KAAP 310 Unit 3 (only urine)
1/112
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
113 Terms
urinary system
2 kidneys
2 ureters
urinary bladder
urethra
Functions of kidneys
primary function is excretion
Blood filtration and excretion of toxic metabolic wastes
Regulation of blood volume, pressure, and osmolarity by regulating water output
Regulation of electrolyte and acid base balance of body fluids
Secretion of erythropoietin - stimulates production of RBCs and supports O2 carrying capacity of blood
Regulation of calcium homeostasis and bone metabolism through calcitriol synthesis
Clear hormones and drugs from the blood - limiting their action
Detoxification of free radicals
Help support blood glucose level through synthesis of glucose from amino acids in cases of extreme starvation
Waste
any substance that is useless to the body or present in excess of the body’s needs
Metabolic waste
waste substance produced by the body
nitrogenous wastes
small nitrogen containing compounds
the most toxic of our metabolic wastes
50% of nitrogenous waste is urea (byproduct of protein catabolism)
other nitrogenous wastes include:
uric acid- produced by catabolism of nucleic acids
creatinine- byproduct of creatine phosphate catabolism
both less toxic than ammonia but must be eliminated due to potential harm
How are nitrogenous wastes created?
proteins hydrolyzed into amino acids
NH2 group is removed from each amino acid
-NH2 forms ammonia (exceedingly toxic)
Liver converts ammonia to urea (CO(NH2)2 (less toxic)
BUN
blood urea nitrogen
level of nitrogenous waste in the blood
typical concentration 10-20 mg/dL
azotemia
elevated BUN that can indicate renal insufficiency
can progress to uremia - syndrome of diarrhea, vomiting, dyspnea, and cardiac arrythmia stemming from the toxicity of nitrogenous wastes
Excretion
process of separating wastes from the body fluids and eliminating them from the body
carried out by 4 body systems
Respiratory
excretes CO2, small amounts of other gases, and water
Intergumentary
excretes water, inorganic salts, lactate, and urea in sweat
Digestive
eliminates food residue
excretes water, salts, CO2, lipids, bile pigments, cholesterol, and other metabolic wastes
Urinary
excretes a broad variety of metabolic wastes, toxins, drugs, hormones, salts, H+, and water
Gross anatomy of kidney
lateral surface is convex
medial surface is concave with a slit (hilum)
hilum
admits renal nerves, blood vessels, lymphatics, and ureter
What layers of connective tissue protect the kidneys
renal fascia
immediately deep to the parietal peritoneum
binds kidney and associated organs to abdominal wall
perirenal fat capsule
layer of adipose tissue
cushions kidney and holds it in place
fibrous capsule
encloses the kidney
protects from trauma and infection
what are the kidneys suspended in?
collagen fibers
renal parenchyma
glandular tissue that forms urine
C shape in frontal section
encircles renal sinus
divided into 2 zones divided by the corticomedullary junction
renal cortex (outer)
extend into renal columns
renal medulla (inner)
divided into renal pyramids
bases of pyramids face cortex
blunt point of pyramids (renal papilla) face the sinus
renal sinus
cavity occupied by blood and lymphatic vessels, nerves, and urine-collecting structures
adipose tissue fills remaining space
minor calyx
surrounds papilla of each renal pyramid
collects urine
combine with 1-2 others to form major calyx
2-3 major calyces converge in sinus to form renal pelvis
ureter
tubular continuation of the renal pelvis that drains the urine down to urinary bladder
glomerulus
spheroidal mass of blood capillaries in the kidney that filters plasma and produces glomerular filtrate - further processed into urine
how much blood do kidneys receive in a minute?
1.1 L
21% of cardiac output - renal fraction
mostly meant to remove waste than to meet kidney tissue’s metabolic demands
Circulation to Kidneys
a renal artery supplies each kidney
aorta → renal artery → segmental artery → interlobar arteries → arcuate arteries → cortical radiate (interlobular) arteries →
finer branches
→ afferent arterioles → glomerulus → efferent arteriole → (mostly) peritubular capillaries/(1-2%)vasa recta →
veins
→ cortical radiate (interlobular) veins → arcuate veins → interlobar veins → renal vein → inferior vena cava
renal tubule
reabsorbs most of water and solutes that filter out of the blood at the glomerulus
returns them to the bloodstream through network peritubular capillaries around the nephron
vasa recta
network of vessels that supply 1-2% of total renal blood flow to the renal medulla
its capillaries carry away water and solutes reabsorbed by the sections of the tubule they’re at
how many nephrons does each kidney have?
