Unit 4 - Abdominal Vascular Pathology
1/24
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
25 Terms
IVC thrombus
usually occurs from propagation of thrombus from another origin
thrombus propagation from lower limbs = most common
can develop secondary to obstructive processes that reduce IVC flow
sono feats:
distention pre-obstruction and continuous flow (instead of pulsations or respiratory variations)
blockage obstructs any reflections from cardiac contractions or changes w respiration
absence of flow if occluded
presence of material within vein lumen
echogenicity varies w age of clot
iliac vein thrombus:
difficult to diagnose bcuz manual compressions by sonographer aren’t possible at this lvl
so we rely on indirect findings such as: loss of phasicity in the CFV
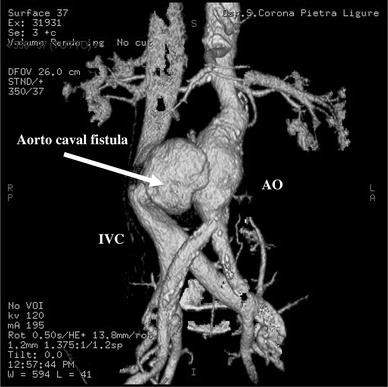
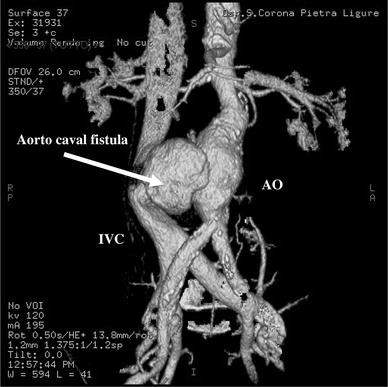
fistulas
aortocaval fistula (aorta to IVC fistula) can occur spontaneously or from trauma
usually a complication of an abdominal aortic aneurysm (AAA)
portocaval fistulas (bw vena cava and portal venous system) may be surgically created to relieve portal HTN
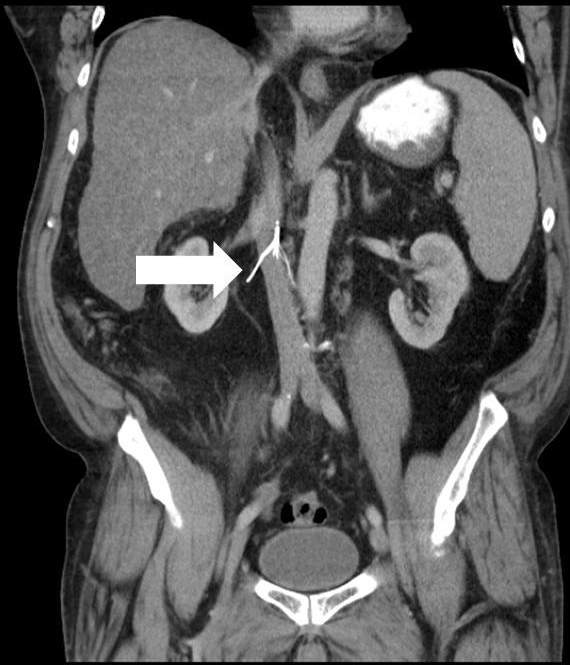
may-thurner syndrome
aka iliac vein compression syndroms (IVCS)
lt. common iliac vein is compressed bw the rt. common iliac artery and the underlying vertebral body
pts. usually present w left iliofemoral DVT or chronic left lower extremity pain & edema
may see loss of phasicity in lower venous sys
neoplastic obstruction
IVC flow obstruction caused by primary tumors that typically propagate from hepatic or renal veins
rare
extrinsic tumors can also cause compression or invasion into IVC (abdo tumors along midline)
sono feats:
visualization of intraluminal tumor
tumor will demonstrate blood flow within, thrombus wont
visualization of extrinsic tumor mass that compresses & obstructs IVC
variable echogenicity
dilation of IVC and tributary veins below lvl of obstruction
continuous flow below the point of obstruction

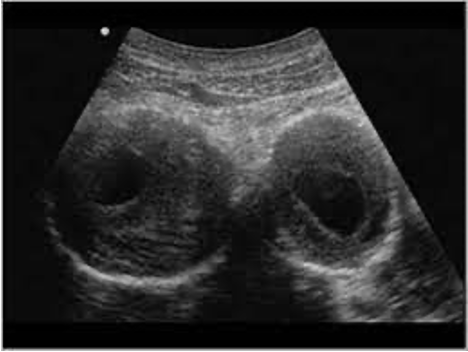
This patient most likely has which of the following pathologies?
