PHR 946 - Block 4: Cardiac Arrhythmias
1/22
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
23 Terms
arrhythmia
abnormal heart rhythm
- abnormality in: site of origin of impulse, rate/ regularity of impulse, or conduction of impulse
- may precipitate or worsen: ischemia, scarred/ diseased cardiac tissue, over-stretching of cardiac fibers
mechanism of arrhythmias
disturbances of impulse formation
- shortening duration of diastolic interval (tachycardia)
- lengthening duration of diastolic interval (bradycardia)
- effects on pacemaker rate (diastolic membrane potential, slope of phase 4 depolarization, threshold potential)
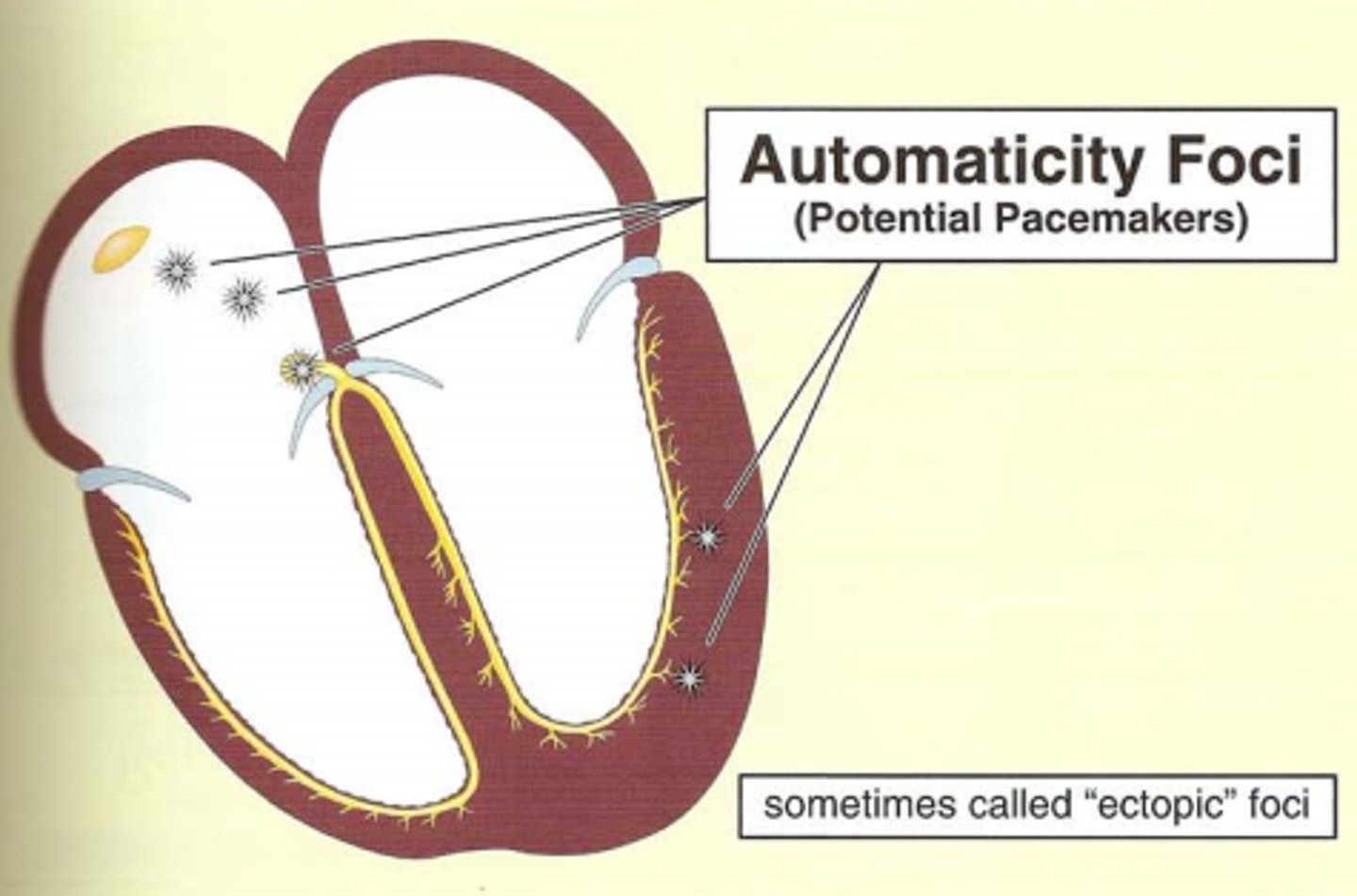
automaticity
the ability of the heart to generate and conduct electrical impulses on its own
- spontaneous generation of electrical impulses that spreads throughout the heart
