OB Cornell Notes Ch 14-16
1/53
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
54 Terms
Prenatal Yoga
Helps relax and manage stress and overall fitness
Gentle stretching and deep breathing
Perineal and Abdominal Exercises
Exercises/Pelvic Floor contractions (kegels)/abdominal muscle contractions
Makes em stronger and more supple for labor
Also pelvic floor ctxns (kegel’s) and abdominal muscle ctxns.

Tailor Sitting
Kinda like butterfly stretch
One leg in front of the other (not cross ankles cus circulation); push knees down
Sit for 15mins a day to allow perineum to become supple

Squatting
Literally just squats
Same idea as tailor sitting
Do it 15mins daily
Useful for second stage labor
Pelvic Rocking
Helps relieve backache during pregnancy early labor by making the lumbar spine more flexible
Done on hands and knees, lying down, or standing

Birth Aids
Activities used for distraction to displace feelings and thoughts around early labor symptoms
Playing cards, listening to specific music

BRADLEY (PARTNER-COACHED) METHOD
Premise: pregnancy is joyful, natural process that partner should play active role in
Reduce pain by abdominal breathing, encouraged to walk, use internal focus point to disassociate
DICK-READ METHOD
Premise: fear -> tension -> pain, therefore prevent fear from occurring by achieving education on childbirth and focus on breathing
PSYCHOSEXUAL METHOD
Premise: extension of Dick-Read; includes conscious relaxation, active calming of mind while discomforted, progressive breathing to flow rather than struggle; embrace them
HYPNOBIRTHING
Help people focus on meditative practices during ctxns so they stay relaxed and free of fear.
LAMAZE PHILOSOPHY (gate control theory)
Premise: gate control theory of pain relief; stimulus response conditioning; use controlled breathing and stimulation (rubbing, massage, heat/cold) to reduce anxiety
Components of labor
The passage (pelvis)
The passenger (fetus)
The powers of labor (uterine contractions)
The psyche (mental state)
The passage (pelvis)
The route a fetus must travel from the uterus through the cervix and vagina to the external perineum.
If disproportion between fetus and pelvis occurs, pelvis structure is at fault
If presenting part is not its narrowest diameter, fetus is at fault
The passenger (fetus)
Body w/ widest diameter is head
4 superior bones: frontal, biparietal, occipital
Fontanels spaces compress during birth to aid in molding; presence can be assessed for fetal position during labor
Biparietal diameter – smallest; anteroposterior diameter when fetus is in full flexion (chin to chest)
Fetal altitude, fetal lie, fetal presentation, and fetal position
Cardinal movement
The powers of labor (uterine contractions)
Effective uterine ctxns have:
rhythmicity
progressive increase in length and intensity
accompanying dilation of the cervix.
The psyche (mental state)
Those who manage best in labor typically have a strong sense of self esteem and a meaningful support person
complete flexion
Optimal fetal attitude; the head flexed forward so much that the chin touches the sternum (vertex). This occupies the smallest space possible.
fetal lie & presentation
Fetal Lie = How the baby is oriented relative to the mother's body (head-to-toe direction)
Longitudinal lie: Baby is aligned head-to-toe with mother (normal, most common)
Cephalic: Head down (vertex presentation) — ideal for vaginal delivery
Breech: Buttocks/feet down
Transverse lie: shoulder down — Baby is sideways across the uterus
fetal position
The relationship of the presenting part to a specific quadrant and side of the pregnant person’s pelvis. In a vertex presentation, the occiput (O) is the chosen point. If the occiput of a fetus points to the left anterior quadrant, the fetal position is LOA the most common fetal position. Fetus in these positions are born the fastest: LOA>ROA
Labor can be extended if the position is posterior (ROP or LOP) and may be more painful because the rotation of the fetal head puts pressure of the sacral nerves.
_OA = good
_OP = pain
Engagement
refers to the settling of the presenting part of a fetus far enough into the pelvis that it rests at the level of the ischial spines the midpoint of the pelvis.
Station
is the relationship of the presenting part of the fetus to the level of the ischial spine.
