GI Exam 2 Part 7: Pathophysiology of Bowel Diseases
1/45
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
46 Terms
what are inflammatory bowel diseases (IBD)
a group of related disorders that are characterized by chronic inflammation of the intestine that results in marked dysfunction of the digestive tract
what are the 3 IBDs
Crohn's disease
Ulcerative Colitis
microscopic colitis
what is indeterminate colitis
features of both UC and CD
Crohn's disease
more in the upper regions of the large and small intestine
-involving all layers of the bowel wall in any part of the GIT
-distal colon is NOT involved
-discrete regions can be affected
ulcerative colitis
more in the lower regions of the large intestine and the colon
confined to the large intestine
what population is UC more common in
males
what population is CD more common in
women
what area of the world are IBDs more common in
more prevalent in the western world
peak of IBD diagnosis
16-25 years old is the peak
CD may peak again at 76-85
CD declines more with age while UC is more constant
what symptoms are shared between IBS and IBD
pain and discomfort, urgency and bloating, alteration of bowel habits
how is IBS (irritable bowel syndrome) different than IBD
IBS is usually characterized as functional disease with diagnosis based on a cluster of symptoms but NO structural abnormalities
· IBD is characterized by inflammation/ulceration, i.e. “organic” changes in the small and/or large intestines, which are not associated with IBS
what are other terms for IBS (irritable bowel syndrome)
spastic colon, spastic colitis, mucous colitis, nervous stomach and nervous diarrhea
symptoms of IBS
· Abdominal discomfort and pain
· Bloating, mucous in stools, diarrhea, constipation, or alternating diarrhea and constipation
· Depression, anxiety, or stress
what are the 3 subtypes of IBS
o Diarrhea-predominant (IBS-D)
o Constipation-predominant (IBS-C)
o Alternating diarrhea and constipation
symptoms of IBD
· Abdominal pain or discomfort along with diarrhea, vomiting, and rectal bleeding
· Bloating, mucus in the stools, or a sense that you have not completely emptied your bowels
· Reduced appetite and unintended weight loss
· Most people’s symptoms are so mild that they never see a doctor for treatment
which symptoms are more common in Crohn's disease
· Diarrhea
· Abdominal pain and tenderness
· Loss of appetite and weight
· Fever
· Fatigue
· Rectal bleeding
· Perianal lesions
· Stunted growth in children
· Complications
o Fistula, perforation, abscess
· Upper gastrointestinal symptoms
· Extra-intestinal manifestations
Pathophysiology of IBD
· TLA1 immunological staining shows immune cell invasion in the intestinal tissues
o Not see in IBS, only IBD
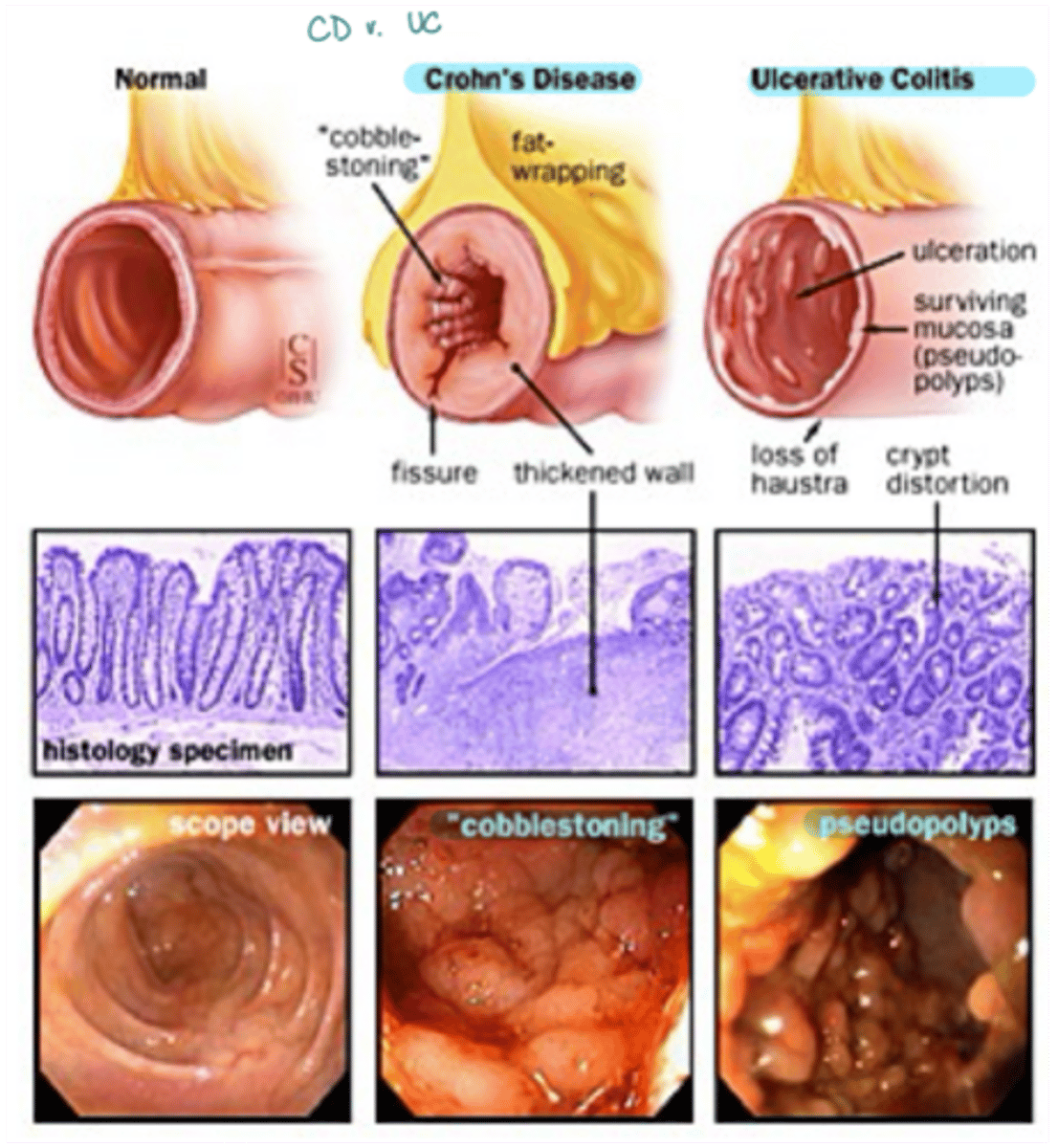
CD vs UC presentation
