neuro
1/670
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
671 Terms
List the CNs
- CNN 1 - Olfactory
- CNN 2 - Optic
- CNN 3 - Oculomotor
- CNN 4 - Trochlear
- CNN 5 - Trigeminal
- CNN 6 - Abducent
- CNN 7 - Facial
- CNN 8 - Vestibulocochlear
- CNN 9 - Glossopharyngeal
- CNN 10 - Vagus
- CNN 11 - Accessory
- CNN 12 - Hypoglossal
True or false: Menace is a reflex
- False; It is a learned response
CNs of the menace response?
- Afferent: CNN II (Optic Nerve)
- Efferent: CNN VII (Facial Nerve)
Lesions affecting menace?
- Most common in forebrain lesions
- Cerebellar disease
Visual testing options?
- Exam room navigation
- History of any changes
- Maze
- Light vs. dark room
- Menace
CNs of PLR?
- Afferent: CNN II (Optic Nerve)
Efferent: CNN III (Oculomotor Nerve)
What factors can confound interpretation of PLR?
- Ophthalmologic disease (i.e., iris atrophy can cause asymmetry, retinal disease)
CNs of the palpebral reflex?
- Afferent: CNN V (Trigeminal Nerve)
- Efferent: CNN VII (Facial Nerve) -> Orbicularis oculi muscle
When performing the palpebral reflex on the medial canthus of the eye, which branch of CN V is stimulated? What about the lateral canthus?
- Medial: Ophthalmic
- Lateral: Maxillary
CNs of the retractor bulbi reflex?
- Afferent: CNN V (Trigeminal Nerve; Ophthalmic branch)
- Efferent: CNN VI (Abducens Nerve)
CNs involved in vestibulocochlear movement?
- Afferent: CNN VIII (Vestibulocochlear Nerve)
- Efferent: CNN III, IV, VI (Oculomotor, Trochlear and Abducent Nerves)
Which nerves innervate ocular muscles?
- Oculomotor: Dorsal, medial and ventral recti and ventral oblique
- Trochlear: Dorsal oblique muscle
- Abducens: Lateral rectus and retractor bulbi
Medial strabismus indicates dysfunction in which CN? What about ventrolateral strabismus?
- Medial: Abducens
- Ventrolateral: Oculomotor
Three types of pathologic nystagmus?
- Horizontal
- Rotary
- Vertical
Horizontal or rotary nystagmus that is non-changing implies __________ vestibular localization. Any nystagmus that changes with position or has a vertical character implies a more ________ lesion.
- Peripheral
- Central
Nystagmus is named for the fast or slow component?
- Fast
True or false: The Dolley's eye reflex is a physiologic nystagmus in which the slow phase is mediated by the brainstem and the oculocephalic component is mediated by the cerebrum.
- True (Normal reflex is present when moving the pt's head causes eyes to move in opposite direction to maintain the gaze fixed forward)
When is testing the oculocephalic/Doll's eye reflex most fruitful?
- Cases of head trauma
How is vestibular rebound tested?
- Turn head to either side 45 degrees and let the head fall after - the rebound occurs secondary to over compensation by the normal side (indicative of dysfunction)
How is cerebellar rebound tested?
- Hold head straight up and let fall
- Lack of cerebellar control results in dramatic acceleration of the head downward
CNs which mediate nasal/facial sensation?