1.2 million wow
parts of a nephron
renal corpuscle - filters blood plasma
renal tubule - converts filtrate to urine
Renal Corpuscle
consists of glomerulus and the glomerular capsule that encloses it
parietal (outer) layer - simple squamous
capsular space - filtrate collecting separation
visceral (inner) layer - podocytes wrapped around capillaries of glomerulus
glomerular capsule
double walled capsule around each glomerulus of the kidney
receives glomerular filtrate and empties into the proximal convoluted tubule
vascular pole
afferent arteriole enters capsule
brings blood to glomerulus
efferent arteriole leaves capsule and carries blood away
urinary pole
parietal wall of capsule turns away from the corpuscle and gives rise to renal tubule
simple squamous epithelium of capsule turns simple cuboidal in tubule
mesangial cells
pack spaces among capillaries of glomerulus
physically support capillaries
aid in regulating glomerular blood flow
phagocytize tissue debris
prevent clogging of glomerular filtration membrane
renal tubule
duct that leads away from the glomerular capsule and ends at the tip of a medullary pyramid
divided into 4 regions
proximal convoluted tubule - part of nephron
nephron loop - part of nephron
distal convoluted tubule - part of nephron
collecting duct - receives fluid from many neprhons
proximal convoluted tubule (PCT)
longest and most coiled of the four regions
arises from the glomerular capsule
simple cuboidal epithelium with prominent microvili (a lotta absorption)
nephron loop
long U-shaped portion of renal tubule found mostly in the medulla
descending limb
begins where PCT straightens out and dips toward/into the medulla
ascending limb
returns to cortex and travels parallel to descending
thick segments
simple cuboidal epithelium
initial part of descending and all of ascending
heavily engaged in active transport of salts (high metabolic activity & loaded w/ mitochondria)
thin segments
simple squamous epithelium
forms most of descending limb
low metabolic activity
very permeable to water
distal convoluted tubule (DCT)
begins shortly after the ascending limb reenters the cortex
shorter and less coiled
cuboidal epithelium
nearly devoid of microvili
end of nephron
collecting duct
receives fluid from DCTs of several nephrons as it goes back into the medulla
converge toward tip of a medullary pyramid, and near the papilla they form a papillary duct
simple cuboidal epithelium
papillary ducts
end in pores at the conical tip of each papilla
urine drains from these pores into minor calyx that encloses papilla
simple cuboidal epithelium
flow of fluid from where glomerular filtrate is formed to urine
glomerular capsule → proximal convoluted tube → nephron loop → distal convoluted tube → collecting duct → papillary duct → minor calyx → major calyx → renal pelvis → ureter → urinary bladder → urethra
juxtamedullary nephrons
close to the medulla
very long nephron loops that extend as far as the apex of renal pyramid
15% of all nephrons - major contributors to maintenance of osmotic gradient in medulla
cortical nephrons
farther from medulla
relatively short nephron loops that dip only slightly into the outer medulla before turning back
turn back even before leaving the cortex
some have no nephron loops at all
why are nephron loops important?
