opthalmic drug delivery
1/12
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
13 Terms
Anatomy of the eye: the cornea as the absorption barrier
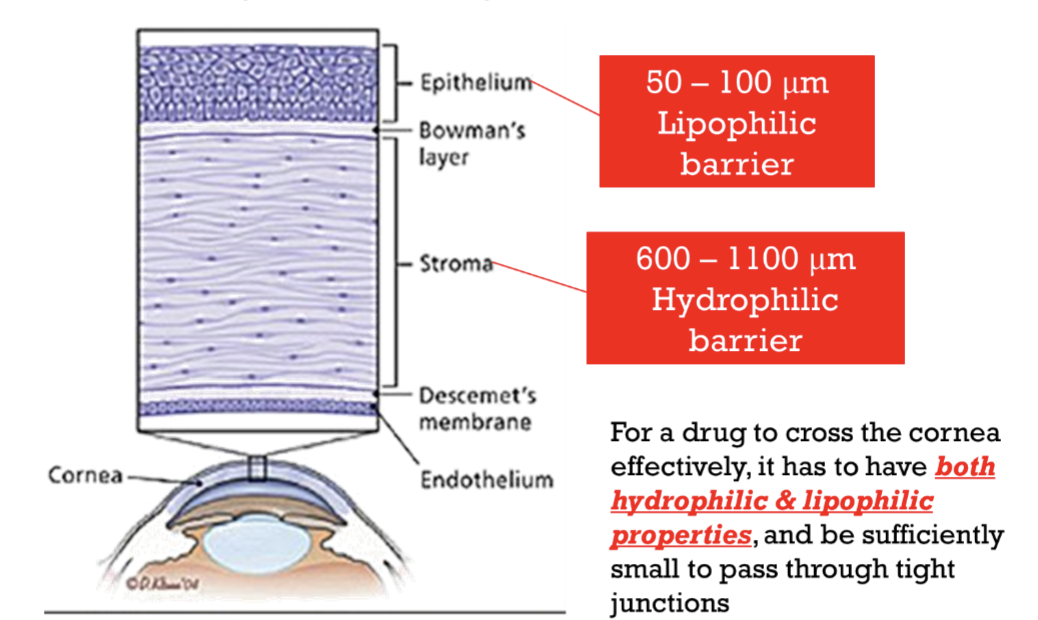
~ 0.5 to 0.7 mm & is composed of five layers
Squamous stratified epithelium
thickness of ~ 50-100 μm & a turnover of about one cell layer/day.
The tight junctions and hydrophobic domains in this layer make it the most important barrier to drug delivery. Lipophilic barrier to hydrophilic drugs
Bowman's membrane
an acellular homogenous sheet of ~ 8-14 μm. Not a barrier
Stroma or substantia propia
~ 90 % of the corneal thickness with 600 -1100 μm thick.
Contains ~ 85% water & is relatively open & will normally allow the diffusion of hydrophilic solutes. Hydrophilic barrier to lipophilic drugs.
Descemet's membrane
~ 6 μm in thickness and is a strong, resistant membrane. Not a barrier.
Endothelium
Maintains normal corneal hydration.
Is in direct contact with the anterior chamber & has a passive influx of water from the aqueous humor towards the stroma.
Thus, a drug must have both hydrophilic and lipophilic properties for passive transcellular transport.