may-thurner syndrome
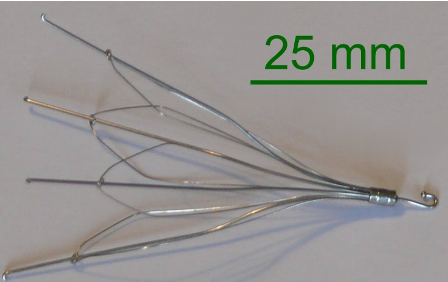
IVC filter
device placed into IVC percutaneously, just below the renal veins, to trap any lower extremity venous thromboemboli before they reach the heart and lungs
percutaneous placement is through common femoral or jugular vein » doesn’t significantly obstruct blood flow
indicated when a pt. has known lower extremity venous thrombosis, or at risk for redeveloping thrombosis, and anticoagulation therapy is contraindicated
most devices consist of thin metal struts joined at one end to form the shape of a cone
sono findings:
should be situated below renal veins
metal struts appear as echogenic lines
should have pulsatile flow in VC above the filter, and phasic flow below
What is the most common pathology affecting the inferior vena cava?
thrombus propagation
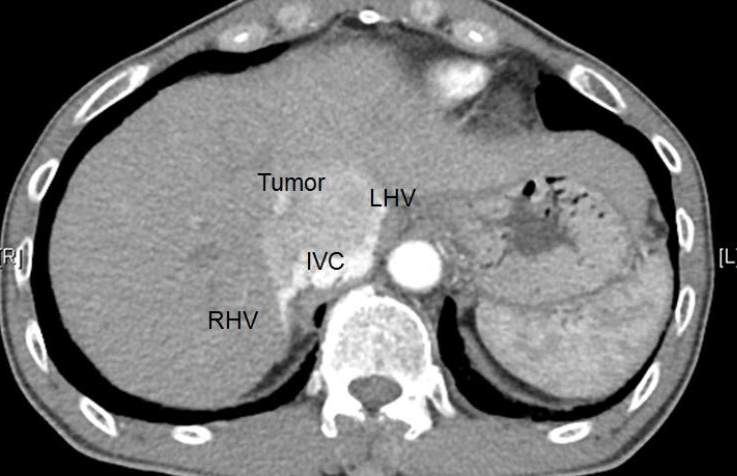
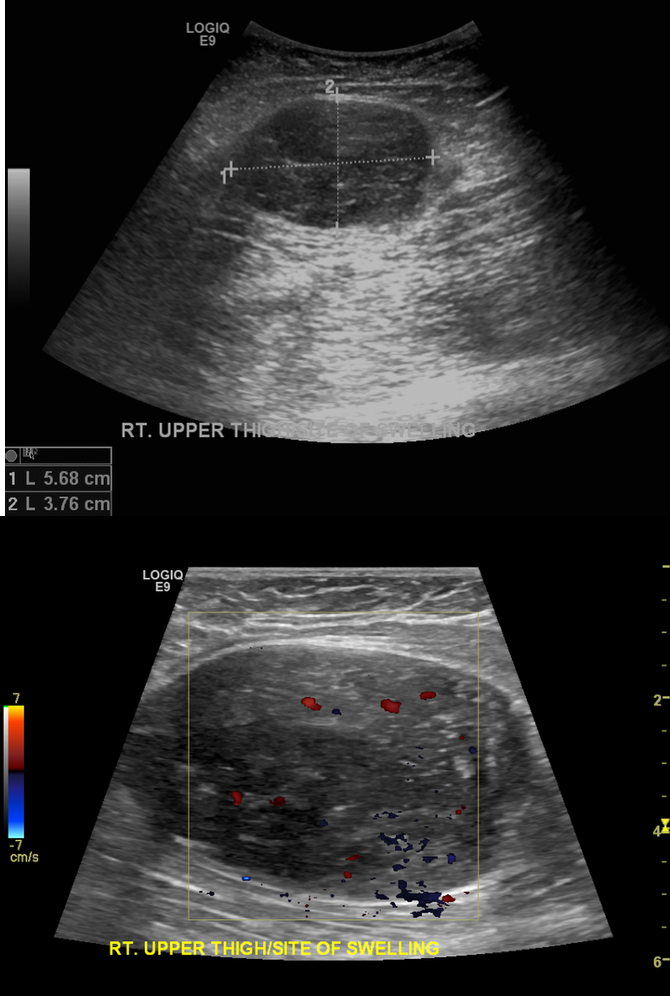
Which of the following matches with the findings below?
