40. GAT 2: Principles of Genomics (Application)
1/49
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
50 Terms
What is Familial hypercholesteraemia's (FH) inheritance pattern?
Autosomal Dominant Pattern
- There is a 50% (1 in 2) likelihood that each child of an affected parent will also be affected.
What is BRCA variants inheritance pattern?
Autosomal Dominant Pattern
- There is a 50% (1 in 2) chance that each child will inherit the variant from a parent who is a carrier.
What is Cystic Fibrosis' Inheritance Pattern?
Autosomal Recessive Pattern
- There is a 25% (1 in 4) chance that each child will inherit the variant from a parent who is a carrier.
What is Familial Hypercholesterolaemia (FH)?
A genetic condition that causes high cholesterol from birth.
It is one of the most common inherited conditions, affecting about 1 in 250.
What is the risk of cardiovascular events in untreated FH?
If untreated:
- 50% of men with FH will have a heart attack by age 50
- 30% of women with FH will have a heart attack by age 60
Early diagnosis enables cholesterol-lowering medicines that significantly reduce this risk.
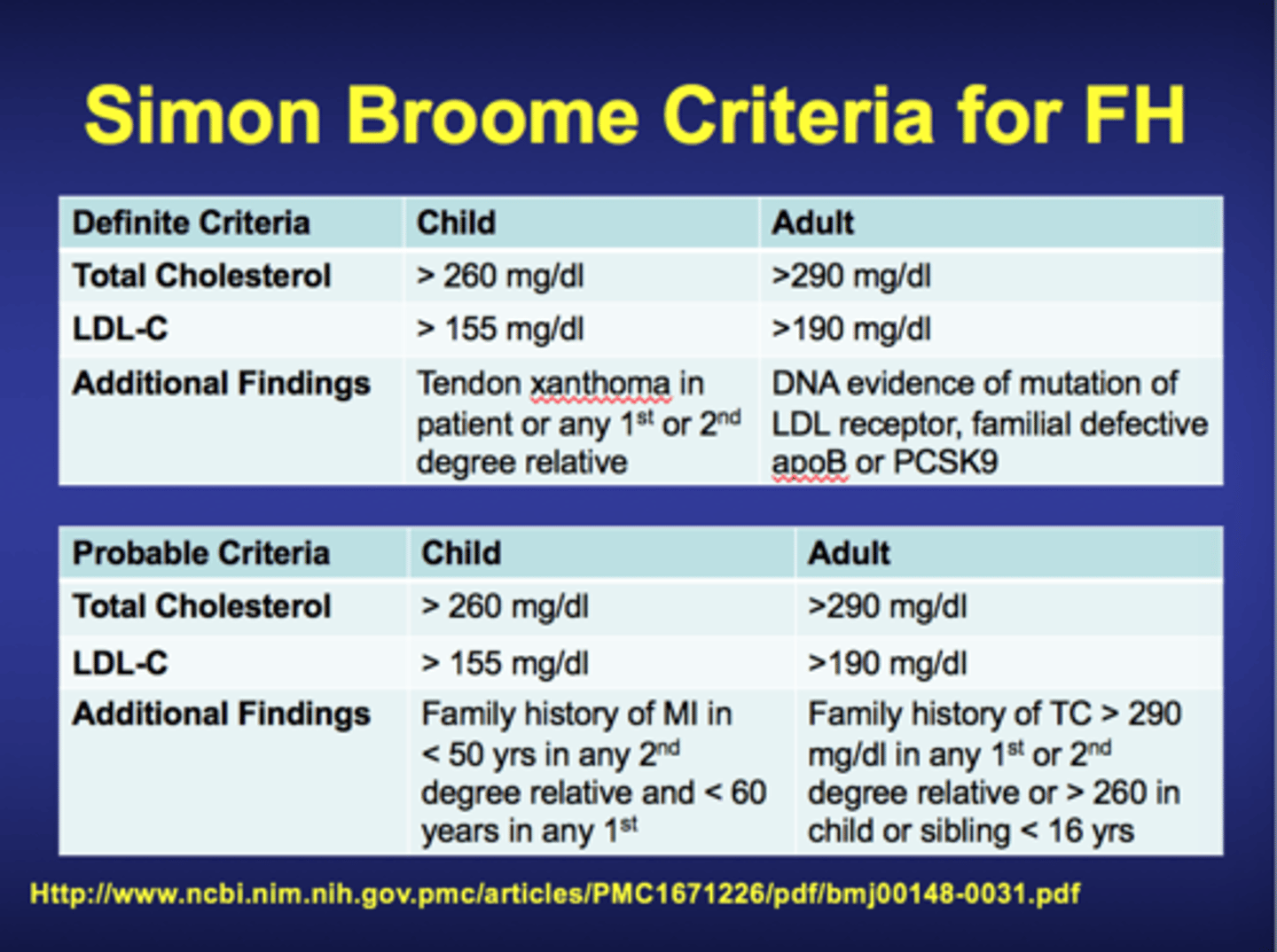
How can possible FH be identified?
