Radiology II Final- Combined
1/269
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
270 Terms
radiation categories
electromagnetic radiation
ER- wave and quantum theory
ER spectrum
ionization
effects of ionizing radiation on biology
key target of radiation-induced damage
-DNA
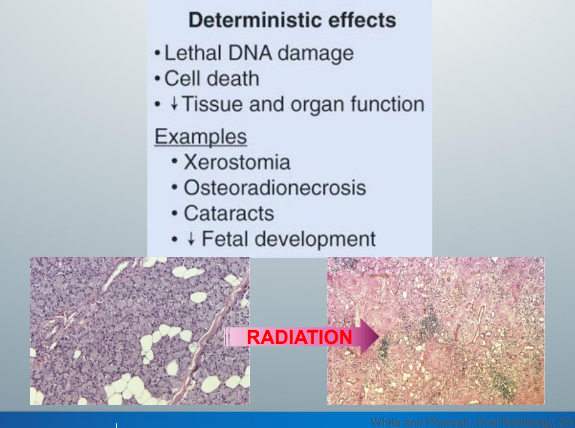
deterministic effects
oral complications post-radiotherapy
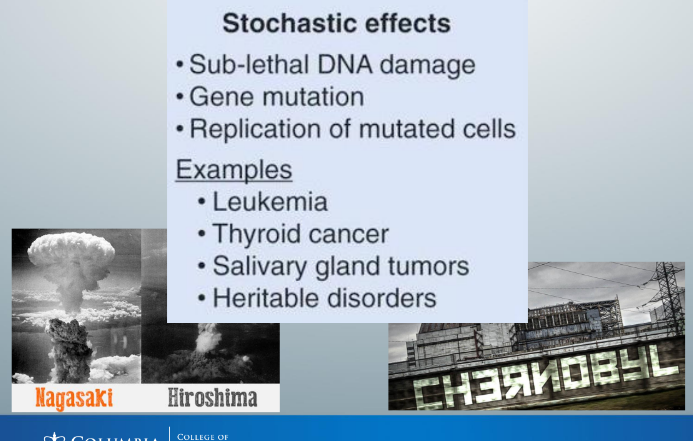
stochastic effects
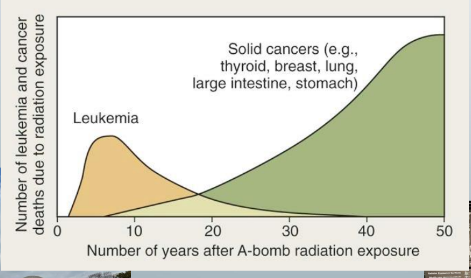
incidence of radiation-induced leukemia and solid cancers
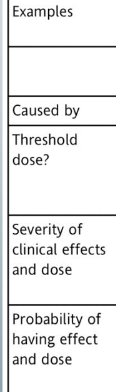
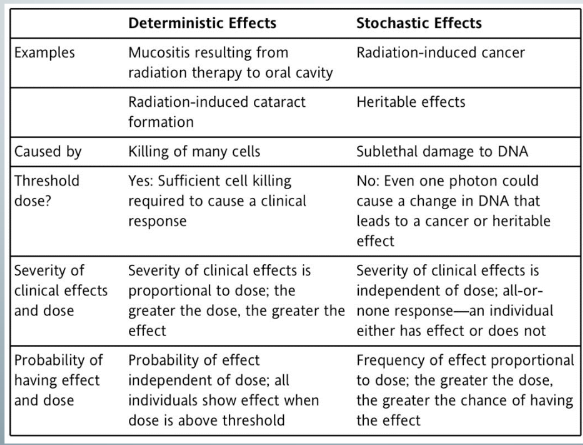
deterministic v. stochastic effects
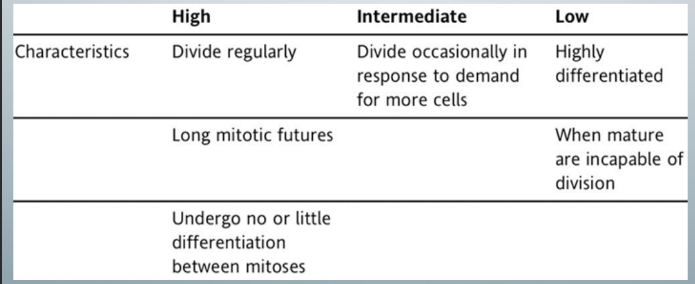
radiosensitivity of cells
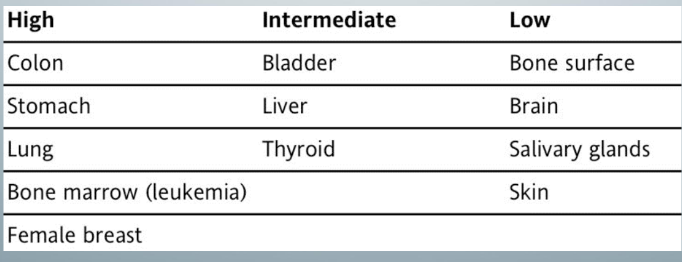
susceptibility of different organs to radiation-induced cancer
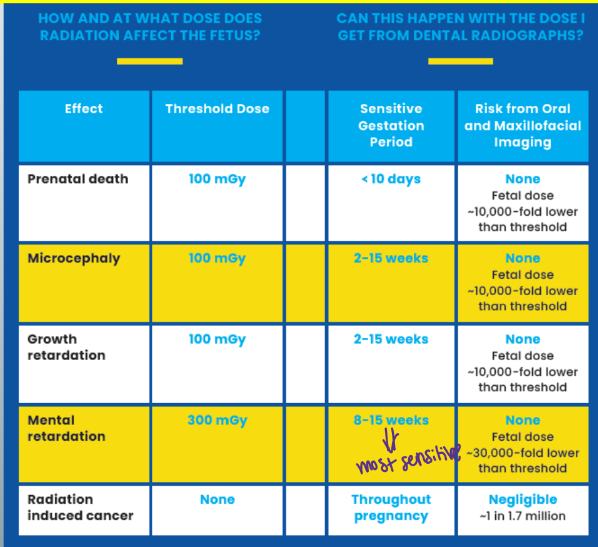
radiation effects on the embryo and fetus
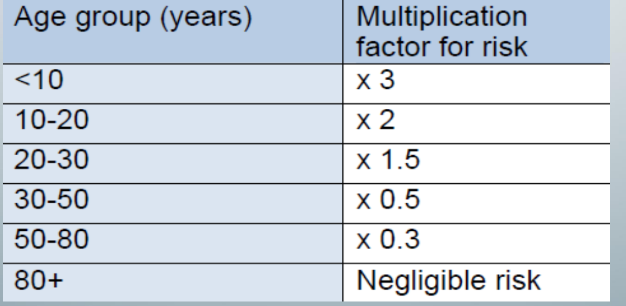
age group, multiplication factor for radiation risk
background of radiation
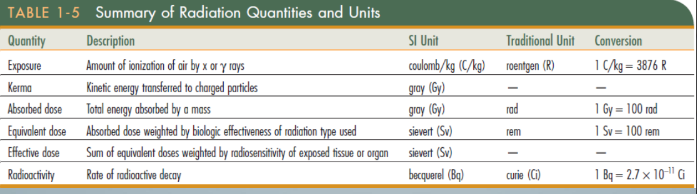
quantity, description, SI unit, traditional unit, conversion
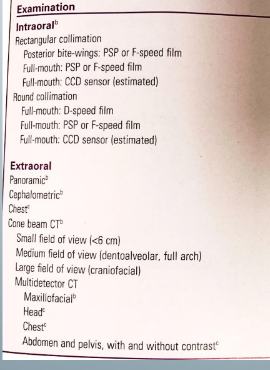
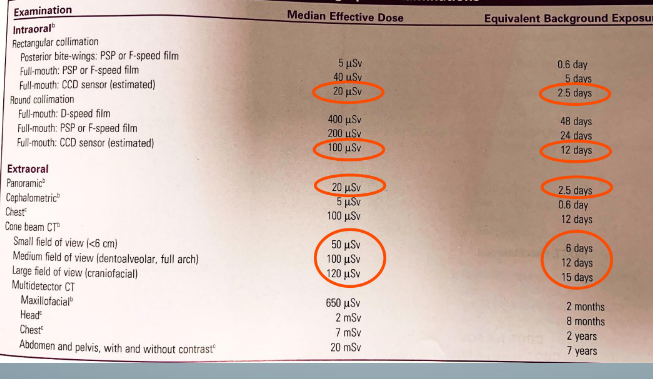
exam, median effective dose, equivalent background exposure
dental x-rays and risk of meningioma study
4 reasons why estimation of risk of radiation-induced cancer from dental imaging is difficult
ALARA
-as low as reasonably achievable
-every effort should be made to keep the dose to all individuals as low as practical (economic and social factors being taken into account)
-no patient exposure limit → up to the provider to decide how much radiation to expose patients to
means for reducing x-ray exposure
collimation
position and distance rule
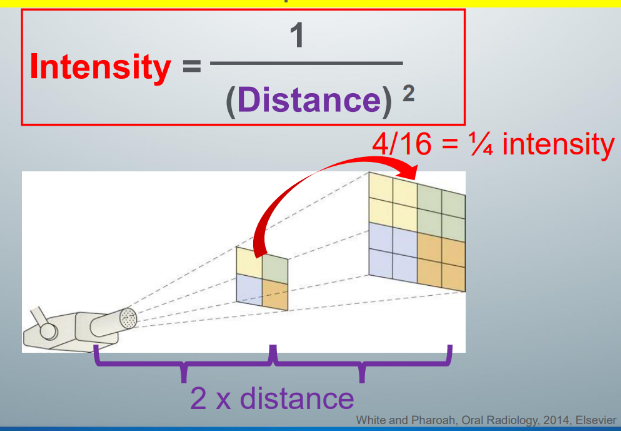
inverse square law
ALADA
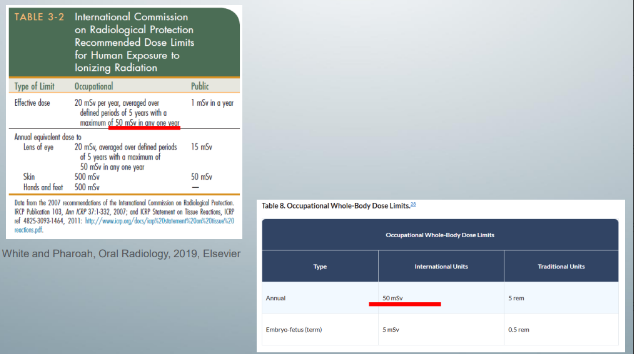
occupational whole-body dose limits
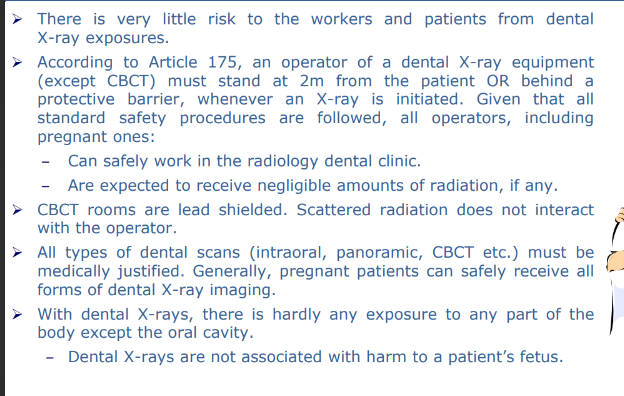
pregnant dental workers and patients
radiation
-transmission of energy through space and matter
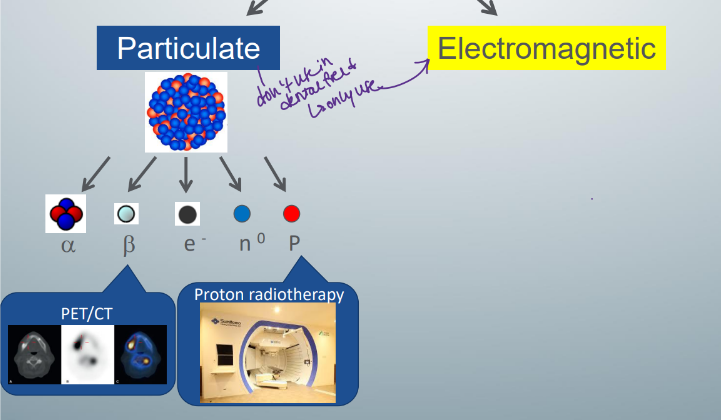
-2 types of radiation: particulate and electromagnetic
particulate radiation
-released when large, unstable, radioactive atoms spontaneously break down or decay
-radioactive atom is unstable because it contains unequal numbers of protons and neutrons (usually more neutrons than protons)
-to stabilize themselves, radioactive atoms decay, releasing subatomic particles and are transmuted into another element
subatomic particles
-alpha particles: helium nucleus consisting of 2 protons and 2 neutrons, protons and neutrons make the mass of an alpha particle HEAVY and slow