- typically the sinus node is the primary pacemaker due to its inherent automaticity
heart stimulation and inhibition
- the heart is stimulated by the sympathetic cardioacceleratory center
> at SA node primarily
- the heart is inhibited by the parasympathetic cardioinhibitory center
cardiac electrophysiology
controlled spread of electrical currents
- contracts rhythmically, pumps blood
- currents produced by pacemaker cells, specialized conducting tissue, and heart muscle
- currents can be recorded by ECG using electrodes
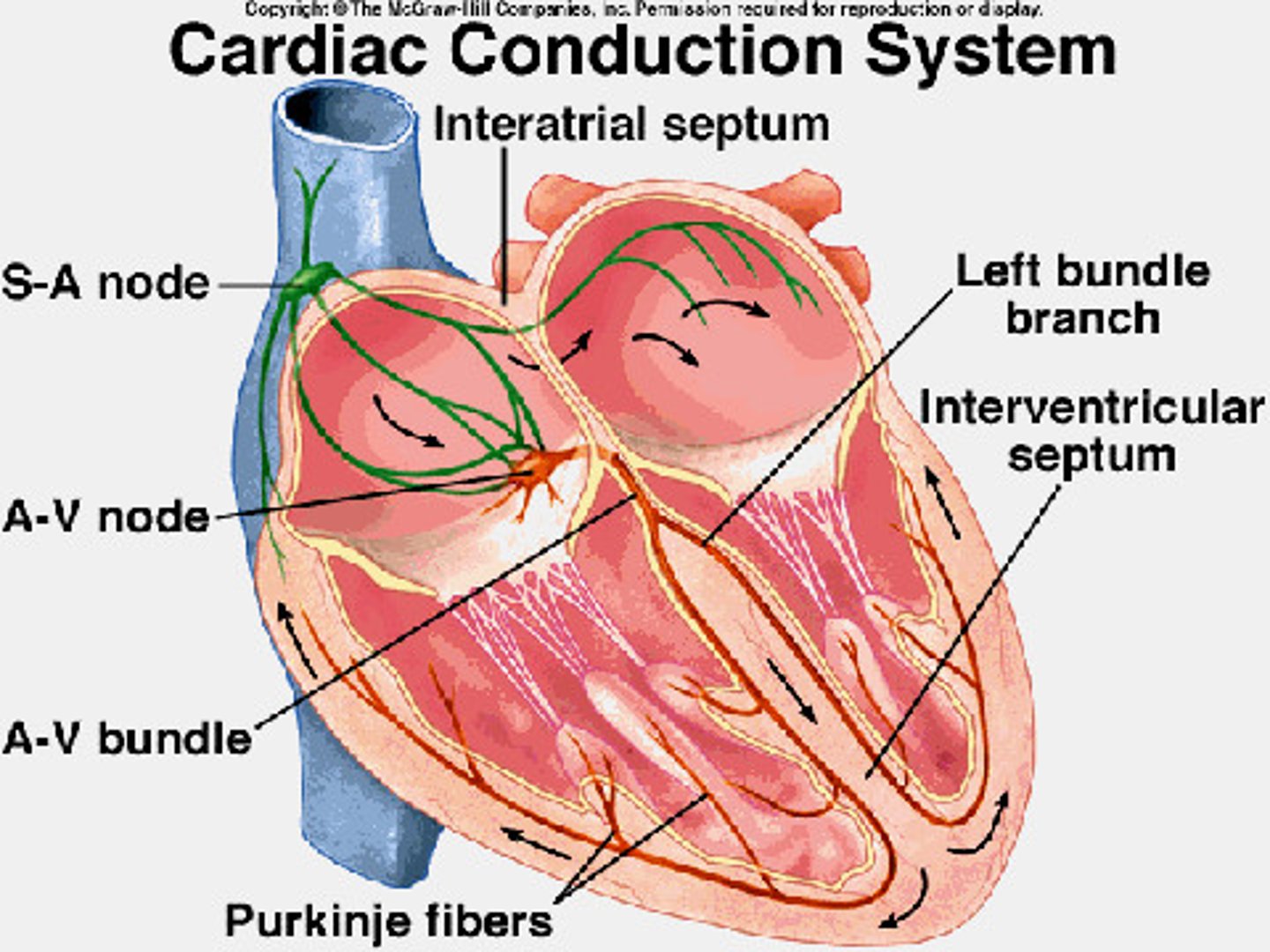
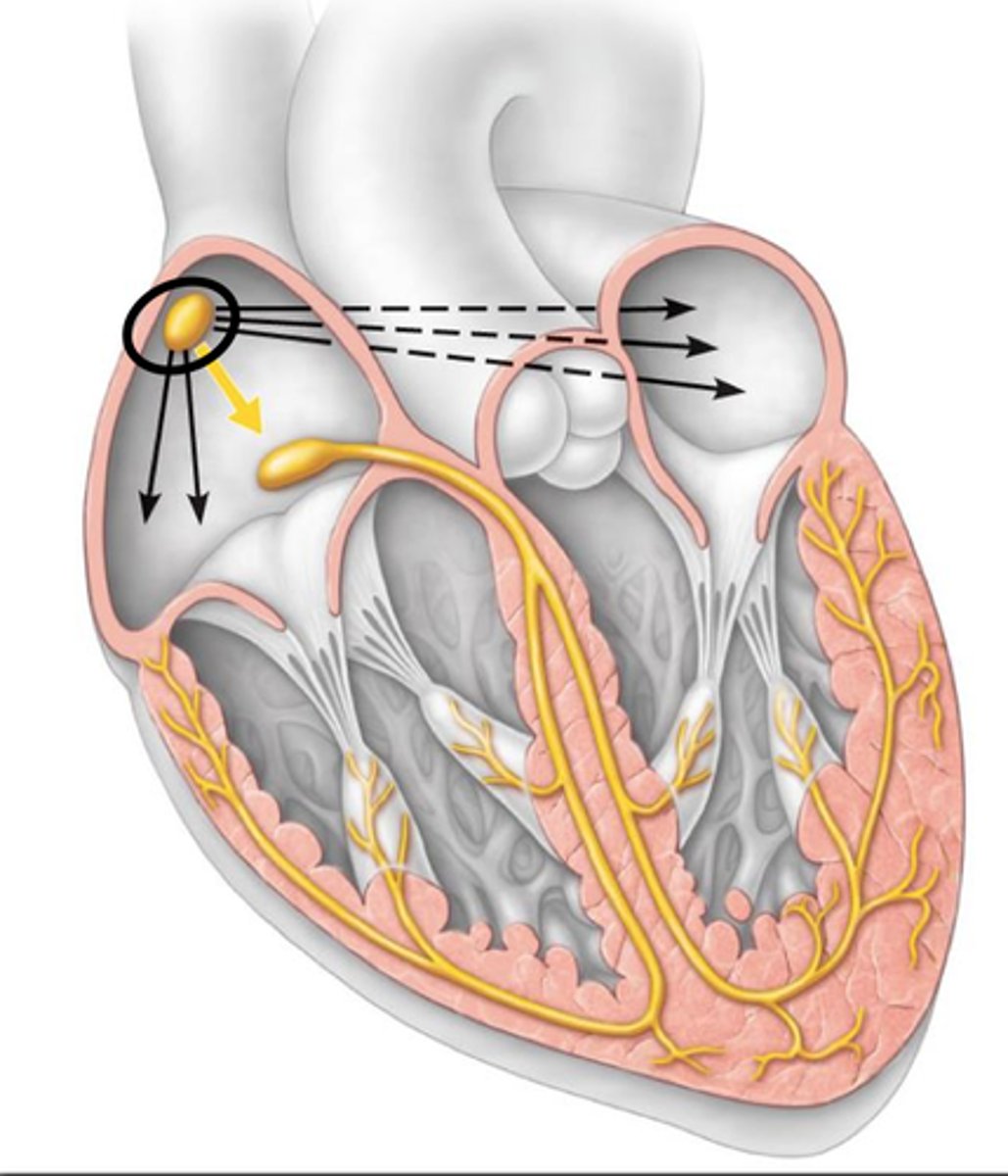
conduction system
1. SA node
- generates impulse, atrial excitation begins
- functions as the normal pacemaker
- slowest velocity
2. AV node
- impulse delayed
3. His bundle branches
- impulse passes to heart apex, ventricular excitation begins
4. Purkinje fibers
- ventricular excitation complete
- fastest velocity
