chapter 12: duplex ultrasound of lower extremity arteries
1/51
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
52 Terms
signs and symptoms of chronic arterial insufficiency
intermittent claudication
rest pain
nonhealing ulcers; gangrene
trophies changes (hair loss, nail thickening,skin changes)
signs and symptoms of acute arterial insufficiency
pallor
pulselessness
paralysis
paresthesia (pins & needles)
intense pain
coolness
supine
most common position is — with knee slightly flexed and thigh abduction
lateral decubitus
— position may be used to evaluate:
popliteal artery
tibioperoneal trunk
peroneal artery
curvilinear 5-2 MHz and/or phased array 3-2 MHz transducers
useful for aortoiliac scanning and deeper lower extremity vessels in heavier limbs
linear 7-4 MHz transducer
useful for the majority of lower extremity vessels
high-resolution, linear 18-7 MHz transducer
may allow better visualization of more superficial vessels, especially near ankle and foot
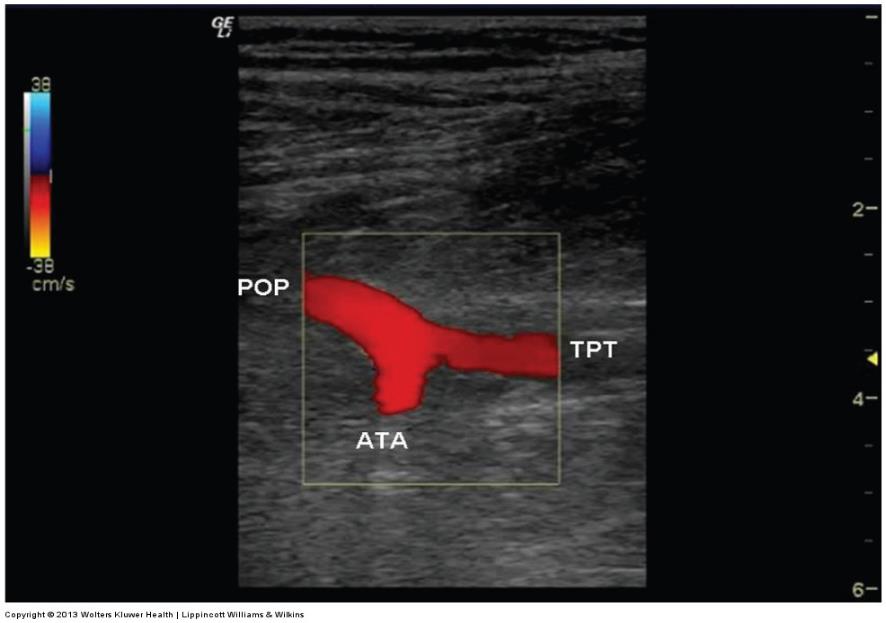
anterior tibial artery
the only vessel that we don’t scan on the venous side
PFA
only needs to be evaluated in its proximal segment
SFA
should be evaluated throughout its entire length in the thigh
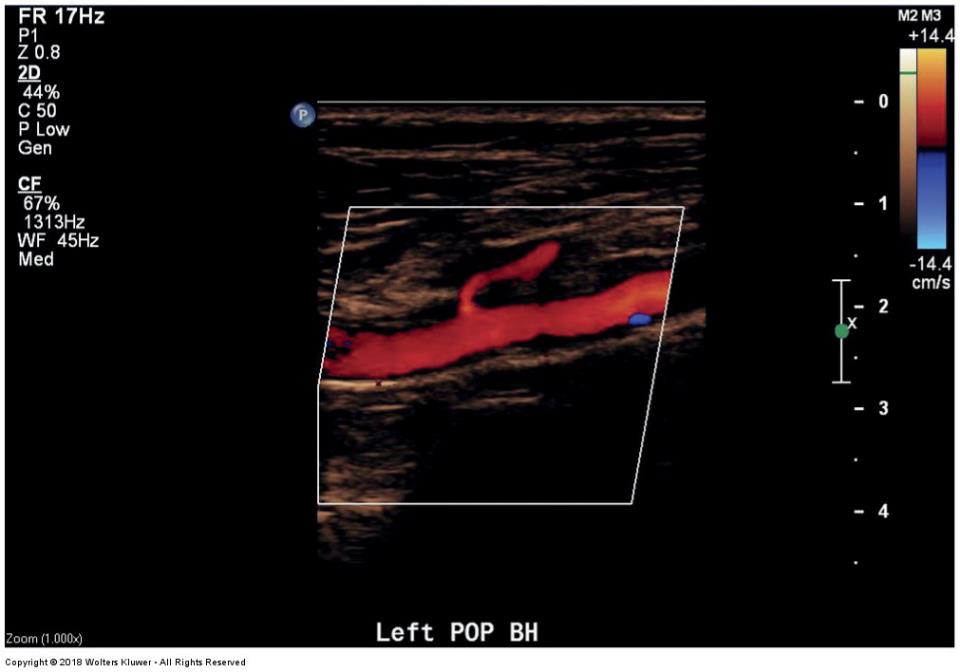
popliteal artery
SFA becomes — as it passes through the adductor canal
PA (popliteal artery)
is examined through the popliteal fossa
multiple small branches present including gastrocnemius arteries
sural arteries
the gastrocnemius is also known as the
anterior tibial origin
can be seen in popliteal fossa then remainder can be followed with an anterolateral approach
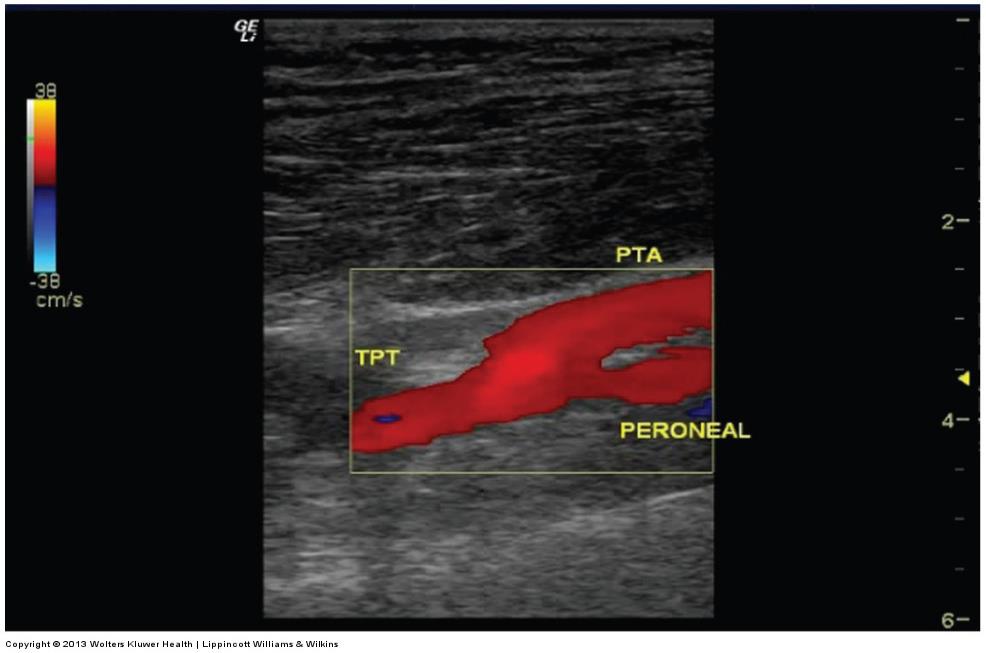
