BIO-375 Exam #2
1/88
Earn XP
Description and Tags
Unit 2- Sensory Systems
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
89 Terms
Dorsal Column/Medial Lemniscus (Epicritic) Tract
The sensation of vibration, fine touch, and tactile
Starts with mechanoreceptors
Spinothalamic/Anterolateral (Protopathic) Tract
The sensation of temperature, pain, itch, and tickle.
Starts with free nerve endings
Proprioceptive
The body’s internal sensation of spatial awareness, position, and movement.
Directly communicates with cerebellum
Mechanoreceptors
Specialized sensory receptors that convert mechanical stimuli (touch, stretch, pressure, vibration, etc.) into nerve impulses.
Found in different parts of the body
Receptor Neuron
The primary afferent neurons
The cell body is located in the dorsal root ganglia
Pseudo unipolar neuron (two branches- peripheral and central branches)
Heavily myelinated - fast conduction velocity (↑R)
High Resolution
Is the resolution higher or lower when there is a large density of receptors with small receptive fields?
Transduction
The conversion of mechanical stimuli into electrical impulses.
Stretch receptors cause ion channels to open, causing depolarization
Receptor Potential
The initial electrical response to a mechanical stimulus.
Graded potential - amplitude dependent on the strength of the stimulus
If the stimulus is strong enough to reach the threshold, it will generate an action potential
Fast Adapting Receptors
Receptors that respond to changes in stimuli and are essential for detecting dynamic environmental changes.
Slow Adapting Receptors
Receptors that respond continuously to a stimulus and provide sustained information about a static stimulus.
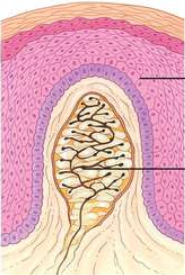
Merkel Discs/Receptors
Slow-adapting mechanoreceptors that are important for detecting form, texture, edges, and light touch.
Only receptor cells located in the epidermis
Highest spatial resolution
Highest density in glabrous tissue

Meissner (Tactile) Corpuscles
Rapid adapting mechanoreceptors that are important for detecting movement across the skin, slippage, light touch, and high-frequency vibration
4x more sensitive than Merkel discs
Small receptive fields, but larger than Merkel discs
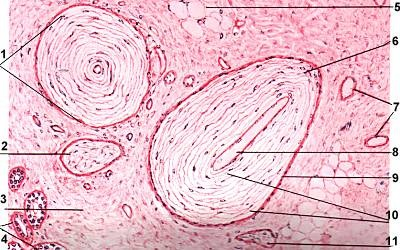
Pacinian (Lamellar) Corpuscle
A fast-adapting and extremely sensitive mechanoreceptor that is important for detecting gross pressure changes and vibration.
Very large receptive fields
Very common throughout the body
Ruffini (Bulbous) Corpuscle
A slow-adapting mechanoreceptor that is responsible for detecting skin stretch and finger position/movement.
Connected with proprioception

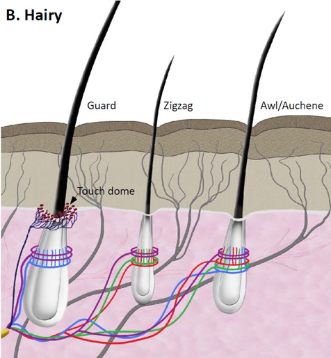
Circumferential Lanceolate Endings
A type of hairy skin mechanoreceptor that is slow-adapting and detects light touch and hair movement.
Light purple
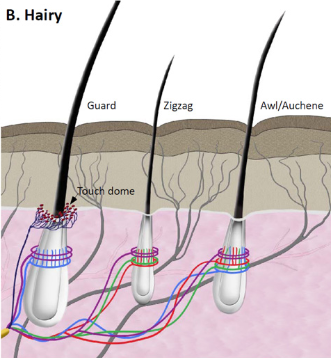
Longitudinal Lanceolate Endings
A type of hairy skin mechanoreceptor that is rapidly-adapting and detects hair deflection, hair movement, and directional discrimination.