5. repolarization
SA node
pacemaker of the heart
- small collection of specialized cells in the right atrium
- densely innervated with adrenergic and cholinergic nerve terminals
- neurotransmitters control discharge rate
> sympathetic nerve terminals: positive chronotropic response; beta-1 receptor activated pathway
> parasympathetic nerve terminals: negative chronotropic response; acetylcholine activating muscarinic receptors
- signals the atria to contract and pump blood into left and right ventricles, then signal spread to conduction tissue in the AV junction, spreads to left and right bundle branches, and transmits stimulus to ventricular muscle cells
sick sinus syndrome
sinus node dysfunction
- severe depression of sinus node function
- leads to dizziness/ syncope from excessive bradycardia
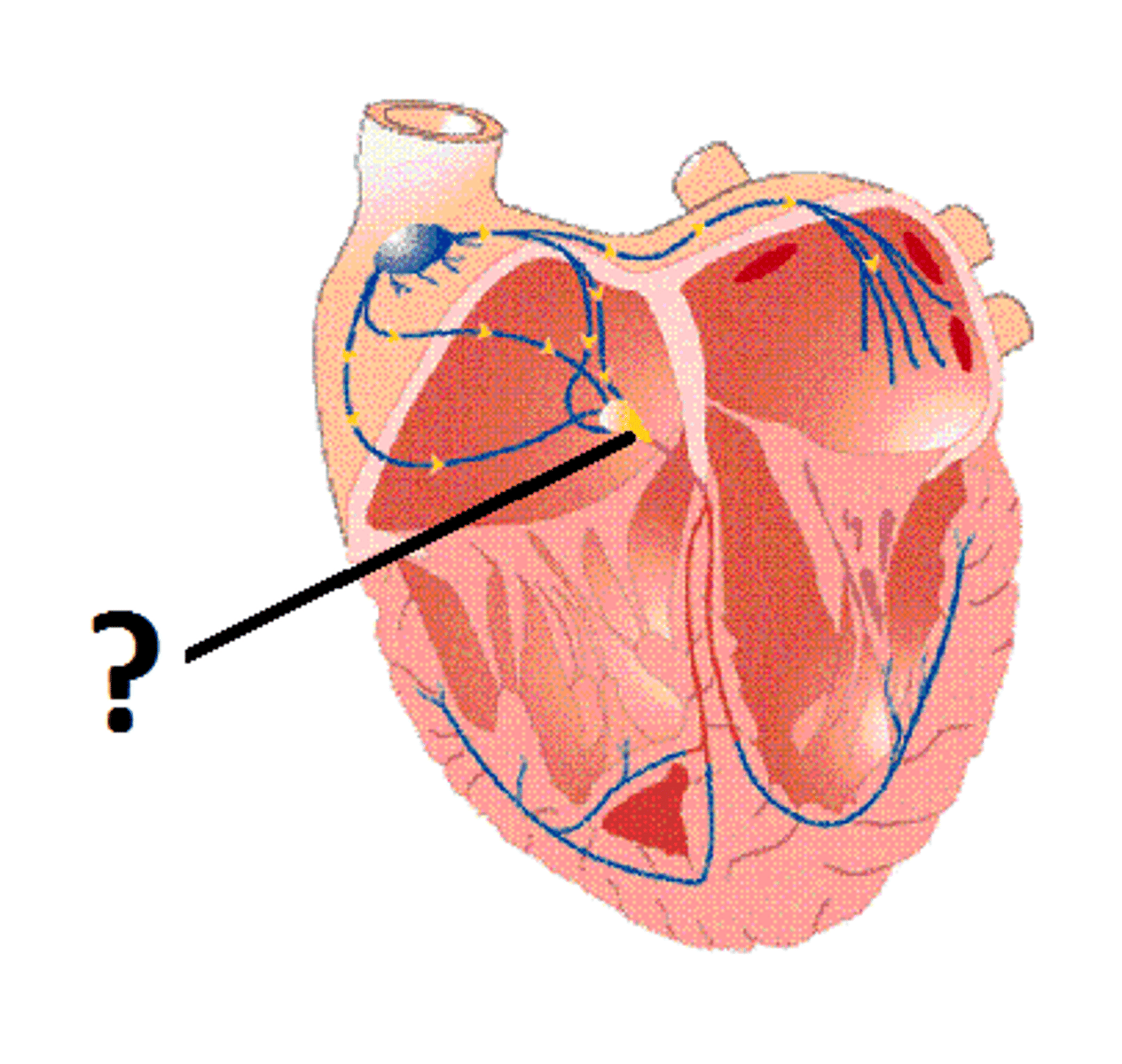
AV junction
relays electrical impulses from atria into ventricles