posterior tibial & popliteal artery
can be followed with a medial approach
peroneal
may also be examined with a posterolateral approach
spectral doppler
used as primary tool to categorize disease
when disease is present (stenosis)
velocities and waveforms should be recorded proximal to the stenosis, in the stenosis, and distal to the stenosis
1.5
if there is a bulge in a vessel and it is — times bigger than the proximal portion of the artery then it is an aneurysm
pitfalls of ultrasound
calcified vessels
extremely low flow
uncooperative patients
swelling and/or depth of vessels may limit visualization
exam length in complicated cases
normal arterial walls
are smooth and uniform
atherosclerotic plaquing
can be described as
homogeneous or heterogeneous
smooth or irregular
aneurysmal disease
can be bilateral and multilevel
aneurysm is present if the diameter of a vessel is 1.5 times bigger than the adjacent, more proximal segment
presence or absence of thrombus should be documented (embolic risk)
abnormal color findings
aliasing
reduced flow channel
color bruit
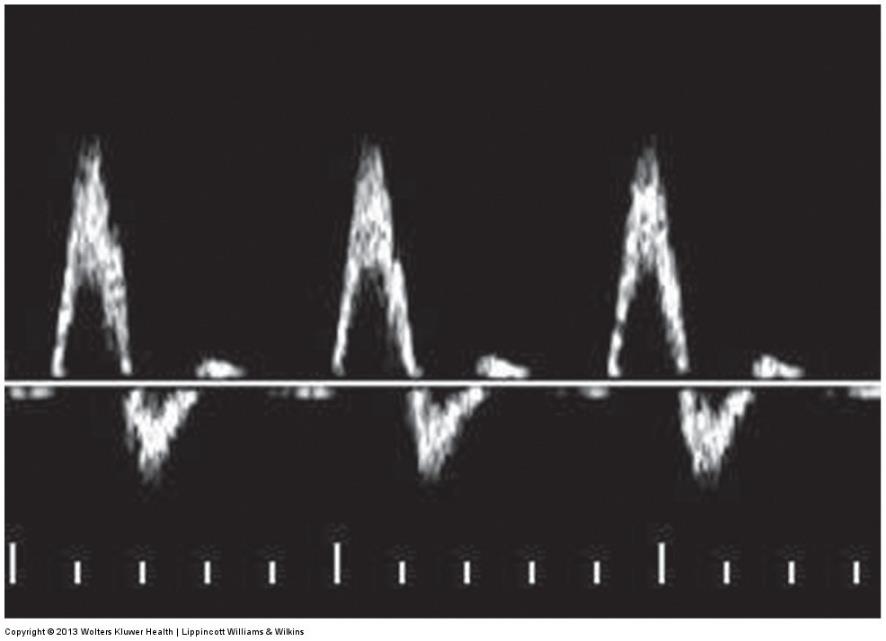
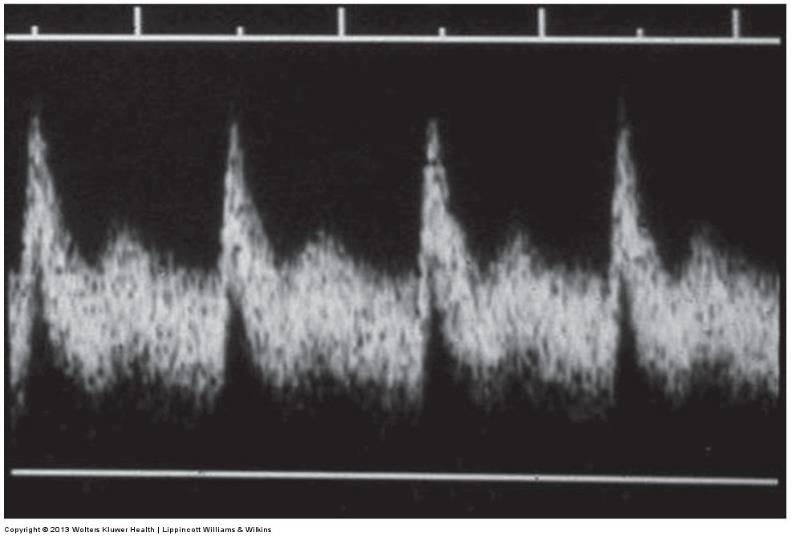
normal findings of spectral analysis
PSV that does not increase
normal, high resistance spectral waveform
sharp upstroke
rapid deceleration
reflected wave with retrograde flow in early diastole
brief wave of antegrade flow in mid to late diastole
abnormal findings of spectral analysis
focal velocity increases
50%
PSV velocity ratio >2 = > — stenosis
velocity doubles
70%
PSV velocity ratio >3 = > — stenosis
velocity triples
distal to a hemodynamically significant stenosis (starts to affect the down flow)