- Using routine cholesterol checks, family history, and applying diagnostic criteria such as the Simon Broome Criteria.
- Possible or definite cases should be offered genetic testing.
What are the NICE case-finding criteria for FH in primary care? (NICE CG71)
Systematically search primary care records for people:
- Younger than 30 years with total cholesterol > 7.5 mmol/L
- 30 years or older with total cholesterol > 9.0 mmol/L
These are the people at highest risk of FH.
What additional clinical information would support a diagnosis of "definite" FH using Simon Broome criteria?
Clinical signs in the patient or a first-degree relative such as:
Tendon xanthoma - swollen tendons on knuckles or Achilles
Xanthelasma - raised, pale, yellowish patches around eyes/eyelids
OR
DNA-based evidence of an LDL-receptor mutation, familial defective apo B100, or a PCSK9 mutation.
Name an alternative diagnostic criterion to Simon Broome for FH.
The Dutch Lipid Clinic Network (DLCN) score.
Who is eligible for FH DNA testing on the NHS?
A person is eligible if:
- They meet the Simon Broome criteria for possible or definite FH
OR
- They have a DLCN score greater than 5
What is cascade testing in the context of FH?
Once a pathogenic variant has been found in one person, it is much easier to find the same variant in family members because geneticists already know what to look for, they don't need to search all possible genes that can cause the disease.
What are the treatment options for FH? (NICE CG71)
Lipid-lowering medication titrated to achieve at least a 50% reduction in LDL-C concentration:
• High-potency statins — first line
• If required, intensify with ezetimibe, a PCSK9 inhibitor, bile acid sequestrants and/or fibrates
Plus appropriate lifestyle advice (diet, exercise, smoking, alcohol).
Lipid-modifying drug therapy for children/young people with FH should usually be considered by age 10.
What contraception advice should be given to women/girls with FH on lipid-modifying therapy? (NICE CG71)
The risks for future pregnancy while taking lipid-modifying drugs should be discussed and revisited at least annually.
- Tailored information about pregnancy and contraception should be given.
- A choice of effective contraception methods should be offered.
- Combined oral contraceptives (COCs) are not generally contraindicated, but because there is a small potential increased risk of cardiovascular events, other forms of contraception should be considered.
How are BRCA1 and BRCA2 variants associated with cancer?
A BRCA gene variant does not cause cancer on its own. If the genes are mutated so the proteins don't function properly, the cell's ability to repair DNA damage is impaired.
Mutations from normal cell division can accumulate, cell division can run out of control, and this can lead to cancer.
What is the difference between germline and somatic variants?
Germline variant = occurs in a gamete (egg/sperm) or germ cells = inherited.
Somatic variant = arises during an individual's lifetime in tissues other than germ cells, so cannot be passed on to offspring = acquired.
Why are germline BRCA variants important to hereditary cancer risk?
Most cancers result from somatic mutations, which is why many cancers are localised.
- Germline variants in cancer predisposition genes (such as BRCA) are present in all the body's cells (including cancer cells) and are associated with hereditary increased risk of cancer.
Which cancers are BRCA gene variants associated with?
Breast cancer - men and women
Ovarian cancer - women
Prostate cancer - men
Pancreatic cancer - men and women
Both men and women have both BRCA genes and can pass germline variants on to their offspring.