- Afferent: CNN V (Trigeminal)
- CNN XI (Accessory n.; mediates body movement away from stimulus) and CNN VII (Facial n.; mediates twitching of skin)
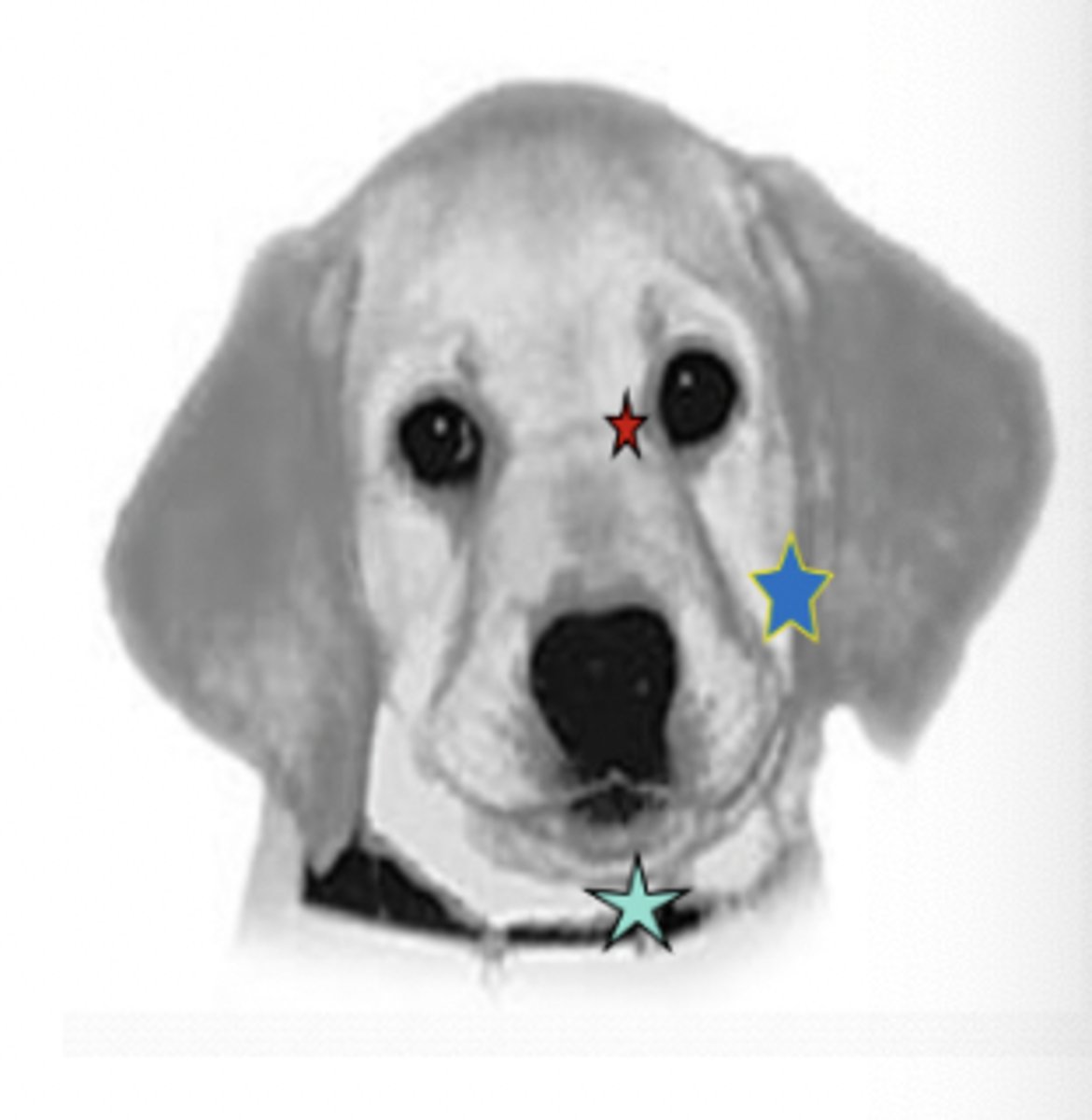
What are the three branches of the trigeminal nerve?
- Ophthalmic (red)
- Maxillary (blue)
- Mandibular (green)
The motor component of the mandibular branch of the trigeminal nerve innervates what muscles?
- Innervates muscles of mastication (Masseter, temporalis, rostral digastricus, pterygoid, mylohyoid muscles)
Facial symmetry and signs such as drooping lips/drooling/dropping food are mediated by which CN?
- CN VII
How does one assess function of CNs IX, X, XI, and XII? If dysfunction is observed, one should beware of which disease?