-beta particles: if positively charged = positron, if negatively charged = electron, both are light and fast
use of particulate v. EM radiation
-in medicine, particulate used in PET scans and some types of radiation therapy
-in OMF radiology, use EM
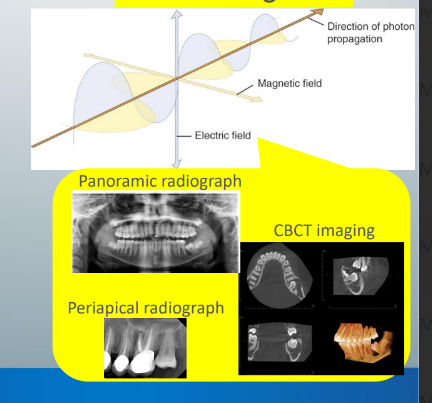
EM radiation
-movement of energy through space as a combination of electric and magnetic fields
-generated when the velocity of an electron (or any other charged particle) is changed
-2 theories: wave and quantum
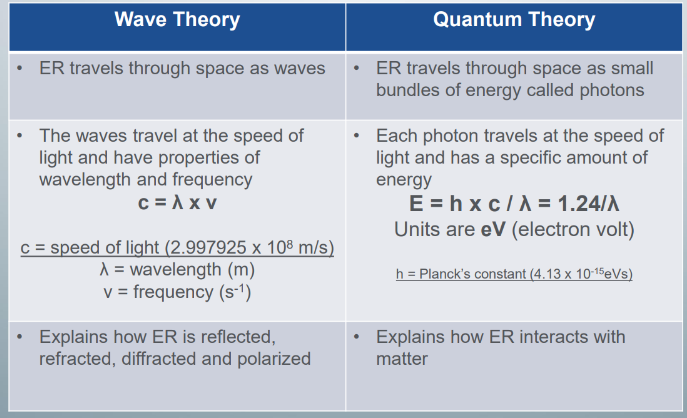
wave theory
-describes ER to travel through space as waves
-waves travel at the speed of light and are governed by an equation, which states that the waves have wavelengths and frequencies
-explains how ER is reflected, refracted, diffracted, and polarized
quantum thoery
-describes ER to travel through space as small bundles of energy (photons)
-each photon also travels at the speed of light but has a specific amount of energy called photon energy
-photon energy measured din eV and is related to wavelength (E=1.24/lambda simplified)
-explains how ER interacts with matter
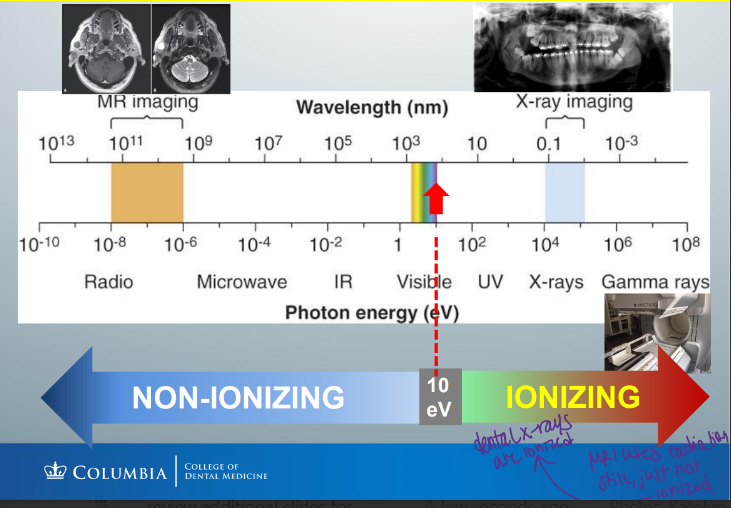
types of EM radiation
-radiowave, microwave, infrared, visible light, UV light, x-rays, gamma rays
-all travel at the sped of light, but all have different energies, wavelengths, and frequencies
-usually, high-energy photons (x-rays, gamma rays) characterized by energy (eV)
-medium energy photons (visible light, UV light) characterized by wavelength (nm)
-low energy photons (radiowaves, microwaves) characterized by frequency (Hz)
it is the _____ that determines whether a type of ER can ionize or not
-ENERGY
-photon energies greater than 10 eV are ionizing
-therefore, radiowaves, microwaves, IR, and visible light cannot ionize matter and are non-ionizing
-UV light, x-rays, and gamma rays are ionizing radiation
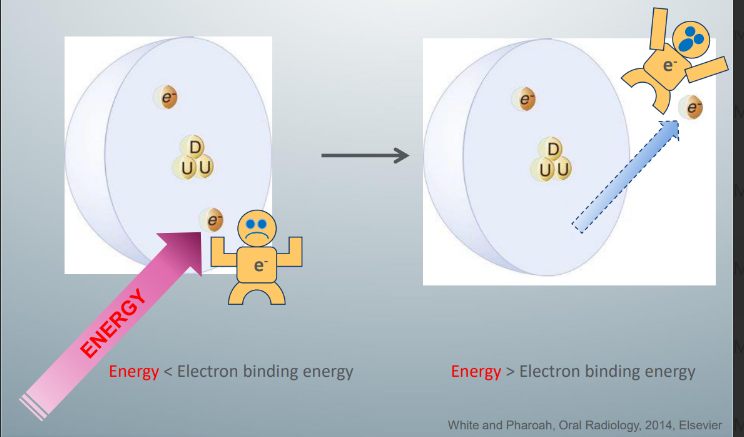
ionization
-electrons exist in different orbits and are bound to the nucleus by an electrostatic force (electron binding energy)
-electrons in the inner orbit (closer to nucleus) are more tightly bound than those in outer orbits
-larger atoms have greater binding energies because larger atoms have more protons to bind electrons more tightly
-neutral atoms have the same number of electrons and protons in an atom
-ionization (formation of an ion) occurs when a neutral atom loses an electron to become a positive ion
how can atoms be ionized?
-can be ionized by enough energy to overcome the electron binding energy
-this energy can be heat, particulate radiation, and ionizing EM radiation
