omm spring practical 3
1/62
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
63 Terms
dx sc joint
proximal clavicle
spring test (superior to inferior, anterior to posterior)
the side that has less springing is the side you’ll diagnose
check motions by placing two fingers at proximal clavicle
have patient move (abduct, adduct, flex, extend)
name for direction of ease
dx ac joint
spring test superior to inferior in distal clavicle
you can ask pt which side they’re having issues with
dx side with most restriction
check range of motion by passively moving pt arm
compare both sides (check one arm at a time)
movement pairings
adduct, external rotation, inferior glide
abduct, internal rotation, superior glide
dx gh joint
assess active ROM (ballerina pose - dysfunctional side is the one with the lower arm) or ask pt which side bothers them
Place digits 3 and 4 on ball anteriorly and thumb on humerus posteriorly
do passive ROM and check for restriction
dx ulnohumeral joint
tell pt to do active forearm pronation and supination
ballerina pose (arms go overhead)
is there’s a side that’s bothering you?
Feel for both medial and lateral olecranon process.
Two-hand hold possible OR place thenar/hypothenar on one end then cup using fingers while other hand grabs wrist rather than hand instead.
Naturally elbow should be 5-45°
Test for ROM (Abduct, adduct, flex, extend)
greater angle with carrying position = prefers aBduction
aBduction SD = arm is more angulated = increased carrying angle.
aDduction SD = arm appears straighter = decreasing the carrying angle (producing a “gunstock deformity”).

dx radial head / radioulnar joint
Easy posterior glide on pronation = posterior SD
Test active ROM bilateral
Locate medial epicondyle then go to lateral epicondyle then more distal
Divot when arm is extended and go to the BOTTOM of the divot. Feel the bone and PINCH
Pt arm flexed 90
Test for right area using pronation and supination
Dx focused on more proximal area

dx radiocarpal joint (wrist)
test active ROM bilateral
Put thumbs on anterior/palmar surface of proximal carpals. On backside, fingers are monitoring posteriorly.
Compare side to side with wrist flexion and extension
Now do radial and ulnar deviation.
On practical just need to name one of the SD if you find two.
dx oa (cervical spine)
OA joint = “opposite always” (deep sulcus = side of rotation so SB will be opposite of that)
for examination: translate head from left - right and right to left with head in neutral position
dx: determine translation (gives S/R) check with slight flexion/extension
ex: if motion is greater from L to R, freedom is side-bent L and rotated right (restriction in right side-bending), if restriction of lateral translation is MORE signficant in flexion, but goes away in extension, then the segment is extended
dx aa (cervical spine)
AA joint = rotation only
you must be standing
1. ensure pt nods head forward to lock out OA joint
2. flex pt next to approx 45 degrees until locking occurs below the AA joint in the rest of the cervical spine
3. slowly rotate head from midline to left and then midline to right
if head rotates more freely to the right the diagnosis is AA Rr
dx c2-c7
follows type 2-like (rotation & side bending = same)
check for flexion/extension
cervical landmarks:
C2 - mandible
C3 - hyoid
C4 - superior aspect of thyroid
C5 - thyroid cartilage
C6 - cricoid ring
C7 - vertebral prominence
dx t1-t4 or t5-t12
screen (TART changes)
T1-T3 = TP is same level as SP
T4-T6 = TP ½ level up
T7-T10 = TP whole step up
T11 = TP ½ level up
T12 = TP same level
thumb rolling superior = flexion, inferior = extension
dx ribs
TART changes (i.e. red reflex, skin drag)
spring test while pt is prone
focus on side with + spring test
assess breathing
inhalation dysfunction = likes to stay inhaled (will have trouble moving caudad in exhalation)
exhalation dysfunction = likes to stay exhaled (will have trouble moving cephalad in inhalation)
BITE = inhale (bottom rib = key rib); exhale (top rib = key rib)
side w/ less motion = dysfunctional side, name for freedom
rib 1-5 = pump handle
rib 6-10 = bucket handle
dx lumbar spine
dx can be done seated
sphinx = testing for extension
child’s pose = testing for flexion
landmarks = iliac crest btwn L4/L5
Type 1 = opposite N S R
Type 2 = same side F/E R S
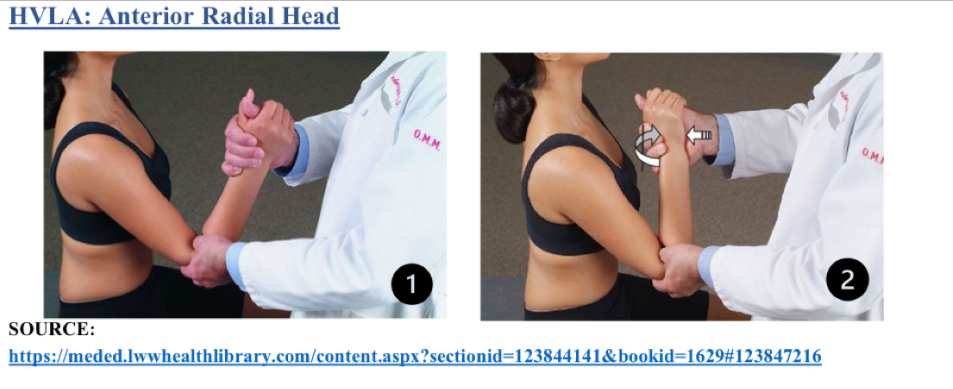
hvla anterior radial head
Pt seated, physician stands facing pt
Thumb on anterior head
Other hand is shaking hands
Rotate forearm into pronation until barrier
Flex into barrier
Thrust is a flex from hand holding wrist
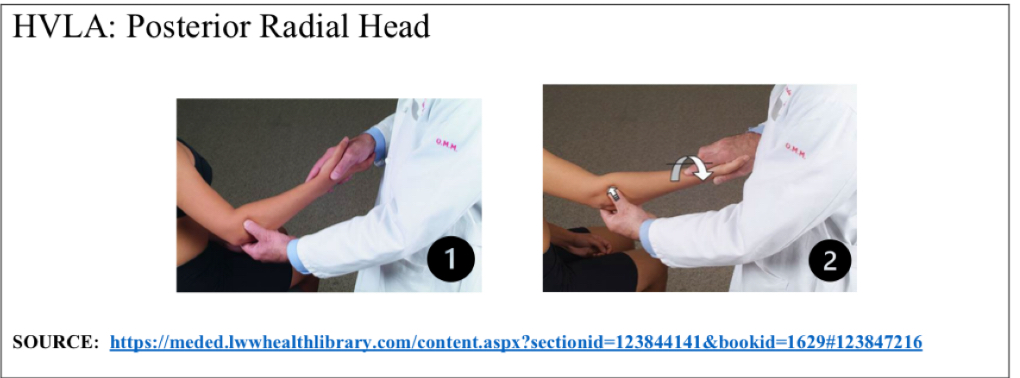
hvla posterior radial head
Pt seated, physician stands facing pt
Thumb on posterior aspect of radial head
Other hand holds pt hand like hand shake
Supinate forearm into barrier
Extend forearm into barrier
Thrust into extension
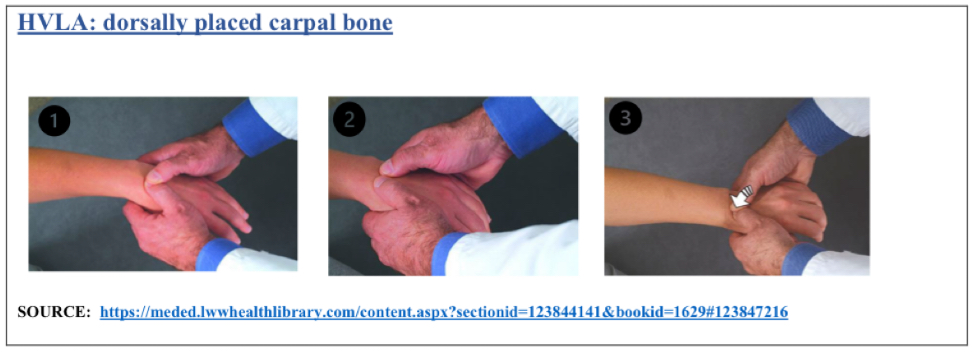
hvla displaced carpal (standard)
Dorsal displaced = flexed sd
Ventral displaced = extended sd
Pt seated, physician faces pt
Hold wrist like dx
Extend/flex into barrier while maintaining pressure
Thrust is baby whip further into barrier
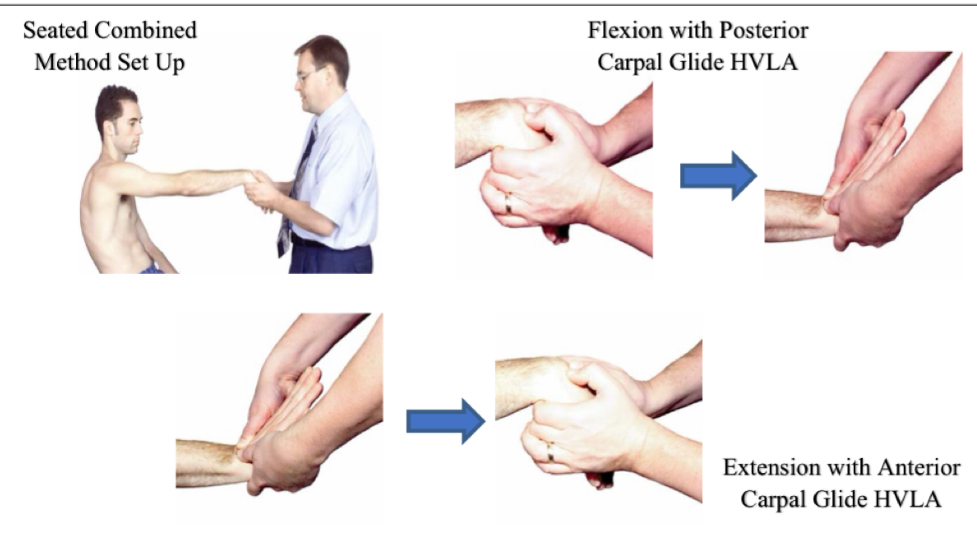
hvla seated combined method
Pt seated, physician faces pt
Hold wrist like dx
Extend/flex into barrier while maintaining pressure
pt will lean back for slightly back for traction
Thrust is baby whip into barrier
Flex SD w posterior glide
Extension SD w anterior glide
hvla ulnohumeral
ABd with medial glide
Pt seated, physician in front of pt
Thumb under medial epicondyle and thenar eminence will act as fulcrum
Other hand holds wrist to ADd and slight extension
Thrust on both hands. Olecranon goes lateral, wrist goes medial
ADd with lateral glide
Pt seated
Thumb on lateral aspect of olecranon and extend elbow slightly
Abduct forearm into barrier
Thrust is olecranon goes medial and wrist lareral.
