Ill Unit 5 (liver, endocrine)
1/32
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
33 Terms
jaundice
-yellow discoloration from abnormal bilirubin metabolism or bile flow
—most bilirubin is formed from Hgb breakdown (this is unconjugated, organs cannot filter it)
—liver makes and excretes conjugated bilirubin
-types
—hemolytic jaundice: d/t increased RBC breakdownn (SCD & other anemias, blood transfusions)
—hepatocellular jaundice: d/t liver unable to excrete bilirubin (hepatitis, cirrhosis, liver CA)
—obstructive jaundice: bile flow is obstructed through liver or biliary system (tumors, hepatitis, cirrhosis, stones, strictures, pancreatic CA)
causes clay-colored stools b/c no bile in intestine, dark urine b/c bilirubin ends up there
-best places to assess: sclera, palms, earlobes
hepatitis
-d/t virus, drugs (Tylenol, Tegretol, Zocor), ETOH, chemicals (arsenic, mercury), autoimmune
-reportable disease
-some people may only carry the virus w/o S/S
-5 types
—A & E are transmitted fecal-oral
—B, C, & D are transmitted percutaneous/parenteral (blood, intercourse, pregnancy)
-phases of S/S
—pre-icteric for 1-4 mo: no jaundice yet; anorexia, weight loss, HA, fever, nausea, RUQ pain, fatigue
—icteric for a few wks: jaundice, dark urine, clay-colored stools, malaise, fatigue, pruritis (from bile) GI S/S like pre-icteric
—post-icteric for 1-4 mo: no jaundice anymore
hepatitis care
-complications:
—A/E: none usually
—B/C/D: chroinc infection, liver CA, LF
-dx: Ab/Ag test (dx type), high bilirubin (serum & urine), high PT/INR/PTT (liver makes coagulation fx), high AST & ALT, high LDH
-vax for hep A and B (3 shots)
tx hepatitis
-acute tx:
—many meds must be avoided; also alcohol
—small frequent meals, high-carb, high-kcal, low-fat
—antiemetics
-chronic tx:
—antivirals to slow progression (Interferon: causes leukopenia)
—liver CA screen q6mo
—hepatitis Ab (IgG)
given to pt exposed to hepatitis
-standard precautions, private room
cirrhosis
-insidious onset, chronic progressive liver destruction
—liver cells are replaced w/ fibrous CT
-early S/S: anorexia, dyspepsia, flatulence, N/V
-later S/S: jaundice, peripheral edema/anasarka, ascites (d/t low albumin → low OP)
-other S/S: weight gain (fluid), encephalopathy, neuropathy, splenomegaly, abdominal pain/distention, angiomas, palmar erythema, pupura/petechiae
-causes varices, hematemesis, amenorrhea, impotence, pancytopenia, low Na+/K+/albumin
portal HTN
-complication of cirrhosis
—causes enlarged swollen veins d/t compression from fibrosis
—causes esophageal and gastric varices from increased BP → bleed risk
esp d/t low clotting fx
tx: IV vasopressin, ligation, Sengstaken-Blakemore tube inserted into esophagus to sxn & tamponade
—nursing: pt should avoid alcohol, ASA, certain foods, coughing (prevent/tx URI), NSAIDs
hepatic encephalopathy
-complication of cirrhosis
—d/t high ammonia levels (liver cannot convert into urea for excretion)
—causes change in mental responsiveness and disorientation
—nursing: restrict protein to prevent ammonia formation
—tx: lactulose (also a laxative!)
monitor mental status throughout day to assess med effectiveness
cirrhosis care
-dx: LFTs (AST, ALT, GGT), liver biopsy (bleed risk!), PT/INR/PTT, high albumin/bilirubin/ammonia
—EGD (esophageogastroduodenoscopy)
-tx: rest!