-since ionization can only occur if there is enough energy to overcome the electron binding energy, only certain types of ER in the spectrum (high energies) are ionizing
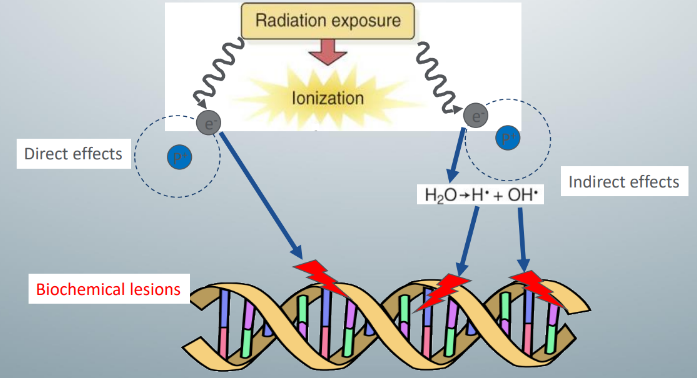
harm to biologic systems
-x rays can damage biologic systems directly and indirectly
-direct effects: occur when x rays ionize biologic molecules to form free radicals that damage cellular components
-indirect effects: occur when x rays ionize water to form hydrogen free radicals and hydroxyl free radicals in a complex reaction (radiolysis of water)
-hydrogen and hydroxyl-free radicals damage the cellular components
-since biologic systems comprise approx. 70% water, 2/3rds of biologic effects of x rays are indirect effects, the rest is from direct effects
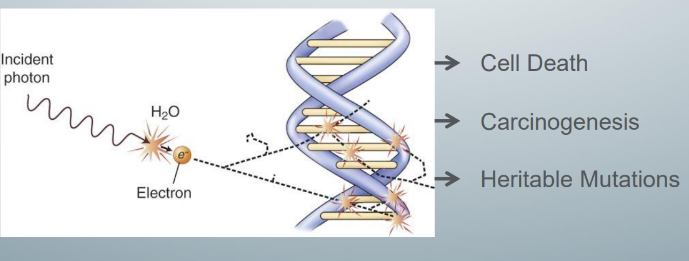
most important target in the cell for x-ray induced damage
-DNA because DNA damage can lead to cell death, carcinogenesis, and heritable mutations
-these 3 possible outcomes of radiation-induced DNA damage govern the clinical manifestation of radiation-induced DNA damage
if radiation kills cells
-the cells die and the associated tissue and organs are damaged
-clinically, this type of radiation-induced tissue reaction (deterministic effect) presents to us as tissue and organ malfunction
-example of deterministic effect: xerostomia after radiotherapy
-deterministic effects do not immediately manifest clinically- there is a latent period between the time of radiation exposure and the onset of the effect
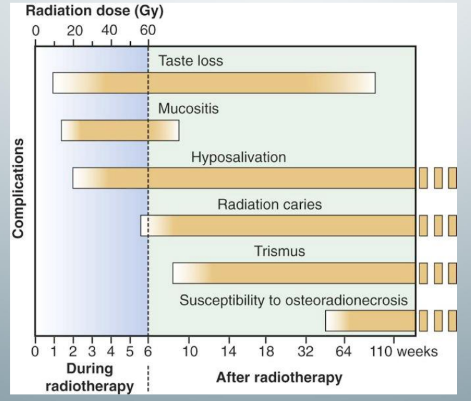
timeline for deterministic effects of oral cancer patients treated with radiotherapy
-known as complications of oral radiotherapy
-in short-term effects, the mechanism of injury is direct cell death
-in long-term effects, the mechanism of injury is fibrosis of blood vessels, creating a radiation-induced hypovascular environment that decreases cellular resistance to infection and loss of cellular function
-classic triad of osteoradionecrosis: hypovascularity, hypoxia, hypocellularity
if radiation damages the cellular DNA but the cell does not die
-the cell cannot repair the damaged DNA and we have mutations
-stochastic effects: sub-lethal radiation-induced damage
-clinically presents as cancer due to the replication of mutated cells or heritable mutations
-there is also a latent period
latency period of radiation-induced leukemia in atomic bomb survivors
-7 years after radiation exposure
-radiation-induced solid tumors (thyroid, salivary gland) occur at least a decade after radiation exposure
what determines the outcome of radiation-induced DNA damage?