maintain osmotic gradient in medulla that helps the body conserve water
juxtamedullary nephrons huge contributors
Renal plexus
nerves and ganglia wrapped around each renal artery
issues nerve fibers to blood vessels and convoluted tubules of nephrons
carries:
sympathetic innervation from abdominal aortic plexus
afferent pain fibers
role of sympathetic fibers in renal innervation
stimulation by sympathetic fibers of renal plexus reduces glomerular blood flow, and consequently urine production
respond to falling blood pressure by stimulating kidneys to secrete renin - enzyme that activates hormonal mechanisms for restoring blood pressure
renin
enzyme that activates hormonal mechanisms for restoring blood pressure
parasympathetic innervation in kidneys
arise from vagus nerve
function unknown
Stages of Kidney converting blood plasma to urine
glomerular filtration
tubular reabsorption
tubular secretion
water conservation
glomerular filtrate
fluid in capsular space
similar to blood plasma except that it has almost no protein
tubular fluid
fluid from proximal convoluted tubule through distal convoluted tubule
differs from glomerular filtrate because of substances removed/added by tubule cells
urine
once fluid enters the collecting duct
undergoes little alteration beyond this point except for change in water content
glomerular filtration
process in which water and some solutes in blood plasma pass from capillaries of glomerulus into capsular space of the nephron
has to pass through filtration membrane (3 barriers)
fenestrated endothelium of capillary
basement membrane
filtration slits
fenestrated endothelium of capillary
endothelial cells of glomerular capillaries are honeycombed with large filtration pores
highly permeable
pores small enough to exclude blood cells from filtrate
basement membrane
consist of a proteoglycan gel
a few large molecules may penetrate small spaces and cross
most would be held back (larger than 8 nm)
negatively charged smaller molecules can be held back by negative charge on proteoglycans through repulsion
protein composition of blood plasma and glomerular filtrate
blood plasma - 7%
glomerular filtrate - 0.03% (traces of albumin and smaller polypeptides)
filtration slits
podocyte of glomerular capsule with a bulbous cell body and several thick arms
each arm has foot processes that wrap around capillaries and interdigitate with each other
create negatively charged filtration slits that are an additional obstacle to large anions
what molecules can pass freely through the filtration membrane into the capsular space
almost any molecule smaller than 3 nm can pass freely and appear in the urine
water
electrolytes
glucose
fatty acids
amino acids
nitrogenous wastes
vitamins
these have about the same concentration in glomerular filtrate as blood plasma
some solutes of low molecular weight are retained in blood stream due to their binding to plasma proteins that can’t pass through membrane
what can allow albumin or blood cells to filter through?
damage to the filtration membrane
kidney infections
trauma
strenuous exercise
reduces perfusion of kidneys
deteriorates glomerulus due to hypoxia
leaks protein/blood into filtrate
proteinuria (albuminuria)
presence of albumin in urine
hematuria
presence of blood in urine
Filtration pressure
blood hydrostatic pressure (BHP) ~60 mm Hg
results due to size difference between afferent and efferent arteriole
glomerulus has a large inlet and small outlet
hydrostatic pressure in capsular space ~18 mm Hg
results from high rate of filtration and continual accumulation of fluid in capsule
colloid osmotic pressure (COP) ~32 mm Hg
glomerular filtrate = almost protein free and no significant COP
net filtration pressure (NFP) in kidneys
60out - 18in - 32in = 10 mm Hg
why do glomerular capillaries absorb little to no fluid?
Although BHP also drops throughout course of glomerular capillaries, it is still high enough to solely engage in filtration
hypertension
high blood pressure in glomeruli increase vulnerability to hypertension
ruptures glomerular capillaries - scarring the kidneys (nephrosclerosis)
promotes atherosclerosis of blood vessels (including renal)
diminishes renal blood supply
over time this often leads to renal failure, leading to more hypertension and initiating a positive feedback loop
Glomerular filtration rate
amount of filtrate formed per minute by the 2 kidneys combined
for every 1 mm Hg of net filtration pressure, a young adult male’s kidneys produce ~12.5 mL of filtrate per minute = filtration coefficient (Kf)
GFR = NFP x Kf
filtration coeeficient (Kf)
depends on permeability and surface area of filtration barrier
10% lower in women than in men
glomerular filtration rates in humans
males: 180 L/day
females: 150 L/day
what happens when GFR is too high?
fluid flows through the renal tubules too rapidly for them to reabsorb the usual amount of water and solutes
urine output rises and creates a threat of dehydration and electrolyte depletion
what happens when GFR is too low?