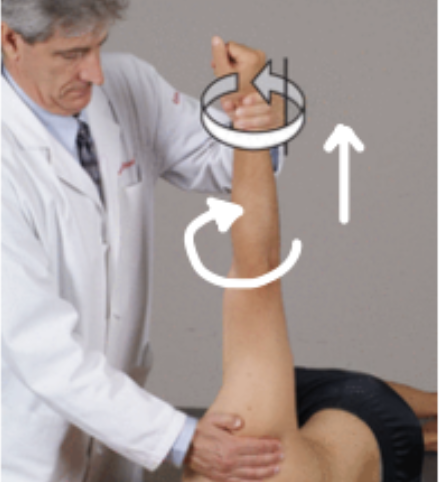
met sc joint - adduction sd (superior glide)
patient is supine
stand on same side of dysfunction
place one hand on proximal clavicle
other hand grabs wrist to extend and internally rotate arm
patient raises arm to ceiling
engage in barrier by moving arm down (no need to further internally rotate)
repeat 3-5 times + passive stretch
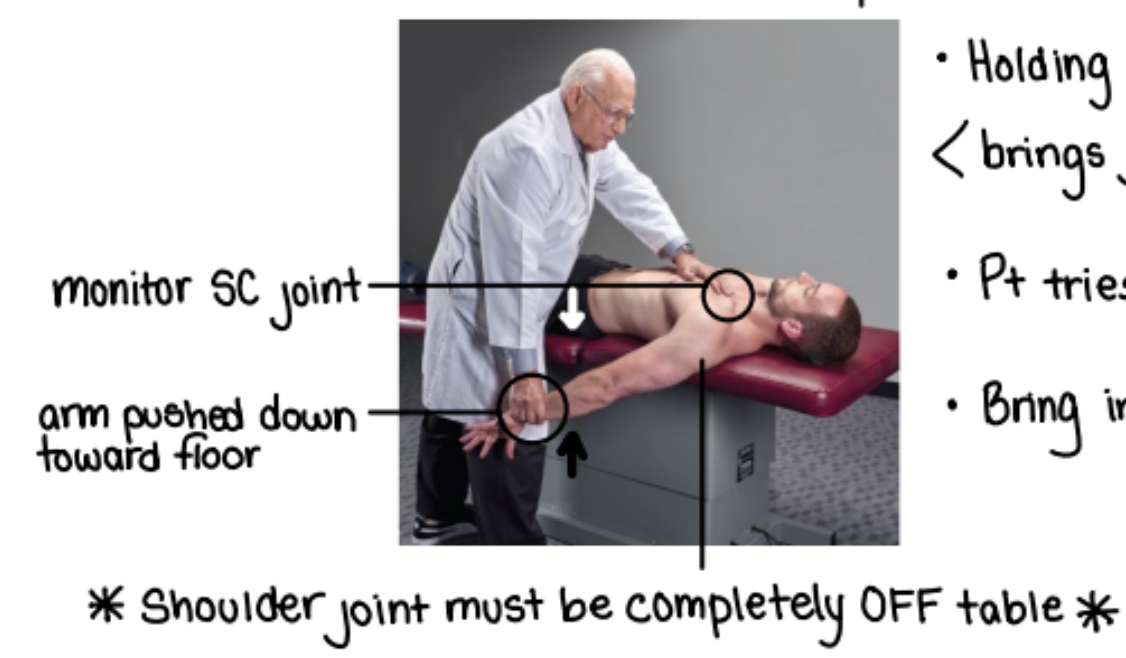
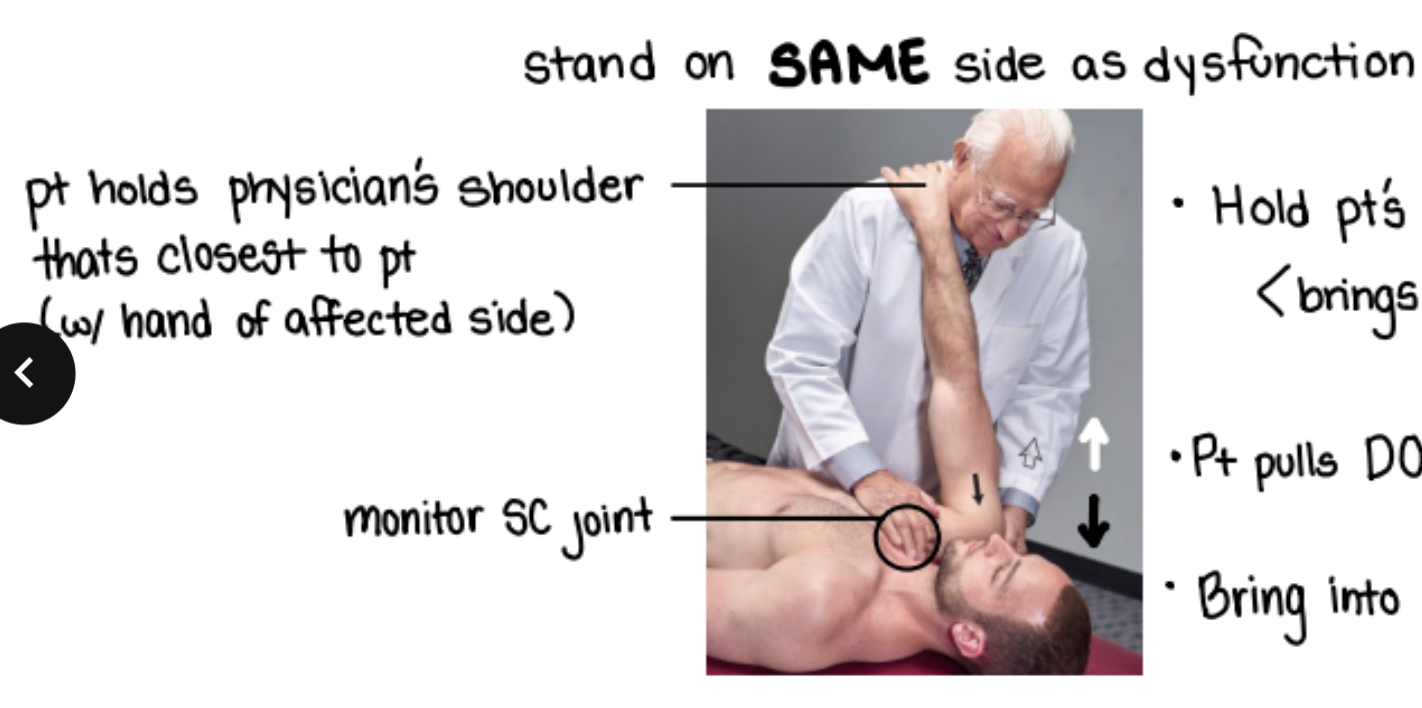
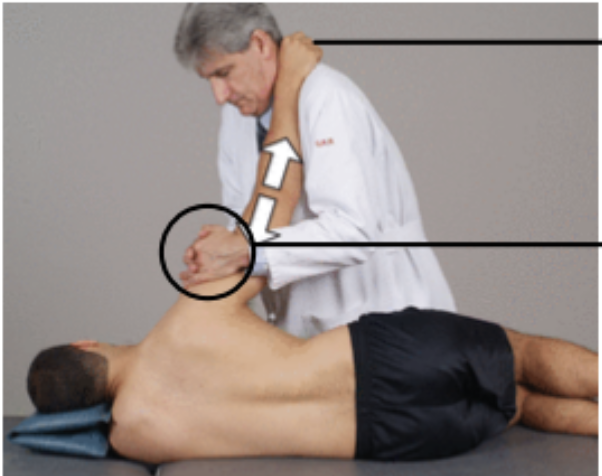
met sc joint - extension sd (anterior glide)
patient is supine
stand on same side of dysfunction
with one hand monitor SC joint
other hand cups scapula
ask patient to hold onto your shoulder with their SD arm
pull scapula up which moves distal clavical anterior (kind of balances the dysfunction out since SC joint is anterior)
patient pulls shoulder back
engage in barrier by pulling scapula further up
repeat 3-5 times + passive stretch
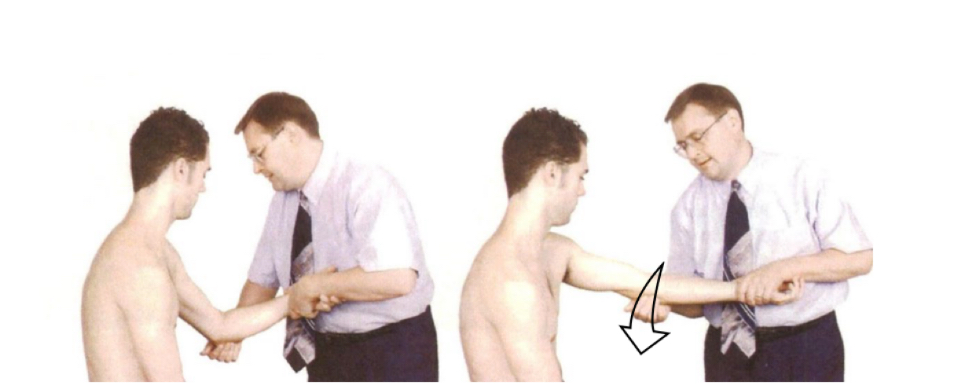
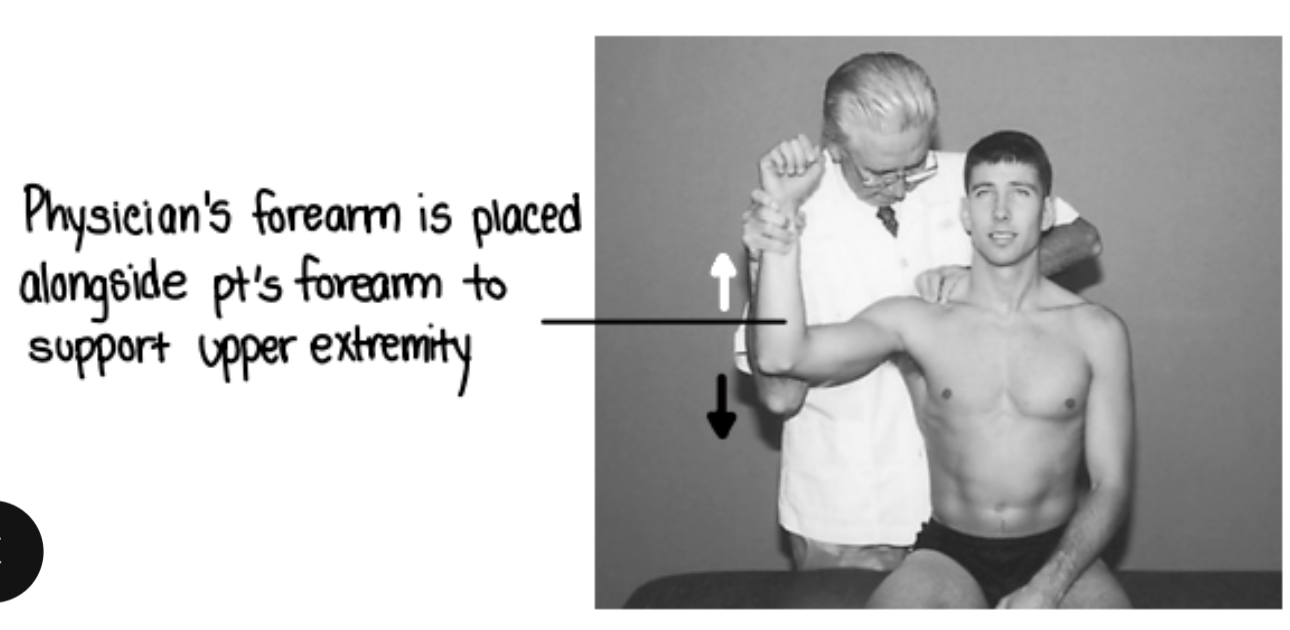
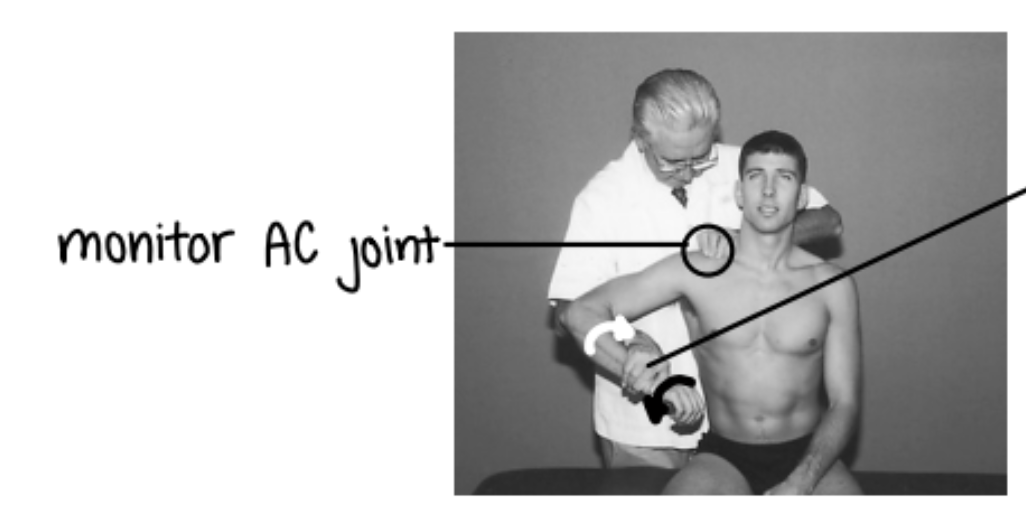
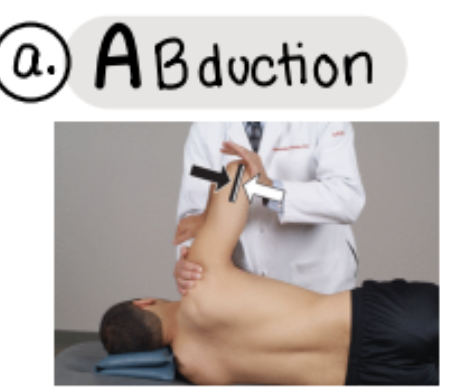
met ac joint - internal rotation sd
patient is seated + you stand behind them
stabilize lateral end of clavicle
monitor AC joint
flex 30, abduct 90
hold distal forearm
EXTERNALLY rotate
pt will internally rotate
met ac joint - external rotation sd
patient is seated + you stand behind them
stabilize lateral end of clavicle
monitor AC joint
flex 30, abduct 90
weave through to hold distal forearm
INTERNALLY rotate
pt will externally rotate
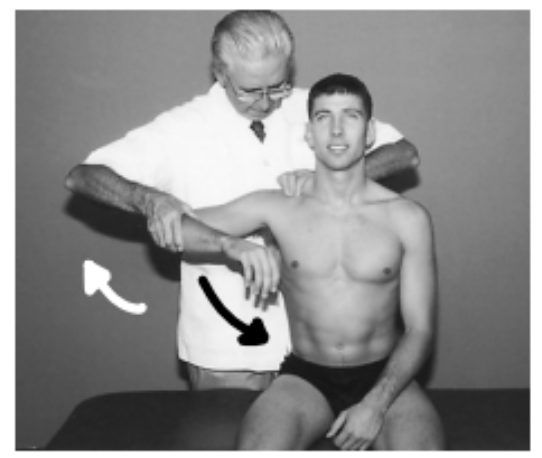
met ac joint - adduction sd
patient is seated + you stand behind them
compress distal clavical towards AC joint
flex 30 + abduct into barrier
patient adducts/moves to freedom
met gh joint (spencer position based on dx)
spencer positions:
extension → flexion sd
flexion → extension sd
circumduction (compression/traction) → idk wot the sd would be sorry
abduction → adduction sd
adduct → abduction sd
internal rotation → external rotation sd
pumping → idk wot this would be either LOL
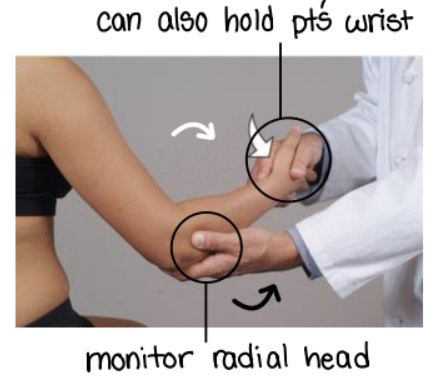
met elbow (radial head)
pronation sd = posterior radial head
monitor radial head with one hand
other hand holds pt’s wrist
supinate pt forearm to engage in barrier
pt tries to pronate forearm against resistance
bring into new barrier by adding supination
repeat 3-5 times + passive stretch
supination sd = anterior radial head
same set up just opposite movement