neoplastic IVC obstruction
While performing a post-IVC filter sonogram, it is important to _______.
rule out IVC propagation
assess for echogenic material within filter
ensure device tip is below renal veins
What can you conclude from this image of an IVC filter?
there’s IVC perforation from the filter
filter strut extends outside IVC
This image was taken from a patient during a routine IVC filter follow-up ultrasound. What can you conclude? This image was taken from a patient during a routine IVC filter follow-up ultrasound. What can you conclude?
there’s thrombosis within IVC

What is the purpose of the device imaged below?
(This image shows vascular filling through the arteries only.)
offer alternative treatment for when antocoagulant therapy is contraindicated
prevent pulmonary embolism
break up deep venous thrombosis emboli
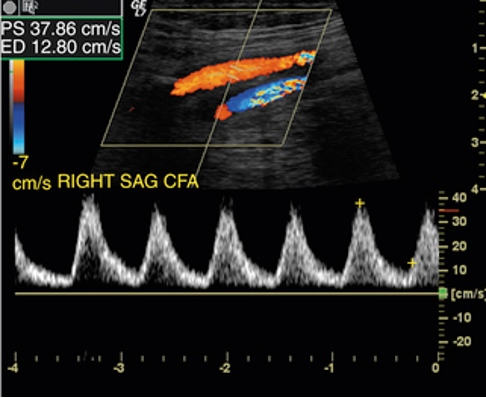
While scanning a patients' left lower leg, you notice the common femoral vein flow is continuous without any respiratory variation. What do you suspect this patient may have?
may-thurner syndrome
Which of the following is associated with extrinsic compression of the inferior vena cava?
neoplasm
atherosclerosis
intimal thickening that causes narrowing and hardening of the arteries » leading to stenosis
common sites for plaque build-up:
near the origin of the renal arteries (infrarenal most common)
bifurcation into common iliac arteries
men>women
inc. chance w age
complications:
aneurysm
emboli
occlusion
direct sono findings:
narrowed luminal diameter or absence of flow
VR > 2.0 = stenosis >50%
post-stenotic turbulence
indirect sono findings:
monophasic CFA spectral tracings (normal CFA tracings are triphasic)
PSV </= 45cm/s

arterial occlusion
can lead to tissue ischemia and gangrene
emboli can cause acute occulision in distal arteries
LeRiche’s Syndrome:
occlusion of the abdo aorta that also involves the iliac bifurcation
collateralization to the leg is through epigastric vessels
may see tardus parvus waveforms in femoral arteries
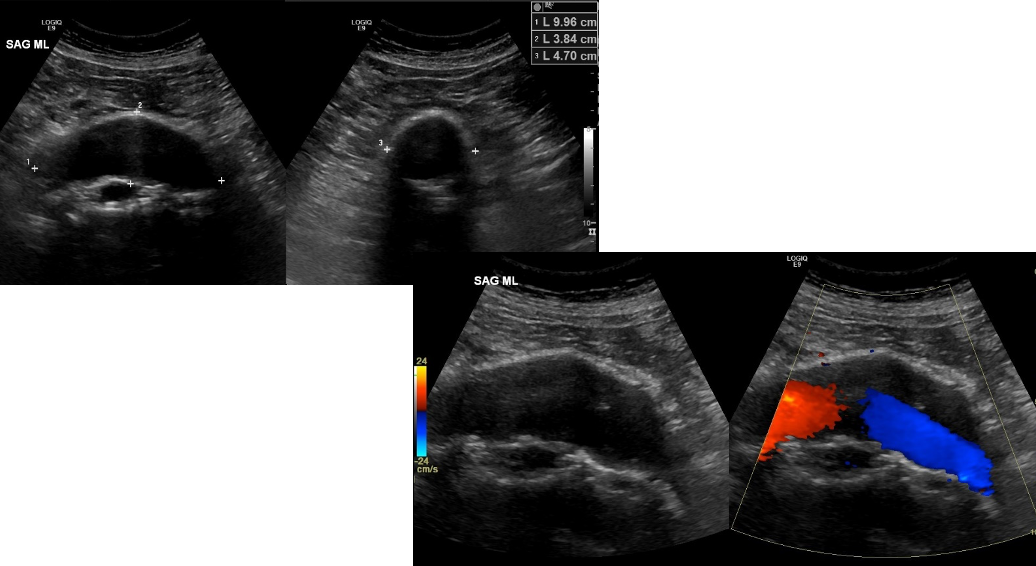
abdominal aortic aneurysm (AAA)
localized weakening and thinning of an arterial wall » causing dilatation of all 3 layers
may rupture into IVC » causinf massive A-V fistula OR rupture into duodenum w upper GI bleeding (RARE)
males>females
most found inferior to renal arteries
commonly associated w:
iliac, femoral, and popliteal aneurysms