Blue, green, and red
Proprioceptors
Mechanoreceptors that are responsible for detailed continuous information essential for complex movements and to prevent injury (reflexes)
Unconscious of it majority of the time
Very low threshold
Very wide and heavily myelinated axons
Types:
Muscle Spindles
Golgi Tendon Organs
Modified Ruffini
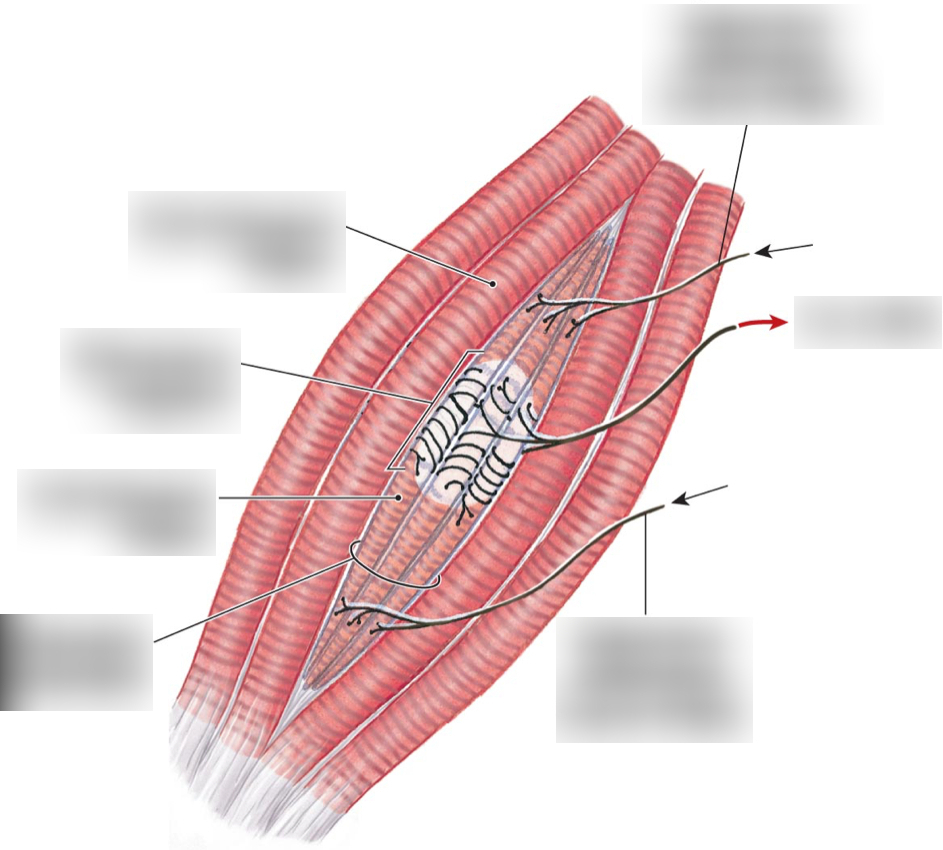
Muscle Spindle
A type of proprioceptor that detects the length and stretch of muscles
Moves with the muscle
Has its own motor neuron
Has 2-3 afferent (sensory) neurons that detect dynamic info (changes in length) and static info (constant length)
Run parallel to muscle fibers
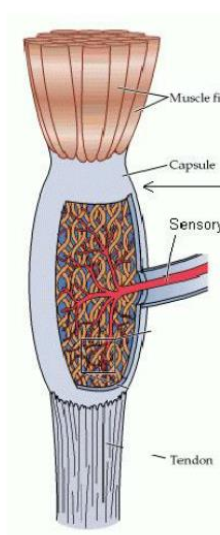
Golgi Tendon Organs
A type of proprioceptor that monitors both muscle tension and force and is made of collagen and sensory fibers.
Runs in series with the muscle and is located in the musculotendinous junction
Modified Ruffini
A type of proprioceptor that detects the position/angles of a joint
Joint receptor
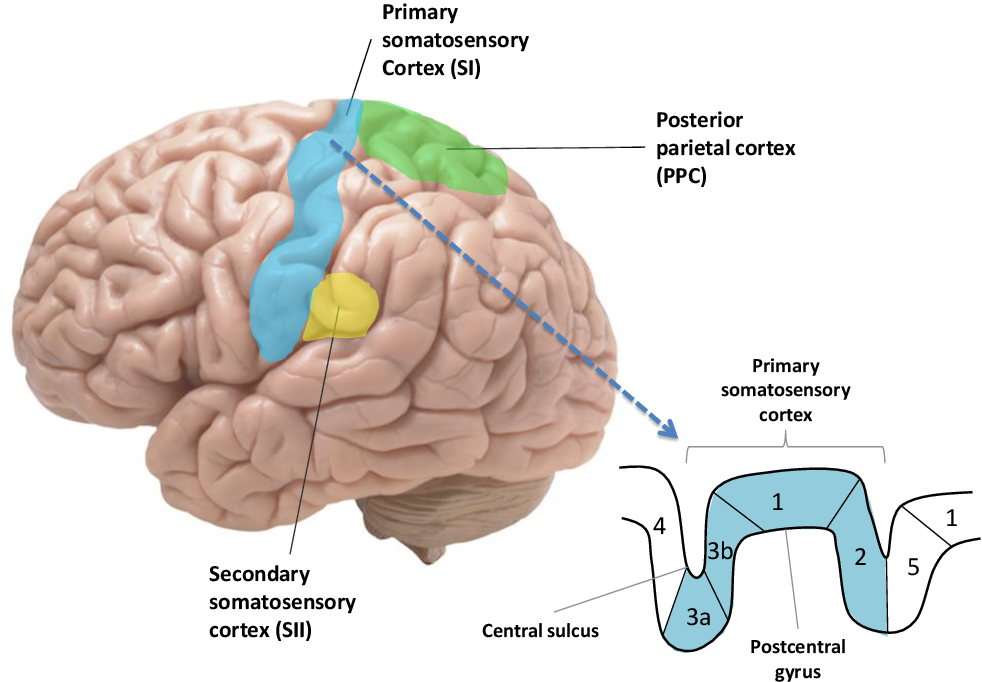
Area 3a
What area(s) of the primary somatosensory cortex does position sense/proprioception?