pronate pt’s forearm
pt tries to supinate
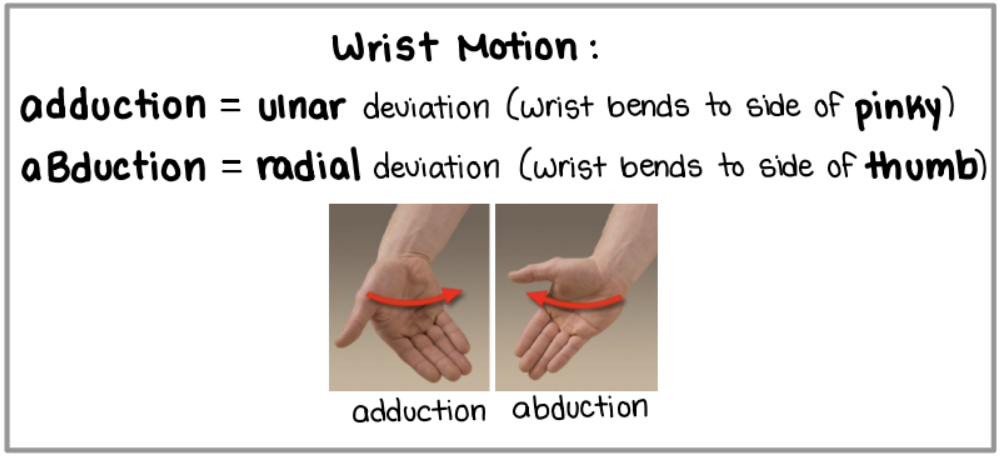
met wrist
monitor radiocarpal joints!
abduction sd = pt prefers deviation to thumb
physician moves pt wrist into adduction (to pinky)
pt tries to move wrist into abduction (to thumb)
bring into new barrier by moving wrist more towards pinky
adduction sd = pt prefers deviation to pinky
same set up as above just opposite movements
extension sd
physician oves pt wrist into flexion
pt tries to move wrist into extension
bring into barrier by moving wrist further into flexion
flexion sd
same set up as above just opposite movements
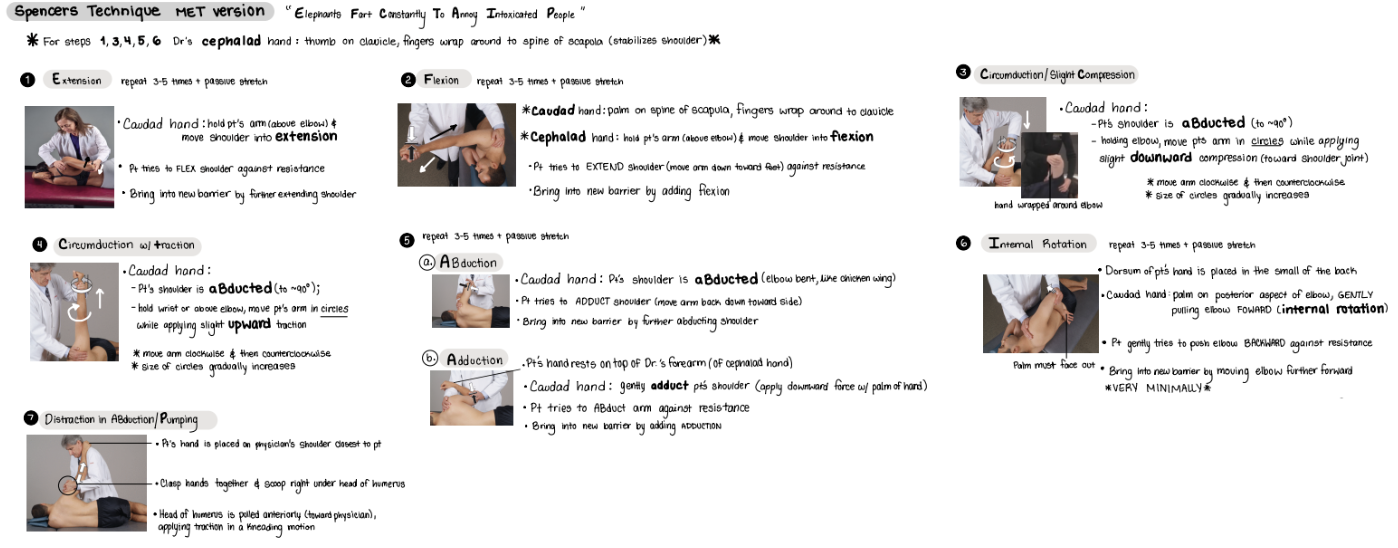
full spencer (7 steps) articulatory technique without met
elephants fart constantly to annoy intoxicated people
note that the techniques are where you position the patient
extension
flexion
compression (circumduction)
traction (circumduction)
abduction/adduct
internal rotation
pumping
spencer technique - extension
patient on lateral recumbent (on their side)
cephalad hand grabs patient’s shoulder to lock AC and SC joint
caudad hand holds patient’s arm above elbow and moves shoulder into extension
patient resists by flexing shoulder
repeat 3-5 times + passive stretch
if articulatory (not MET), then just pulse

spencer technique - flexion
patient on lateral recumbent (on their side)
caudad hand’s palm on spine of scapula + fingers wrap around clavicle
cephalad hand holds patient’s forearm and moves shoulder into flexion
patient resists by extending (moving arm toward the feet)
repeat 3-5 times + passive stretch
if articulatory (not MET), then just pulse

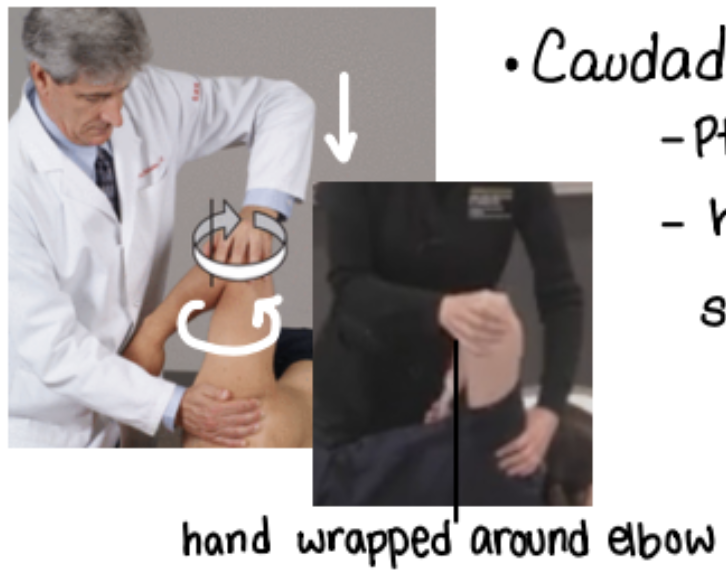
spencer technique - compression w/ circumduction
patient on lateral recumbent (on their side)
abduct patient’s shoulder to 90
cephalad hand holds shoulder
caudad hand on elbow, applying downward pressure, circumducting
spencer technique - traction w/ circumduction
patient on lateral recumbent (on their side)
abduct patient’s shoulder to 90
cephalad hand holds shoulder
caudad hand on wrist, applying traction (upward tension), circumducting
spencer technique - abduct
patient on lateral recumbent (on their side)
patient shoulders abduct (chicken wing) to restrictive barrier
cephalad hand is placed on shoulder
patient grabs physician’s arm (same one that’s holding shoulder)
patient resists by adducting
repeat 3-5 times + passive stretch
if articulatory (not MET), then just pulse
spencer technique - adduct