fluid flows sluggishly through the tubules
gomeruli reabsorb wastes that should be eliminated in the urine
azotemia may occur
how to adjust GFR quickly
change glomerular blood pressure
done through 3 mechanisms:
renal autoregulation
sympathetic control
hormonal control
Renal autoregulation
ability of nephrons to adjust their own blood flow and GFR without external (nervous or hormonal) control
enables them to maintain a relatively stable GFR in spite of changes in arterial blood pressure
ensures stable fluid and electrolyte balance despite the many circumstances that substantially alter one’s blood pressure
2 mechanisms of autoregulation
myogenic mechanism
tubuloglomerular feedback
myogenic mechanism
stabilizes GFR based on the tendency of smooth muscle to contract when stretched - blood flow and filtration remain fairly stable
when arterial blood pressure rises - stretches afferent arteriole
arteriole constricts and prevents blood flow into glomerulus from changing drastically
when arterial blood pressure falls - afferent arteriole relaxes
allows easier blood flow into glomerulus
tubuloglomerular feedback
mechanism by which the glomerulus receives feedback on the status of the downstream tubular fluid and adjusts filtration to regulate:
its composition
stabilize nephron performance
compensate for fluctuations in blood pressure
involves juxtaglomerular apparatus, macula densa, and granular cells
juxtaglomerular apparatus
found at very end of nephron loop, where it reenters renal cortex
loop contacts afferent and efferent arterioles at the vascular pole of the renal corpuscle
macula densa
patch of slender, closely spaced sensory cells on one side of the loop
where tubuloglomerular feedback begins
cells absorb Na+, K+, and Cl-; water follows osmotically
cells swell and secrete ATP from basal surfaces
ATP metabolized into adenosine by mesangial cells
stimulates granular cells
granular (juxtaglomerular) cells
modified smooth muscle cells wrapped around the afferent arteriole and to a lesser extent the efferent arteriole
stimulated by adenosine created by macula densa
respond to rising adenosine levels by constricting the afferent arteriole
reduces blood flow into glomerulus, reducing GFR and completing negative feedback loop
mesangial cells may also contract - constricting glomerular capillaries and reducing filtration
basic steps of going from high to reduced GFR
high GFR
increased NaCl load in nephron loop
macula densa secretes ATP
mesangial cells metabolize ATP to adenosine
adenosine stimulates granular cells
afferent arteriole constricts
reduced GFR
how does the tubuloglomerular feedback process affect the distal convoluted tubule?
distal convoluted tubule has a limited capacity for NaCl reabsorption
tubuloglomerular feedback process helps prevent overloading the distal convoluted tube with NaCl
preventing excessive NaCl and water loss in urine
what is an additional effect of granular cells?
their granules release renin in response to blood pressure, which initiates a renin-angiotensin-aldosterone mechanism
contributes to the restoration of blood pressure and supporting blood volume
2 important things to keep in mind about renal autoregulation
doesn’t completely prevent changes in GFR
maintains dynamic equilibrium - fluctuates within narrow limits
changes in BP do affect GFR and urine output
can’t compensate for extreme BP variations
GFR remains stable within a range of 90-180 mm Hg
Below 70 mm Hg - glomerular filtration and urine output cease (hypovolemic shock)
Sympathetic control of glomerular filtration
sympathetic stimulation and adrenal epinephrine constrict afferent arterioles
reduces GFR and urine output while redirecting blood from kidneys to heart, brain, and skeletal muscles (where it is more urgently needed)
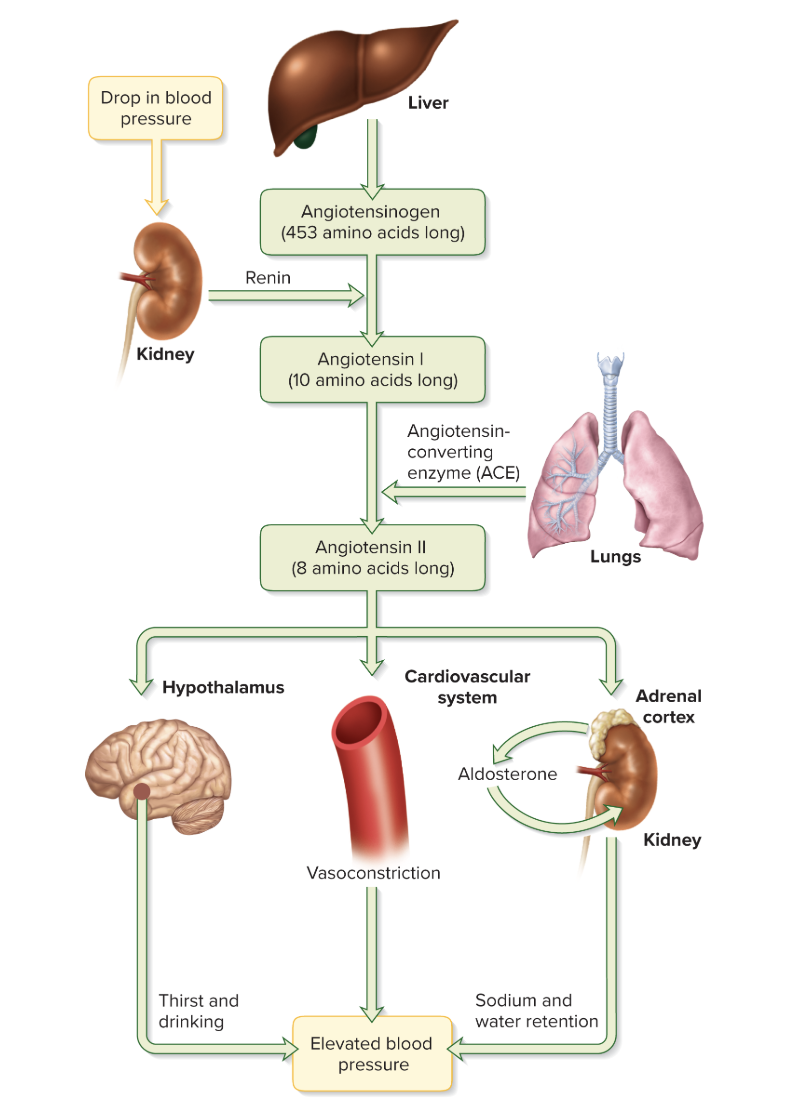
Renin-Angiotensin-Aldosterone Mechanism
substantial drop in BP detected by baroreceptors in aorta and carotid arteries
transmit a signal to the brainstem, leading to various corrective sympathetic reflexes
sympathetic fibers stimulate granular cells to secrete renin