ectatic: mild enlargement of aorta
cigarette smoking is a risk factor
parameters:
~1.5x normal caliber (compared to adj. segment) is considered aneurysmal or >/= 2cm (outer-outer wall)
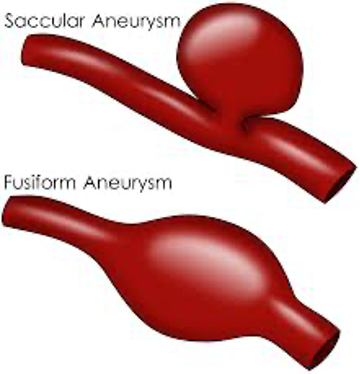
two AAA types:
FUSIFORM
most common
usually infrarenal
all 3 layers bulge out symmetrically
may contain thrombus
SACCULAR
focal outpouching/asymmetric dilatation
rare, least common
assoc. w/ infection
treatment:
recommended once 5-5.5cm diameter reached
treatment is imperative at 6cm » risk for rupture inc.
sono findings:
possibly turbulent color dopp flow within aneurysm
dec. velocities and may show lower resist.
iliac artery aneurysms
often involved w aneurysmal dilatation of the lower abdo aorta
considered aneurysmal when diameter inc. by 50% compared to adj. segment OR >/= 1.5cm
3.5cm = intervention recommended
usually associated w atherosclerotic disease
often found bilaterally
can cause compression on ureters » can lead to hydronephrosis
dissection
abdo aorta dissection is most often from an intimal tear descending from the thoracic aorta
usually stops at an aortic branch origin or at lvl of atherosclerotic plaque
more common in African Americans, Caucasians 2nd
male:female » 3:1
sono findings:
membrane may be seen appearing to divide the artery into 2 compartments » showing diff. flow rates and/or direction in each
visible membrane appears to flutter or move w/ blood flow
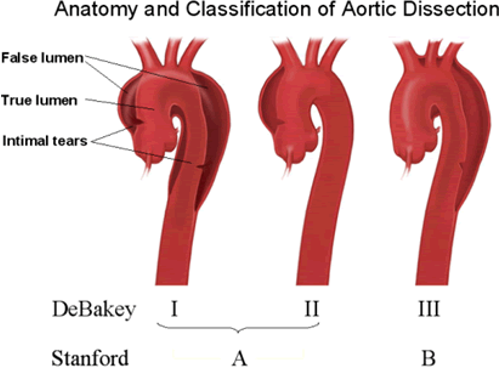
DeBakey classification:
DeBakey I = starts at prox. ao. origin » down to abdo aorta (MOST COMMON)
DeBakey II = starts at prox. ao. origin
DeBakey III = starts post-left SCA (2ND MOST COMMON)
Standord classification:
Stanford A = starts at prox. ao. (MOST COMMON)
Stanford B = starts post-left SCA (2ND MOST COMMON)
pseudoaneurysm (PSA)
usually preceded by arterial cannulation in rt. common femoral artery
often pulsatile, palpable mass
sono findings:
large, hypo mass
connected to artery by tract or neck
high velo. to-and-fro waveform in neck
“ying-yang” flow within mass
occasionally there’s flow disturbance within artery at the site of defect
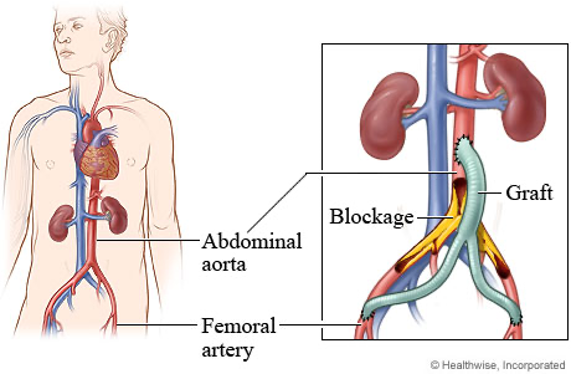
aortic bypass grafts
traditional method of aortic aneurysm repair, but not commonly used anymore
functions for ~10ys+
three types:
simple tube grafts:
limited to aorta only
AAA opened longitudinally » graft places inside » native aorta wrapped around graft