-deterministic effects depends on dose- effects occur ONLY when the dose of the radiation exceeds a threshold, once the dose exceeds the threshold, the greater the dose, the more severe the deterministic effect
-stochastic effects depends on how lucky you are- there is NO threshold dose, there is NO grade of severity- you either get cancer or not; the higher the dose, the more likely cancer or mutation will occur
cells that are most sensitive to radiation
-those that have a high mitotic rate, many future mitoses, primitive differentiation
-examples: hematopoietic stem cells in bone marrow, lymphoid organs, basal cells lining the oral mucosa and intestines
-the least radiosensitive cells are those that: rarely (if ever) undergo mitosis, are highly or terminally differentiated (brain cells, muscle cells, mature RBCs)
gestational age and radiation risk
-gestational age 3rd and 4th weeks: no obvious effects, which means they probably undergo spontaneous resorption
-5th-10th weeks: malformations (organ abnormalities)
-11th-17th weeks: IQ deficits associated with stunted growth, microcephaly
-after the 18th week: would be less severe
-after the 27th week: none
-although the most sensitive weeks, 8-15 weeks have no risk in dentistry
vigilance when deciding whether or not to expose children to x-rays
-kids are not smaller adults
-peds are still actively growing, so their cells are highly actively dividing and therefore are more sensitive to radiation changes
-peds are expected to have longer life spans than adult, so they have more chances of getting more x rays for medical and dental purposes in their lifetime and longer life span for cancer to manifest clinically as kids are unlikely to outlive the latent period
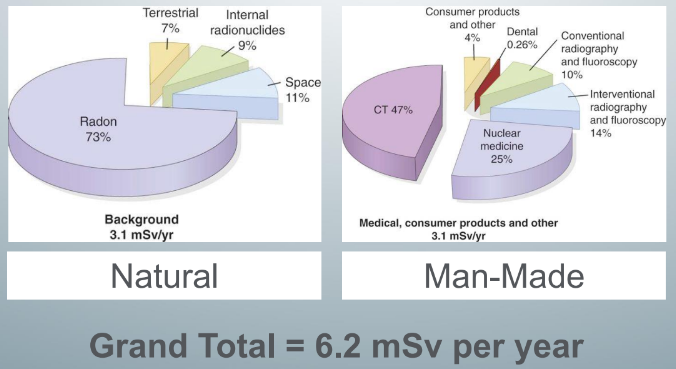
background radiation
-2 types of background radiation: natural and man-made
-total effective dose is 6.2 millisievert
-subtotal natural background and subtotal man-made medical exposure are almost the same
natural background of radiation
-largest contributor is radon (2.3mSv)
-radon is everywhere around you
man-made background radiation
-largest contributor is medical CT (1.5mSv)
-dental exposure very small in comparison (0.007mSv)
types of intraoral radiographs and exposures
-FMS = 2.5 days of background exposure
-if you use round collimation, it would be 12 days of background exposure
-pan = 2.5 days
-CBCT varies depending on the size of the exposure area and units for different companies (about 1-2 weeks)
estimation of radiation-induced cancer is difficult because
-number of known radiation-induced cancers is small and related to high doses
-cancer is prevalent
-radiation-induced cancers are clinically undistinguishable
-the latent period is long, therefore it is difficult to prove that cancer is directly related to earlier radiation exposure
safeguards to minimize x-ray exposure to dental patients
-use F-speed film or digital sensors
-use rectangular collimation
-use a lead apron to cover the gonads
-use a thyroid collar to cover the thyroid gland
-optimize exposure settings for diagnostic use
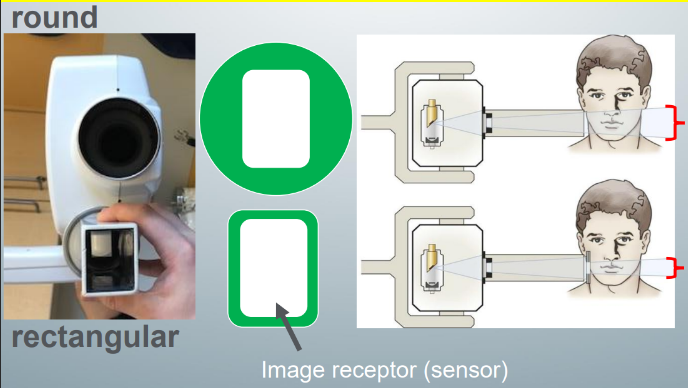
collimation
-process of aligning the x-ray beam to a specific shape
-rectangular aligns the beam to a rectangular shape slightly larger than the size of the rectangular image receptor
-round aligns the beam to a round shape large enough to cover the rectangular image receptor
-rectangular reduces exposure by more than 50% compared to round
-collimator = metallic barrier with an aperture to reduce the size of the x-ray beams and volume of irradiated patient tissue
-dental x-ray beam collimated to a circle not more than 2.75” in diameter
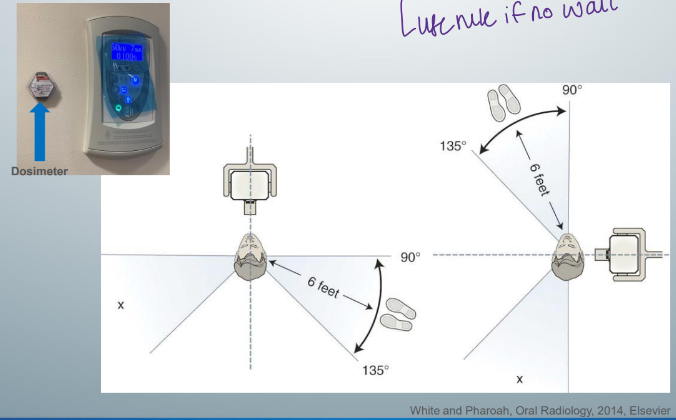
provider protection
-leave the room and hide behind a wall
-if there is no wall, stand at least 6 feet from the patient at an angle of 90 to 135 degrees to the x-ray beam during exposure
-^position and distance rule
intensity of x-ray beam
-inversely proportional to the square of the distance between the source and the point of measure
-when the distance from the source to a target is doubled, the intensity of the beam decreases to 1/4
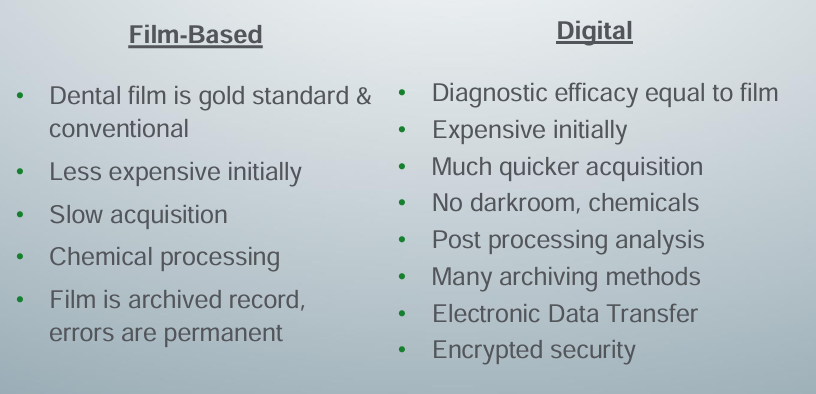
analog v. digital
