide presented on MHC, T cell binds, if strong binding through help of assesory protiens liek CD40, CD40L get 2nd activation signal stops B cell form undergoing apoptosis
and T cell independant response
same 1st signal
but 2nd signal is from activatin TLR on B cell
Transmembrane → secreated
DNA starts off with; VDK regions, constant regions and trasmembarane regions
B cell starts off by removing nay unused VDJ regions noy being used
as moves ot plasma blast removes trasmembrane regions
this is why cannot go back to being B cell affer now a plasma blast no longer express BCR
class switch
happens in Niave B cells
before all express IgM or IgY both look same on surface membarne
when class switch happens
cut out constant regions IgM and IgY with enzyme AID
to add IgG, IgA, IgE
non reversible
happens due to environmnet
IgM
first responder
usually as a pentomer as then has higher avidity (alone has low affinity)
good at triggering phagocytosis and activating complement
made in blood, milk, mucous, saliver
IgA
local task force
higher affinity as post germinal center
exists ad dimer, tetrimer or heximer
in secreations, lung, mucosa
improtant in gut - neytralises pathogenic bacteria in gut
IgG
Specelised task force
High affinity as post germinal center
exists as diner
mostly foudn in blood
good at neutralisation and activating complement
different type IgG1,2,3,4
improtant in vaccination
only Ab that can cross the placenta
what happens in germinal center
its in lymph nodes
have Dz and LZ
GZ ahve proliferation and amplification and muatations of BCR
then they move to LZ where they encounter antigen - if have good binding with antigen and tehn TCR then no apoptosis if bad binding then get apoptosis
thoes BCR that survive go back to DZ to proloferate t
they under go mutations on DNA level by AID enzyme, cuts things out helping them get better at binding antigen
this is somatic hypermuatation
if muattaion makes it worse than die by apoptosis
then surviving B cells will exity to be antibody producing cells and produceing high affinty IgG
IgE
low amounts in serum
exists as dimer
binds to Fc receptor leading to degranulation of histoamines leading to coughing, sneezing..
effective againts paracites
IgD
not much knonw
maybe like IgE binding to Fc recptor
low amounts is secreated in blood
mainly used a s a marker to identify niave B cells
What are the things antibody can do when binds to target
neutralisation IgG
Optimization IgG
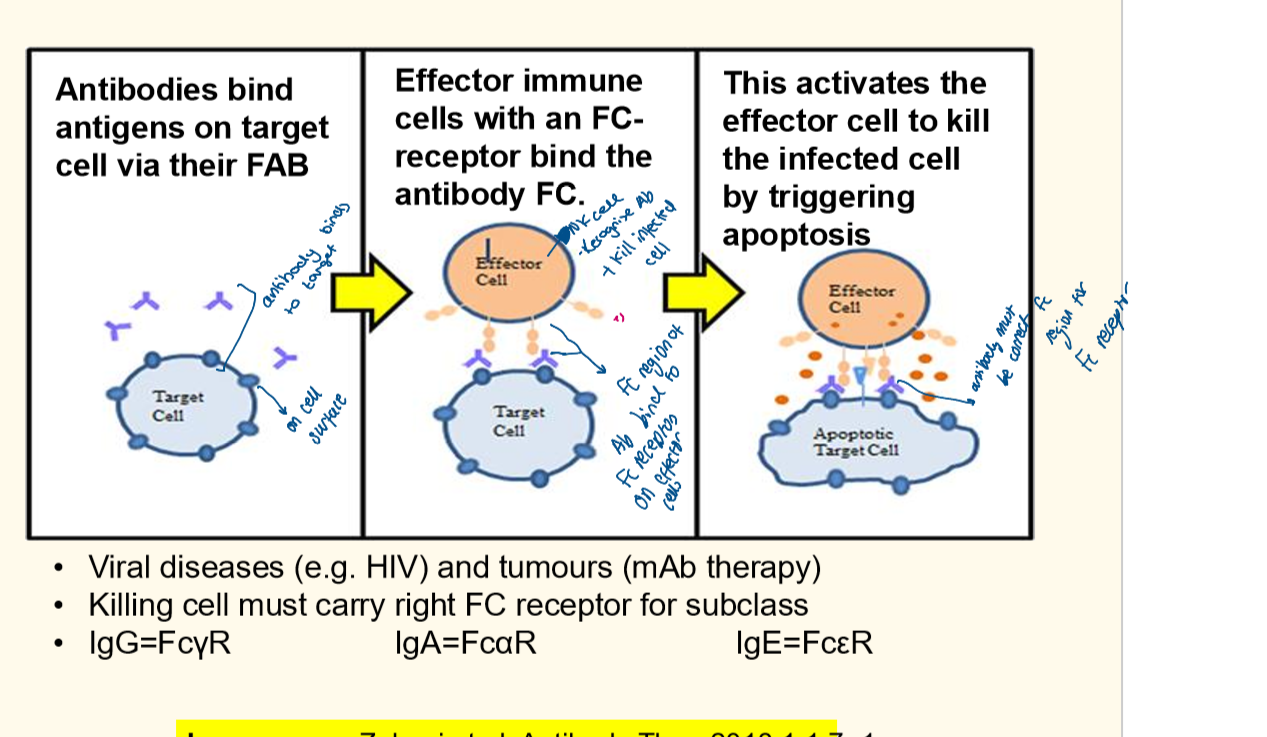
Antibody Dependant Cellular Cytotoxicity IgA/IgG
complement IgM
Neutralisation
antibody binds to part of virus that is needed to enter the cell
so it blocks entry
e.g. In HIV antobodies can bind to part of virus that bonds to human CD4 cells
Fc receptors
phagocytes binds to FC receptors which allow phagocytosis to happen
happens by binding to Fc gamme (IgG)
Antibody Dependant Cellular Cytotoxicity
Complement
antibody binds to pathogen activating C1Q in classical pathway