patient on lateral recumbent (on their side)
patient shoulders adduct (chicken wing) to restrictive barrier
cephalad hand is placed on shoulder
patient grabs physician’s arm (same one that’s holding shoulder)
patient resists by abducting
repeat 3-5 times + passive stretch
if articulatory (not MET), then just pulse

spencer technique - internal rotation
patient on lateral recumbent (on their side)
internally rotate patient’s arm + palms face out + hand placed on back
cephalad hand holds patient’s shoulder
caudal hand is behind patient’s elbow to induce internal rotation
patient resists by externally rotation (pushing elbow backwards)
new barrier is engaged by moving elbow forward
repeat 3-5 times + passive stretch
if articulatory (not MET), then just pulse

spencer technique - pumping
patient on lateral recumbent (on their side)
patient’s hand on physician’s shoulder
both of your hands clasp and “scoop” under head of humerus
pull head of humerus anteriorly (towards you)
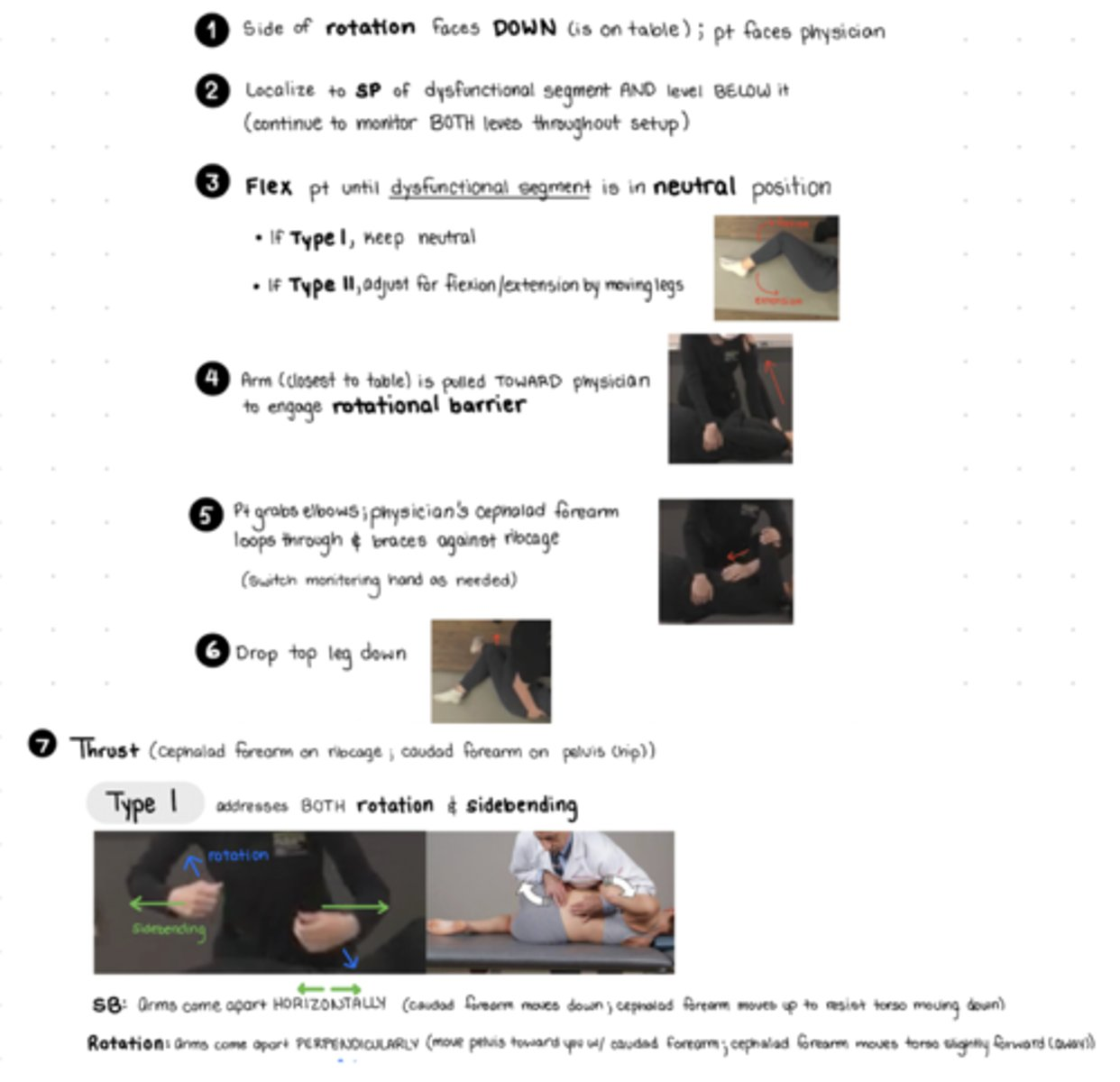
hvla lumbar
side of rotation faces DOWN (on table); pt faces physician
localize SP of dysfunction AND level below (monitor throughout setup)
flex pt until dysfunctional segment is in neutral
if type I = keep neutral
if type 2 = adjust for F/E by moving legs
arm closest to table is pulled TOWARD physician to engage rotation
pt grabs their own elbows; physician’s cephalad forearm loops through and braces ribcage (switch monitoring hand prn)
caudad arm placed on greater trochanter
if type I → keep neutral (no need to adjust)
if type II extension SD → flex legs further until felt at level of dysfunction
if type II flexion SD → tell pt to straighten bottom leg
drop top leg down
THRUST
type 1
arms come APART horizontally (caudad arm moves down; cephalad arm moves up to resist torso moving down)
arms come apart perpendicularly (caudad arm moves pelvis towards you; cephalad arm moves slighly forward/kind of away from you)
type 2
arms come TOGETHER horizontally
arms come apart perpendicularly
like ur punching yourself
hvla thoracic
type 1 SD = neutral, elbow down
type 2 SD = f/e, elbow up
stand on opposite side of rotation
arms opposite over adjacent
thenar eminence on TP, inhale, thrust on exhale
hvla ribs 1, 2 exhalation sd
RaSt
pt seated
physcian leg opposite of SD to stabilize
one hand on pt head, forearm against head to stabilize
mcp of index finger on posterior aspect of dysfunctional rib
thrust directed down and slightly diagonally (as if you were aiming at ur opposite knee)