-digital refers to the numeric format of the image content and its discreteness
-conventional film images can be considered an analog medium- differences in the size and distribution of black metallic silver result in a continuous density spectrum
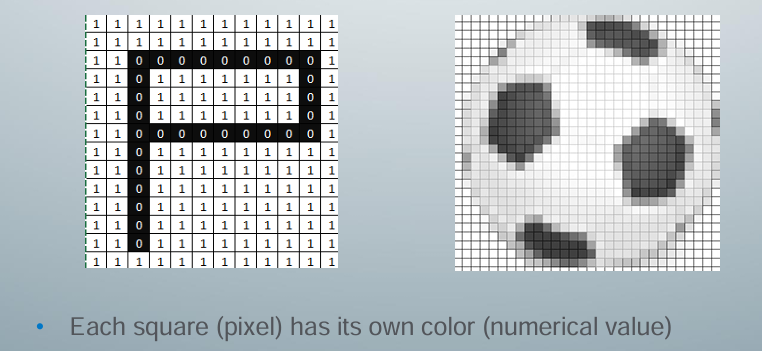
-digital image consists of a large collection of individual pixels
digital
-image made up of a large number of discrete picture elements (pixels)
-location of each pixel uniquely identified by a row and column coordinate within the image matrix
-value assigned to a pixel represents the intensity (gray level) of the image at that location
-at each pixel of an electronic detector, the absorption of x rays generates a small voltage
-more x rays generate a higher voltage and vice versa
-at each pixel, the voltage can fluctuate between a minimum and maximum value, therefore it is an analog signal
analog-to-digital conversion (ADC)
-2 steps: sampling (a small range of voltage values are grouped as a single value) and quantization (every sampled signal is assigned a value)
-narrow sampling mimics the original signal but leads to larger memory requirements for the resulting digital image
-once sampled, the signal is quantized
components of x-ray imaging system: source, detector, processing, display
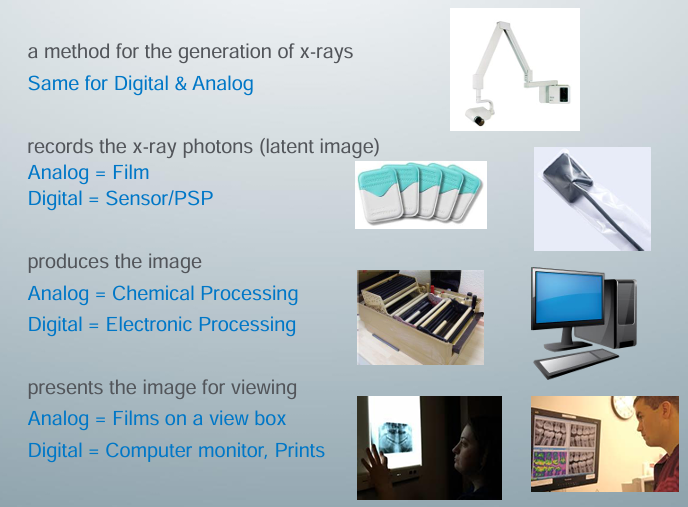
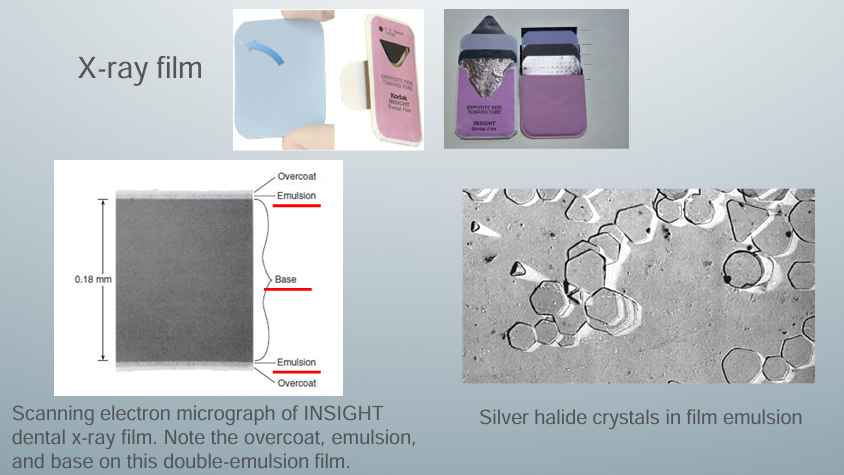
x-ray film
-no longer use film in practice
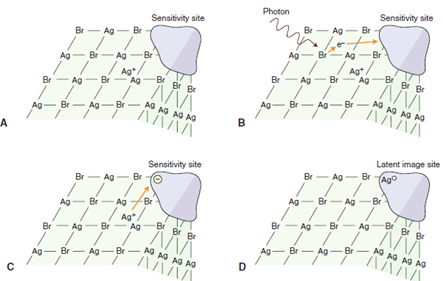
analog (latent image)
A) a silver bromide crystal in the emulsion of an x-ray film contains mostly silver and bromide ions in a crystal lattice, there are also free interstitial silver ions and areas of trace chemicals that form sensitivity sites
B) exposure of the crystal to photons in an x-ray beam results in the release of electrons, usually by interaction of the photon with a bromide ion; recoil electrons have sufficient kinetic energy to move about in the crystal, when electrons reach a sensitivity site they impart a negative charge to this region
C) free interstitial silver ions (with a positive charge) attracted to the negatively charged sensitivity site
D) when the silver ions reach the sensitivity site, they acquire an electron and become neutral silver atoms; these silver atoms now constitute a latent image site, collection of latent image sites over the entire film constitutes the latent image, developer causes the neutral silver atoms at the latent image sites to initiate the conversion of all the silver ions in the crystal into one large grain of metallic silver, the bromine dissolves in the developer
-when a beam of photons exits an object and exposes an x-ray film, it chemically changes the photosensitive silver halide crystals in the film emulsion
-chemically altered silver bromide crystals constitute the latent (invisible) image on the film
-sites containing neutral silver atoms = latent image sites
-overall distribution of crystals after exposure constitutes the latent image
-processing the exposed film in the developer and fixer converts the latent image into the visible radiographic image
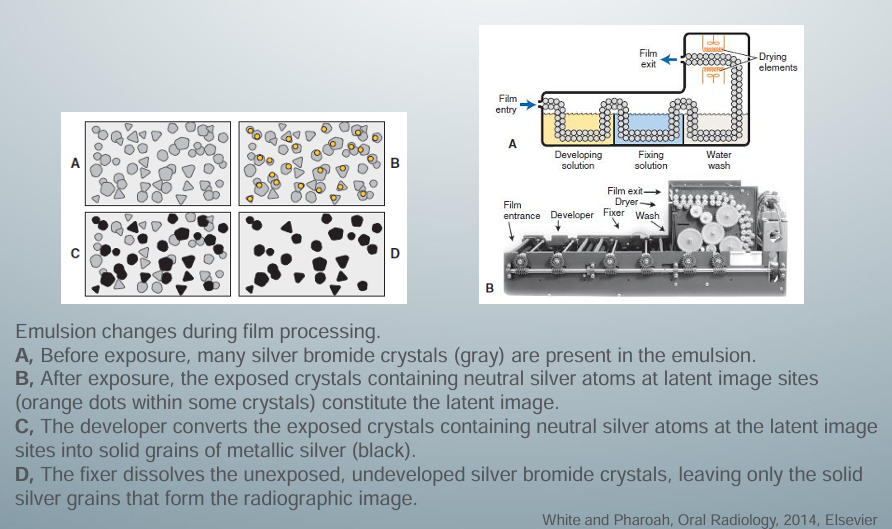
analog processing
-developer reduces all silver ions in the exposed crystals of silver halide to metallic silver grains
-to produce a diagnostic image, this reduction process must be restricted to crystals containing latent image sites
-individual crystals are developed completely or not at all during the recommended developing times
-variations in density on the processed radiographs are the result of different ratios of developed (exposed) and undeveloped (unexposed) crystals
-areas with many exposed crystals are darker because of their higher concentration of black metallic silver grains after development
-fixing solution removes undeveloped silver halide crystals from the emulsion
-replenish the developer and fixer: daily, maintain adequate freshness, adequate concentrations of chemicals
digital
-pixels of a digital image are in a grid with a specific “address” binary system
film-based v. digital imaging
digital imaging receptor
-no computer required to process CID image
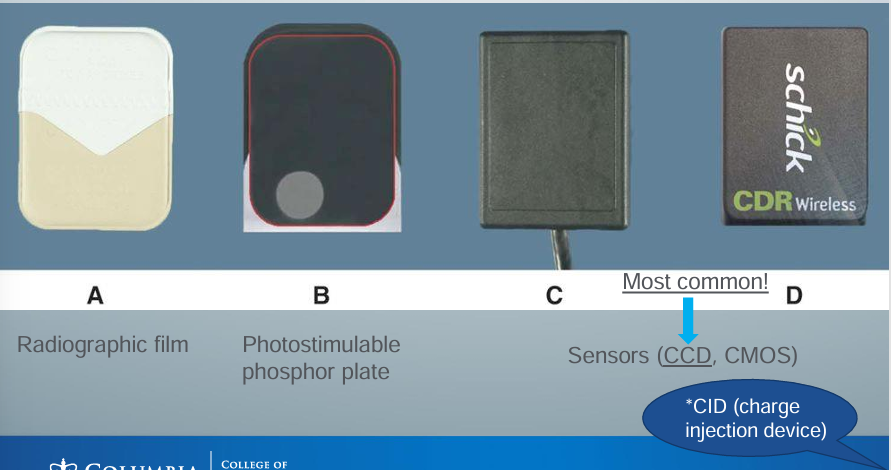
sensors
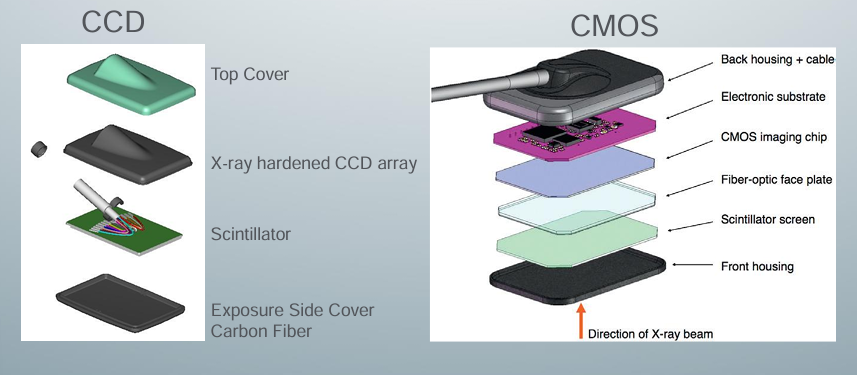
charge-coupled devices (CCD)
-most common!