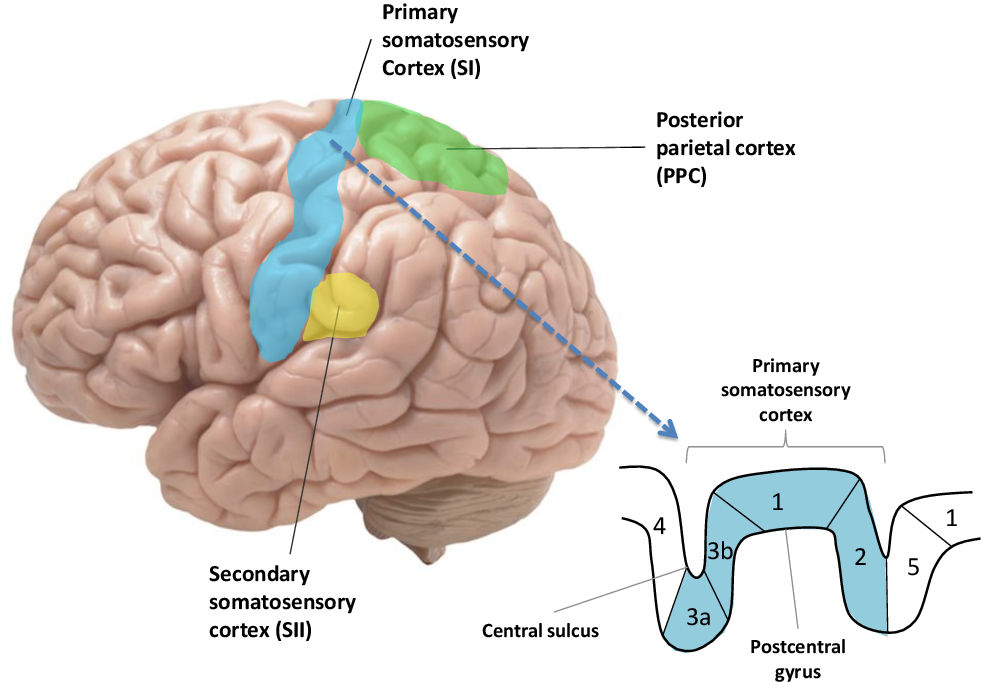
Areas 3b and 1
What area(s) of the primary somatosensory cortex is concerned with cutaneous stimuli?
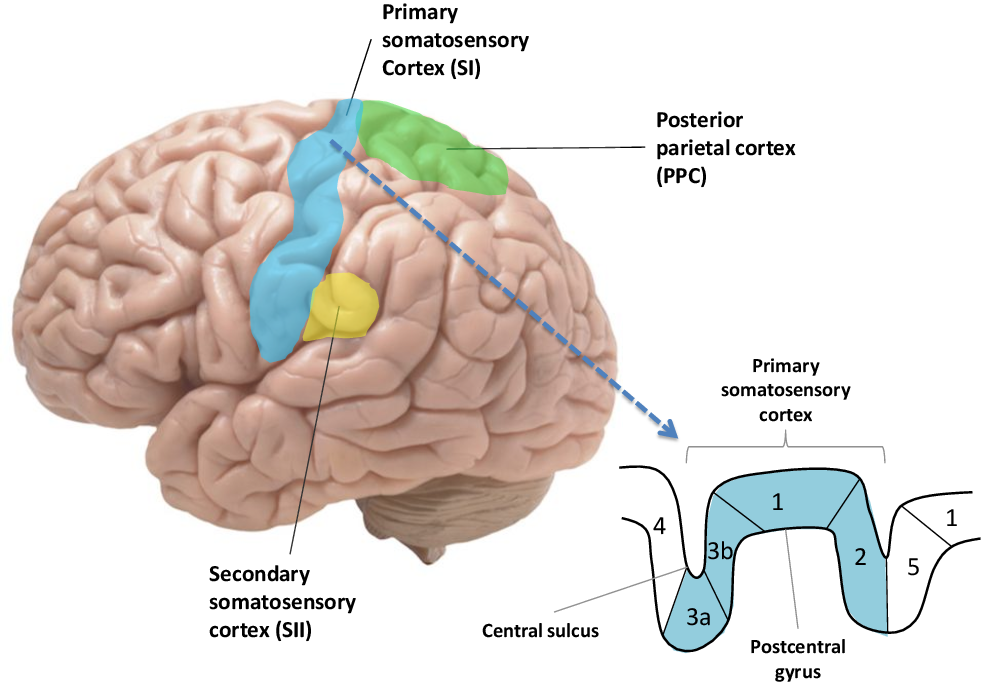
Area 2
What area(s) of the primary somatosensory cortex is responsible for tactile and proprioceptive information?