- upper (proximal): AV node
- lower (distal): His bundle
- divides into right and left bundle branches
- distributes signals to ventricles through Purkinje fibers
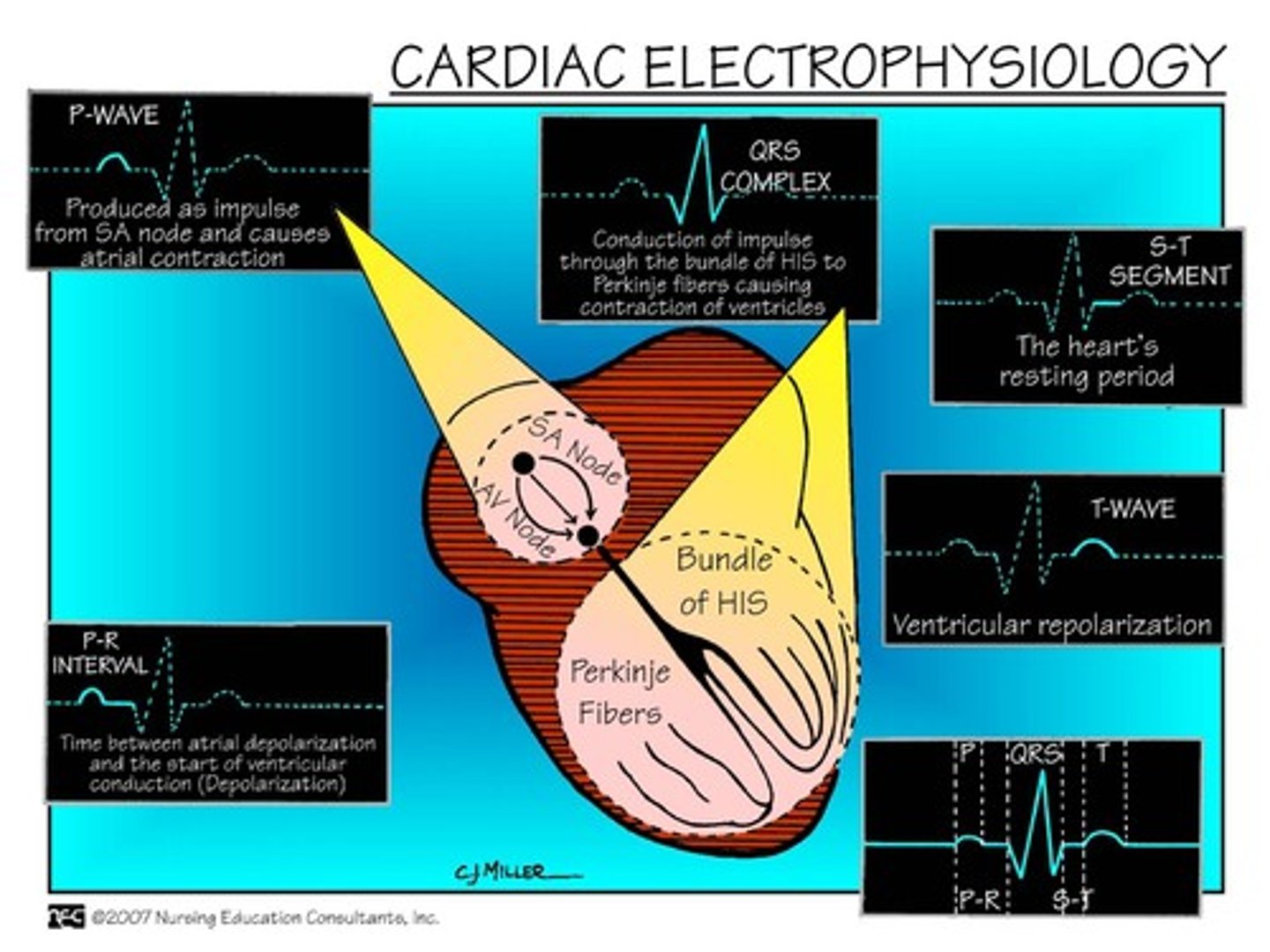
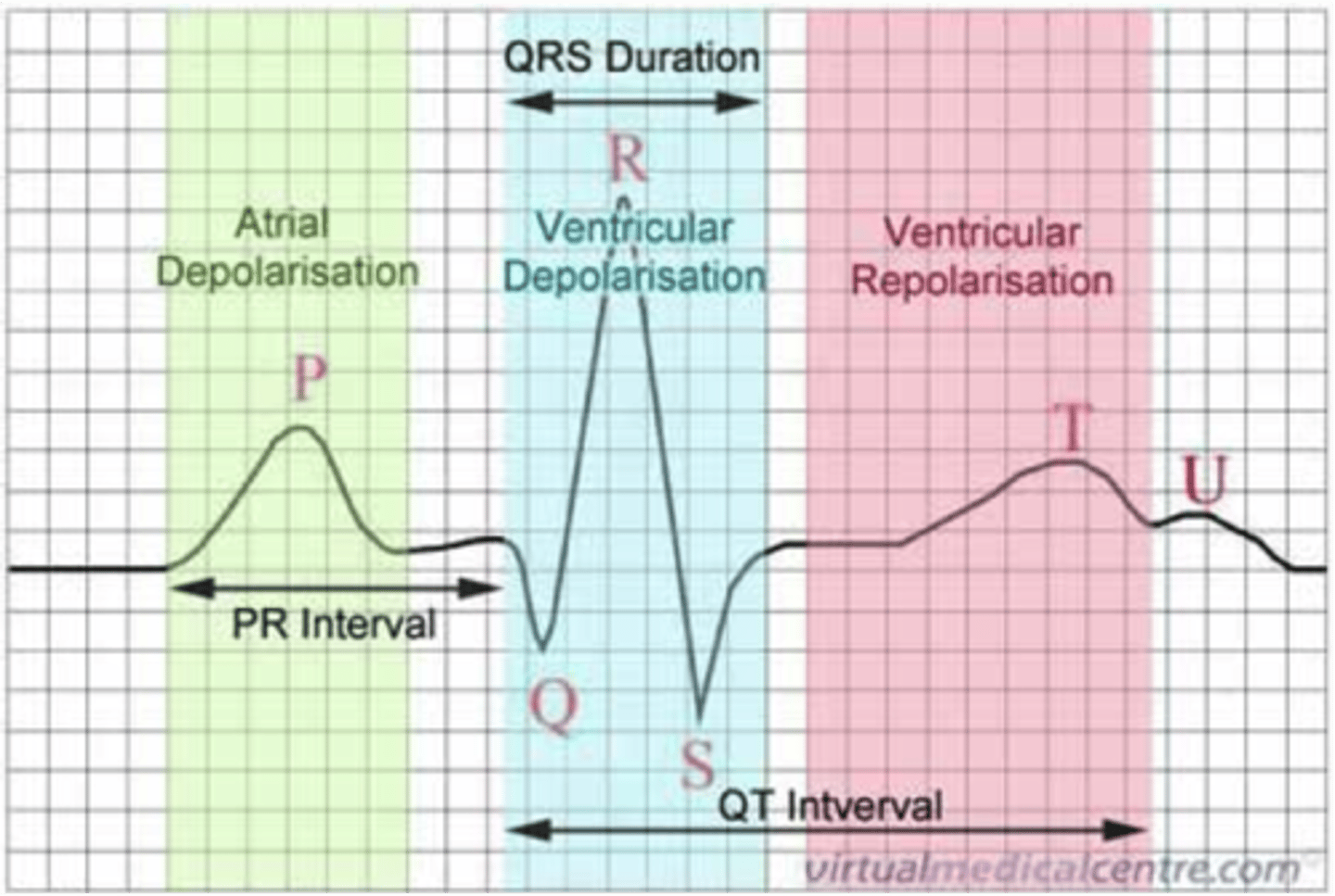
basic ECG
- P wave: atrial depolarization
- PR interval: time from AV node to bundle of His
- QRS complex: ventricular depolarization + atrial repolarization
- T wave: ventricular repolarization
- QT interval: refractory period
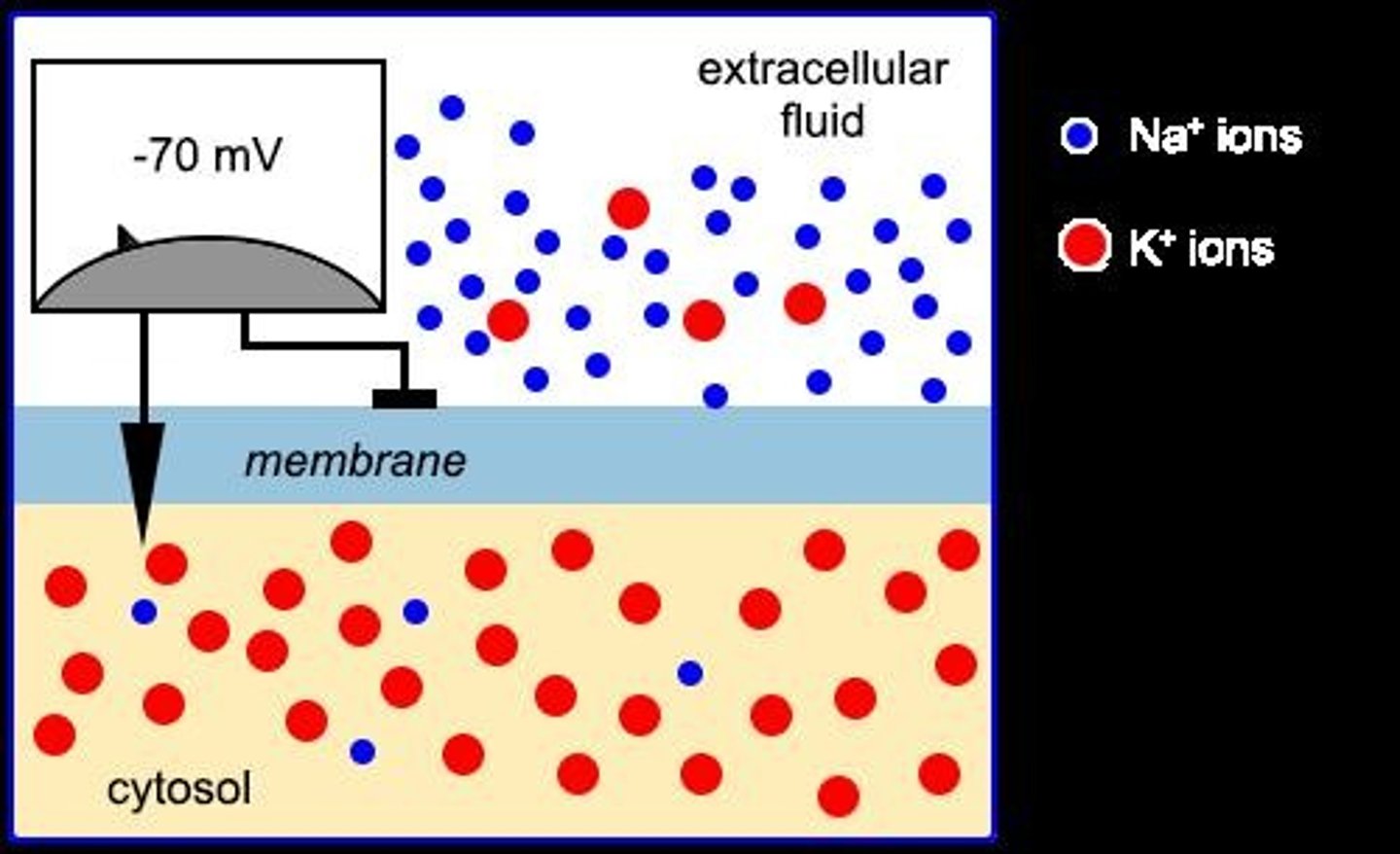
transmembrane potential
- the voltage difference across a cell membrane (intra and extracellular)
- determines cardiac electrical activity
- exists due to selectively permeable cell membrane: more Na+ outside, more K+ inside
- lipid bilayer acts as a barrier to allow movement of ions
electrical signaling
- Na+, K+, Ca²⁺, and Cl- are the major charge carriers