- Through observation of swallowing, tongue movements, and atrophy of muscle groups; Can also palpate cervical muscle mass
- Rabies
Ideal space/factors in which to perform a neurologic exam?
- Quiet room
- Time (May be difficult to be thorough in a 30 min apt slot)
- Carpet or non slippery floor
- Area to observe gait
- Non obstructive areas (no where to hide) for cats
- +/- table for small dogs/cats
Instrumentation needed to perform a neurologic exam?
- Dark room
- Strong light source
- Indirect bio lens
- Hemostats
- Pleximeter/"Neuro Hammer"

*Components of the neurologic exam?
- Mentation/General Observation
- Body/head posture
- CNs
- Gait
- Proprioception
- Motor/spinal reflexes
- Sensory assessment
Two components of mentation and what they are mediated by?
- Level of consciousness (Brainstem; Ascending reticular activating system)
- Content of consciousness (Forebrain)
Categorizations of level of consciousness?
- Alert
- Dull/Obtunded
- Stuporous: Responds to noxious stimuli
- Comatose: No response to noxious stimuli
Categorizations of content of consciousness?
- Appropriate for surroundings
- Agitated or reticent (reserved)
- Aggressive vs. timid
- Changes in habits
- Pacing
- Inappropriate urination/defecation
- Changes in sleep/wake patterns
What is the difference between paresis and paralysis?
- Paresis: Weakness
- Paralysis: Lack of voluntary motor movement
Define Mono vs. Hemi vs. Para vs. Tetra.
- Mono: One limb
- Hemi: One side of the body (right or left limbs)
- Para: One half of the body (front or hind limbs)
- Tetra: All four limbs
What are the three forms of ataxia? Briefly describe them.
- Vestibular - Listing/leaning/rolling/veering
- Cerebellar - Dysmetria/hypermetria of one or all limbs
- Proprioceptive - Crossing over of front/hind limbs/evidence of nail wear/dragging of front or hind limbs
Postural reactions test the function of what?
- The proprioceptive tracts
- Sensory and motor involved
Which postural reactions require movement of the limb to correct for displacement? These reactions are accentuated by __________.
- Hopping, Wheel Barrow, Extensor Postural Thrust
- Weakness
Of hopping, wheel barrow, and extensor postural thrust, which is the most sensitive for minor deficits?
- Hopping
How does one interpret the results of a hopping test in which the pt has poor initiation? What about if the pt has poor follow through?
- Poor initiation: Proprioceptive deficit
- Poor follow through: Motor deficit (paresis)
Why are proprioceptive positioning/placing tests performed with some support of the animal's weight?
- So weakness has less of an influence
How does one perform proprioceptive positioning/placing tests?
- Gently turn animal's paw over and they should immediately replace (Watch out for withdrawal)
- Tactile placing test: Bring the animal to edge of platform/table without being able to visualize it and watch for proper placement
- Visual placing test: Repeat the test above but allow the animal to visualize normally; They should "reach" for the surface
How are withdrawal reflexes tested?
- Noxious stimulus applied to toe and entire limb should flex
- Test both medial and lateral toes
*Which nerves are involved in the withdrawal reflexes of the thoracic and pelvic limbs.
- Thoracic: Axillary, musculocutaneous, median, ulnar and radial nerves (C6-T2)
- Pelvic: Sciatic nerve (L6-S1)
True or false: Withdrawal reflexes require input from the brain.
- False
*The patellar reflex tests which nerve? It should result in what action?
- Femoral nerve (L4-L6)
- Extension of stifle
*The cranial tibial reflex tests which nerve? It should result in what action?
- Peroneal branch of the sciatic nerve (L6-7)
- Flexion of hock
*The extensor carpi radialis reflex tests which nerve? It should result in what action?
- Radial nerve (C7-T1)
- Slight extension of carpus
*How is the perineal reflex tested? What nerve is involved?
- Light stimulation of the perineum with forceps -> Should "wink"
- Pudendal nerve (S1-3)
*Nerves of the brachial plexus?