the spectral waveform can be expected to have
more low resistance characteristics (flow throughout diastole)
delay rise to peak systole (tardus parvus)
decreased distal resistance (arteriovenous fistula, trauma, cellulitis, post exercise)
antegrade flow can be expected throughout diastole
sharp systolic upstroke will be preserved
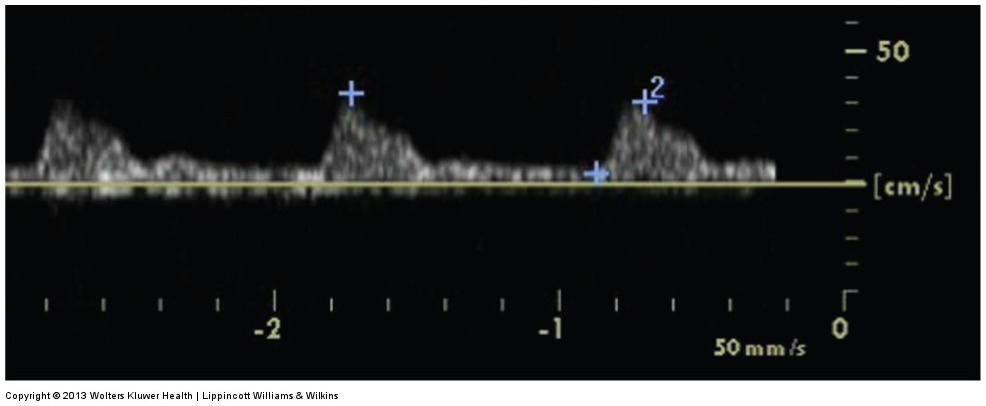
proximal to an occlusion or near occlusion
spectral waveform will display
very high resistance pattern
antegrade flow component only during systole
no flow during diastole
contrast arteriography
still considered the gold standard for diagnosis of arterial stenosis
contrast arteriogaphy can be used when duplex imaging is limited, such as
severe arterial calcification
severe edema or morbid obesity
extremely limited run-off
extensive skin wounds