- movement across the cell membrane = current producing excitation signals in myocytes
- ion channels in lipid bilayer allows ions through selectively
cardiac action potentials
- depolarization: positively charged ions (Na+, Ca²⁺) flow in → intracellular potential decreases → charge inside approaches 0
- repolarization: specific ion channels and pumps return ions to their pre-depolarized concentrations → re-establishes concentration gradient and allows for next action potential
> mediated by Na+/K+ ATPase pump: 3 Na+ out, 2 K+ in
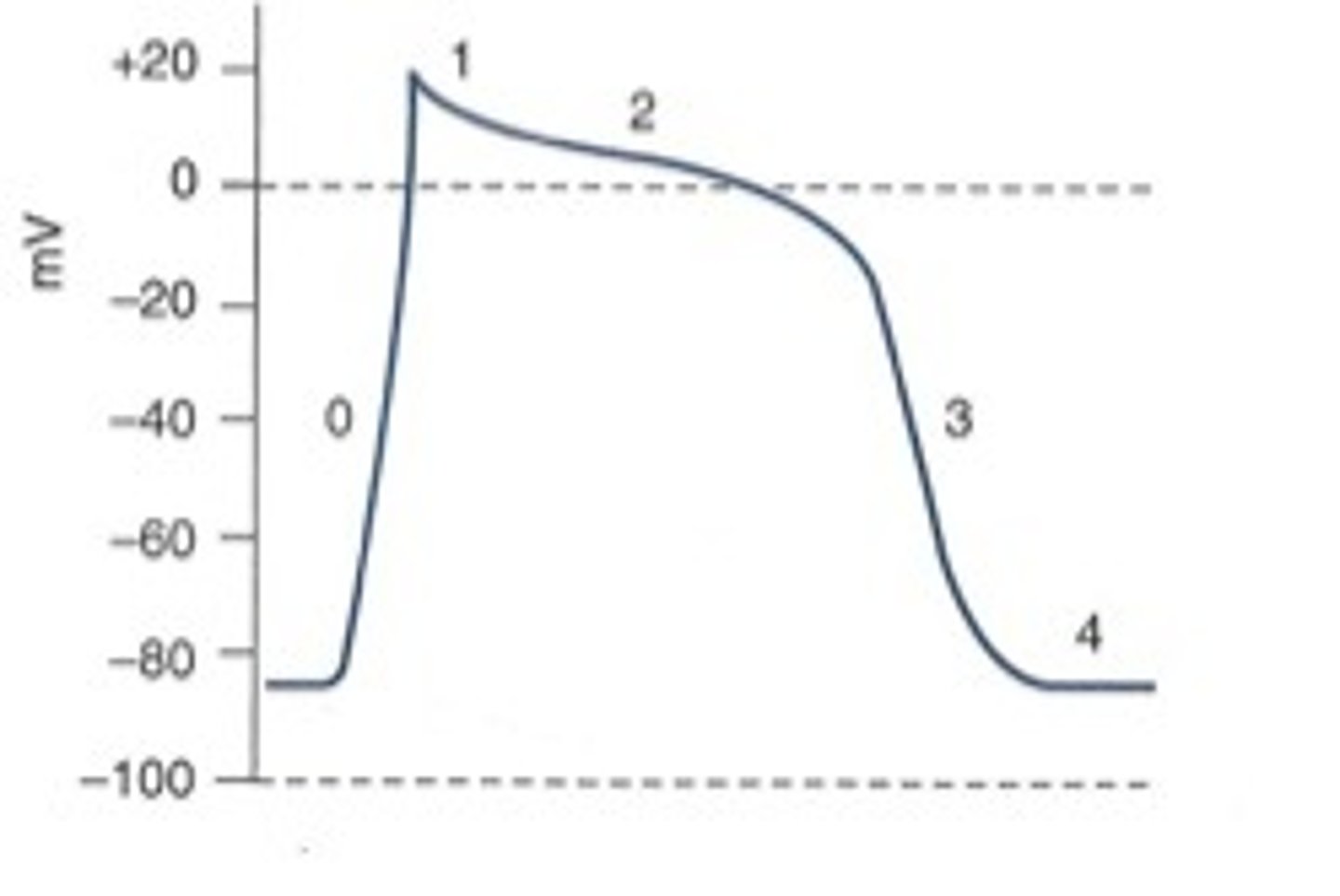
in pic:
0: rapid depolarization
1: early rapid repolarization
2: plateau results from competition between: repolarizing outward current (K+) & inward current (Ca²⁺)
3: final rapid repolarization from: inactivation of L-type Ca²⁺ channels & activation of delayed-rectifier K+ currents
4: resting membrane potential