—pericentesis for ascites
empty bladder first (lengthy procedure), have pt lay still
—peritoneovenous shunt for portal HTN and varices
—Na+ restriction and diuretics (Aldactone) for edema
-nursing: oral hygiene, soft toothbrush (bleed risk) small frequent meals, high-Fowler’s (ascites causes dyspnea), skin care (turn q2h), avoid straining for stool, elevate edematous limbs & scrotum
—assess I&O, daily weights, abdominal girth
—safety concerns d/t encephalopathy (neuro assessments q2h)
liver CA
-early S/S like cirrhosis
-dx: US, CT, MRI, angiography, percutaneous biopsy
—ERCP (endoscopic retrograde cholangiopancreatography) to visualize pancreatic and bile duct; pt must lay still
—AFP (elevated d/t primary liver CA)
-need palliative care (poor prognosis: death w/in 6-12 mo)
-if CA is only in liver and has normal LFTs and portal BP, partial hepatectomy may treat
acute pancreatitis
-pancreatic enzymes are activated w/in pancreas (instead of small intestine) and auto-digest → bleeding
-usually d/t gallbladder disease, or alcoholism
—also biliary tract disease, viral infections, penetrating duodenal ulcers, CF, meds, smoking
-S/S: severe, deep, piercing, continuous abdominal pain in LUQ radiating to back, worsened by eating; N/V, tachycardia, jaundice, decreased or absent bowel sounds
—Grey Turner’s spots & Cullen’s sign
-complications: hTN; respiratory complications like pleural effusion, pneumonia, ARDS; hypocalcemia (→ tingling, tetany, Chvostek & Trousseau)
care for acute pancreatitis
-dx: elevated amylase and lipase, abdominal US, CT
-tx: drain pseudocyst or abscess to prevent rupture
—place pt NPO & give IVF
—analgesics (IV morphine)
—antispasmodics (Bentyl)
—remove gallstones or gallbladder
chronic pancreatitis
-d/t alcoholism
—also gallstones, tumors, trauma, CF
—may or may not follow acute pancreatitis
-S/S: abdominal pain that comes and goes, weight loss, mild jaundice, dark urine, steatorrhea
—leads to DM
care for chronic pancreatitis
-dx:
—elevated: amylase, lipase, bili, ALP, ESR, WBC
—CT, MRI, ERCP, stool analysis
-tx: NPO, then low-fat bland diet; avoid alcohol, nicotine, caffeine; small frequent meals, DM meds
—meds: Pancrease (enzyme), antacids, H2-blockers, PPIs, antidepressants (for neuropathic pain)
—surgery to divert bile flow:
via T-tube
via bile duct anstomosis into jejunum
via Roux-en-Y (panreatojejunostomy): pancreatic duct anastomosis into jejunum
pancreatic CA
-risk fx: smoking, chronic pancreatitis, DM, fam hx, high-fat diet, red meat
-S/S similar to pancreatitis: pain, jaundice, N/V, weight loss
-very poor prognosis (often metastasized at time of dx)
-tx: meds for N/V, opioids for pain, insulin, pancreatic enzymes; semi-Fowler’s
—chemo, radiation, surgery
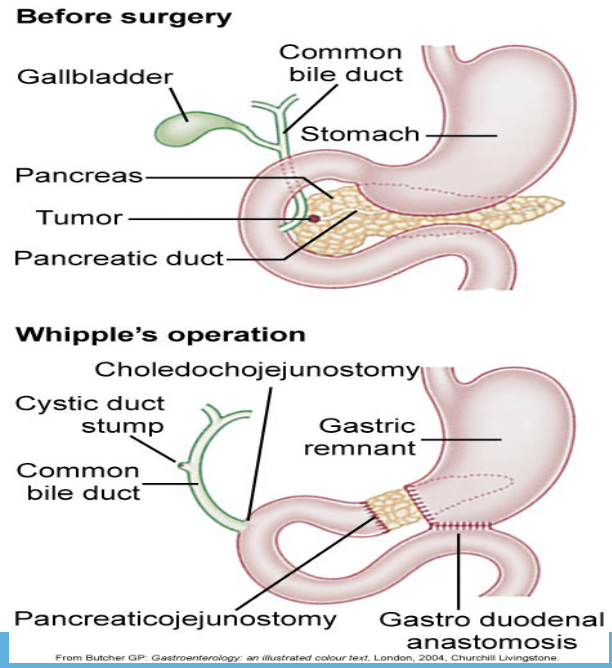
pancreatic cancer surgery
Whipple’s operation / radical pancreaticoduodenectomy
-resection of proximal pancreas, duodenum, distal stomach and distal common bile duct
-anastomosis created between pancreatic duct, common bile duct, and stomach to jejunum
cholelithiasis and cholecystitis
-S/S: severe RUQ pain (worse after high fat meal)
-may lead to pancreatitis
-dx: US, ERCP, HIDA scan
-tx: low-fat high-fiber diet, clear liquid diet
—anticholinergics
—shock-wave lithotripsy
—laparoscopic or incisional cholecystectomy
levothyroxine / Synthroid / Levoxyl
-TH replacement
-100-400 mcg/day (start out 25-50 and gradually increase)
-usually oral, but can be IV for rapid replacement (1/2 dose)
-give 1 hr before breakfast or 2 hr after
-take for life
-nursing: monitor HR & BP, monitor for AEs and allergic reactions, monitor thyroid labs, check other meds
problems with levothyroxine
-AEs: irritability, insomnia, HA, tremors, tachycardia, arrythmias, N/V/D, appetite change, weight loss, hair loss
—report immediately: chest pain, palpitations, nervousness
-contra: maybe ASA allergy
goiter
-thyroid cells are hyper- or hypoactive
-d/t lack of iodine or TH
-dx: TSH, T4
-tx underlying cause
hyperthyroidism
-increase in T3 and T4 levels
-more common in women
-d/t pituitary problems, stress, autoimmune, excess iodine intake
-often d/t Grave’s disease
—autoimmune idiopathic: Ab created against TSH receptor sites → thyroid enlargement