- SSMARMU
- Suprascapular
- Subscapular
- Musculocutaneous
- Axillary
- Radial
- Median
- Ulnar
How is vertebral palpation performed?
- Cervical: Ventral palpation starting at thoracic inlet (Too much muscle mass dorsally) with gentle flexion and extension
- Thoracolumbar: Over dorsal spinous processes or just lateral to them while supporting gently under the abdomen
Which nerve and muscle are involved in the cutaneous trunci/panniculus reflex? How can it be interpreted
- Lateral thoracic nerve (C8-T1) >> cutaneous trunci muscle
- As you perform caudal to cranial, if there is a deficit you will begin seeing rxn approximately 2 vertebral bodies caudal to the lesion
When is the Panniculus reflex most sensitive?
- When voluntary motor is lost
A pt walks into your clinic with a normal gait and a history of seizures. Should you test for superficial/deep pain during your neurologic exam?
- No (If pt is walking normally, do not need to check for pain)
True or false: When testing for deep or superficial pain, a withdrawal of the limb indicates the pt perceived the pain.
- False
What are the key divisions of the nervous system?
- Brain
- Spinal Cord: C1-C5 / C6-T2 / T3-L3 / L4-S2 segment
- Neuromuscular
What are the key divisions of the brain?
- Forebrain (Cerberum/Telencephalon)
- Thalamus (Diencephalon)
- Brainstem
- Cerebellum (Note it is in a very vulnerable location)
- Ventricles
What are the lobes of the forebrain?
- Frontal Lobe: Intellect and behavior
- Temporal Lobe: Emotion (Aggression, fear)
- Parietal Lobe: Proprioception and nociception
- Occipital Lobe: Vision
Which structure produces CSF?
- Choroid plexus
Obstruction of the ventricles of the brain can result in what?
- Hydrocephalus
What comprises white and grey matter?
- Grey matter: Nuclei
- White matter: Axons
Components of the neuromuscular division of the nervous system?
- Nerve root(s)
- Peripheral Nerve
- Neuromuscular junction
- Muscle
Disease of which component of the nervous system will result in change in the content of consciousness?
- Forebrain disease (Behavior, habits, intellect, personality, abnormal elimination habits, abnormal wake/sleep cycles, failure to recognize O, change in demeanor)
*Common signs of forebrain disease?
- Seizures (Focal/Partial/Generalized)
- Altered mental status (disorientation, change in routine, lethargy)
- Circling (Wide), pacing, obsessive or aimless wandering (All in the direction of the lesion, usually)
- Head pressing
- Proprioceptive ataxia
- Papilledema, irregular respiration
- Contralateral deficits: Partial CN deficits, CP deficits, hemiparesis, hemi-sensory loss, UMN reflexes, visual impairment with normal PLR
*Signs of thalamic disease?
- Normal or abnormal gait
- Altered mentation/behavior
- Aggression/excitability
- Circling/Pacing/Wandering/Head pressing
- Bilateral CNN II deficits (lesion at the level of the optic chiasm): Pupil dilation, visual loss, decreased PLR
- Abnormal temperature regulation (Hyper/hypothermia)
- Abnormal appetite (Increased or decreased)
Thalamic disesae can cause what other disorders?
- Endocrine disturbances: DI, DM, Cushings (I.e. pituitary macroadenoma), Addison's
- Seizures
Components of the brainstem?
- Midbrain
- Pons
- Medulla
*Main finding of brainstem disease?
- Change in level of consciousness (alert/obtunded/stuporous/comatose) but appropriate
*Other clinical findings of brainstem disease?
- Level of consciousness change
- Ipsilateral conscious proprioceptive deficits
- Spastic (UMN) weakness or paralysis of all four limbs or limbs on the ipsilateral side
- UMN reflexes ipsilateral to side of the lesion
- Ipsilateral multiple CNN deficits (III-XII) -> Complete LMN deficits
- Ventilatory/PLR changes
*Function of cerebellum?
- Functions to regulate the range, rate and force of a movement
- Inhibitory
*Dysfunction of the cerebellum results in what?