-introduced in 1987 for dentistry
-high grade pure silicon- an amorphous silicon wafer
-contains an array of pixels- a process of transferring accumulated light or x-ray photons from one electronic well to another to a read-out device
-pixels are coupled to each other
-high quality image
-more expensive
-coupled to the surface by fiberoptics- material increases the x-ray absorption efficiency of the detector
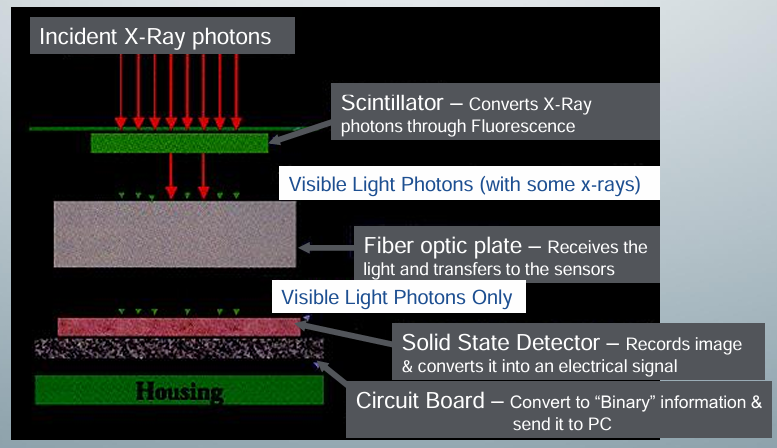
CCD function
-once the x-ray exposes the CCD sensor, the x-ray photons are converted to fluorescence by the scintillator
-fiber optic plate then receives the visible light photons to transfer to the sensors
-fiber optic plate eliminates x rays
-only visible light photons reach the solid state detector to record the imagee and convert it into an electrical signal
-circuit board converts to binary information and sends it to the computer
complimentary metal oxide semiconductor (CMOS)
-principle similar to CCD
-simpler circuit design
-less expensive
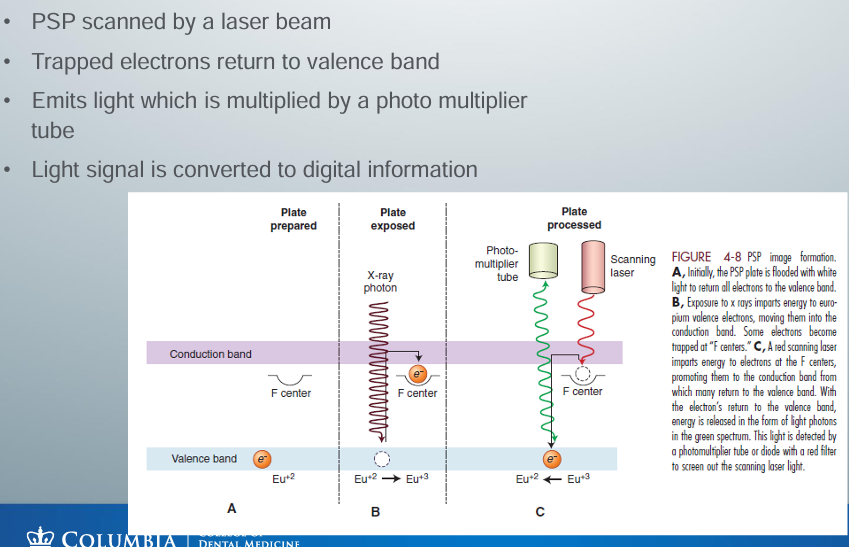
photostimulable phospher (PSP) plate
-storage phosphor
-composed of europium-activated barium fluorohalide
-similar to the intensifying screen phosphors, but PSP traps a significant number of electrons in its phosphor which is later read by a laser beam
-PSP absorbs x-ray energy and release energy as light when stimulated by another light of an appropriate wavelength
-to the extent that the stimulating light and phosphorescent light wavelengths differ, the two may be distinguished and the phosphorescence can be quantified as a measure of the amount of x-ray energy that the material has absorbed
-stores a portion of the energy as valence electron
-voltage signal quantified by an analog-to-digital converter and stored and displayed as a digital image
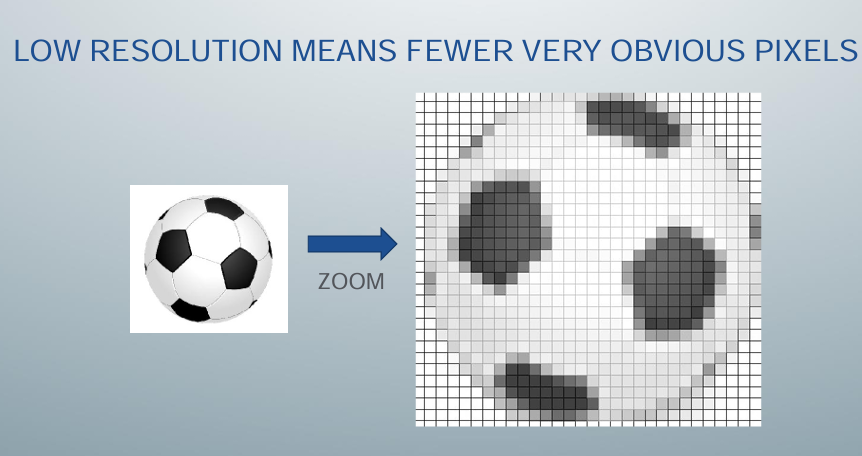
digital detector characteristics- resolution
-ability to identify 2 different objects that are close to each other
-digital images: >10 line pair/mm, eyes: 4-6 line pair/mm
-spatial frequency at which a digital image is sampled (sampling frequency) is often a good indicator of resolution
-why dots-per-inch (DPI) is used to express resolution for digital images
-decreasing pixel size and increasing DPI increase resolution
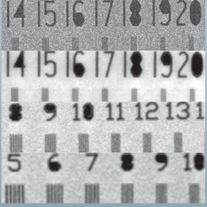
line pair/mm
-line pairs per millimeter
-resolution units
-test objects consisting of sets of very fine radiopaque lines separated from each other by spaces equal to the width of a line are constructed with a variety of line widths
-a line and its associated space are called a line pair (lp)
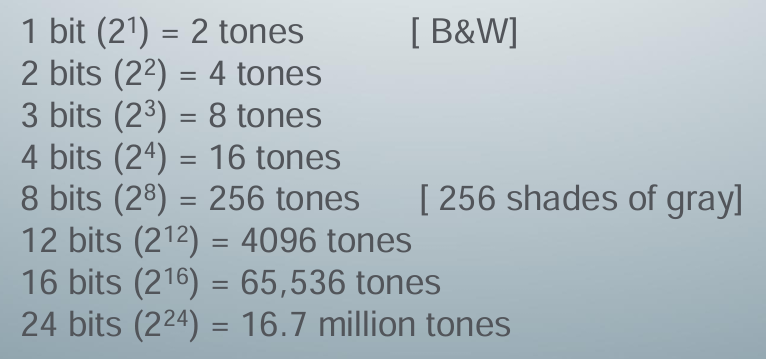
bits and shades of gray
-binary calculations for the number of tones represented by common bit depths
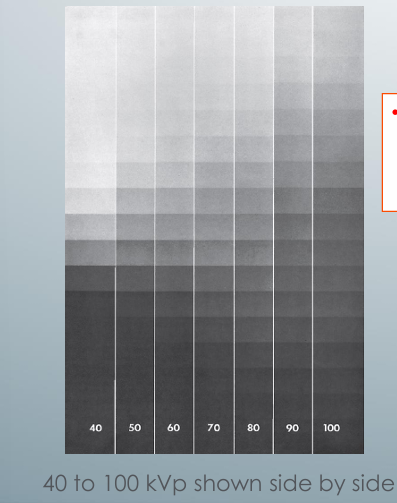
contrast
-the long gray scale (low contrast) image with high kVp and the short scale (high contrast) image when using low kVp
-term describing a radiograph’s range of densities
-density difference between light and dark regions on a radiograph
-subject contrast: range of characteristics of the subject that influences radiographic contrast, influenced largely by the subject’s thickness, density, and atomic number