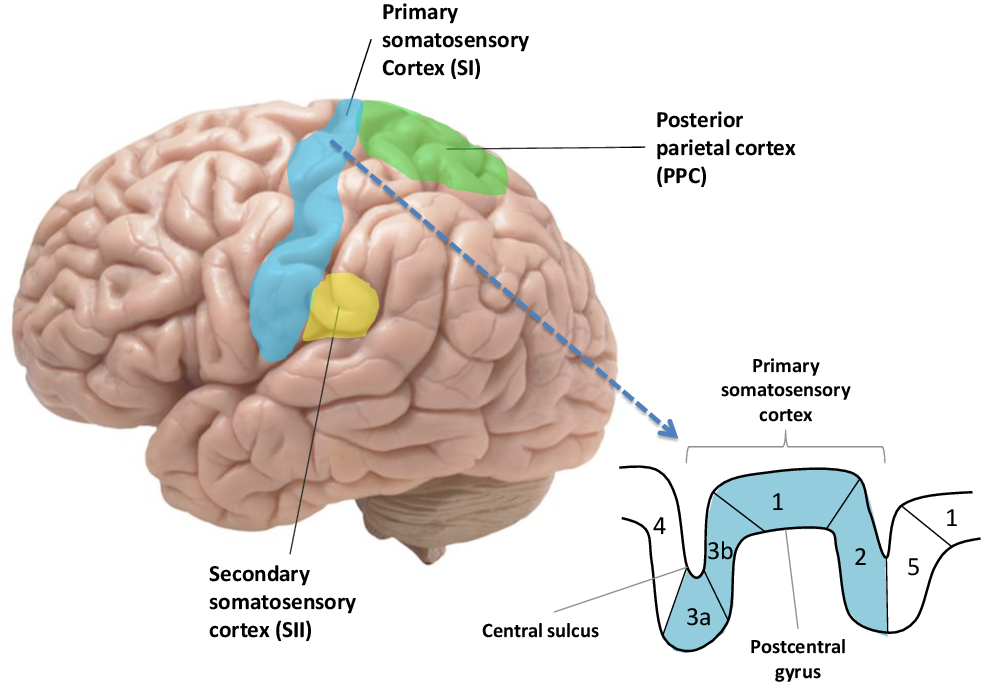
Area 1 and 2
Where does Area 3b send its information to?
General Body
What part of the body does sensory information get sent to the VPL of the thalamus?
Face/Head
What part of the body does sensory information get sent to the VPM of the thalamus?
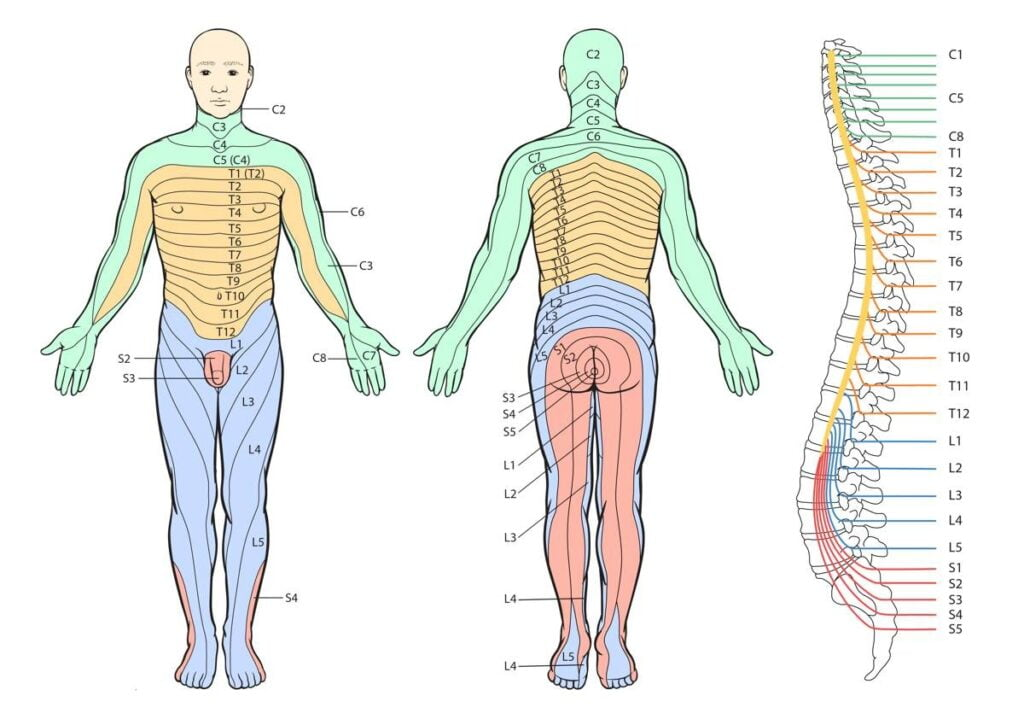
Dermatomes
A spinal root exists on each side of the spinal cord at every level of the spinal cord and each represents a _________.