0 station
when the presenting part is at the level of the ischial spine
-1 to -4 cm
if above the ischial spine
+1 to +4 cm
if presenting below the ischial spines
+3 station
crowning; the presenting part can be seen at vulva
False contractions
Benign and remain irregular |
Felt first abdominally + remain confined to abdomen and groin |
Often disappear with ambulation/sleep |
Do not increase in duration, frequency, or intensity |
Do not add cervical dilation |
True contractions
Begin irregularly but become regular and predictable |
First felt in lower back, sweeps to abdomen |
Continues no matter activity level of PT |
Increases in duration, frequency, and intensity |
Achieve cervical dilation |
First stage of labor
takes abt 12hrs
3 segments: latent, active, transition
Latent: from 0-5cm dilated, contractions mild n last ~30s
Active: 6-7cm, cervical dilation occurs more rapidly, contractions ~60s and q3-5mins
Transition: contractions reach peak intensity 8-10cm dilated, pt in intense discomfort, may have n/v, lose control & modesty, irritable
latent
from 0-5cm dilated, contractions mild & last ~30s
active
6-7cm, cervical dilation occurs more rapidly, contractions ~60s & q3-5mins
transition
contractions reach peak intensity 8-10cm dilated, pt in intense discomfort, may have n/v, lose control & modesty, irritable
Nursing care during 1st stage
Empower birthing parent
Respect contraction time
Promote position changes
Help fetal alignment (squatting or being on all fours may help)
Promote voiding; bladder care, void q2hrs during labor
Second stage of labor
Pushing stage
Full dilation and cervical effacement to birth of infant
Fetal head pushed out of birth canal; extends then rotates to bring shoulders into best line with pelvis
Body of baby then born
Nursing care during 2nd stage
Encourage PT to be in comfy position and breathe any way that is natural
danger of Chorioamnionitis – infection of membrane; increases likelihood of c-section (danger of prolonged second stage)
Baby born; cut cord and clamp
Third stage of labor
Placenta stage
Begins with birth of infant, ends with delivery of placenta, placental separation, and placental expulsion
1-30mins (normal)
Nursing care during stage 3 + 4
If pt uterus has not contracted back to normal, massage fundus to encourage
Oxytocin to help with contraction
If excessive bleeding with poor uterine contractions, administer IM hemabate or methergine (responsibility: no contraindications like HTN or asthma)
Signs of placental separation
Signs placenta has loosened + ready to deliver (think of placenta like a scab)
Lengthening of cord
Sudden gush of blood from vagina
Placenta visible at vaginal opening
Uterus contracts and feels firm again
Maternal Danger signs of labor:
Gestational HTN, >140/90
LBP (+ elevated HR = possible hemorrhage)
Abnormal pulse >100bpm (possible hemorrhage)
Inadequate ctxns: (potential uterine exhaustion)
Prolonged contractions (could compromise fetal well-being because it interferes with adequate uterine artery filling)
Abnormal lower abdominal contour (full bladder you will see bulge, however full bladder may not allow fetal head to descend and bladder may be injured by fetal head; pee q2hrs)
Fetal Danger signs of labor:
High/Low fetal HR (110-160bpm norm)
Meconium staining (stressed baby in womb; indicative of hypoxia; REPORT)
Hyperactivity; frantic movement (sign of hypoxia)
Low O2 sat (<40% needs further assessment)
Auscultation of the fetal heart sounds:
In a vertex presentation, fetus heart sounds are best heard through the fetal back.
In cephalic presentation, they are heard loudest low in the patient’s abdomen.