isolates graft » lessening chance of infection
end-to-side
end-to-end
extravascular connections » graft connects prox. and dist. arteries outside vessel lumen
sono assessment post-op:
assess for pathological fluids and PSA formation at anastomotic sites
sono findings:
examine full length of graft & all anastomotic sites
should measure the graft diameter
grafts generally have a textured or tram track appearance
they’re also echogenic
graft velo. compared to baseline study
very high or very low velo. are indicative of stenosis/graft failure
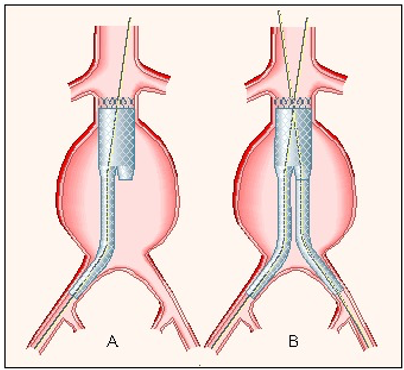
endovascular aortic repair (EVAR)
aka endograft, stent-graft, or transluminally placed endovascular graft
graft placed transluminally through small femoral incisions (via femoral arteriotomy) and deployed remotely
comprised of intravascular metallic stents
fenestrated grafts are for placements that involve overlapping aortic branches
these grafts have strategically placed holes where branch origins would be covered by the graft otherwise
purpose:
exclude aneurysm sac from the effects of blood press. and flow » eliminating risk of rupture
advantages:
less invasive then standard surgical repair
most common types:
bifurcated (most common)
straight tube
uni-iliac
contraindications for EVAR:
aneurysm tortuosity
excessive prox. neck diameter (graft may migrate)
limited prox. neck length
severe iliac artery disease
marked iliac artery tortuisity
vascular complications:
infection, PSA, stenosis, thrombosis, dissection, AVF
possible graft complications:
graft migration, twisting/kinking
incomplete stent deployment, graft “limb” separation, stent fracture
endoleaks:
blood flowing outside of the endovascular graft and into the aortic aneurysm sac
endotension:
inc. in aneurysm size in the absence if endoleak
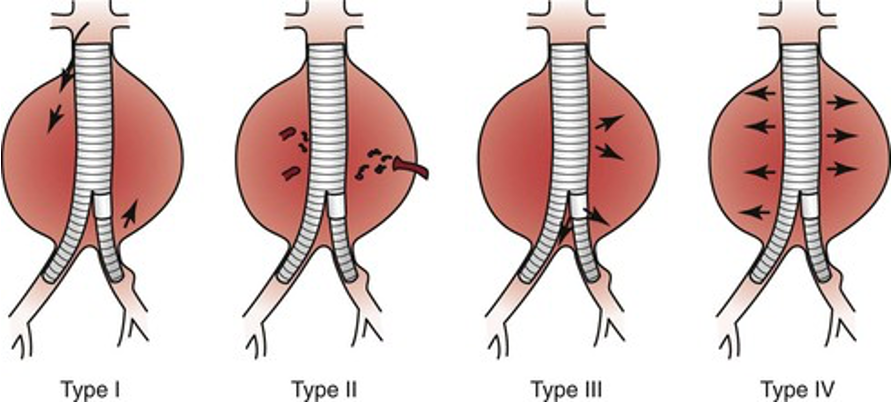
categories of endoleaks
type I - attachment leak
leak is ar prox. or distal end of graft or endograft iliac limbs
color flow shows jet at point of leak
type II - branch leak
retrograde flow from aortic branches into aneurysmal sac
may or may not see inflow from IMA, lumbar, internal iliac arteries, etc.
type III - device related
leaking through the body of the graft, from graft-to-graft connections, or through a graft defect/hole
may or may not be able to identify by u/s
type IV - unidentified site
microleak through graft material (porosity blush)
not seen by u/s
EVAR ultrasound