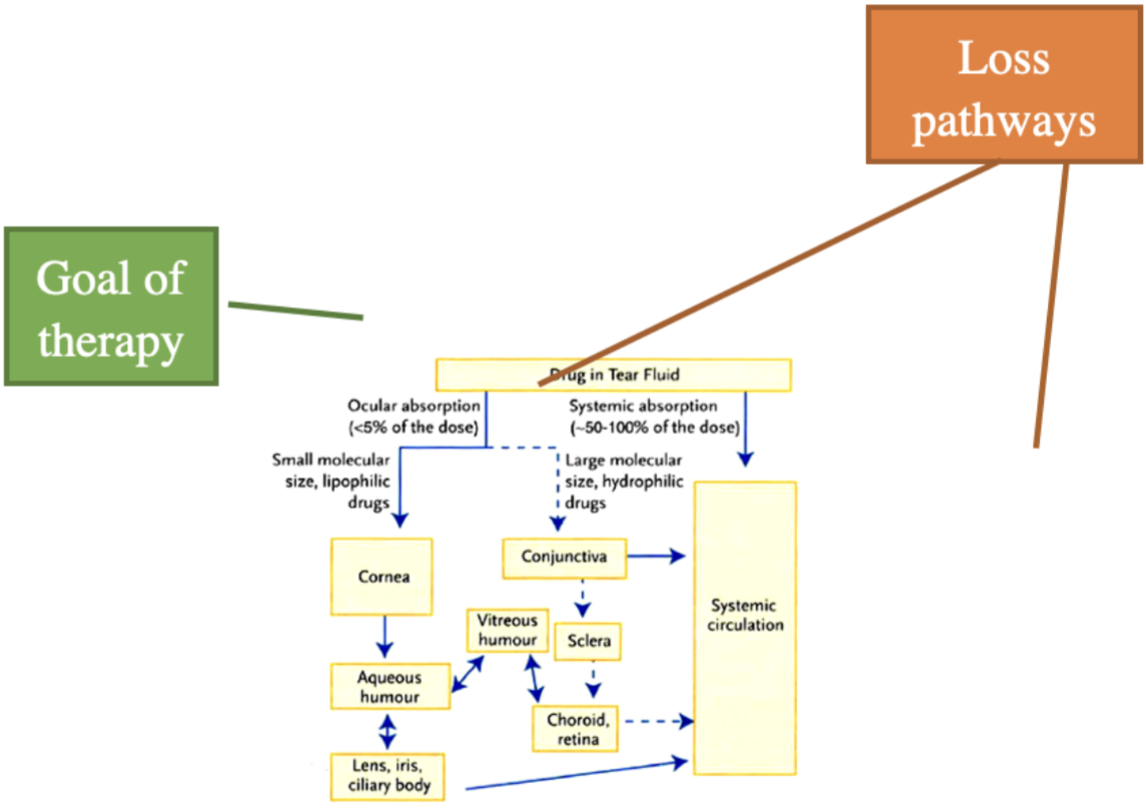
Absorption pathways into the eye
Passive transcellular diffusion via the
Cornea (local action)
Only 5% of administered dose reaches the aqueous humour
Works best with small, lipophilic drugs
Further drug loss can occur through melanin binding or metabolism
perivascular spaces in the conjunctiva or sclera. (systemic absorption/ loss pathway)
Large hydrophilic molecules are quickly absorbed into systemic circulation
Overall ocular bioavailability is very low compared to the dose administered.
Remember goal is local action
Loss due to systemic absorption
Through conjunctival absorption &
Nasolacrimal drainage
~ 90% of the administered dose
Keep in mind the dose administered to the eye is so low that systemic side effects are minimal even if 100% of the dose is absorbed systemically.
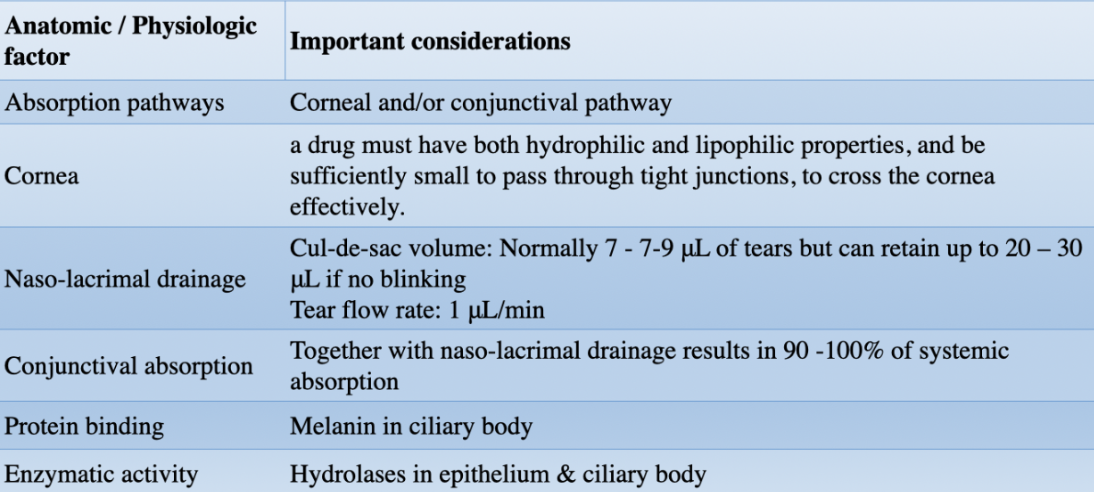
Challenges anatomical and physiological
LO2: analyze the physiochemical characteristics needed for ophthalmic drug delivery.
cornea is the primary barrier to topical delivery to the eye, only small molecules with the appropriate hydrophilic, lipophilic balance are appropriate candidates.