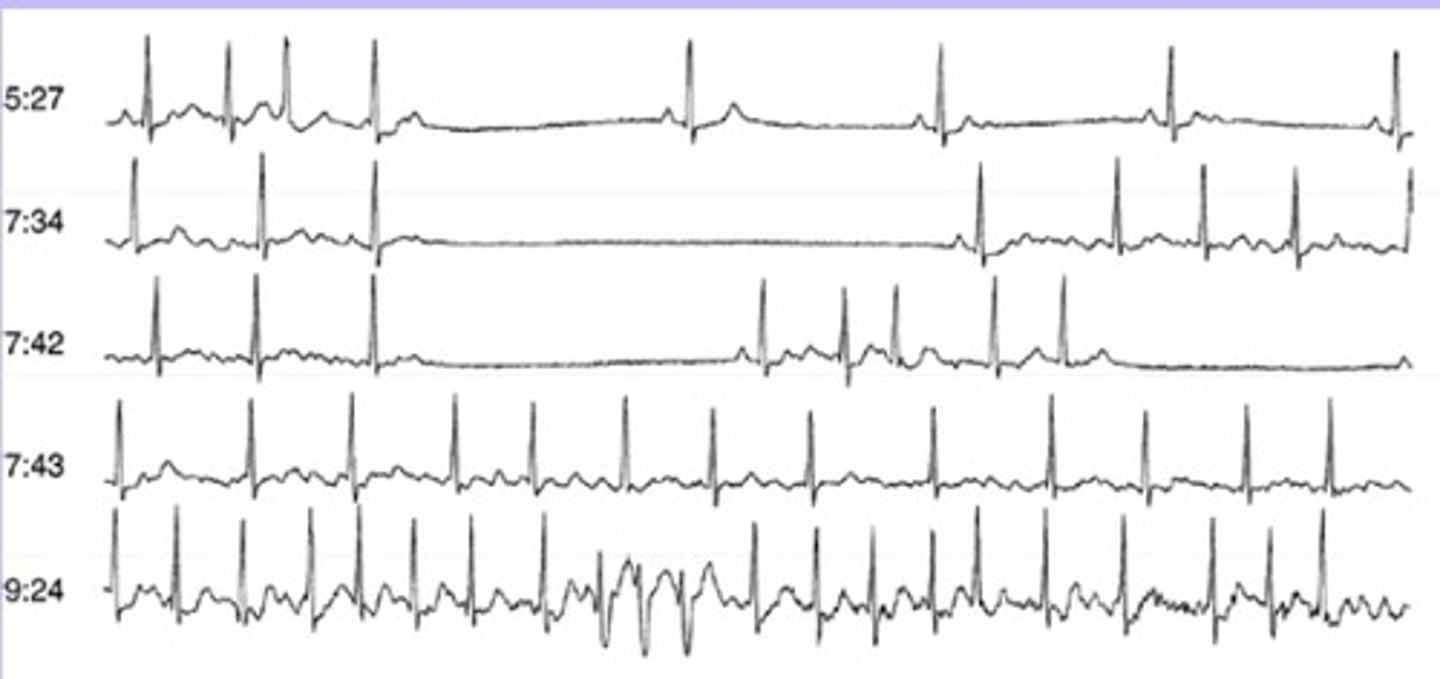
arrhythmia overview
bradycardia: slow heart rate
- sinus brady
- AV blocks
tachycardia: fast heart rate (>100 bpm)
- supra-ventricular
- ventricular
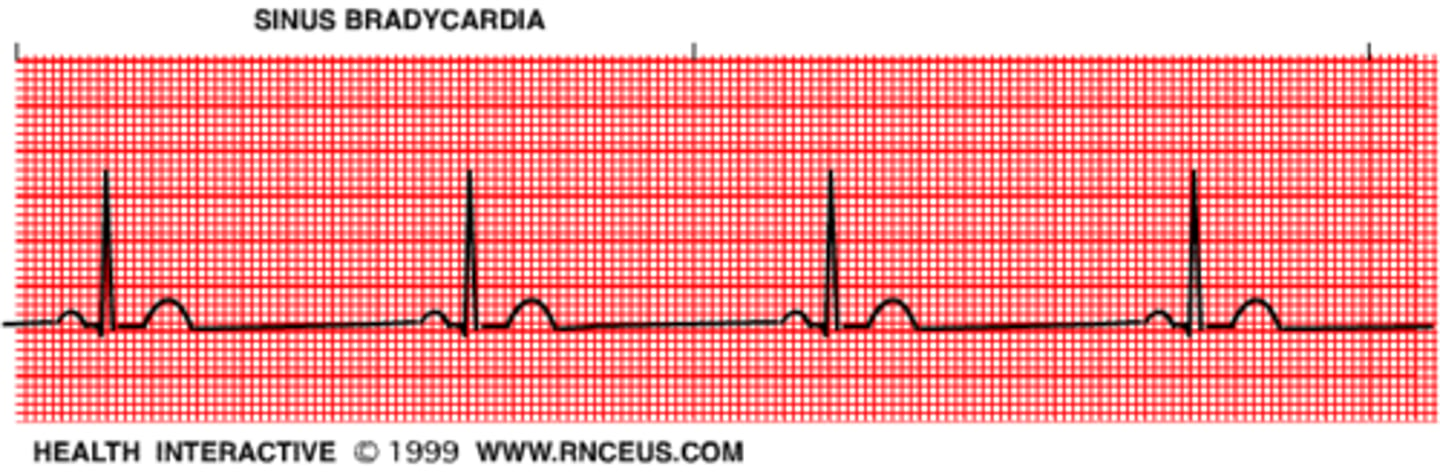
sinus bradycardia
slow rate, normal rhythm
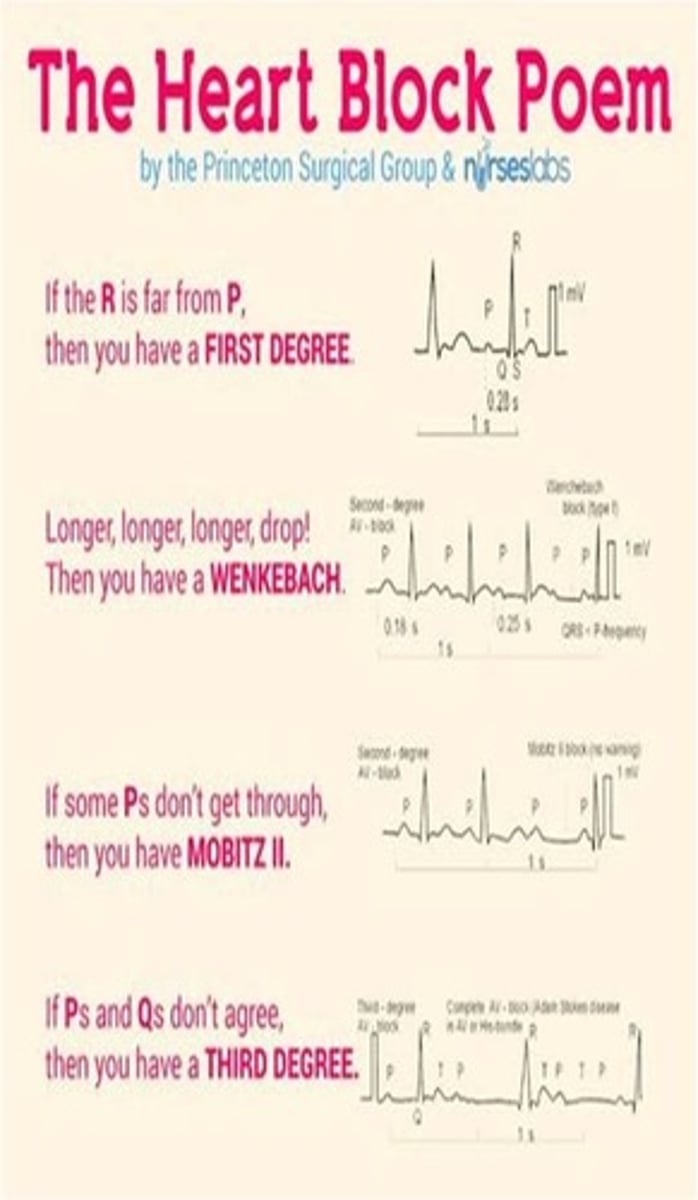
AV blocks
delay in conduction from AV nodes to ventricles; slow rate
- 1st degree: extended P-R interval
- 2nd degree: dropped QRS complex
- Mobitz type I: gradual prolongation of P-R before a block
- Mobitz type II: constant P-R interval before a block
- 3rd degree: complete block
- very slow HR, very wide QRS; no communication between atrium and ventricle
*2nd degree type II and 3rd degree may be indications for a pacemaker
bradycardia risks & symptoms
risks
- age
- ASCVD
- heart infection
- hypothyroidism
- inflammatory disease
- medications
symptoms
- syncope