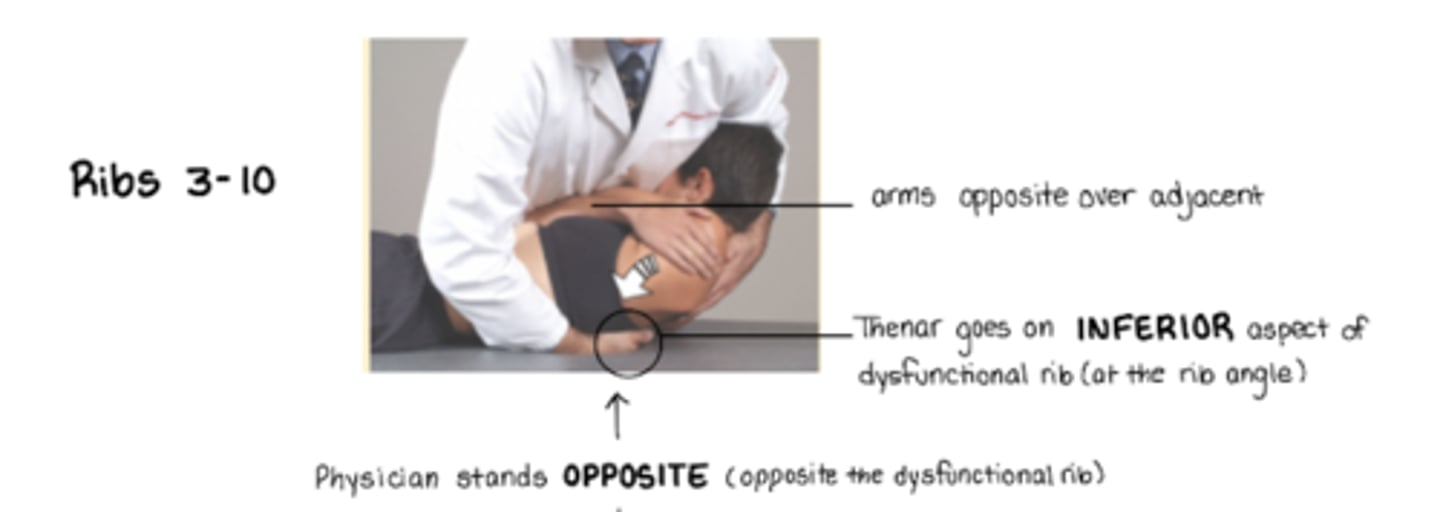
hvla ribs 3-10
pt supine, arms opposite over adjacent
stand on OPPOSITE side of dysfunctional rib
thenar eminence on ___ angle of rib angle to push rib back
inferior aspect of rib angle for exhalation sd → ribs stuck down
superior aspect of rib angle for inhalation sd → ribs stuck up
(basically thoracic HVLA other than hand placement)
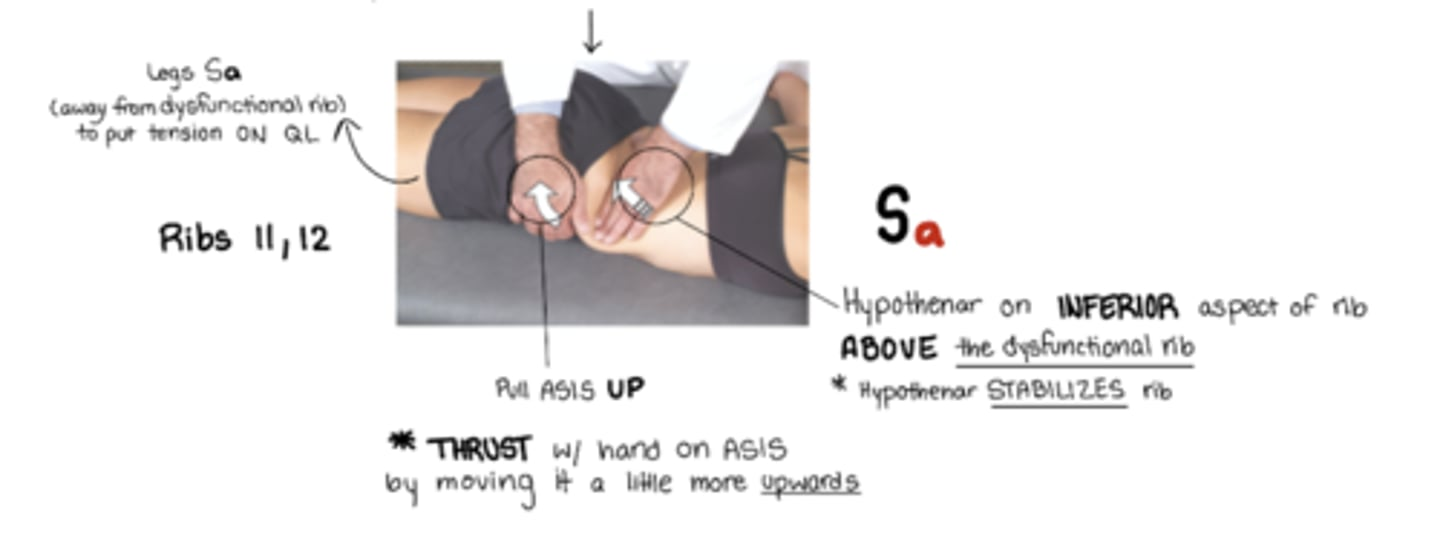
hvla ribs 11, 12 exhalation sd
exhalation sd
Sa = legs away from dysfunctional rib
stand OPPOSITE of dysfunctional rib
active hand: hand pulls UP on ASIS to push rib back down
other hand: hypothenar eminence on inferior aspect of rib ABOVE dysfunctional rib to stabilize rib
ribs stuck UP
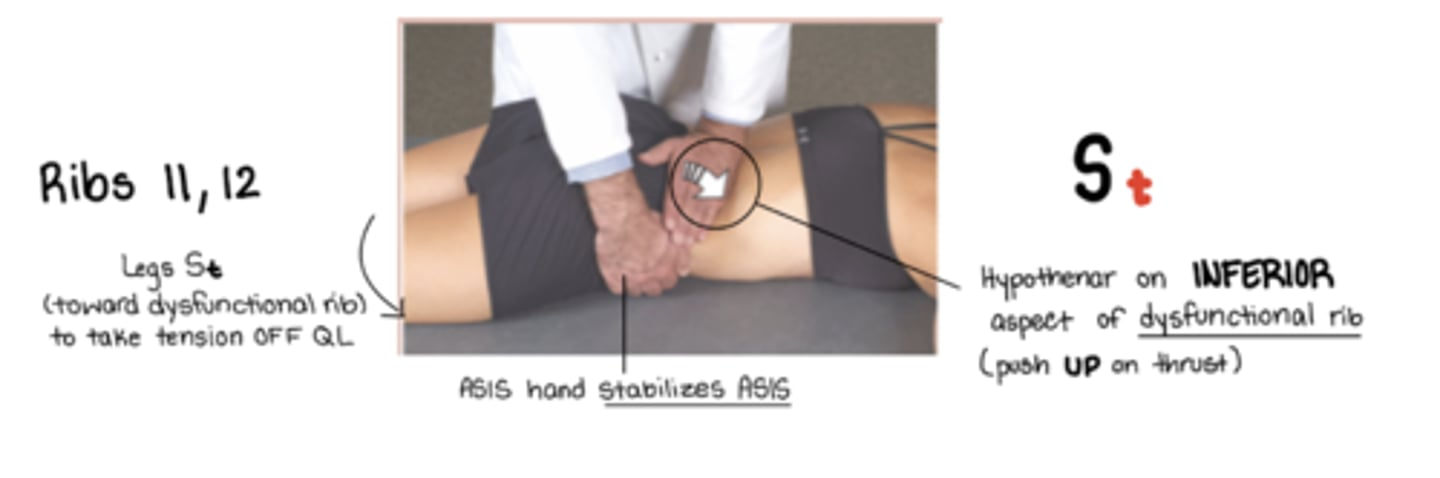
hvla ribs 11, 12 inhalation sd
inhalation sd
St = legs away from me
standing OPPOSITE side of dysfunctional rib
hypothenar eminence on inferior aspect of dysfunctional rib - to push rib back UP
(other hand stabilizes on ASIS)
ribs stuck DOWN
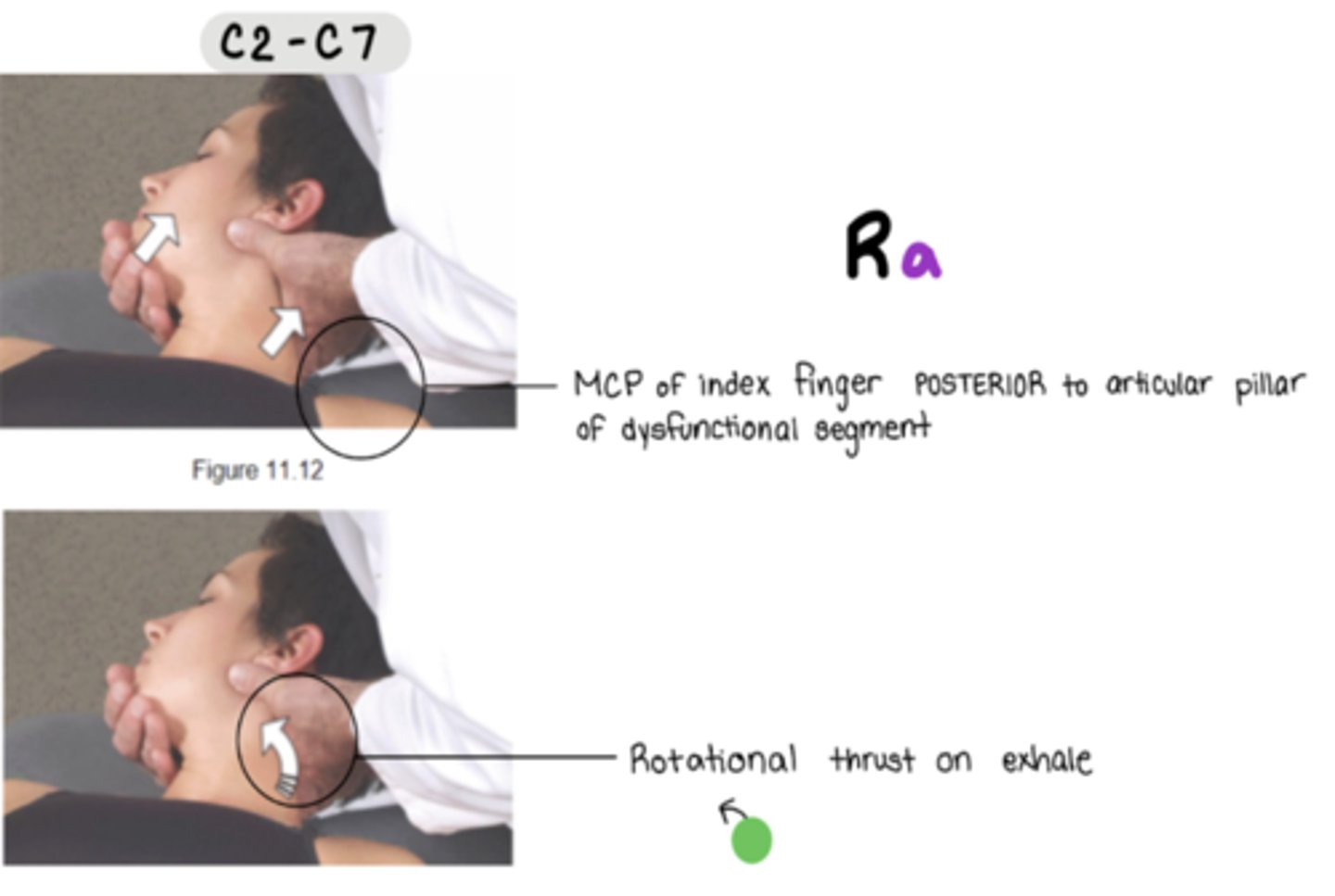
hvla cervical (c2-c7)
stand on SAME side of dysfunctional rotation component
MCP of index finger POSTERIOR to articular pillar of dysfunctional segment
**must lock out
can slightly flex to point and also side bend towards to initiate lockout
cs shoulder - supraspinatus
F Abd ER
Location is in belly of supraspinatus muscle
Pt supine
Physician sits by pt at level of shoulder girdle
Palpate tender point and use other hand to move arm
Flex arm 45 degrees, abduct 45 degrees, externally rotate (like a parade wave or Statue of Liberty)
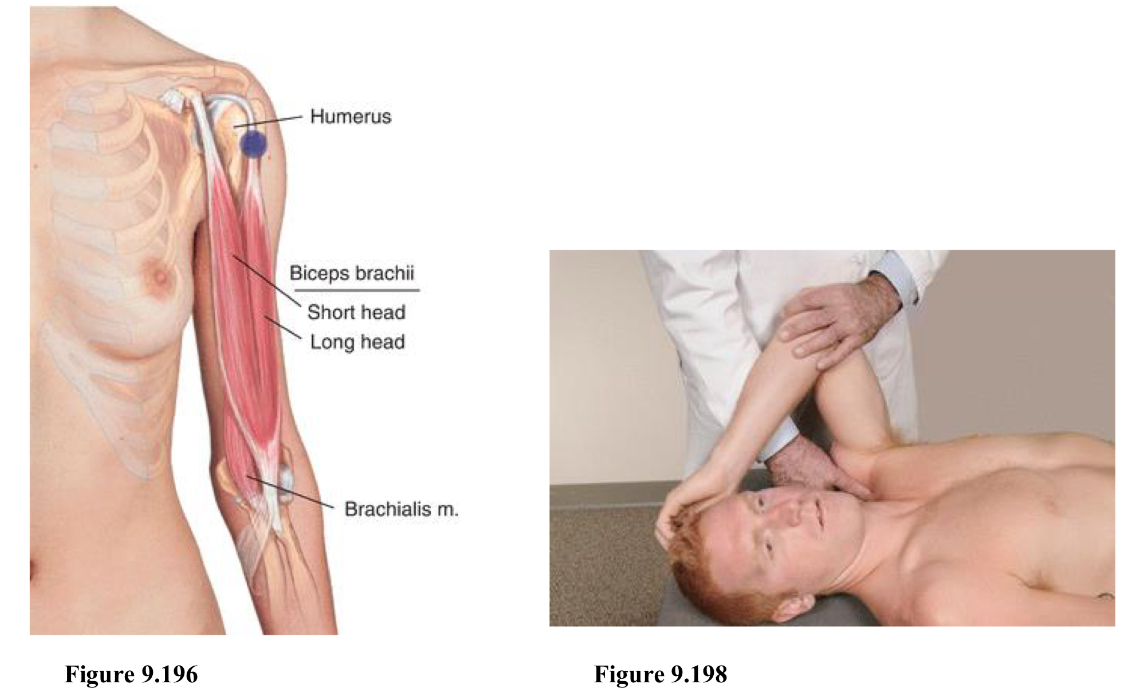
cs shoulder - biceps brachii (long head)
F Abd IR
Location is over the tendon of the biceps muscle in the bicipital groove
Pt supine
Physician sits or stands same side of point
Point is found at the bicipital groove (flex to feel for tendon)
Flex, abduct, and internally rotate (like you’re scratching head)
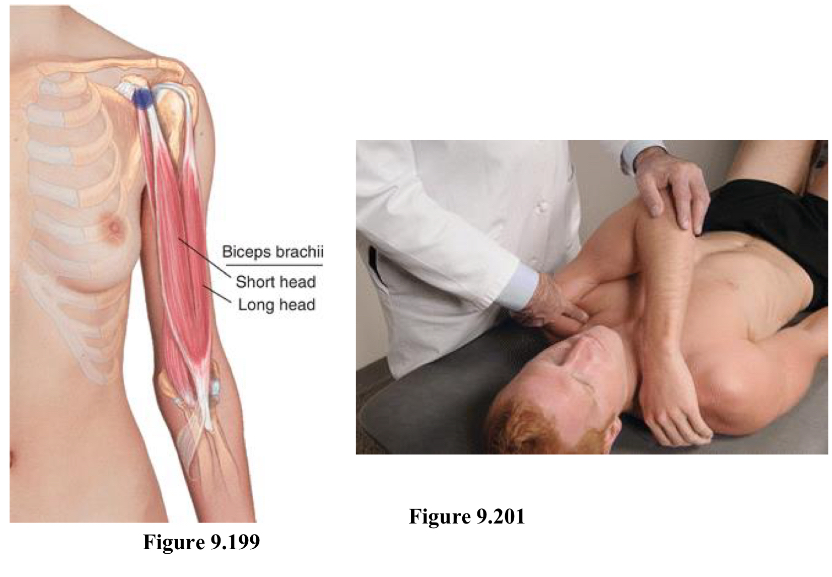
cs shoulder - biceps brachii (short head) / coracobrachialis
F Add IR
Location is at the inferolateral aspect of the coracoid process
Pt supine
Physician can stand from either side
Start at AC joint and follow down until you feel a bony prominence (will need to move through muscle). Then go inferior and lateral of coracoid process to locate point.
Tip - feel for humeral head and point will be slightly medial to that. Or just cup and thumb should feel it.
Shoulder stays on table!!!!