Sensory!
Plasticity
The brain’s ability to rewire itself and try to recover from injury/illness.
Allows us to learn new skills
Study with primates where finger usage was mapped out on the brain, the third digit was removed, and the other fingers took over that area of the brain
Pain
Physical suffering or discomfort caused by illness or injury
Our perception of a stimulus
Experienced differently for everyone
Exists to remove oneself from harmful situations, to protect damaged tissues, and to learn to avoid similar occurrences.
Can become maladaptive/pathological- Chronic
Nociception
The detection of the stimulus that causes pain
Neural pathway = Spinothalamic/Anterolateral (Protopathic)
Nociceptors
Receptors made up of free nerve endings that are used to detect potentially damaging thermal, chemical, or mechanical stimuli
In epidermis
Peripheral pain receptors
Very high threshold (damaging heat detected around 45 °C
Axons are lightly myelinated or not myelinated
Very slow
Tightly wired to reflexes- signal only has to travel to the spinal cord
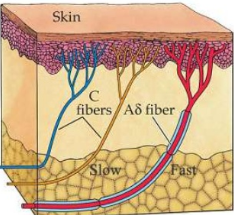
Aδ Fibers
Type of nociceptor fiber that corresponds to the first pain, which is tingling or sharp pain, and is more rapid than the other (has a thin layer of myelin)
Type 1- sensitive to mechanical and chemical stimuli
Type 2- sensitive to thermal (noxious) stimuli
C Fibers
Type of nociceptor fiber that corresponds to the second pain which is delayed/diffuse (no myelin), characterized as a dull ache or a burning sensation
Some of these fibers are polymodal - detect mechanical, chemical, and thermal stimuli
Some are specific - detect only one type of stimuli
Superficial Somatic
A type of pain/nociception that is the easiest to localize and treat.
Ex. Scrape on the skin
Deep Somatic
A type of pain/nociception that is more difficult to determine the exact location and more difficult to treat.
Ex. Pulled muscle
Visceral
A type of pain/nociception that is always diffuse, the most difficult to locate and treat, and causes referred pain
Low resolution
Need imaging/testing to determine
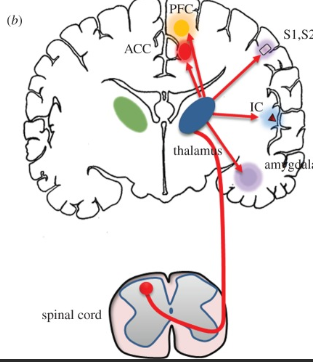
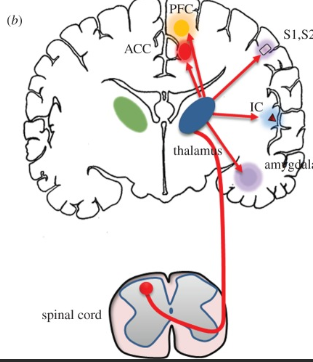
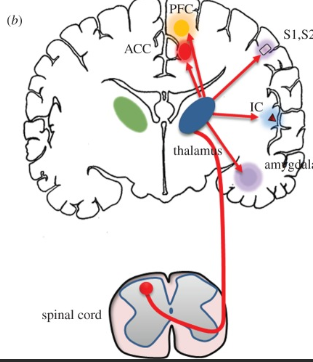
Main Pain Pathway
Emotional/Memory Pathway
Descending Pathway (can +/- pain signals)
What are the three components to the pain pathway?