-dense regions of bone and teeth absorb most of the incident radiation, whereas soft tissue facial profile transmits most of the radiation
-most clinicians select a kVp in the range of 60 to 80
-at higher kVp values, the exposure time is reduced but the loss of contrast may be objectionable because subtle changes may be obscured
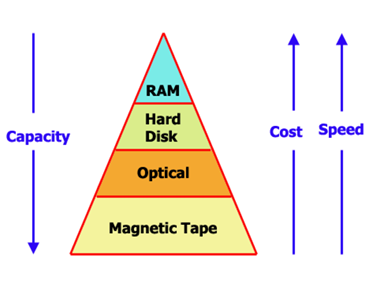
archiving
-storage, capacity, speed
-capacity
-data format (DICOM)
-image compression
-access time
-transfer rate
display
-computer monitor (best)
-print on paper
-print on films
advantages and disadvantages of digital imaging
-advantages: reduced radiation dosage, immediate image acquisition, consistent quality, image manipulation, improved archiving and retrieval, elimination of processing equipment and chemicals (environmental issues, elimination of dark room)
-disadvantages: cost (initial), receptor size and patient comfort, computer memory requirements, data safety (back up), potential fradulent image manipulation, lifespan of sensor, quality depends on monitor and printer, print quality often not optimal, unwanted manipulation of images, infection control issues
means for reducing x-ray exposure
-radiographic prescription criteria
-choice of dental x-ray equipment (rectangular collimation, long aiming cylinder, fast image receptors, rare-earth intensifying screens)
-lead apron and thyroid collar
-diagnostic exposure settings
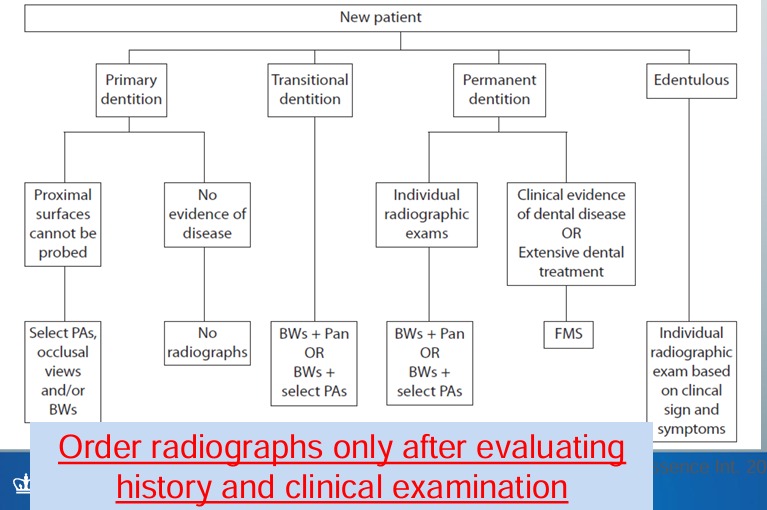
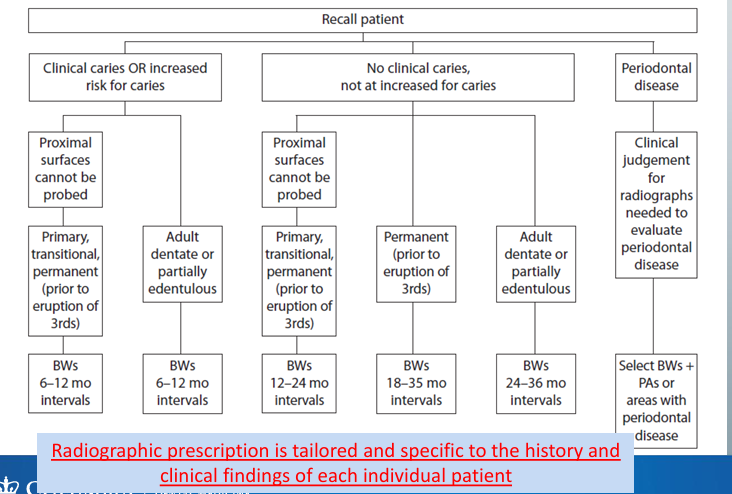
radiographic prescription
-medical/dental history and clinical findings
-are radiographs needed for this patient?
-prescribe x-rays only when needed, based on history and clinical exam
-prescription tailored and specific to each patient
-practice supported by the FDA and endorsed by the ADA
new patient radiographic prescription criteria
recall patient radiographic prescription criteria
potential concerns of radiograph prescription
-lawsuits for failure to diagnose: if you follow guidelines on radiographs endorsed by the ADA that help establish the standard of care, have no concerns
-radiation fear- ionizing radiation causes cancer, but we learned this has only been shown at high doses (atomic bombings, nuclear fallouts)
-if there is a clinical reason for imaging, take the image
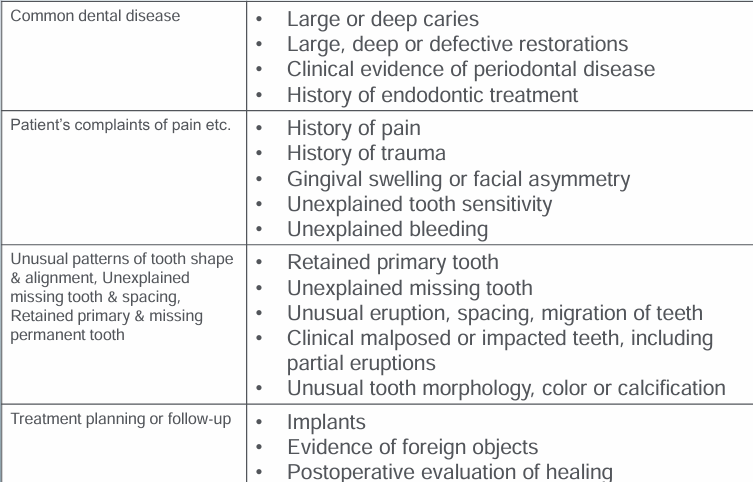
clinical indicators for radiographs
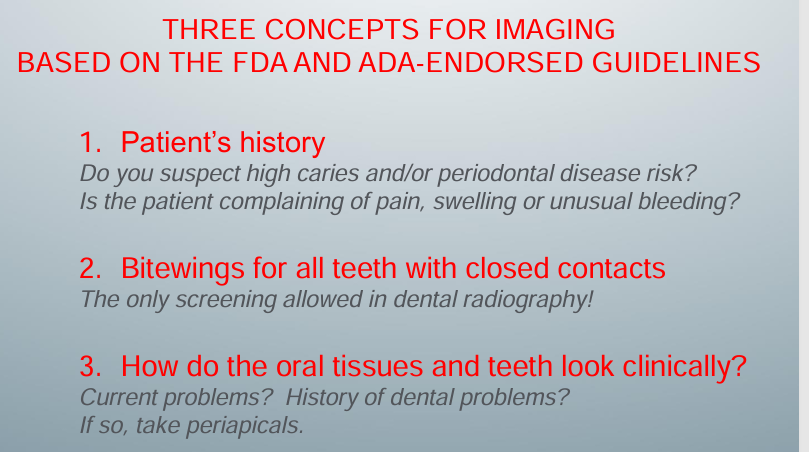
simple, 3-step process in radiographic prescription- step 1
-images of the patient’s CC, a clinical problem, image it using the appropriate views, PA, or pan
step 2
-bitewings for interproximal caries
-only for all teeth with closed proximal contacts
-screening BWs are allowed
step 3
-PAs for current/history of clinical problems
-caries and large restorations, defective restorations, gingival recession and periodontitis, endo tx, unusual tooth color and morphology, retained root tips, partially erupted tooth, gingival or vestibular swelling
radiographic prescription summary
considerations for pregnant patients
-dental imaging is allowed and indicated based on patient’s CC