elbow and shoulder are flexed, shoulder minimally adducted and internally rotate (same side arm crosses to grab onto opposite shoulder)
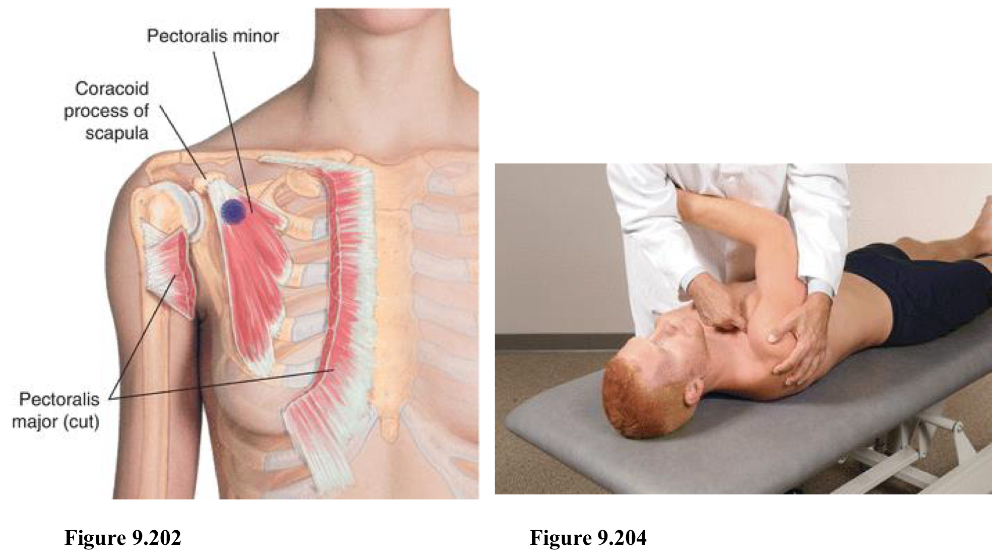
cs shoulder - pec minor
F Add
Location is inferior and medial to the coracoid process
Pt supine
Physician stands opposite of tender point
Point is inferior and medial to coracoid process
Arm is adducted across chest, shoulder/scapula is pulled anterior, inferior, and medial
Shoulder should be OFF table
Can stabilize by holding arm or forearm
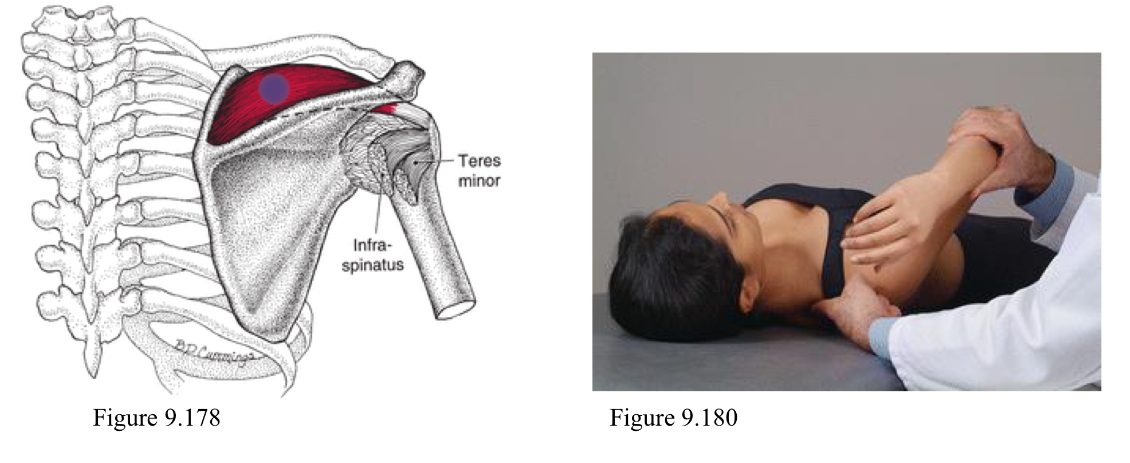
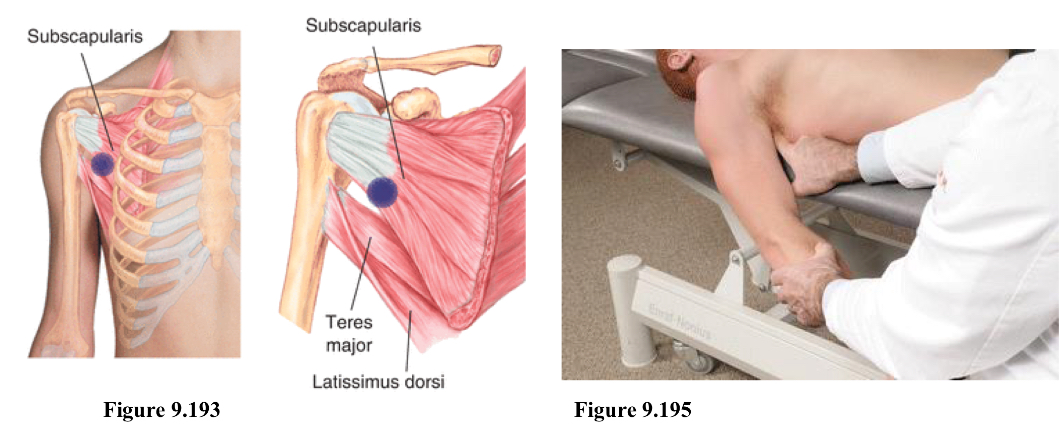
cs shoulder - subscapularis
E IR
Location is at the anterolateral border of the scapula on the subscapularis muscle pressing from an anterior lateral to posteromedial direction
Pt supine
Physician sits or stands on same side
Locate Scapula, follow the lateral border, press deeper as your go superior (must go through muscle layers)
Tender point is on anterior surface of scapula, palpating in a posterior and medial direction. (Deep enough as you should not be able to see your finger tip)
Shoulder is extended and internally rotated
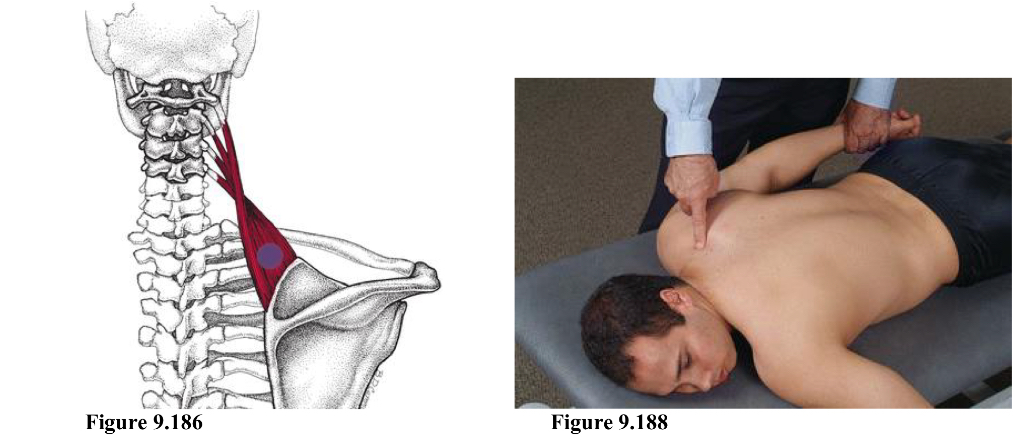
cs shoulder - levator scapulae
IR Abd traction
Location is on the superior medial border of the scapula at the attachment of the levator scapula
Pt prone with head looking away from point and arms at the sides
Physician sits on same side
Find spine of scapula, follow border up, point is superior and medial of the border
Physician caudad hand grabs pt wrist while other hand holds point.
Internally rotate pt shoulder and add mild to moderate traction and minimal abduction
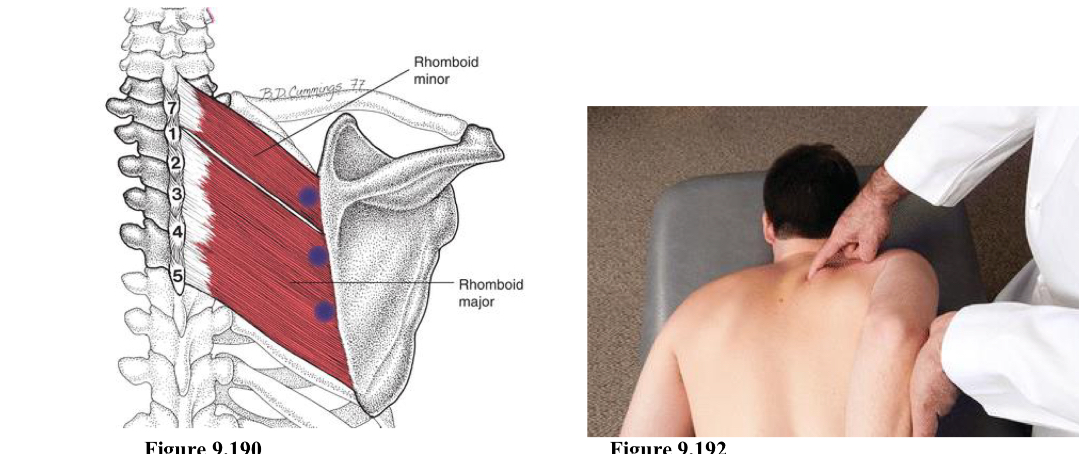
cs shoulder - rhomboid minor/major
E Add
Location is along the medial border of the scapula at the attachment of the rhomboid muscles
Pt prone
Physician stands on either side (Cornick stood on opposite side)
Point is along medial border of scapula. Press medial to lateral. Shoulder be between spine of scapula and angle of scapula.
One hand on point, other hand holds elbow to set into position.
Shoulder is extended and adducted by pulling arm/elbow posterior and medial
Try to have pt hand stay on side and not on their back.
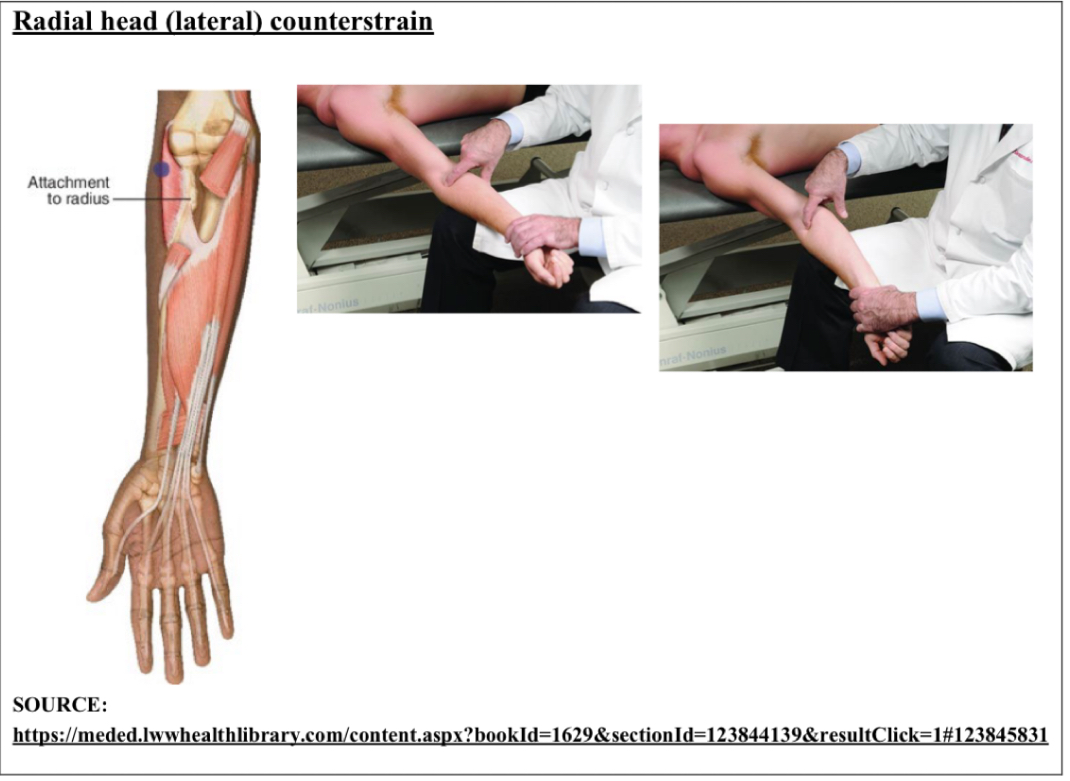