MW: ≤ 500 Da
Log Ko/w: between 1 to 3
Ester prodrugs: can be used, which rely on the metabolic properties of their eye to convert to the active drug.
These prodrugs are usually more lipophilic and therefore have better penetration across the cornea.
LO3:analyze the formulation characteristics needed for ophthalmic drug delivery.
Issues with formulating drugs for the eye
Eye is very sensitive
Easily infected
Easily damaged
Requires sterile and preserved products
Retention of product in the eye is difficult
Low volume of instillation (20-30 uL)
Ideal installation volume to decrease blinking reflex and decrease naso-lacrimal drainage: 7-10 uL
Removal by tears (naso-lacrimal drainage)
Isotonic solutions preferred to reduce loss due to naso-lacrimal drainage
Using viscosity enhancers & mucoadhesives can increase contact time with the eye eg. Cellulose derivatives & polyvinyl alcohol (PVA)
Use non-irritating drugs & excipients
If suspensions are used size of particles < 10 µm
Formulation pH should be between 7 – 7.7
LO3
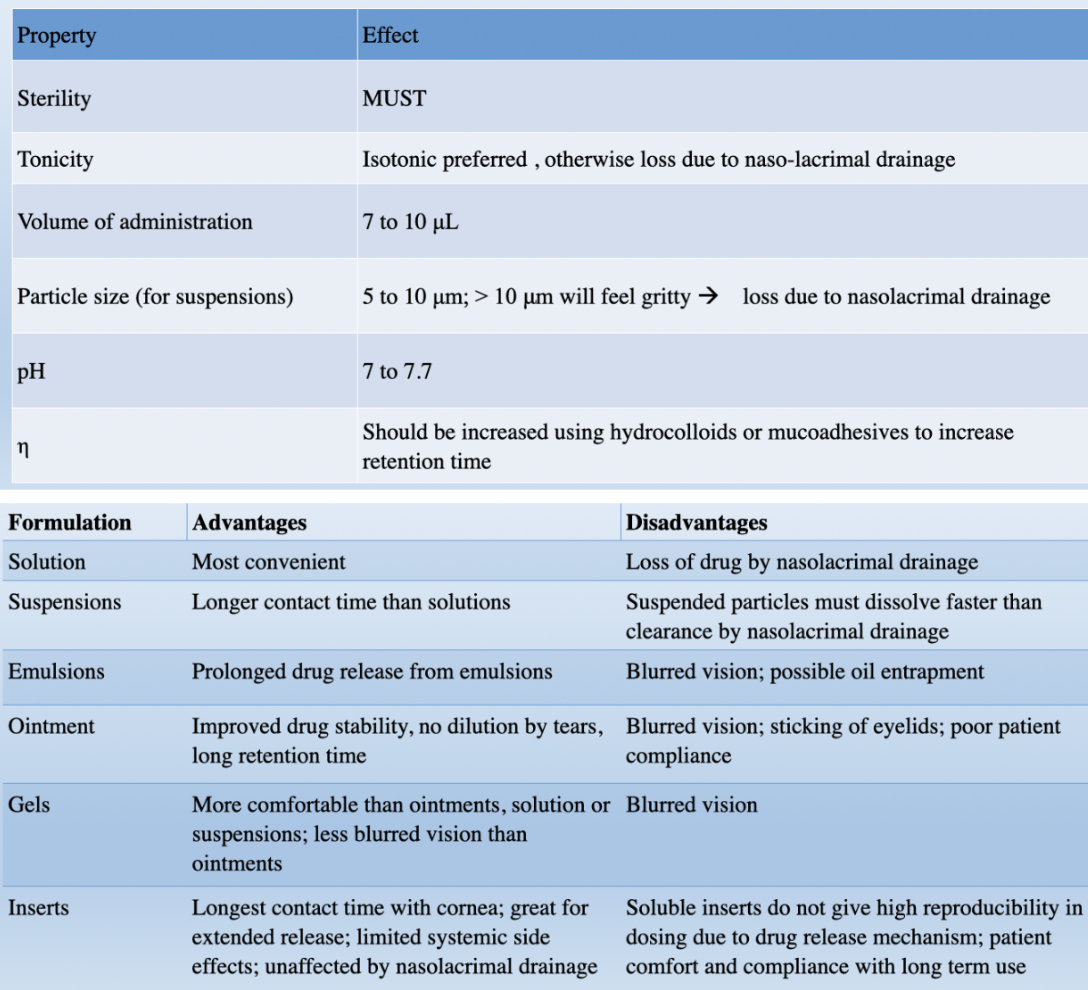
Solutions
Most common and inexpensive
Most convenient in terms of usage
Available as multidose or unit dose
Multidose MUST have preservative
Typical formulation
Drug
Viscosity enhancers to ↑ contact time
Tonicity agents to ↓ nasolacrimal drainage
Buffering agents to ↓ nasolacrimal drainage
Surfactants or co-solvents to enhance solubility
Preservative
Vehicle
Eg. Betimol

Timalol maleate ophthalmic solution
Reduces intraocular pressure
Formulation
Drug:Timalol maleate @ 0.25 % or 0.5 %
Buffer: Sodium Phosphate
Preservative: Benzalkonium chloride
pH = 7.0
274 – 328 mOsm
Emulsions
Limited products available due to stability issues
Available as multidose or unit dose
Multidose must have preservative
Typical formulation
Drug
Viscosity enhancers to ↑ contact time
Tonicity agents to ↓ nasolacrimal drainage
Buffering agents to ↓ nasolacrimal drainage
Surfactants to stabilize the interface
Oil
Water
Preservative
Vehicle
Eg. Restasis

Cyclosporine A 0.05% ophthalmic emulsion
Increase tear production
Formulation