- dizziness/ lightheadedness
- fatigue
- SOB
- chest pain
- confusion/ memory problems
medications that cause bradycardia
- beta blockers
- calcium channel blockers
- alpha antagonists (clonidine)
- anti-arrhythmics
- cardiac glycoside (digoxin)
- antipsychotics (lithium, amitriptyline)
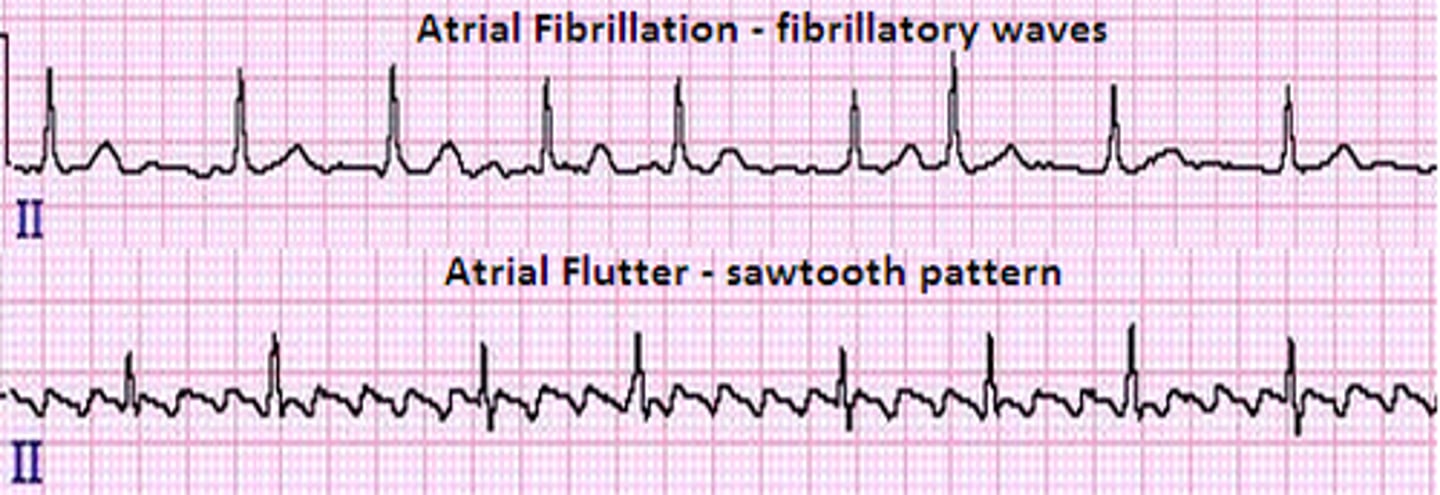
supra-ventricular tachycardia
SVT
rapid, regular heartbeats originating at or above the AV node
- atrial fibrillation (afib): atria quiver instead of normal beat
> no/ very coarse fibrillatory waves
- atrial flutter: atria depolarizes several times between each ventricular depolarization
> sawtooth
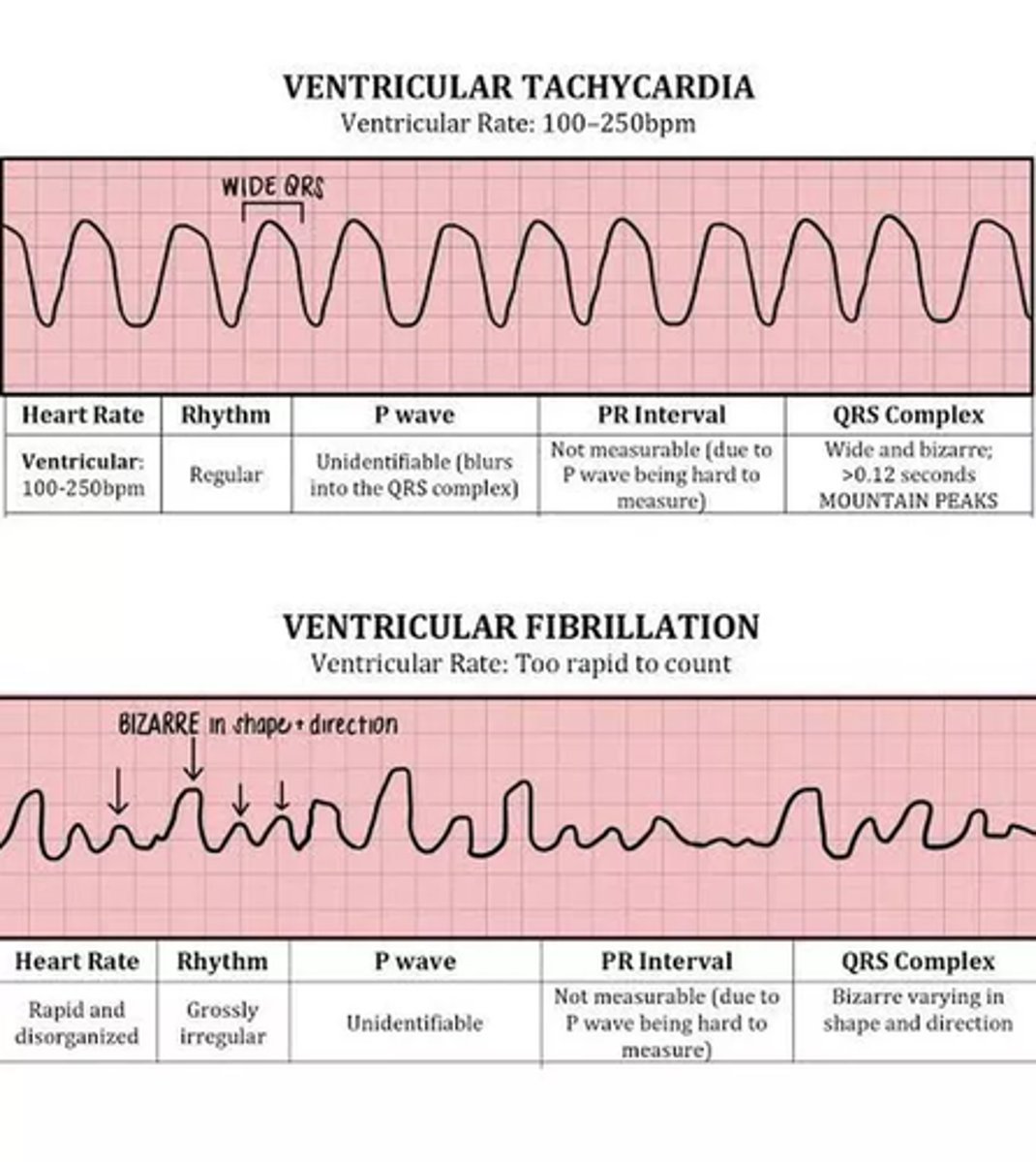
ventricular tachycardia
very rapid heartbeat beginning in ventricles
- sinus tach: fast rate, normal rhythm
- premature ventricular complex (PVC):
> 2 = couplet, 3 = triplet, 4 = V-tach
> common, only treated if bothersome