cs radial head
E Sup Val
Point is anterolateral aspect of radial head at attachment of supinator
pt supine, physician same side as point
pt elbow in full extension, forearm supinated
fine tune w/ supination and valgus force
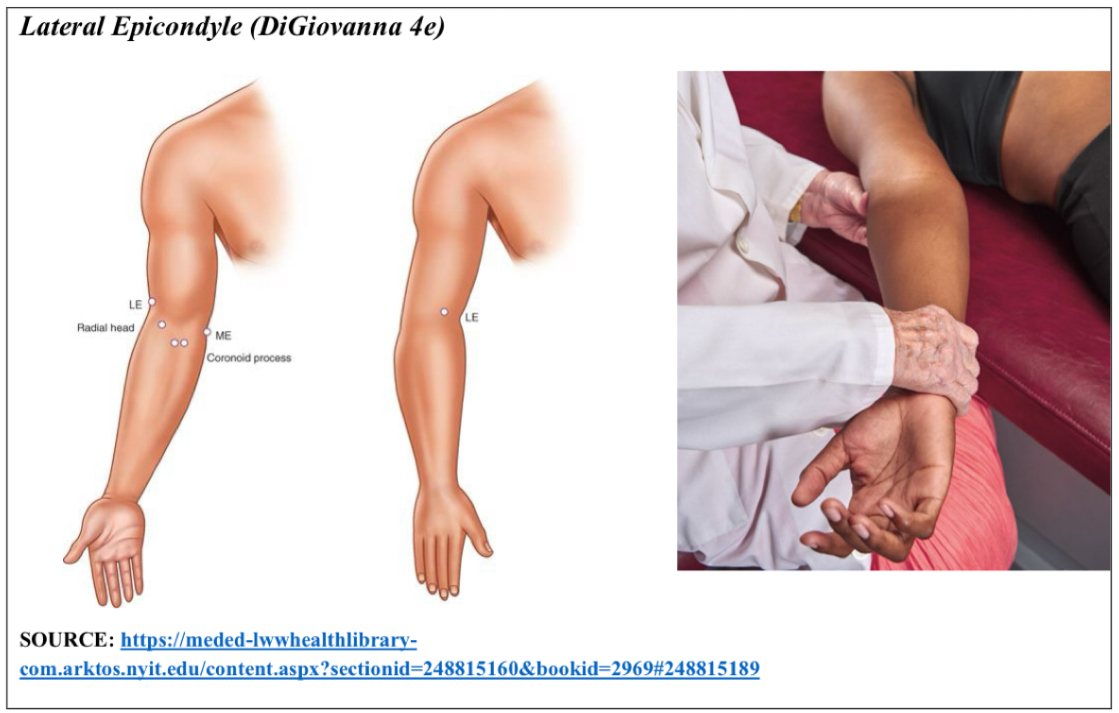
cs lateral epicondyle
E Sup Abd
Point is lateral epicondyle of humerus
pt supine, physician on same side of point
pt elbow fully extended. Use table as fulcrum to put arm into position
arm supinated and abducted with varying amounts of force
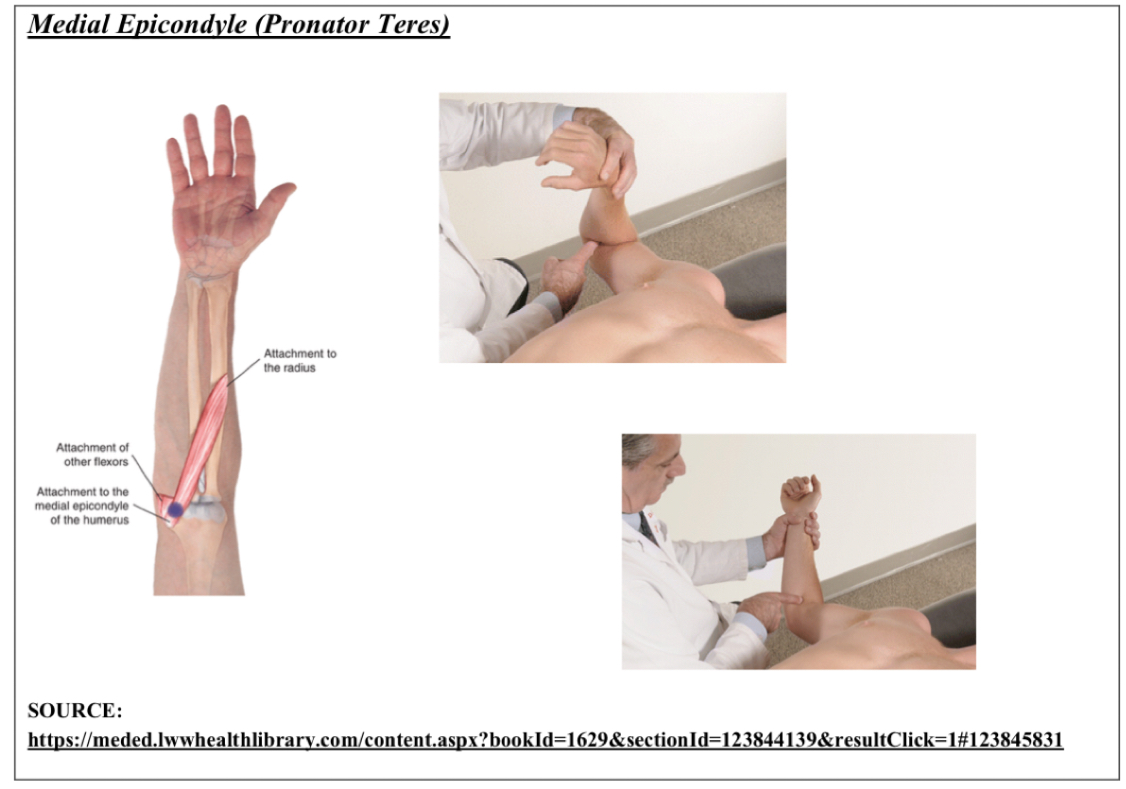
cs medial epicondyle
F Pro ADd with slight flexion of wrist
Point is medial epicondyle of humerus at common flexor tendon and attachment of pronator teres
pt supine, physician on same side of point
pt elbow flexed, wrist pronated, forearm slightly adducted, wrist slightly flexed
fine tune with elbow flex, wrist pronation, forearm adduction
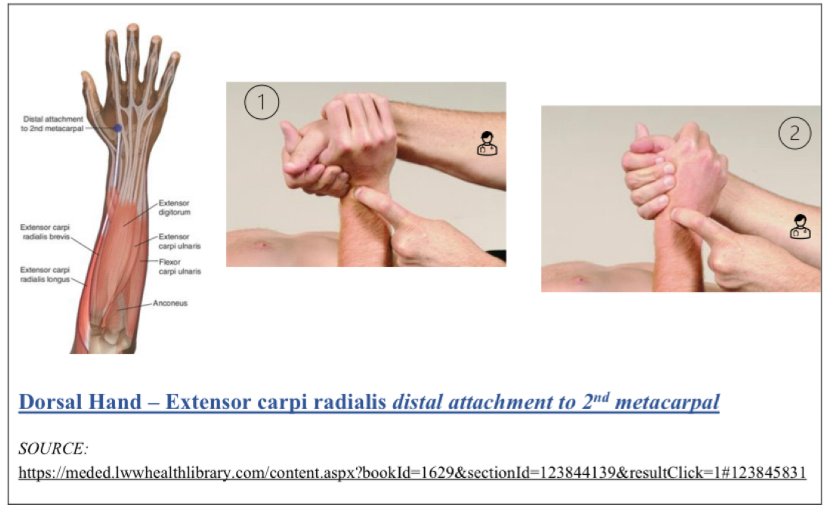
cs extensor carpi radialis (dorsal)
Wrist extension, slight abduction (radial side)
Distal end and Dorsal surface of 2nd metacarpal in extensor carpi radialis
Like if you palpate 2nd MC joint then go down to tendon
pt either seated or supine, physician faces pt
pt wrist extended and abducted (radial deviation)
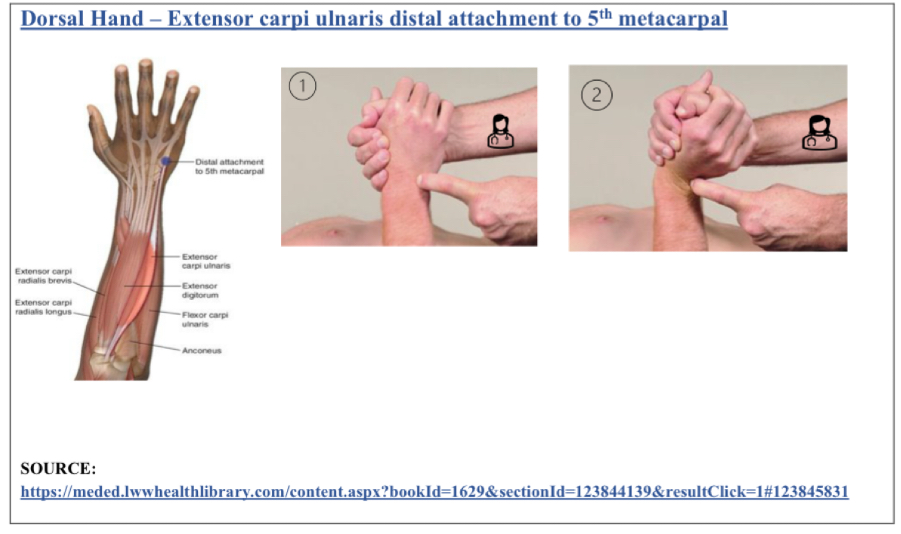
cs extensor carpi ulnaris distal attachment to 5th metacarpal
Wrist extension, slight Add
dorsal surface of 5th MC joint in extensor carpi ulnaris muscle
pt either seated or supine, physician faces pt
pt wrist extended and adducted (ulnar deviation)
cs abductor pollicis brevis
F wrist, ABd thumb
Radial aspect of palmar base at 1 MC joint (abductor pollicis brevis)
pt seated or supine
locate point w/ index finger
pt wrist flexed, thumb abducted

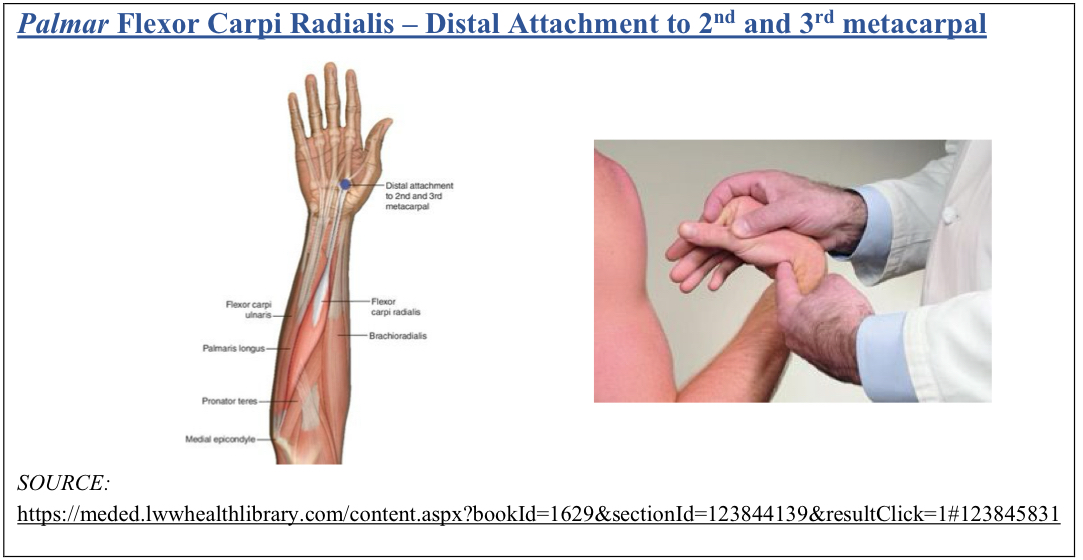
cs flexor carpi radialis
F ABd(radial)
distal attachment to 2nd and 3rd MC joint
pt seated or supine, physician faces pt
pt wrist flexed and abducted (radial deviation)
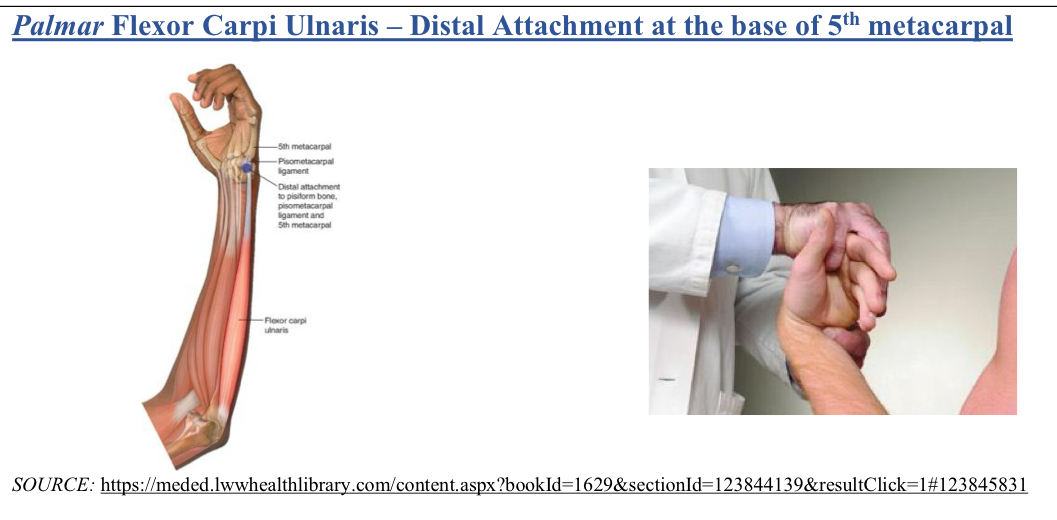
cs flexor carpi ulnaris
F aDd (ulnar)
Located t palmar base of 5th MC in flexor carpi ulnaris
pt seated or supine, physician faces pt
pt wrist flexed and adducted (ulnar deviation)
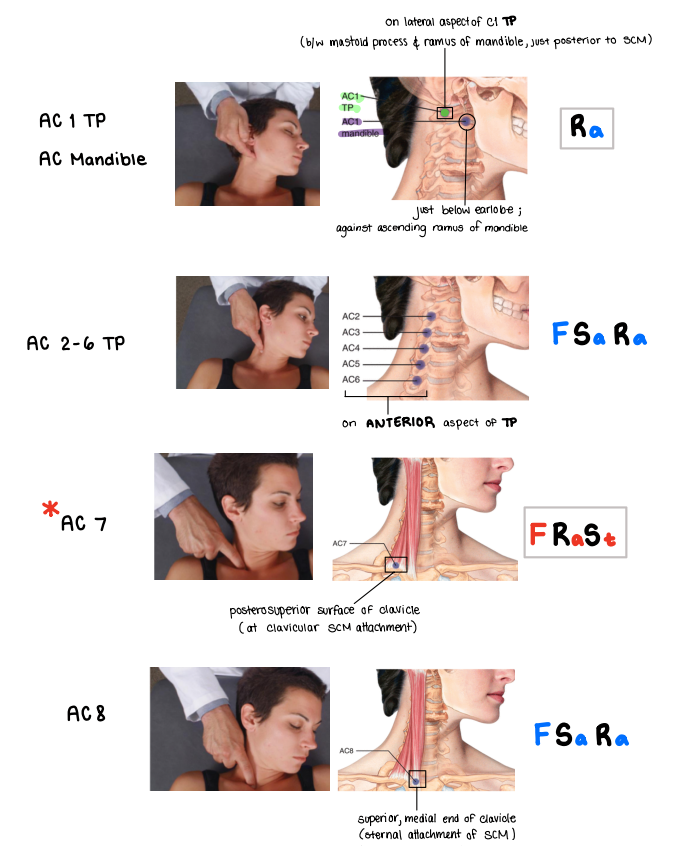
cs anterior cervical
Patient will be supine!