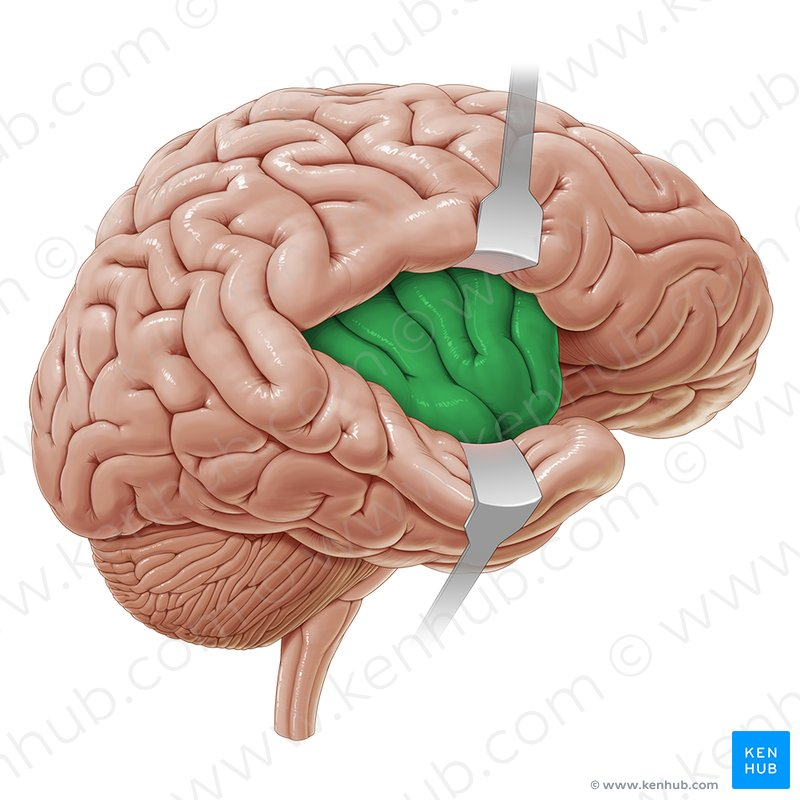
Insular Cortex
Part of the pain pathway that is located in the cortex and is responsible for the perception of the quality of the pain.
Hint: IC
Anterior Cingulate Cortex
Part of the pain pathway that is responsible for the emotional status when experiencing pain.
Hint: ACC
Hippocampus
Part of the pain pathway that is responsible for creating new memories based on a pain experience.
Hint: HC
Amygdala
Part of the pain pathway that is responsible for plasticity and emotions such as fear and anxiety.
Periaqueductal Grey
Part of the pain pathway that is located in the midbrain and is responsible for inhibitory output (try to lessen nociceptor signal)
Hint: PAG
Medulla
Part of the pain signal that works to either increase of decrease the nociceptor signal
Hint: NRM
Spinal Input
thalamus
Nociceptor Signal
What components of the pain pathway make up the MAIN pain pathway?
Amygdala
Insular Cortex
Anterior Cingulate Cortex
What components of the pain pathway make up the Affective-Motivational Part?
Periaqueductal Gray
RVM (Medulla)
What components of the pain pathway make up the descending part?
Gate Theory of Pain
The idea that stimulation of other parallel mechanoreceptors will make the pain feel somewhat better
Ex. rubbing or squeezing the toe after stubbing it
Hyperalgesia
When something that wouldn’t normally cause a significant amount of pain does because of sensitization.
Increase in both stimulus intensity and pain intensity
Allodynia
When something that normally is non-noxious (doesn’t cause pain) does cause pain because of sensitization.
Increase in both stimulus intensity and pain intensity
Sensitization
An inflammatory response/signal after the first pain/initial injury lowers the threshold of the nociceptors, causing the stimulus intensity and pain intensity to increase.
Use-Dependent Plasticity
What type of sensation of pain without stimulus is this?
Caused by a severe traumatic injury that took a long time to heal
Synapses along the pain pathway were strengthened (central sensitization)
Neuropathic Pain
What type of sensation of pain without stimulus is this?
Caused by a lesion or disease of the somatosensory system (damage to neurons along the pathway)
Ex. Central Neuropathy- stroke, neurodegenerative diseases, spinal cord injury, syringomyelia, MS
Ex. Peripheral Neuropathy- trigeminal neuralgia, diabetic neuropathy, HIV infection, chemotherapy
Autoimmune Disorders
What type of sensation of pain without stimulus is this?
Chronic inflammation
Ex. Rheumatoid Arthritis, Lupus, etc.
Acute Pain
Which pain is the easiest to treat?
Chronic vs. Acute vs. Neuropathic
Neuropathic Pain
Which pain is the most difficult to treat?
Chronic vs. Acute vs. Neuropathic
Breakthrough Pain
Activity-related pain that is common in cancer patients
Some level of pain was already being managed, but then it gets worse with changing activity
NSAIDs
Drugs used for pain relief and to try to stop the inflammatory response after injury that target the enzyme that produces prostaglandins (part of the inflammatory response)
Ex. Ibuprofen, Aspirin, Naproxen, Celebrex, Meloxicam
Enzyme = Cox (Cyclooxygenase)
Cox also found in other places (Cox1), so taking a lot of this medication can be damaging (Ex. cause ulcers)
Some prescription medications made to only target Cox2
Opioids/Opiates
Drugs used for pain relief that bind to specific receptors that are found all throughout our body/pain pathway
μ (mu) receptors
Ex. Morphine, Codeine, Oxycodone
Receptors found in both the pre-synaptic terminal and post-synaptic cell
Difficult for pain signal to go through
Congenital Insensitivity to Pain
The inability to feel pain
Rare genetic disorder
Very dangerous because you won’t know if you are injured or have an illness like appendicitis
Saccades
Rapid, jerky, ballistic movements of both eyes in the same direction.