- Dysinhibition
*Signs of cerebellar disease?
- Dysmetria of the head (Intention tremor)
- Dysmetria of the eyes (Pendular or oscillatory nystagmus)
- Dysmetria of the limbs (Hypermetria, goose-stepping)
- Truncal/Cerebellar ataxia (Hypermetria to dysmetria, cerebellar rebound)
- Absence of behavior change (normal mentation)
- Absence of proprioceptive deficits/weakness
- Ipsilaterally absent menace
- Broad-base stance with preservation of strength
*Key features of vestibular disease?
- Head tilt (Only exception is bilateral otitis media-interna)
- Vestibular ataxia ("Drunken sailor")
- Pathologic nystagmus
What structures run within the middle ear?
- CN 7 and sympathetic tract (chorda tympani)?
Forms of physiologic nystagmus?
- Oculocephalic reflex - Forebrain (move head quickly side-side, eyes slow return to center)
- Doll's eye reflex - Brainstem (move head slowly side-side, eyes quickly return to center)
Forms of pathologic nystagmus?
- Sustained and non-positional
- Positional
- Horizontal/rotary/vertical downbeat
Describe peripheral vestibular nystagmus. What about central?
- Peripheral: Sustained, non-changing, rotary or horizontal nystagmus with fast phase away from side of head tilt
- Central: Changes with position, rotary, horizontal, or vertical downbeat
Peripheral vestibular disease can occur where? What about central?
- Peripheral: CNN VIII and its receptor
- Central: Flocculonodular lobe (cerebellum), vestibular nuclei, (medulla), MLF
*Signs of peripheral vestibular disease?
- Head tilt towards side of lesion
- Loss of balance, rolling, falling usually toward the side of the lesion
- Sustained, non-changing horizontal or rotary nystagmus (Fast phase away from lesion)
- Normal to increased myotatic reflexes
- +/- increased extensor tone on side opposite head tilt
- Normal strength/proprioception
- Normal CNN reflexes (Exception is CNN VII/Horner's Syndrome if otitis media)
- Strabismus of affected side
*Signs of central vestibular disease?
- Head tilt away from lesion (if paradoxical) or towards the lesion
- Loss of balance/falling/rolling
- Positional/changing nystagmus away from lesion
- Other brainstem signs: Ventrolateral strabismus, complete LMN deficits of CN I, VI, VII, +/- cerebellar signs, change in level of consciousness, hemiparesis/CP deficits ipsilateral, vomiting/nausea
*Signs of a C1-C5 lesion?
- +/- tetraparesis/plegia in severe cases
- Hyperpathia (pain) of the neck
- Ipsilateral CP deficits or bilateral in fore/hindlimbs
- +/- Ipsilateral hemiparesis/plegia
- UMN fore- and hindlimb reflexes
- Neck fasciculations
- Normal withdrawal reflexes in all four limbs
- +/- intact pain perception
- +/- diaphragmatic paralysis (Phrenic nerve involvement in C4-C6)
- Abnormal head carriage
- Root signature (Lameness associated with nerve root impingement)
*Signs of a C6-T2 lesion?
- Ipsilateral hemiparesis/plegia (if severe)
- Ipsilateral CP deficits fore/hind limbs
- LMN signs (hyporeflexia) fore limb(s)
- UMN signs (hyperreflexia) hind limb(s)
- +/- Horner's Syndrome (T1 - T3)
- Abnormal head carriage +/- cervical pain
- +/- loss of conscious pain perception
What disease affecting C6-T2 are Dobermans predisposed to?
- Disc-associated low cervical spinal cord compression
*Signs of a T3-L3 lesion?
- Ipsilateral or bilateral paraparesis/paraplegia
- CP deficits one or both hind limbs
- UMN reflexes in hind limbs
- +/- UMN tone fore limbs if T13-L2 lesion severe (Border cells)
- Spinal hyperpathia (thoraco-lumbar area or referred)
- +/- panniculus loss
- +/- loss of conscious pain perception hind
*Signs of a L4-S2 lesion?