-fetal exposure only about 1micro Gy even if we take intraoral images of teeth in all 4 quadrants
-follow principle of ALARA
considerations for patients who received head/neck radiotherapy in which at least 50 Gy of radiation was used
-dental imaging still allowed and indicated based on CC and clinical findings
-high risk for radiation-induced xerostomia and caries (deterministic effects)
-tell them that dental exposure is insignificant compared with what they have already received (micro v. milli Gray)
-dental exposure cannot exacerbate or cause the tissue damage associated with radiotherapy (like mucositis and osteoradionecrosis)
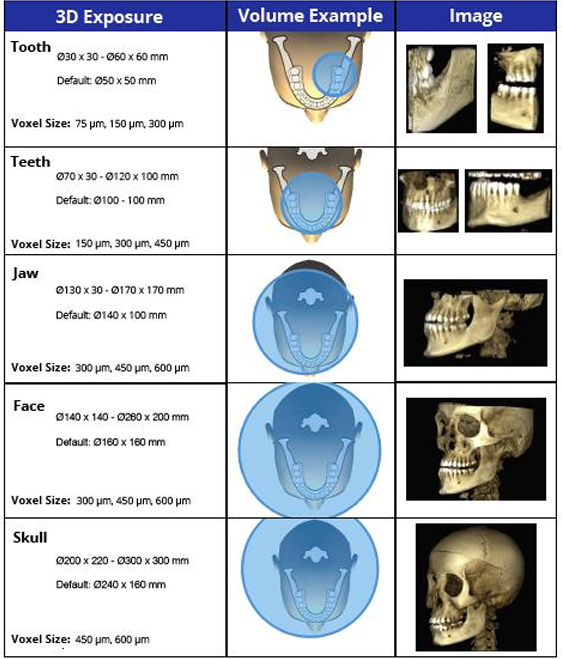
FOV in dentistry
-field-of-view
-anatomical area included in the volume
-consider the balance between dose savings and best image quality
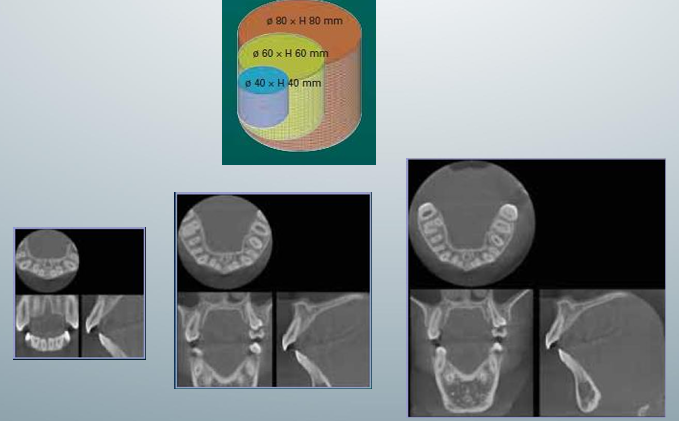
3D exposure, volume example, image for FOV
-top one called “limited”: focused or restricted FOV scans providing high-resolution images of limited regions
-second and third ones “one jaw” or “both jaws”: provide image of the maxilla or mandible or both
-fourth one “face”: images from the skull base to the chin
CBCT guidelines from NCRP
-use the smallest FOV to reduce patient exposure
-CBCT cannot be an alternative modality of BW, pano, and ceph
-CBCT should not be taken without a history and clinical exam
-CBCT should not be used as the primary or initial imaging modality when a lower dose alternative is adequate for the clinical purpose
-when refer pt for CBCT, give sufficient clinical information in the request form
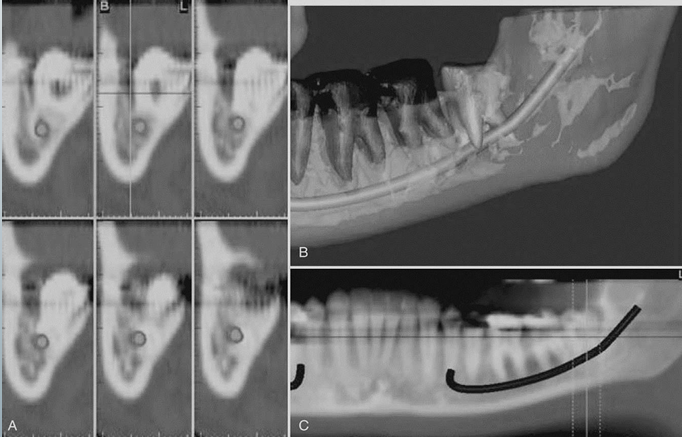
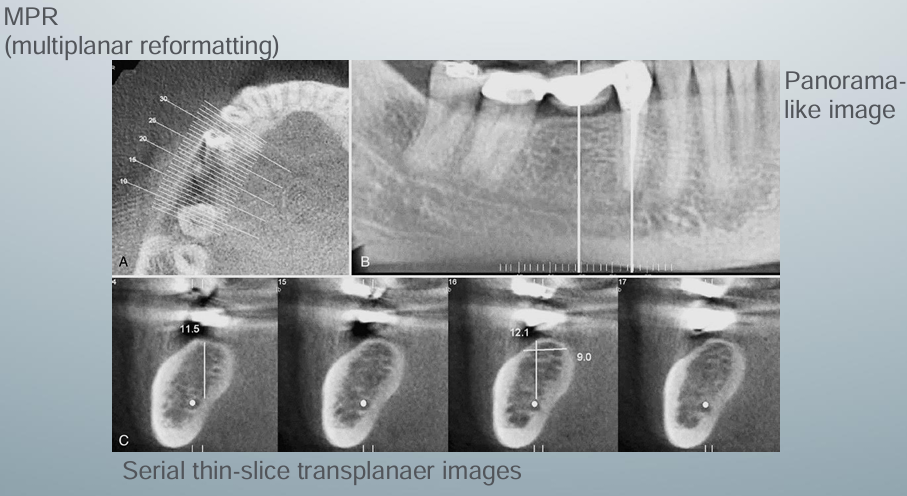
CBCT for implant site assessment
-curved planar MPR (multiplanar reformatting) accomplished by aligning the long axis of the imaging plane with the dental arch in A
-provides a region panorama-like thin-slice image in B
-serial thin-slice transplanar images are often generated (C), which are useful in the assessment of specific morphologic features such as the location of the inferior alveolar canal for implant site assessment and for allowing measurement of the available alveolar bone height and width
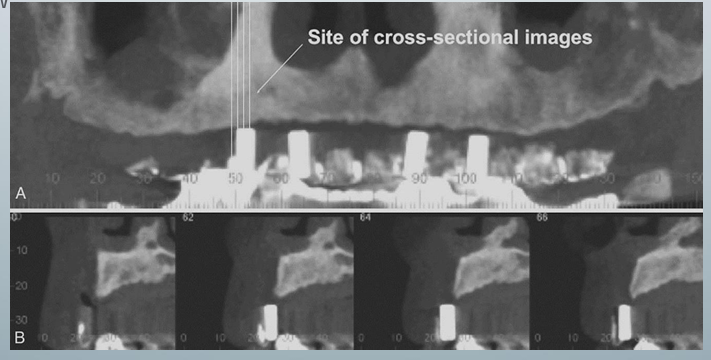
use of a diagnostic stent
-providers fabricate a diagnostic stent or radiographic guide, depending on the case
-stents provide fiducial radiographic landmarks that can be used to correlate the proposed clinical location and angulation of implants with the available alveolar bone
-pan projection in A provides an overview of the location
-serial cross-sections in B indicate alveolar bone height
CBCT for assessment of supernumerary teeth
-can investigate the location of the relationship with adjacent structures such as other teeth, the inferior alveolar canal, the maxillary sinus, etc.
-2D cannot provide the information

extraction treatment planning
-A is a cross-sectional view
-B is third-party software used to demonstrate the location of the inferior alveolar canal to an impacted third molar in 3D images
-C is an MPR reformatted image using proprietary software demonstrating the proximity of the root of an unerupted and impacted third molar associated with the IA canal