renin acts on angiotensinogen (protein in blood plasma) to split off a 10 amino acid peptide called angiotensin I
in the lungs and kidneys, angiotensin converting enzyme (ACE) removes two more amino acids → converting it to angiotensin II
angiotensin II restores fluid volume and blood pressure
angiotensin II (a baddie) and her impact
leads to effects that rise blood pressure through water loss, encouraging water intake, and constricting blood vessels
potent vasoconstrictor
widespread vasoconstriction raises the mean arterial BP throughout body
in kidneys, constricts efferent arterioles less than afferent
raises glomerular BP and GFR - target is to prevent drastic reduction in GFR
ensures continued filtration of wastes from blood even w/ low BP
constriction of efferent arterioles lowers BP in peritubular capillaries downstream - strongly enhances reabsorption of NaCl and water from nephron - returning it to bloodstream instead of losing it in urine
stimulates the adrenal cortex to secrete aldosterone
promoting sodium and water reabsorption by distal (and proximal) convoluted tubule and collecting duct
stimulates posterior pituitary to secrete antidiuretic hormone
promotes water reabsorption by collecting duct
stimulates sense of thirst and encourages water intake
the birth and legacy of angiotensin II
Liver gives us angiotensinogen
when kidney senses drop in blood pressure it tells renin to chop up angiotensinogen to get angiotensin I
angiotensin I lowkey just angiotensin II before glam
it goes to the dressing rooms in the lungs and kidneys, gets even more snatched using ACE, and steps outside:
angiotensin II hits the hypothalamus and suddenly everyone is thirsty and drinking
in the cardiovascular system angiotensin II makes everyone feel like they have to suck in, causing vasoconstriction
when it goes to the adrenal cortex it tells aldosterone to pop out and suddenly all the sodium and water don’t wanna leave
angiotensin II told everyone to step it up, increasing blood pressure all over the body
proximal convoluted tubule
reabsorbs ~65% of glomerular filtrate
removes some substances from the blood and secretes them into the tubule for disposal in the urine
great length and prominent microvili = absorptive surface area
abundant large mitochondria = provide ATP for active transport
tubular reabsorption
process of reclaiming water and solutes from the tubular fluid and returning them to the blood
PCT reabsorbs greater variety of chemicals than any other part of nephron
2 routes of reabsorption
Transcellular route
Paracellular route
transcellular route
involved in tubular reabsorption
substances pass through the cytoplasm and out the base of epithelial cells
paracellular route
involved in tubular reabsorption
substances pass through gaps between cells
water movement in tubular reabsorption
tight junctions between epithelial cells are leaky and allow significant amounts of water to pass through
involves solvent drag - as water travels through epithelium, it carries a variety of dissolved solutes
direction of movement of water and solutes
enter tissue fluid at base of epithelium, and are then taken up by the peritubular capillaries
Sodium Chloride in tubular reabsorption
important for all aspects as it creates an osmotic and electrical gradient, which drives reabsorption of water and other solutes into epithelial cells
most abundant cation in the glomerular filtrate
2 types of transport proteins that drive sodium uptake
Symports
Na+-H+ antiport
Symports and Sodium Chloride
simultaneously bind Na+ and another solute (glucose, amino acids, lactate)
dont consume ATP
considered secondary active transport because of dependence on Na+-K+ pumps at the base of the cell
Na+-H+ antiport and Sodium Chloride
pulls Na+ into the cell while pumping H+ out of the cell into the tubular fluid
reabsorbs sodium
eliminates acid from body fluids
activated by angiotensin II - exerts strong influence on sodium reabsorption
ATP consuming active transport pump
how is sodium accumulation in epithelial cells prevented?