Drug: Cyclosporine A 0.05%
Oil phase: glycerin & castor oil
Surfactant: Polysorbate 80
Viscosity enhancer: Carbomer copolymer type A
Water phase: Purified water
pH adjuster: NaOH
pH = 6.5 – 8.0
230-320 mOsm
Appearance: white opaque to slightly translucent homogeneous emulsion
only FDA-approved, preservative-free medication in a bottle
Suspensions
More common than emulsions
Particle size <10 um to reduce the feeling grittiness in the eye
Longer contact time than solutions as the particle adhere to the conjunctiva
The rate of particle dissolution must be faster than the naso-lacrimal drainage to have ocular bioavailability
Usually used to admin steroids
Available as multidose or unit dose
Multidose must have preservatives
Typical formulation
Drug
Viscosity enhancers to ↑ contact time
Tonicity agents to ↓ nasolacrimal drainage
Buffering agents to ↓ nasolacrimal drainage
Suspending agents
Preservative
Vehicle
Eg. Blephamide Ophthalmic Suspension

Ointments
Formulated only with oleogenous or absorption bases only as they are the least irritating
The drug is either dissolved or suspended in the base
Ointments have better ocular bioavailability than liquid products due to longer contact time with the eye & because they do not get diluted with tears.
Drawbacks include blurred vision & difficulty in dosing.
Typical formulation
Drug
Base
Preservative
Levigating agent / wetting agent
Eg. Blephamide Opthalmic ointment
Sulfacetamide sodium 10%, prednisolone acetate (microfine suspension) 0.2%
For eye infections
Formulation:
Drugs sulfacetamine sodium 10% & prednisolone acetate 0.2%
Preservative: Phenylmercuric acetate 0.0008%
Wetting agent: Mineral oil
Base: Petrolatum, Lanolin alcohol & White petrolatum
Aqueous Gels
more acceptable than ointments to patients because of ease of use and “feel” issues.
Two types of gels:
formulated like a gel and are used like ointments
Formulated as sol-gels – solution in bottle, gel in the eye due to change in pH or other physiological
Like ointments, sol-gels also cause blurred vision, but unlike ointments can be dosed more accurately.