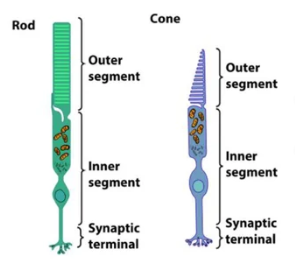
Photoreceptors
Specialized cells located in the retina of the eye are crucial for detecting light, and they play a critical role in phototransduction
Two Types
Rods
Cones
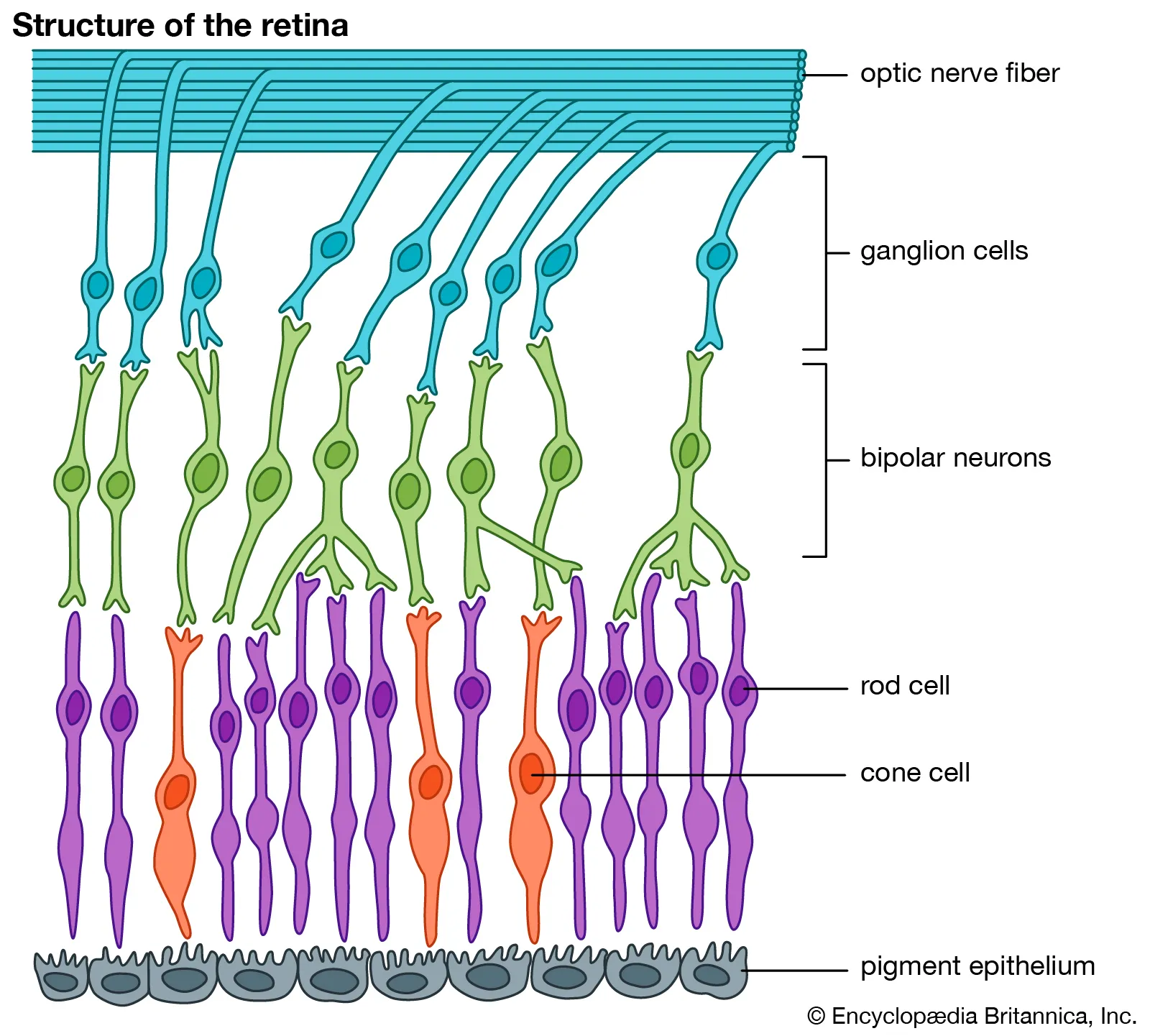
Vertical Pathway of Retina
A series of connections in the retina
Photoreceptors (GP) connect to →
Bipolar Cells (GP) connect to →
Ganglion Cells (AP)
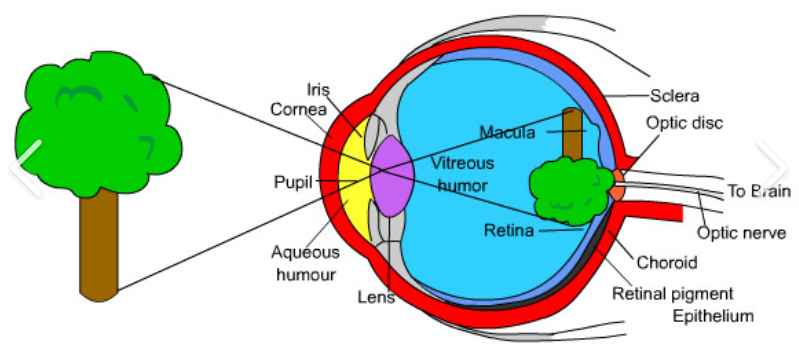
Refraction
Visual information appears in the neural retina as upside down and backwards
Phototransduction
The conversion of photons into electrical signals
Occurs in the outer segment
The outer segment of photoreceptors contains discs with 100s of opsins that detect photons
1) Depolarized
2) More Neurotransmitter
If a room is super dark, will the cell be
1) Depolarized OR Hyperpolarized
2) Release More OR Less Neurotransmitter
***Dark = Max influx of Na+/Ca2+ into the cell
1) Hyperpolarized
2) Less Neurotransmitter
If a room is super bright, will the cell be
1) Depolarized OR Hyperpolarized
2) Release More OR Less Neurotransmitter
***Dark = Max influx of Na+/Ca2+ into the cell
11-cis retinal → 11-trans retinal
When a photon strikes the opsin, what gets converted?