Assessing FHR involves 3 parameters:
Fetal HR baseline, variability, periodic changes
Fetal HR
110-160bpm
Accelerations
+15bpm for 15s, normal inc from fetal movement, change in maternal position, or analgesic
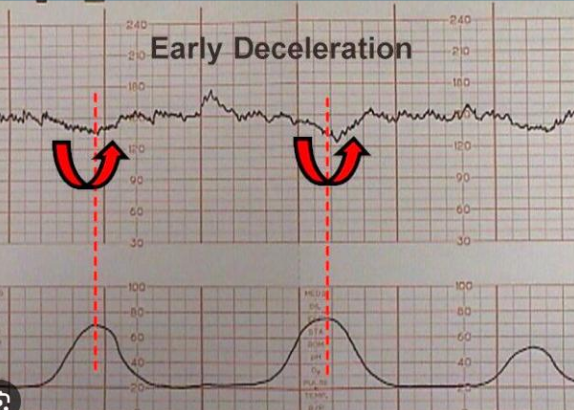
Early decelerations
Normally occur late in labor when fetal head is descended; innocent
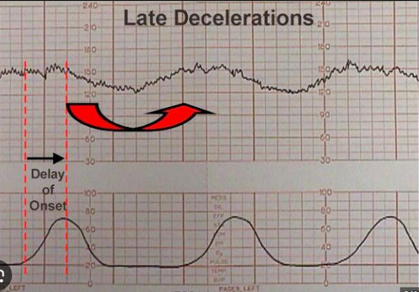
Late decels
onset, nadir, and recovery occur after the beginning, peak and ending of the ctxn, respectively. It suggests utero-placental insufficiency or decreased blood flow to fetus.
Nurse action: immediately change PT position to lateral, O2, IV
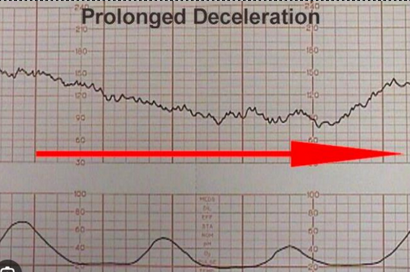
Prolonged decels
sustained drop in HR, may indicate cord compression or maternal HoTN
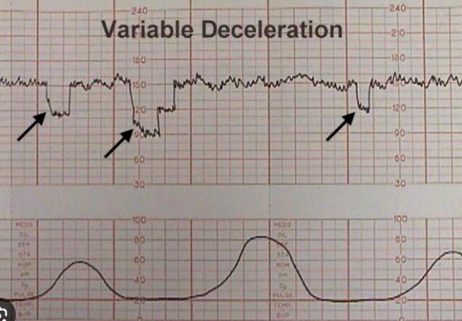
Variable decels
Unpredictable, abrupt drops. May indicate cord compression. Tends to happen after rupture of membranes.
Nurse action: change PT position to lying on lateral. If cord prolapse: O2 and knees to chest position
ACOG FHR categories
Category I (Normal):
Baseline and variability normal
Action: Continue routine monitoring ✓
Category II (Indeterminate):
Some abnormal findings, unclear significance
Action: Keep watching, reassess regularly
Category III (Abnormal):
Clear problems (late decels, absent variability, etc.)
Action: Urgent intervention — change position, O2, IV, stop labor stimulation
If doesn't improve → deliver baby now
In short: I = good, II = watch closely, III = act fast or deliver
Pharmacologic Measures for Pain Relief During Labor
When labor is in the active phase of the first stage, analgesic meds tend to speed up labor. In contrast, in the 2nd stage of labor, epidurals can slow progress and result in more instrumentation or cesarean births.
Opioid (Narcotic) Analgesics
Causes resp depression and fetal CNS depression so timing is important!
Given too early (< 3 cm) will slow labor
Given too close to birth will lethargic sleepy baby
Preferably given when pt is >3hrs from birth so the newborn can breathe easily
Common opioids
Nubian, sublimate, stadol, demerol
narcan should be available to give to the infant at birth PRN
Regional (local) Anesthesia
Benefits:
Completely eliminates pain
Mother awake and aware during birth
Main risk: Hypotension
Treatment: Raise legs, IV fluids, O2
Disadvantage of epidural:
Reduces pushing reflex/effort
Delays fetal descent
Prolongs 2nd stage labor
Increases need for instrument-assisted delivery (forceps/vacuum)
Nursing actions for prolonged 2nd stage labor
change positon (all fours)
let epidural wear off by 2nd stage
oxytocin IV
Aftercare for epidural pt
Position to prevent hypotension:
Lie on side OR
On back with firm towel under left hip
Bladder care:
Epidural numbs sensation → pt can't feel bladder fullness
Nursing action: Remind to void every 2 hours