Like ointments, all gels have long retention times and therefore higher ocular bioavailability than liquid dosage forms
Typical formulation
Drug
Gelling agent
Tonicity agents to ↓ nasolacrimal drainage
Buffering agents to ↓ nasolacrimal drainage
Surfactants or co-solvents to enhance solubility
Preservative
Vehicle
Eg. Timoptic XE Ophthalmic gel formation solution

Timalol maleate @ 0.25 or 0.5 %
For eye infections
Formulation:
Drug: Timalol maleate @ 0.25 % or 0.5%
Preservative: benzododecinium bromide 0.012%.
Tonicity agent: Mannitol
pH: 7.0
Osmolarity: 260-330 mOsm
Vehicle: Water for injection
Tromethamine: alkalizing agent
GELRITE Gellan gum: The gel forming solution contains a purified anionic heteropolysaccharide derived from gellan gum. An aqueous solution of gellan gum, in the presence of a cation, has the ability to gel. Upon contact with the precorneal tear film, TIMOPTIC-XE forms a gel that is subsequently removed by the flow of tears.
Inserts
most accurate of all the topically administered dosage forms
Least systemic side effects
Unaffected by tear flow or nasolacrimal drainage and have extended contact times.
The inserts are of 2 varieties
non-degradable
Soluble inserts are not as reproducible in dosing as drug release mechanisms are dependent on both drug diffusion and insert dissolution.
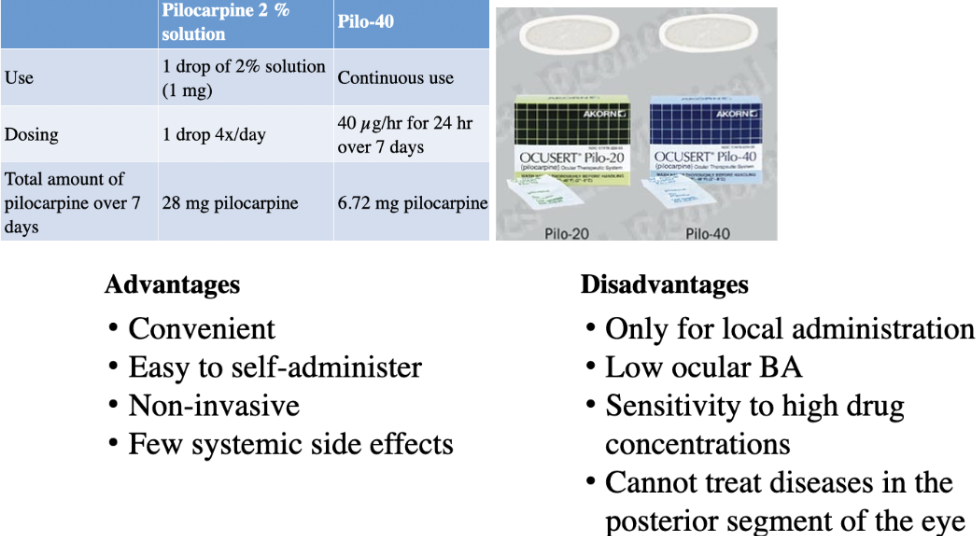
Eg. Ocusert
Pilocarpine @ 20or 40 ug/hr
For reducing intraocular pressure
Formulation:
Drug: Pilocarpine released at 20 or 40 µg/hr
Continuously releases pilocarpine over 7 days
Insoluble ocular insert
Carrier material: Alginic acid
Rate controller: ethylene vinyl acetate copolymer
Annular ring contains titanium dioxide for visibility
First few hours (~ 5 hours) release rate is 3X labeled release rate (burst effect)
Labeled release rate achieved in ~ 6hr
Maximum ocular hypotensive effect in 1 – 2 hr
more on insert
Use of Ocusert
Lower conjunctival cul-de-sac
At bedtime to counteract Pilocarpine-induced myopia
Manipulate from lower to upper cul-de-sac
Before sleep for best retention
Gentle digital massage through lid
Or if retention problems during daytime
Check for presence of OCUSERT®
Before retiring at night
Upon arising
Comparison over 1 week of Pilocarpine 2% ophthalmic solution vs Ocusert® Pilo-40