Na+-K+ pumps in the basal domain of plasma membrane pump Na+ out into the extracellular fluid
(ATP consuming active transport pumps)
Na+ picked up by peritubular capillaries and returned to the bloodstream
Cl- ions follow Na+ due to electrical attraction
Various antiports in the apical cell membrane absorb Cl- in exchange for other anions that they eject into the tubular fluid
Cl- and K+ ions are driven out through the basal cell surface by a K+-Cl- symport
Na+ and Cl- pass through tubule epithelium by paracellular route between cells
Which ions pass through paracellular route with water?
phosphate (also cotransported into epithelial cells with Na+)
magnesium
potassium
Calcium
52% reabsorbed by paracellular route (PCT)
14% reabsorbed by transcellular route (PCT)
reabsorption not dependent on hormones in PCT
33% reabsorbed in nephron (parathyroid influence)
1% excreted in urine
glucose in tubular reabsorption
cotransported with Na+ by sodium-flucose transporters (SGLTs) symports
removed from basolateral surface of cell by facilitated diffusion
normally all glucose is reabsorbed
Nitrogenous wastes in tubular reabsorbption
urea passes through epithelium with water
40-60% of urea in tubular fluid reabsorbed by nephron
also reabsorbs 99% of water, increasing urea concentration in blood/glomerular filtrate
kidney removes about half of the urea in the blood to keep concentration at a safe level
uric acid mostly reabsorbed by PCT
later parts of nephron secrete it back into tubular fluid
creatinine
not reabsorbed - stays in tubule and passes in urine
water in tubular reabsorption
2 thirds of water is reabsorbed by PCT
kidneys reduce 180 L of glomerular filtrate to 1 or 2 L of urine each day
reabsorption of all solutes makes tubule cells and tissue fluid hypertonic to tubular fluid
water follows solutes by osmosis through paracellular and transcellular routes
movement of water in tubular reabsorption
follows solutes by osmosis through paracellular and transcellular routes
transcellular absorption
occurs through aquaporins in apical and basolateral domains of plasma membrane
emables water to enter tubule cells at the apical surface and leave them (to return to the blood) via the basolateral surface
reabsorption proportions in tubular reabsorption
PCT reabsorbs proportionate amounts of solutes and water
Elsewhere in the nephron, water reabsorption varies due to influence of hormones responding to body’s state of hydration
obligatory water reabsorption
Absorption of water at a constant rate in the PCT
Uptake by peritubular capillaries
after water and solutes leave basal surface of tubule epithelium, they reabsorbed by peritubular capillaries
2 mechanisms:
osmosis
solvent drag
what factors promote osmosis into peritubular capillaries
Creation of a high tissue fluid pressure through accumulation of reabsorbed fluid on the basal side of epithelium - physically drives water into capillaries
Narrowness of efferent arteriole decreases resistance to reabsorption - lowers BHP from 60 mm Hg in glomerulus to 8 mm Hg in peritubular capillaries
Protein being retained as water is filtered out when blood passes through the glomerulus - elevates blood’s COP when it leaves the glomerulus
high COP and low BHP in capillaries + high hydrostatic pressure in tissue fluid = balance of forces in peritubular capillaries → favor reabsorption
bonus factor:
angiotensin II constricts afferent and efferent arteriole, reducing blood pressure in peritubular capillaries and reducing resistance to fluid reabsorption
steps of uptake by the peritubular capillaries
Angiotensin II secreted
constricts afferent and especially efferent arterioles
Maintains glomerular blood pressure and glomerular filtration
reduces blood pressure in peritubular capillary
reduces resistance to tubular reabsorption
tubular reabsorption increases
urine volume is less but concentration is high