extremely low flow
limitations of arteriography
delineates patent arterial lumen only
misses thrombosed popliteal aneurysms
fails to visualize outflow and inflow in very low-flow situations
requires potentially nephrotoxic agents
requires use of ionizing radiations
delays prompt treatment
ultrasound image of the popliteal artery with the gastrocnemius artery
ultrasound image of the origin of the anterior tibial artery (ATA) off the popliteal artery w/ the tibioperoneal trunk
ultrasound image of the posterior tibial artery (PTA) and peroneal arteries arising off the tibioperoneal trunk
an ultrasound image of an artery w/ atherosclerotic plaque
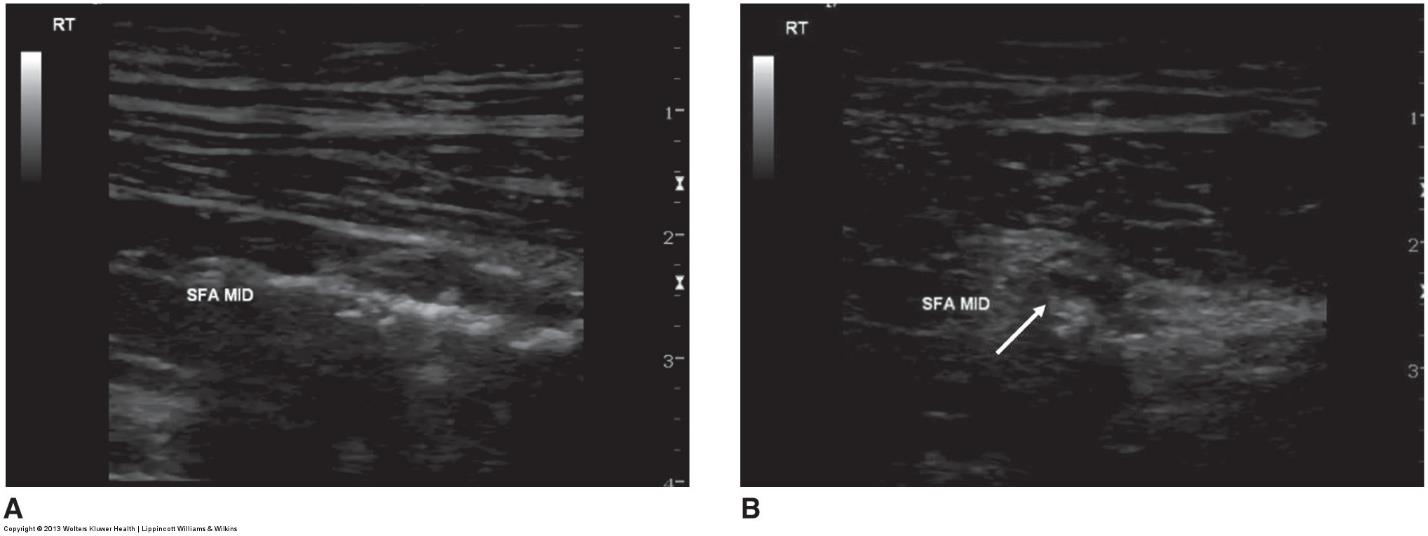
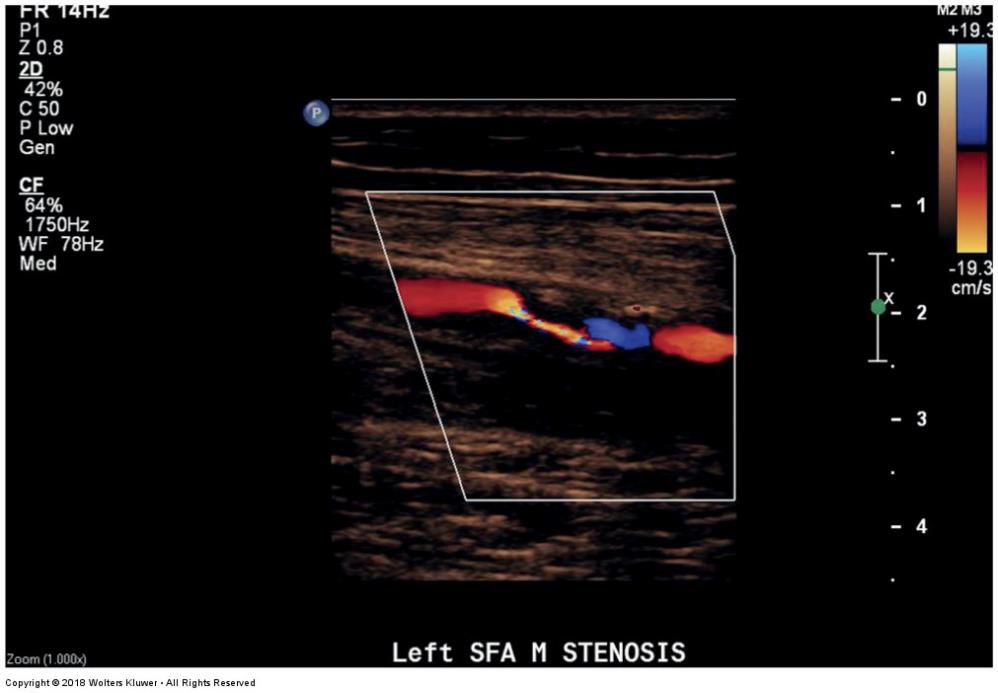
ultrasound image of a color-flow image identifying flow abnormalities associated with hypoechoic arterial plaque