· CD usually presents as "cobblestoning"
· UC usually presents as pseudopolyps that are more segregated
IBD muscle movement
spasms contract the bowel
movement of GI muscles is thought to be uncoordinated
Instead of contracting and relaxing in waves, they contract irregularly and tend to spasm
extraintestinal manifestations of IBD
o Arthritis
o Osteoporosis
o Erythema nodosum
o Pyoderma gangrenosum
o Episcleritis
o Nutritional deficiency
o Hepatobiliary disease
incidence of IBD
· Third decade of life is the period of highest incidence of development
· Relapsing-remitting course of disease can occur
2 environmental risk factors for IBD
intestinal flora and smoking
2 hereditary risk factors for IBD
affected relatives (1st degree relative 10x risk)
genetic polymorphisms (NOD2/CARD15)
immune dysregulation risk factors for IBD
o Failure to down-regulate excess cytokine production
o Apoptosis-resistant immune cells
concordance of IBD
· Concordance for disease in monozygotic/ indentical twins (~50%)
o Much higher than in fraternal twins
genome-wide association study (GWAS) of IBD
o Method that searches the genome for single nucleotide polymorphisms that occur more frequently in people with a particular disease than in those without the disease
§ Compare patient DNA and non-affected people DNA to look for differences in SNPs that then may be associated with the disease
§ Then plotted as a Manhattan plot to look at which SNPs could be associated with the disease
what is the most important genetic loci associated with IBD
IBD1 on chromosome 3
NOD2/CARD15 impact on IBD
the susceptibility gene responsible for linkage of IBD1 locus with Crohn's disease
what are 3 common genetic mutations of CARD15
· Arg702Trp, Gly908Arg, and Leu1007Cis
o Having 2 mutated alleles vastly increases your risk of CD compared to 1 mutation
what are CARD15 mutations associated with?
not associated with UC, only CD
CARD15/NOD2 MOA in IBD
· gene encodes a protein that acts as an intracellular pattern recognition receptor
· CARD domains in protein are important for the activation of pro-inflammatory transcription factor NF-KB
o Mutation dysfunction inflammation
SAR of CARD15/NOD2
· The centrally located nucleotide-binding domain is important for oligomerization of the protein
· The C-terminal leucine-rich repeat region (LRR) provides recognition site for bacterial cell wall products
· NOD2 is a receptor for muramyl dipeptide, a component of the outer wall of certain bacteria
LRR domain of CARD15/NOD2
provides recognition site for bacterial cell wall products
The LRR domain sense of muramyl dipeptide (MDP) motif on a fragment of peptidoglycan (PG), which is a major component of the cell wall of gram-positive bacteria
what regulates CARD15/NOD2
inflammatory cytokines like TNF-a, IFN-y
what does a mutated CARD15/NOD2 do?