What are the treatment/management options for someone with a pathogenic BRCA variant? (NICE CG164)
1. Breast cancer screening = annual screening from age 25–30 for women with pathogenic BRCA variants.
2. Risk-reducing surgery = risk-reducing mastectomies reduce lifetime cancer risk to <5% (lower than the general population).
3. Chemoprophylaxis = three drugs recommended: tamoxifen, anastrozole, raloxifene.
Why does CF affect multiple organ systems?
CFTR protein is present at many sites in the body. So CF affects:
Lungs = impaired CFTR causes thick mucus, hard to clear → chronic respiratory infection and inflammation.
Pancreas = pancreatic insufficiency, requiring exogenous pancreatic enzyme supplementation.
What are the main symptoms of cystic fibrosis?
- Wheezing, coughing, shortness of breath, airway damage
- Malabsorption and poor weight gain
- Jaundice and liver disease
- Diarrhoea, constipation
- Diabetes
- Infertility in males
How is cystic fibrosis screened for and confirmed in newborns?
Screening = newborn bloodspot test (heelprick test) on day 5 of life, which screens for 10 genetic conditions including CF.
Confirmation = sweat test, which checks for excess chloride in a sweat sample.
Why do patients with CF have excess chloride in their sweat?
If the CFTR protein is defective, chloride cannot be reabsorbed into sweat duct cells effectively, so it accumulates in sweat and can be detected on the skin surface.
How do CFTR modulators work?
They act directly on the defective CFTR protein to either:
- Improve cellular processing and trafficking = increasing the quantity of functional CFTR at the cell surface, OR
- Increase gating (channel-opening) probability = resulting in increased chloride ion transport.
Which gene is associated with aminoglycoside-induced ototoxicity in CF patients?
MT-RNR1 (located on mitochondrial DNA).
- Patients with this variant are at much greater risk of ototoxicity (deafness) from aminoglycosides such as tobramycin, gentamicin and amikacin, independent of the drug dose.
What proportion of the population are carriers of a CF variant?
Approximately 1 in 25 people are carriers.
- Carriers have only one variant gene copy and do not have symptoms of the condition.
When did the Human Genome Project run, and what were its key statistics?
- Involved 6 countries and cost $3 billion.
- It remains the world's largest collaborative biological project.
How long does Whole Genome Sequencing (WGS) now take, and how much does it cost?
- Less than a day, and less than £1000.
- This reflects huge advances in sequencing technology, bioinformatics, AI and machine learning.
What was the UK 100,000 Genomes Project, and when was it completed?
Genomics England's first initiative = an internationally groundbreaking project to sequence and study the role our genes and genomes play in health and disease.
- Recruitment was completed in 2018, but research and analysis is still ongoing.
What is the UK Biobank initiative?
Whole Genome Sequencing of 500,000 participants in the UK.
What is the UK Generation Study, and when was it launched?
Launched in 2023.
It involves Whole Genome Sequencing of 100,000 newborn babies.
What was the impact of the 100,000 Genomes Project on rare disease?
It found out that 7% of people are affected by a rare disease in their lifetime.
It helped reduce the diagnostic odyssey by comparing WGS of patients with the same condition to reveal patterns, leading to development and use of targeted treatments.
What was the impact of the 100,000 Genomes Project on cancer?
Identified mutations associated with cancer:
Germline (hereditary) mutations = found by comparing genomes of people with cancer vs without (e.g., BRCA1 and breast cancer).
Somatic mutations = found by comparing genomes from cancer cells vs non-cancer cells in the same patient.
This enabled development of preventative and targeted treatments.
What was set up after the 100,000 Genomes Project?
The NHS Genomic Medicine Service (NHS GMS) to embed genomic medicine into routine NHS care.
How does the NHS Genomic Medicine Service drive equitable access to testing?
Through a single mandated National Genomic Test Directory, which supports a standardised offer of funded testing across England with a new pricing model.
What three areas does the National Genomic Test Directory focus on?
1. Rare and Inherited Disease
2. Cancer
3. Pharmacogenomics
What kind of role do pharmacists play in the NHS Genomic Medicine Service?
Pharmacists support the service through:
- Identifying patients eligible for testing (e.g., case finding for FH in primary care).
- Supporting patients through the testing process.