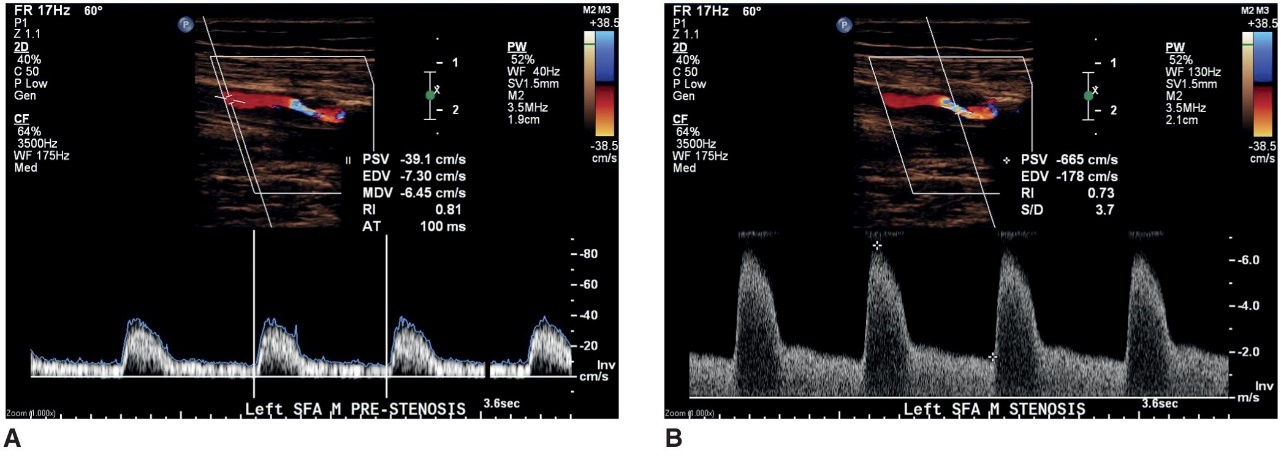
a doppler waveform taken proximal to a stenosis
what does image A represent
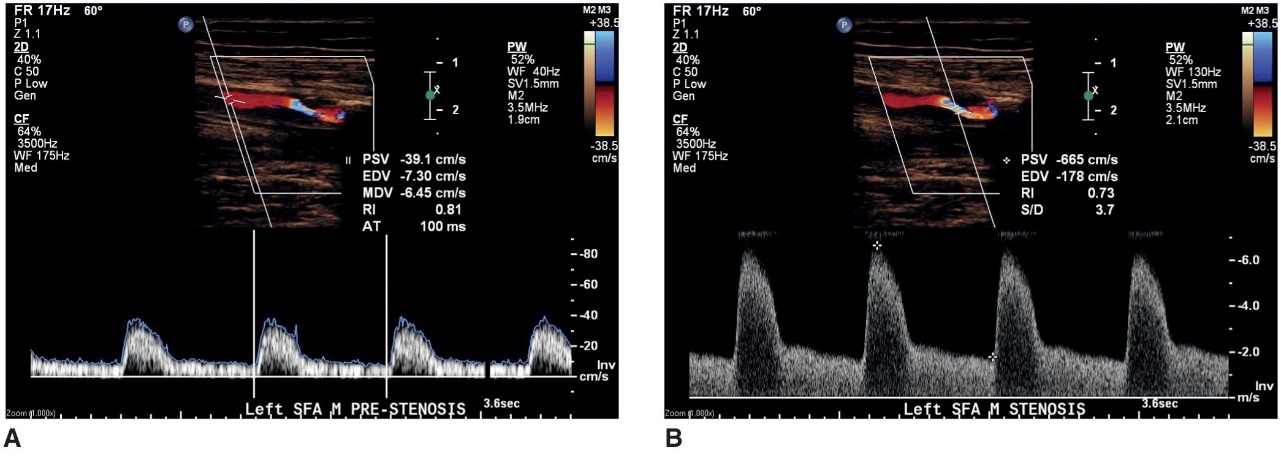
a doppler waveform taken at the area of maximum velocity shift within a stenosis
what does image B represent
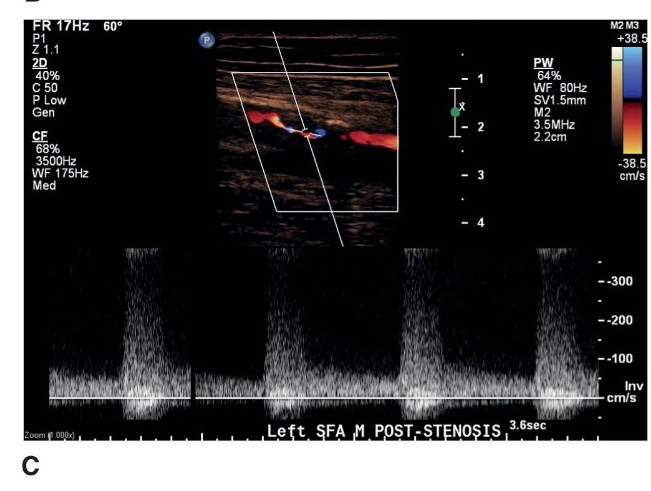
a doppler waveform distal to a stenosis documenting poststenotic turbulence
what does this image represent
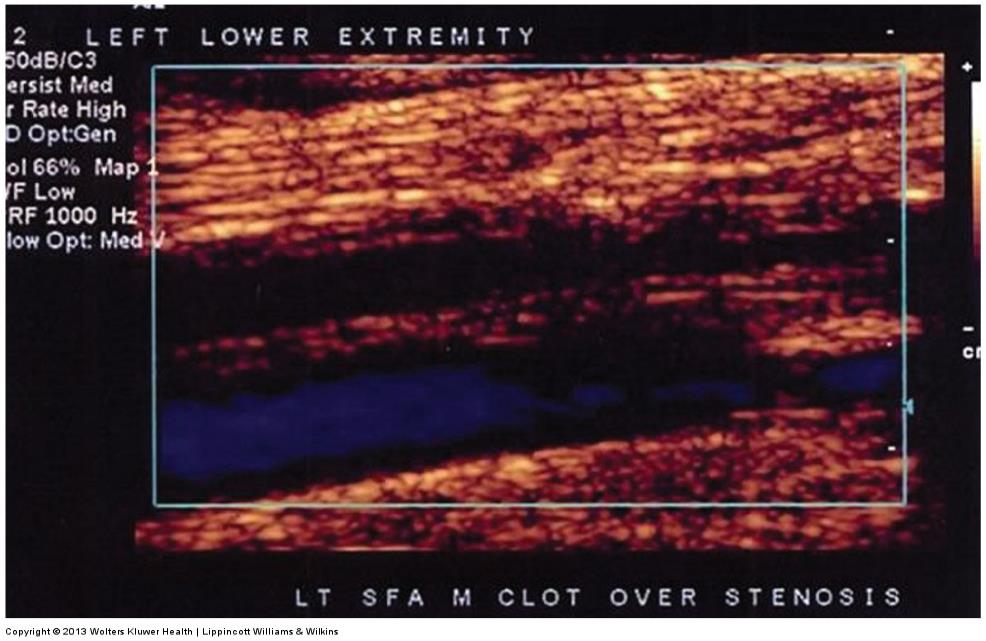
color doppler image of an occluded superficial femoral artery with acute thrombus overlying severe chronic arterial disease
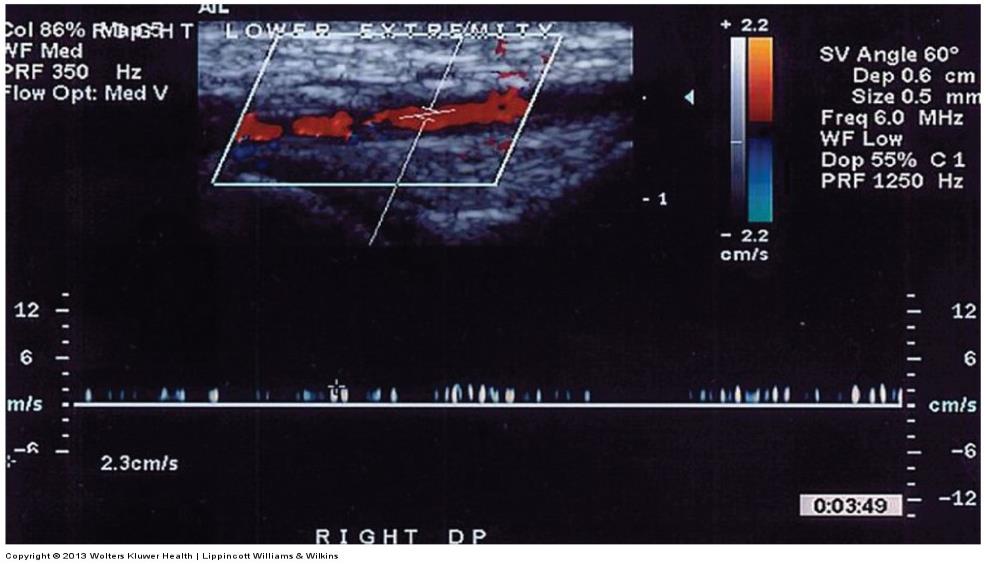
ultrasound image of a very low velocity vessel
color doppler image of a distal PTA with segmental heavy calcifications creating shadows obscuring the arterial lumen
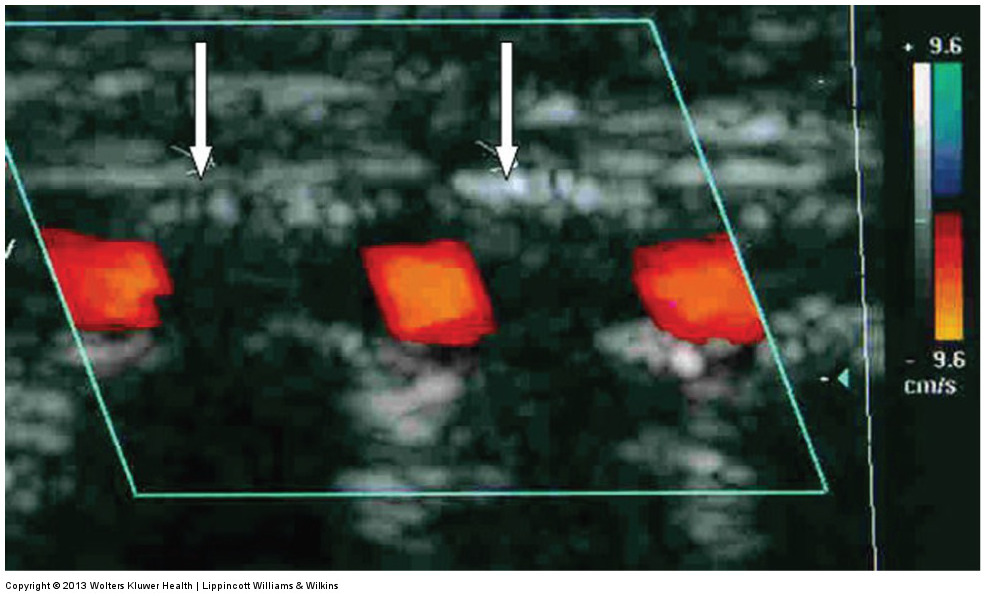