- V-tach: may be sustained (>30 beats/run) or non-sustained
> if pulseless, treat like V-fib
- V-fib: no squeeze (pulseless)
> cannot produce forward flow of blood
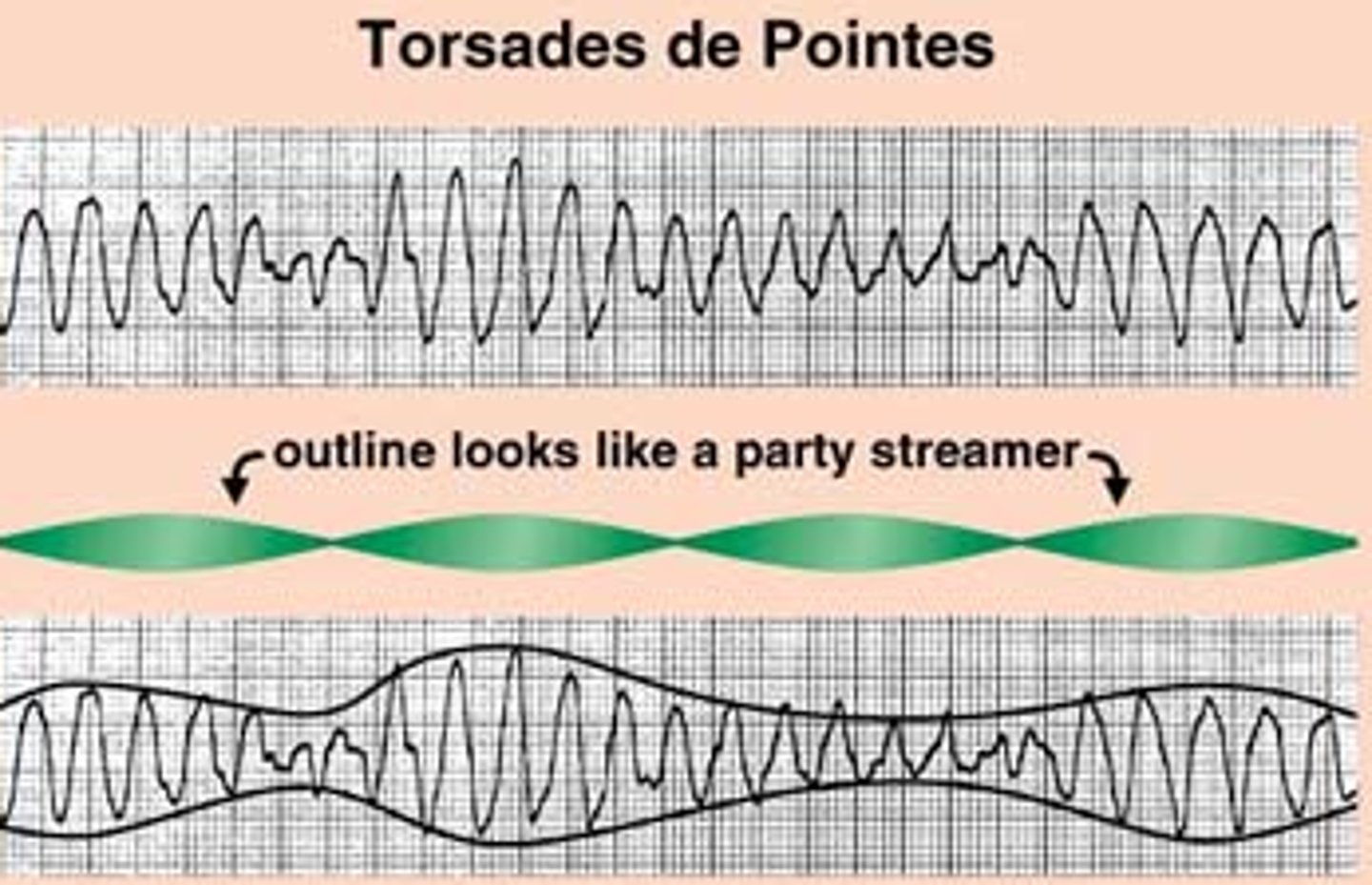
- Torsades de Pointes: result of prolonged QT interval, usually drug induced
Torsades de Pointes
- due to prolonged QT interval
possible causes:
- electrolyte abnormalities (hypo)
- stroke
- female
- liver/ renal disease
- cardiac conditions (congenital, LV dysfunction. myocarditis, SA/ AV block)
- drugs
drugs prolonging the QT interval
- macrolides
- fluoroquinolones
- fluconazole
- antiarrhythmics (amiodarone)
- antipsychotics (haloperidol, quetiapine)
- antidepressants (TCAs, SSRIs)
- ondansetron
- drugs causing hypokalemia/ hypomagnesemia
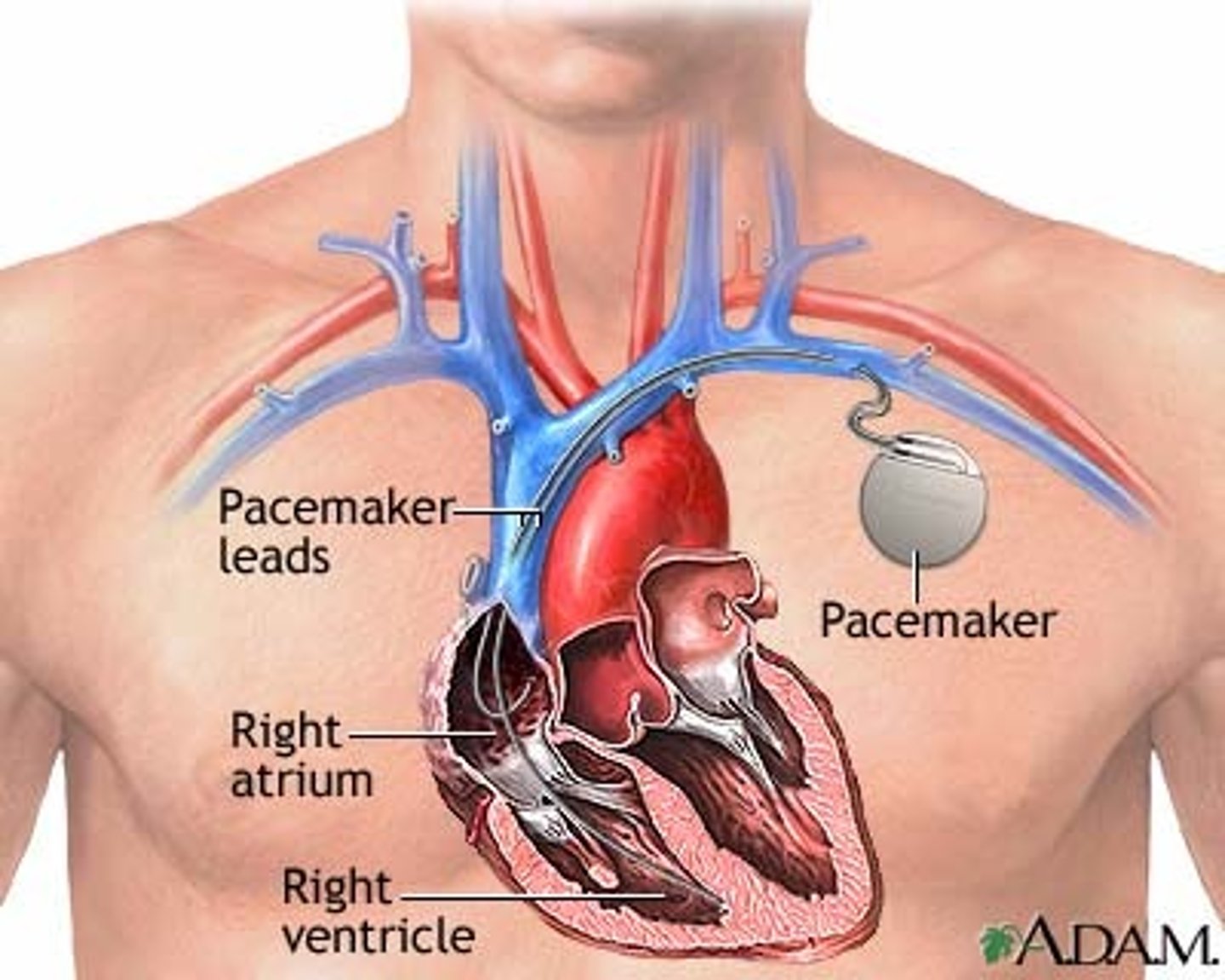
pacemaker implant
device that delivers electrical impulses to the heart to regulate the heartbeat