- Prescribing in line with genomic results (e.g., CFTR modulators for cystic fibrosis).
- Applying pharmacogenomic evidence to optimise medicines.
What is the 2022 NHS Genomics Strategy?
Published by NHS England in 2022, building on Genome UK and other government strategies.
- It outlines the vision for the power of genomics in predicting, preventing and diagnosing disease, and targeting treatment to be accessible to all as part of routine care in the NHS.
What is the NHS 10-Year Plan, and what does it say about genomics?
It is called "Fit for the Future."
- It states that the collision of advances in genomics and analytics will allow the whole model of healthcare to be transformed and put the NHS at the front of the global genomics revolution.
What does the NHS 10-Year Plan mean for genomics? (In terms of service expansion)
The existing NHS Genomic Medicine Service will be expanded to create a new genomics population health service.
- The NHS GMS will reduce the diagnostic odyssey experienced by some patients with rare diseases.
What does the NHS 10-Year Plan mean for genomics? (In terms of cancer and inherited disease)
- Every cancer patient will receive a comprehensive genomic analysis and molecular profiling.
- The NHS GMS will expand genomic testing for inherited causes of major diseases for earlier detection and intervention, including cancer (e.g., BRCA1/2 genes) and cardiovascular disease predisposition (e.g., familial hypercholesterolaemia).
What does the NHS 10-Year Plan mean for genomics? (In terms of pharmacogenomics and records)
Pharmacogenomics will be integrated into routine clinical practice.
- The NHS will develop a Unified Genomic Record, integrating genomic data with relevant clinical/diagnostic data, linked to the Single Patient Record and the NHS App.
What is the National Genomic Test Directory?
A single, mandated directory used to identify the genomic tests funded and available on the NHS in England.
It drives equitable access and supports a standardised offer of funded testing with a new pricing model.
What three categories of tests are listed in the National Genomic Test Directory?
1. Rare and Inherited Disease
2. Cancer
3. Pharmacogenomics
Using the National Genomic Test Directory: which gene is associated with aminoglycoside-induced ototoxicity?
MT-RNR1 (located on mitochondrial DNA).
- Patients with this variant are at much greater risk of ototoxicity (deafness) from aminoglycosides such as tobramycin, gentamicin and amikacin, independent of the dose.
According to the National Genomic Test Directory, who is eligible for cystic fibrosis carrier testing?
Both partners planning a family where there is an increased chance of being a carrier - e.g., if a relative has cystic fibrosis (qualifies under Criteria 2 of the NHSE National Genomic Test Directory).
- The test looks for the 50 most common CFTR variants known to be associated with cystic fibrosis.
Per NICE CG71, what is the case-finding criteria for FH using the National Genomic Test Directory pathway?
Systematically search primary care records for people:
- Younger than 30 years with total cholesterol > 7.5 mmol/L
- 30 years or older with total cholesterol > 9.0 mmol/L
These individuals are at highest risk of familial hypercholesterolaemia.
What is cascade testing, and how does the National Genomic Test Directory support it?
Once a pathogenic variant is identified in one family member, it is much easier to look for that same variant in relatives (geneticists already know what to look for).
- NICE recommends cascade testing for first-, second-, and where possible, third-degree biological relatives of people with a genetic diagnosis (e.g., FH, BRCA).
What is the significance of Jewish ancestry for BRCA testing under the National Genomic Test Directory?
BRCA pathogenic variant is prevalent in 1 in 40 in Ashkenazi Jews.
- Anyone aged 18+ with one or more Jewish grandparents is eligible for BRCA testing regardless of family history.
What does the newborn bloodspot (heelprick) test screen for, in relation to the test directory?
Performed on day 5 of life and it screens for 10 genetic conditions, including cystic fibrosis.
A positive result is followed up with confirmatory testing (e.g., the sweat test for excess chloride to confirm CF).
What four CFTR modulators are licensed in the UK, and what are the active ingredients?
Kalydeco (ivacaftor)
Orkambi (ivacaftor + lumacaftor)
Symkevi (ivacaftor + tezacaftor)
Kaftrio (ivacaftor + tezacaftor + elexacaftor)
Indications are variant-specific (matched to the patient's CFTR genotype).