- Ipsi- or bilateral paraparesis/paraplegia
- Normal fore limb myotatic reflexes, strength
- Hind limb LMN reflexes and diminished withdrawal reflexes unilateral or bilateral (L4 -L6 vs. L7 - S2)
- CP deficits unilateral or bilateral hind limbs
- Urinary/fecal incontinence
- Decreased anal tone, perineal reflex
- Change in tail carriage
- L-S hyperpathia on palpation +/- rectal exam
Caudal cervical spondylomyelopathy is typically a lesion of what spinal cord segment? Signs?
- Typically a C6-T2 lesion
- Hindlimb signs (>forelimb signs) with progressive improvement over time
Signs of a radiculopathy (Nerve root disease)?
- Spinal hyperpathia/hyperesthesia
- Root signature
- Generalized weakness/paralysis
- Voice change
- LMN signs to one limb/multiple limbs dependent on cause
- Normal mentation
- +/- Horner's Syndrome
- Muscle atrophy (focal or generalized)
- +/- Sensory loss
*Signs of a motor neuropathy?
- Flaccid paresis or paralysis of innervated structures (limb, facial muscles, esophagus, anus)
- Neurogenic muscle atrophy
- Reduced or absent reflexes and muscle tone
- Muscle fasciculations/voice change
Signs of a sensory neuropathy?
- Decreased pain response or sensation
- Proprioceptive deficits
- Abnormal sensation or sensitivity (paresthesia) of face, trunk or limbs
- Self-mutilation
- Reduced or absent reflexes without muscle atrophy
Signs of an autonomic (+/- sensorimotor) neuropathy?
- Anisocoria or dilated pupils
- Decreased tear secretion
- Decreased salivation
- Bradycardia
*Signs of a neuromuscular junctionopathy?
- Normal mentation
- +/- palpebral/menace deficits
- Generalized motor weakness or paralysis dependent upon the cause
- Episodic or continual signs
- Normal or hyporeflexic myotatic and withdrawal reflexes
- +/- voice change
Signs of myopathies?
- Generalized weakness
- Exercise intolerance
- Stiff, stilted gait
- Localized or generalized muscle atrophy
- Generalized muscle hypertrophy
- Dimple contracture
- Muscle pain on palpation
- Limited joint movement (i.e., contracture)
- +/- voice change (if severe)
- +/- trismus (inability to open the mouth)
When is neurosurgical intervention an option for an animal with brain trauma?
- Extradural hemorrhage
- Depressed skull fracture(s)
- Worsening neurologic status despite aggressive conservative management
Steps to consider in management of brain trauma?
- BP measurement
- Serial BG measurement
- Serial neuro exams
- Fluid therapy
- +/- steroids (Controversal)
What is spinal cord injury?
- SCI comprises primary and secondary injury along with sustained compression
What is primary spinal cord injury?
- Occurs at impact
- Parenchyma/vasculature directly damaged by compression, contusion, shearing, laceration or stretching
What is secondary spinal cord injury?
- Depletion of neuronal ATP
- Intracellular accumulation of calcium and sodium
- Formation of oxygen free radicals
- Increases in cytokine production/extracellular levels of glutamate, lactic acid, nitric oxide
T3-L3 radiculopathy signs?
- Recurrent back pain
- Positive response to steroids/NSAIDS then relapse once off the drugs
When do pts with T3-L3 radiculopathy need referral?
- Side effects to the drugs
- Recurrence of signs are decreasing quality of life
- Possibility of regression to myelopathy signs
L4-S2 myelopathy/radiculopathy signs?
- Recurrent back pain with minimal neurologic deficits
- Short, choppy gait
- Holding tail down
- Changes in urination/defecation
- Pain on tail extension
- Signs can be recurrent and intermittent
- Intermittent response to NSAIDS or steroids
Indications for immediate referral in pts with T3-L3 signs?
- Signs progress over a period of hours
- Signs are immediate
Indications for immediate referral in pts with C1-C5 or C6-T2 signs?
- Signs progress over a period of hours to days
- Signs are immediate