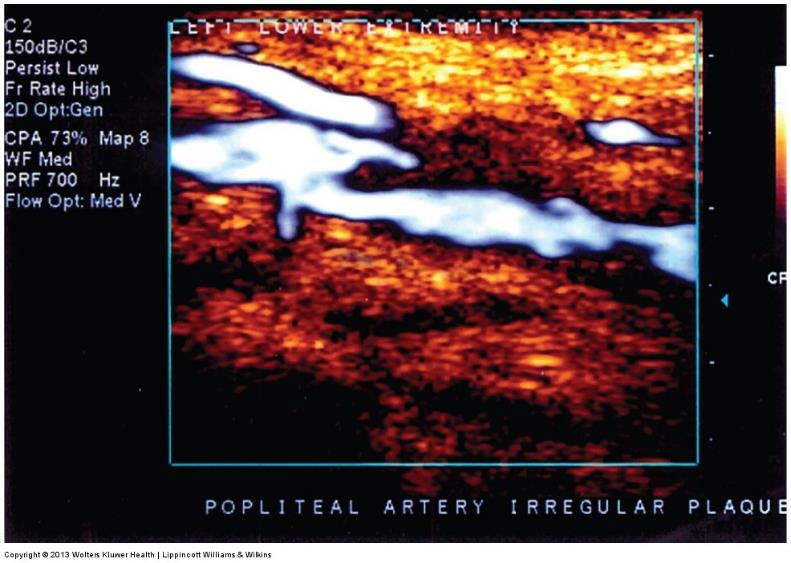
power doppler image of a severely diseased behind knee popliteal artery with very irregular ulcerated plaque surface w/ high embolization potential
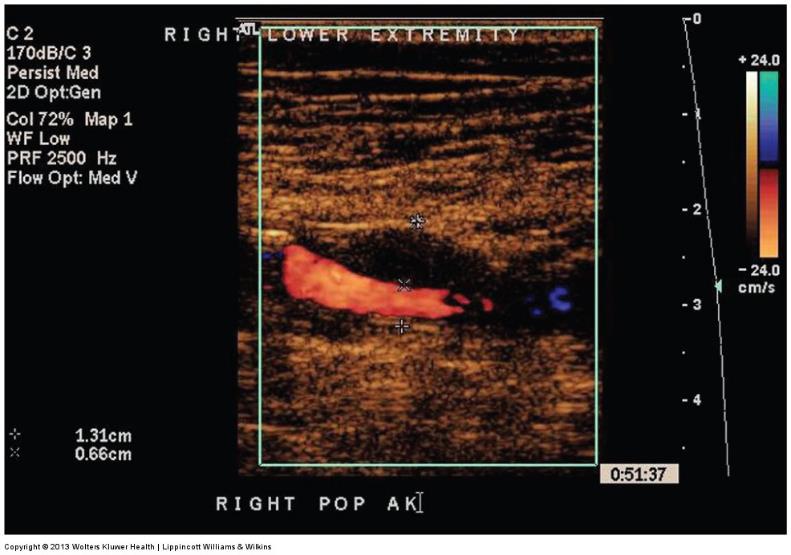
power doppler image of a small behind the knee popliteal artery aneurysm (13.1mm) w/ near-wall mural thrombus
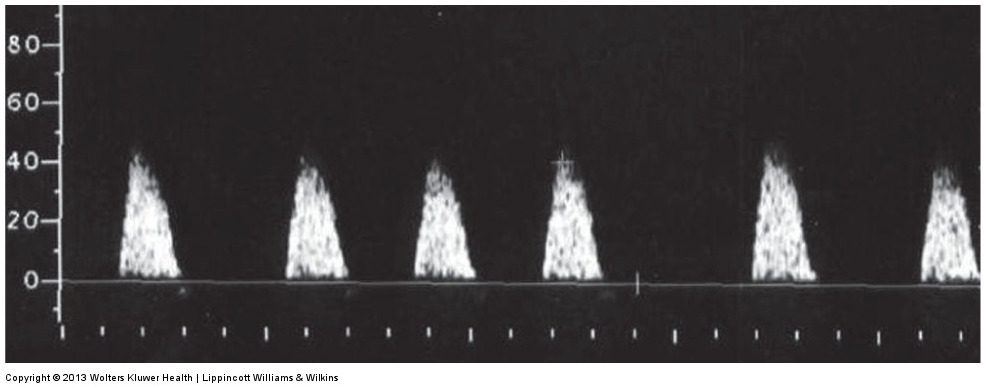
normal multiphasic waveform taken from SFA
an abnormal waveform illustrating constant forward flow throughout the cardiac cycle in addition to a delayed upstroke . distal to high-grade stenosis or occlusion
waveform dusiplaying a normal systolic upstroke with constant forward flow through diastole
an abnormal high resitance waveform with only antegrade flow through systole . this is observed proximal to a near occlusion or occlusion