AC1 = Ra (TP or mandible)
AC2-C6 TP = FSaRa (posterior to SCM)
AC7 = FStRa (posterior/superior surface of clavicle)
AC8 = FSara (medial end of clavicle)
cs posterior cervical
Patient will be supine!
PC1 Inion = FStRa (on inferior nuchal line, lateral to inion)
PC1 Occiput = ESaRa (on inferior nuchal line btwn inion and mastoid)
PC2 Occiput = ESaRa (inferior nuchal line within semispinalis capitis m.)
PC2 SP = ESaRa (superior aspect)
PC3 SP = FSaRa (inferior aspect of one above)
PC4-8 SP = ESaRa (inferior aspect of one above)
c3-7 articular = ESaRa (posterolateral aspect)

cs anterior thoracic
Patient is supine for T1-6
T1 = F (episternal notch)
T2 = F (angle of louis)
T3-6 = F to dysfunctional level
Patient is seated for T7-9
FStRa (slouch to F, move leg out to SB pt, pt wraps arms around leg to R)
use the OPPOSITE leg on table
T7 = ¼ from xiphoid process
T8 = halfway xiphoid and umbilicus
T9 = ¼ from umbilicus
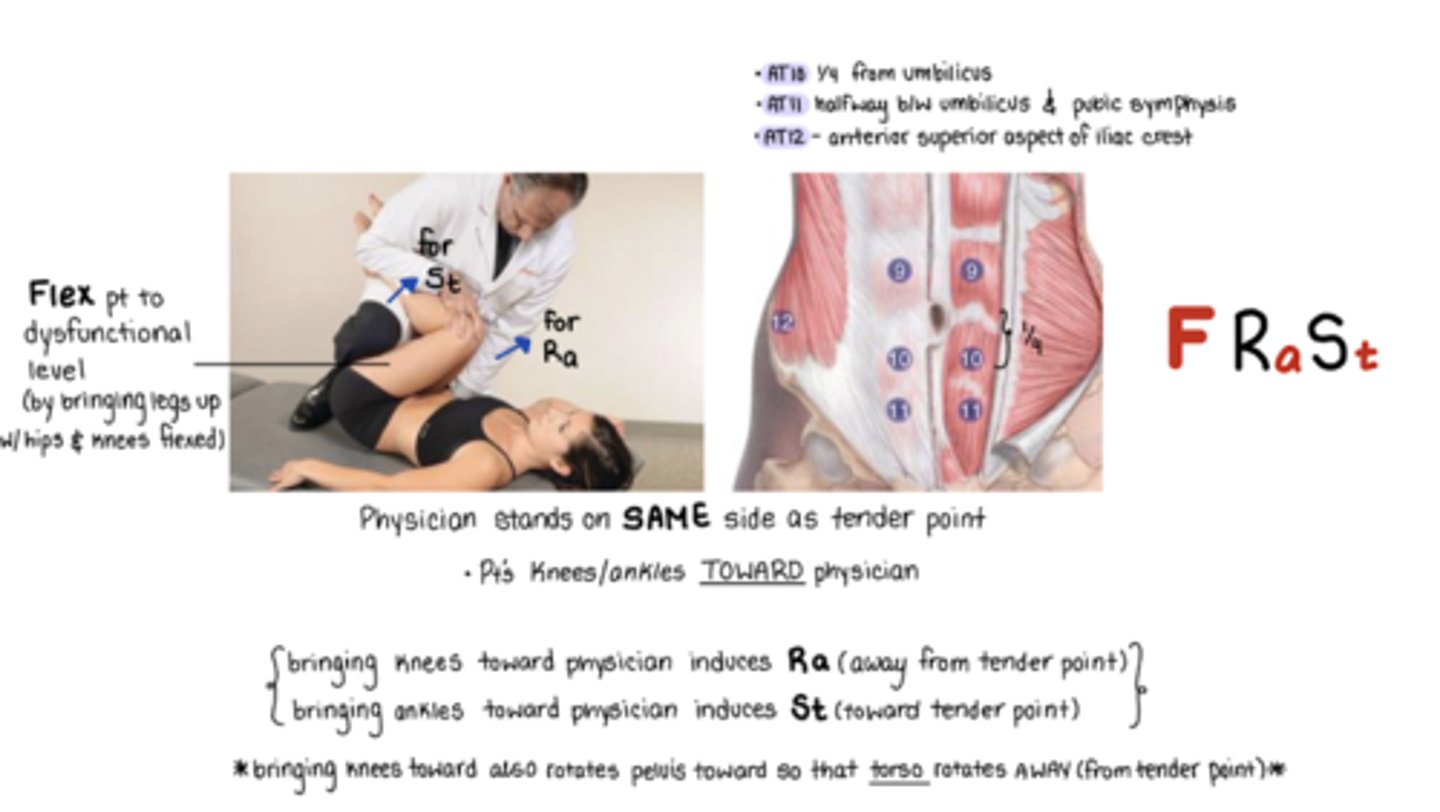
Patient is supine for T10-12
FStRa (stand on same side, flex legs, knees and ankles to me)
T10 = ¼ from umbilicus to pubic symphysis
T11 = halfway umbilicus and pubic symphysis
T12 = anterior superior aspect of iliac crest
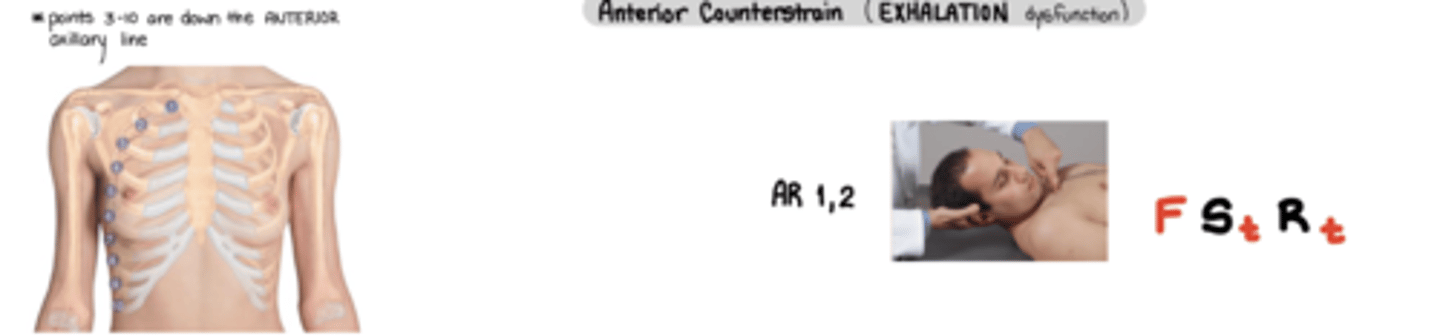
cs anterior rib
anterior = exhalation sd
AR 1,2 = FStRt
AR 3-10 = FStRt
ASS! - anterior same side -> pt mermaid legs same side as TP
Arm back = Rt
Physician moves leg out = St
physician leg on opposite side
cs posterior rib
posterior = inhalation sd
PR 1 = ESaRt
PIE is OP
posterior
I = 1
E = ESaRt
OP = use opposite leg for stabilizing
PR 2-10 = FSaRa
pt mermaid legs opposite of TP
use same side leg
Arm back = Ra
Physician moves leg out = Sa

cs anterior lumbar
1, 5 same side
2, 3, 4 across the floor (opposite side)
AL 1 = FRaSt (medial to ASIS) → knees and ankles to me
AL 2-4 = FSaRt (my little igloo) → knees and ankles to me
AL 2 = medial to AIIS
AL 3 = lateral to AIIS
AL 4 = inferior to AIIS
AL 5 = FSaRa (lateral to pubic symphysis) → knees to me, ankles AWAY

cs posterior lumbar
PL 1-5 SP = ESaRa → EXTEND, ADDUCT, EXTERNALLY ROTATE
stand opposite of TP
IF standing on SAME side → use your knee to help lift leg
hold leg ABOVE knee
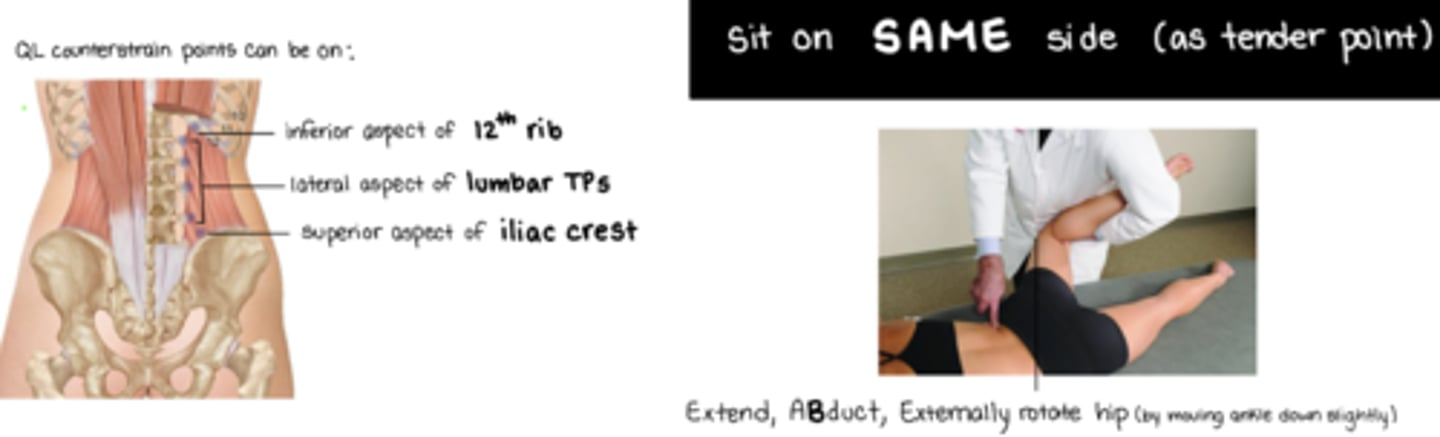
QL = EXTEND, ABDUCT, EXTERNALLY ROTATE HIP
stand on same side of TP
attachments = inferior aspect of 12th rib, lateral aspect of lumbar TPs, superior aspect of iliac crest