Opsin activated
Transducin
After the activation of opsin in the transduction pathway, what gets activated next via phosphorylation?
Transducin α-Subunit activates PDE
After the activation of transducin via phosphorylation in the phototransduction pathway, what subunit of transducin activates what?
Hydrolyze cGMP → GMP
In the phototransuction process, what does the activated PDE do?
Na+/Ca2+ Channel Closes
What happens when cGMP is hydrolyzed into GMP during the phototransduction pathway?
Hyperpolarization and Less Neurotransmitter Released
When the Na+/Ca2+ channel closes, there is decreased Na+/Ca2+ entering the cell, which leads to what?
Light Adaptation
The rapid adjustment of the human visual system that allows us to see a wider variety of luminescence.
Rhodopsin Kinase phosphorylates Rhodopsin
Arrestin binds to phosphorylated Rhodopsin which shuts it down
How is phototransduction stopped?
Guanylate Cyclase
Rhodopsin Kinase
Binding affinity for cGMP and Na+/Ca+ Channel
What three things is calcium inhibitory towards according to light adaptation?
More Difficult
If there is a decrease in [Ca2+] in the photoreceptor, is it easier or more difficult for the Na+/Ca+ channels to close per photon?
Increase in Guanylate Cyclase activity - increase cGMP
Increase in Rhodopsin Kinase activity - more arrestin binding
Increase in cGMP-Na+/Ca+ channel affinity
Decrease in the rate of closing Na+/Ca+ channels
A decrease in [Ca2+] in the photoreceptor leads to what four things occurring in the photoreceptor?
Scotopic Phase
The phase of vision where only rods are used, at the lowest levels of light intensity.
Mesopic Phase
The phase of vision that uses both cones and rods and is during medium light intensity.
Photopic Phase
The phase of vision where only cones are being used because the rods have fully saturated. This is at very high levels of light intensity.
Rods
A type of photoreceptor that has:
Higher sensitivity
Larger receptive field size and lower spatial resolution
Less effective at light adaptation
Slower recovery from saturation
More in number in the retina
Dominate monochrome and peripheral vision
Cones
A type of photoreceptor that has:
Lower sensitivity
Smaller receptive fields and higher spatial resolution
More effective at light adaptation
Faster recovery from saturation
Less in number in the retina
Concentrated in the fovea
Responsible for color vision and fine detail
Color Vision
The type of vision produced by the three types of cones
Short cones (blue)
Medium cones (green)
Long cones (red)
What are the three types of cones and their perspective colors?
Information from at least 2 different cones is compared
How is color perceived?
Color Opponency
The visual system’s mechanism of processing colors in opposing pairs, such as red vs. green and blue vs. yellow, enhancing color contrast and discrimination.
Retinoid Cycle
The retinal pigmented epithelium (RPE) absorbs stray light and is critical for the survival of photoreceptors. It also takes 11-trans retinal and recycles it back into 11-cis retinal to be used by the photoreceptors again.
Off-Center Bipolar and Ganglion Cells
In bright lighting, photoreceptors are hyperpolarized, and smaller amounts of neurotransmitter will be released and will go to the bipolar cells. This bipolar cell pathway will respond the same way the photoreceptor did and hyperpolarize, therefore releasing smaller amounts of neurotransmitter to the ganglion cell, which will then create more less action potentials.
On-Center Bipolar and Ganglion Cells
In bright lighting, photoreceptors are hyperpolarized, and smaller amounts of neurotransmitter will be released and will go to the bipolar cells. This bipolar cell pathway will respond opposite than the photoreceptor did and depolarize, therefore releasing larger amounts of neurotransmitter to the ganglion cell, which will then create more more action potentials.