· The mutated NOD2/CARD15 protein is incapable of sensing lipopolysaccharides or peptidoglycans, and of initiating NF-kB signaling ad impairs its ability to eliminate invasive bacteria in intestinal epithelial cells
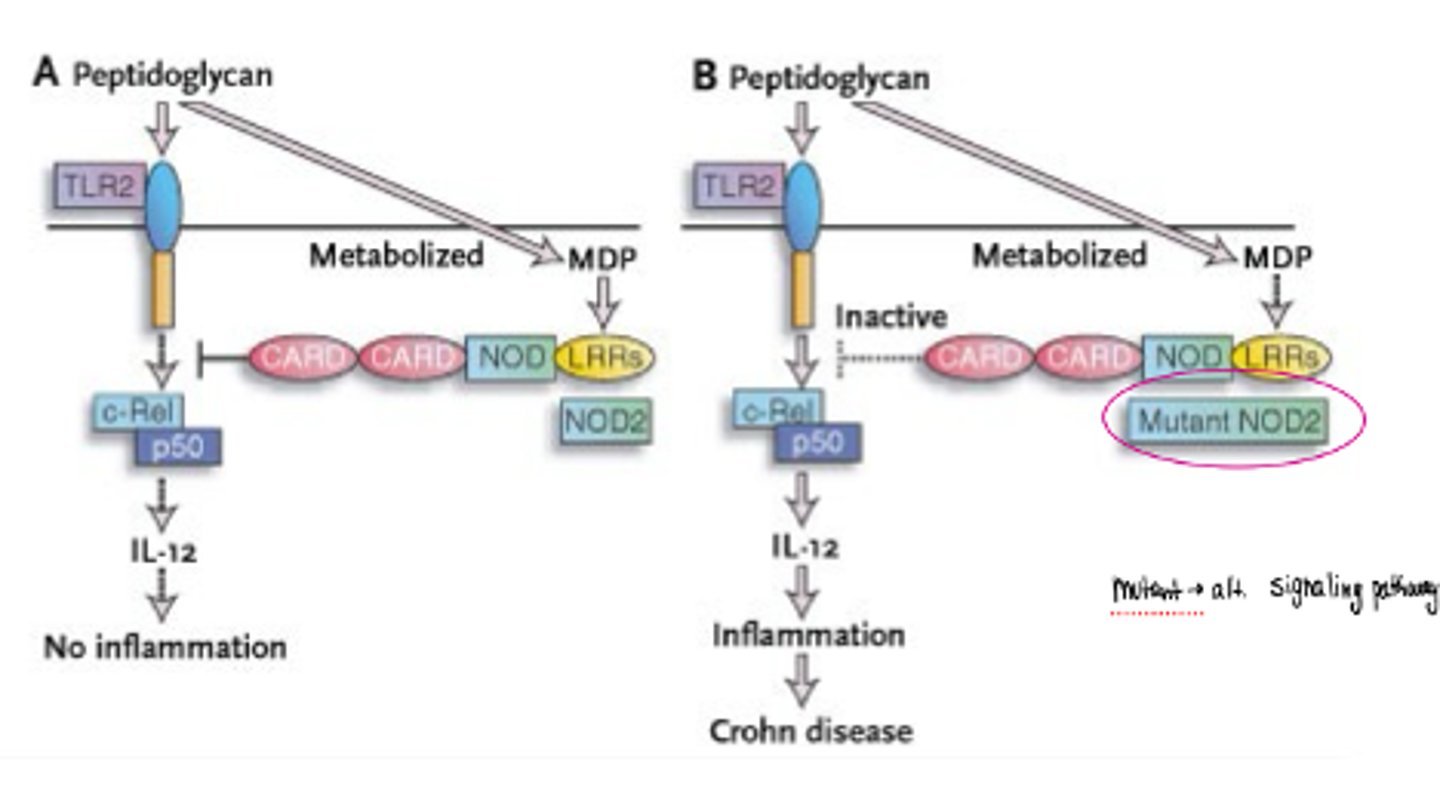
NOD2/CARD15 function
· plays a role in the immune response by recognizing the bacteria molecules which possess the muramyl dipeptide (MDP) and by activating the NF-kB system (c-rel/p50)
immune dysregulation in Crohn's disease
Th1 polarization
o Excessive production of IFN-y, TNF-a, and Il-12
§ Pro-inflammatory cytokines
o Stimulate extravasation of leukocytes at the site of disease
immune dysregulation in Ulcerative colitis
Th2 polarization
o IL-4 and IL-5
o Also have elevated IFN-y and TNF-a (not solely Th2-polarized disease)
Th1 functions
more inflammatory
o Cell-mediated immunity and inflammation
o Intracellular pathogens
§ Viruses, bacteria
o Autoimmunity
o Inflammation
Th2 functions
more allergenic
o Antibody-mediated immunity
o Extracellular parasites
o Asthma, allergy
how does serotonin related to GI disorders
o An imbalance of serotonin in the gut
o An improper reaction of the digestive system to serotonin
o A faulty communication network between serotonin in the gut and the brain and spinal cord
serotonin 2 major roles
modulating intestinal movement and perception of pain
mycobacterium paratuberculosis and IBD
· Mycobacterium paratuberculosis has been identified in CD tissues
o Experts don’t regard it as a biologically plausible factor/cause of IBD
Measles + measles vaccine and IBD
Available evidence doesn’t support an association between IBD and measles infection OR vaccinations
smoking and IBD
is positively correlated with CD
is negatively correlated with UC
may be due to vascular effect of cigarette smoke with CD
bacteria and IBD
o Some bacteria initiate uncontrolled inflammation
o Probiotics can inhibit inflammation