-S/S: enlarged thyroid, heat intolerance, fine straight hair, exopthalmosis, facial flushing, tachycardia, high SBP, breast enlargement, weight loss, muscle wasting, local edema, clubbing, tremors, diarrhea, amenorrhea
hyperthyroidism care
-dx: low TSH, free T4, US, thyroid scan
—EKG (tachycardia, A-fib)
—RAIU: radioactive iodine uptake (rules out Graves)
contra: pregnancy
-diet: high-kcal high-carb high-protein snacks, no caffeine
-meds: propylthiouracil, methimazole/Tapazole, iodine (SSKI), beta blockers
-tx: radioactive iodine therapy (RAI), thyroidectomy
RAI
-destroys thyroid tissue
-done for 2-3 months
-oral
-combine w/ meds
-may cause hypothyroidism
-pregnancy test before
thyroidectomy
-subtotal: 90% removed and 10% regenerated
-for goiter compression, pt unresponsive to antithyroid meds, thyroid CA
-post-op complications: hypothyroidism, hypoparathyroidism, hypocalcemia, hemorrhage, laryngeal nerve famage, infection, thyrotoxic crisis, airway obstruction
hypothyroidism
-causes everything in body to slow down
-d/t:
—primary: destruction of thyroid tissue or defective hormone synthesis
—seondary: pituitary disease decreases TSH, hypothalamus dysfunction decreases TRH
-S/S: cold intolerance, receding hairline and hair loss, facial and periorbital edema, dull-blank expression, extreme fatigue, thick tongue and slow speech, anorexia, brittle nails and hair, mentrual problems, lethargy, apathy, dry scaly skin, muscle aches and weakness, constipation
-late S/S: hypothermia, bradycardia, wieght gain, decreased LOC, thickened skin, heart problems
-*often S/S are similar to aging
myxedema coma
-complication of hypothyroidism
-medical emergency
-triggered by infectino, narcotics, trauma
-causes sudden onset of depressed body system processes
-decreased CO, hypothermia, hTN, respiratory depression, bradycardia, stupor
-tx: IV Synthroid, treat underlying cause
care for hypothyroidism
-dx: TSH, T4, EKG
-tx: lifelong levothyroxine, warm environment, skin care, prevent constipation, daily weights, avoid fatigue
Cushing Syndrome
-d/t prolonged steroid intake, ACTH-secreting pituitary tumor, cortisol-secreting neoplasm
-S/S: thin hair/skin/SQ, red cheeks, supraclavicular fat pad, muscle atrophy, acne, moon face, increased body hair, weight gain, purple striae, pendulous abdomen, easy bruising, slow wound healing
care for Cushing Syndrome
-dx: high cortisol, high Na+, low K+, high BGM
—CBC, 24-hr urine collection (cortisol)
—CT & MRI (adrenal atrophy; lesions on pituitary, adrenal, lung, GI, pancreas
-tx; reduce steroids gradually
-nursing: limit sodium, increase potassium and protein, I&O, daily weights (hypervolemia risk), prevent infections, exercise
tx for Cushing
—“medical adrenalectomy” (Mitotane to kill adrenals)
—adrenalectomy (→ infection risk)
need UA QD to check cortisol
—transphenoidal hypophysectomy (remove pituitary adenoma)
post-op: elevate HOB, oral care q2h, assess nasal drainage
adrenocortical insufficiency
-hypofunction of adrenal cortex
-d/t pituitary or hypothalamus issues, Addison’s disease (autoimmune)
-insidious onset
-S/S (late): fatigue, weakness, weight loss, hypovolemia
-Addison’s S/S: bronze skin, body hair distribution changes, GI problems, hypoglycemia, ohTN
complications of adrenocortical insufficiency
Addison’s crisis
-rapid onset life-threatening emergency
-triggered by trauma, dehydration, stress, infection, surgery, steroid withdrawal
-S/S: tachycardia, hTN, hyperkalemia, hyponatremia, fatigue, dehydration
—kidneys shut down, CVS collapses
-tx: IV hydrocortisone, IVF, Kayexalate
—monitor BP, VS, EKG carefully
care for Addison’s
-tx: lifelong corticosteroids (prednisone) and mineralcorticoids (Florinef)
—higher dose during stress
-sodium (during excess heat)
-teahcing: keep emergency IM hydrocortisone on hand, wear medical alert band
pheochromocytoma
-tumor of adrenal medulla that produces excess catecholamines
-dx: 24-hr urine collection (shows catecholamines and creatinin)
-tx: surgery
—pre-op: do NOT palpate abdomen; monitor HR, BP, EKG
—prevent BP and tachycardia
—need lifelong hormone replacement, glucocorticoids, mineralocorticoids