L24- Brain Ageing
1/50
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
51 Terms
what are the main external brain divisions
frontal lobe
temporal lobe
occipital lobe
parietal lobe
brainstem
cerebellum
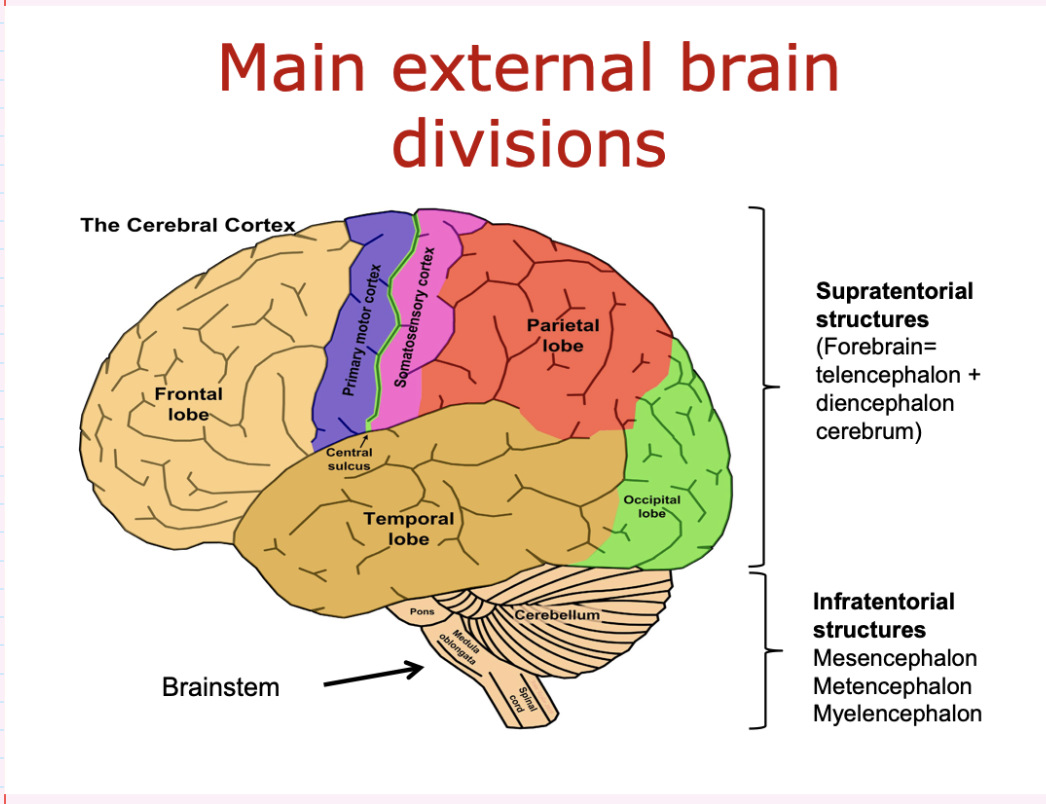
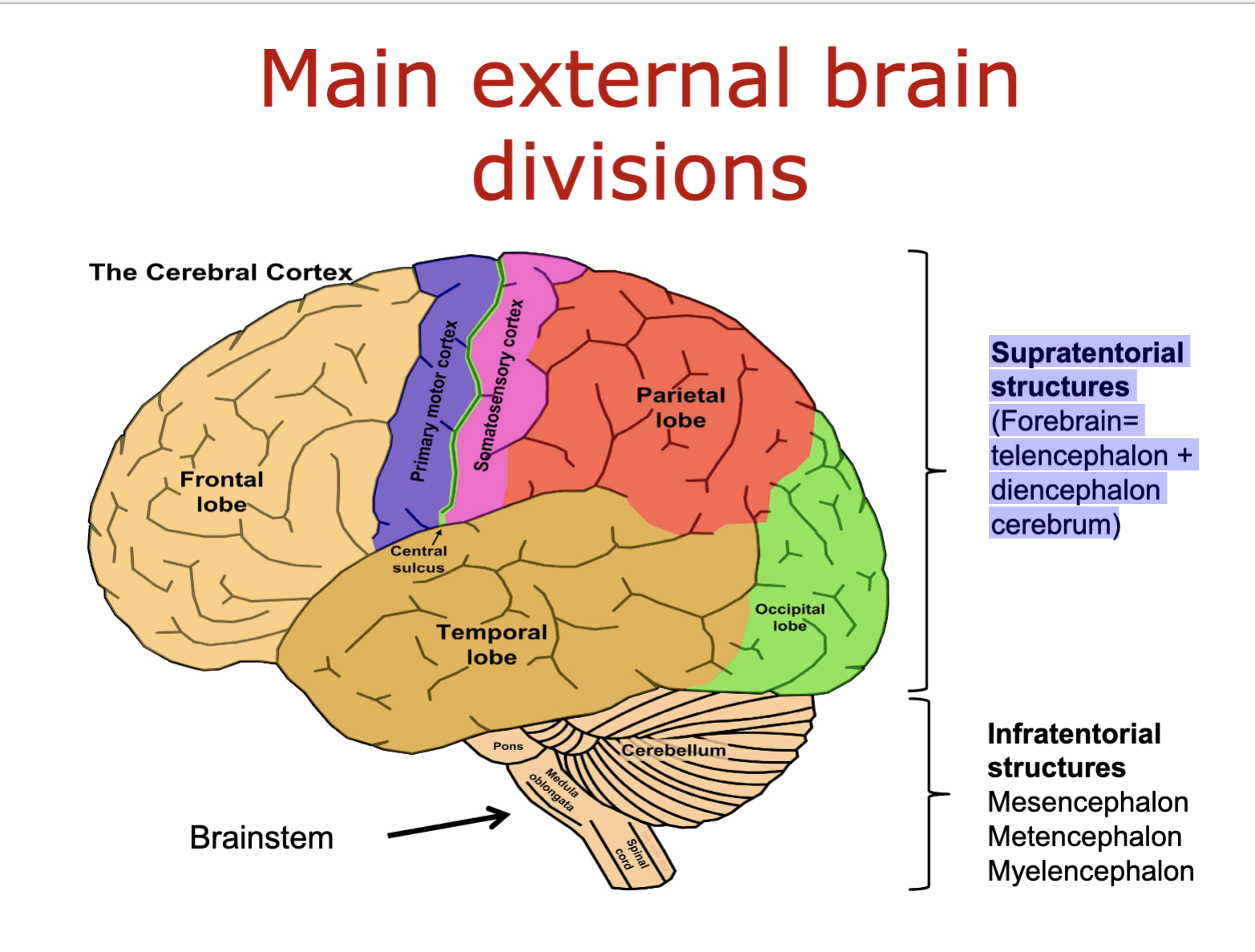
what are the supratentorial structures of the brain
forebrain:
telencephalon
diencephalon cerebrum
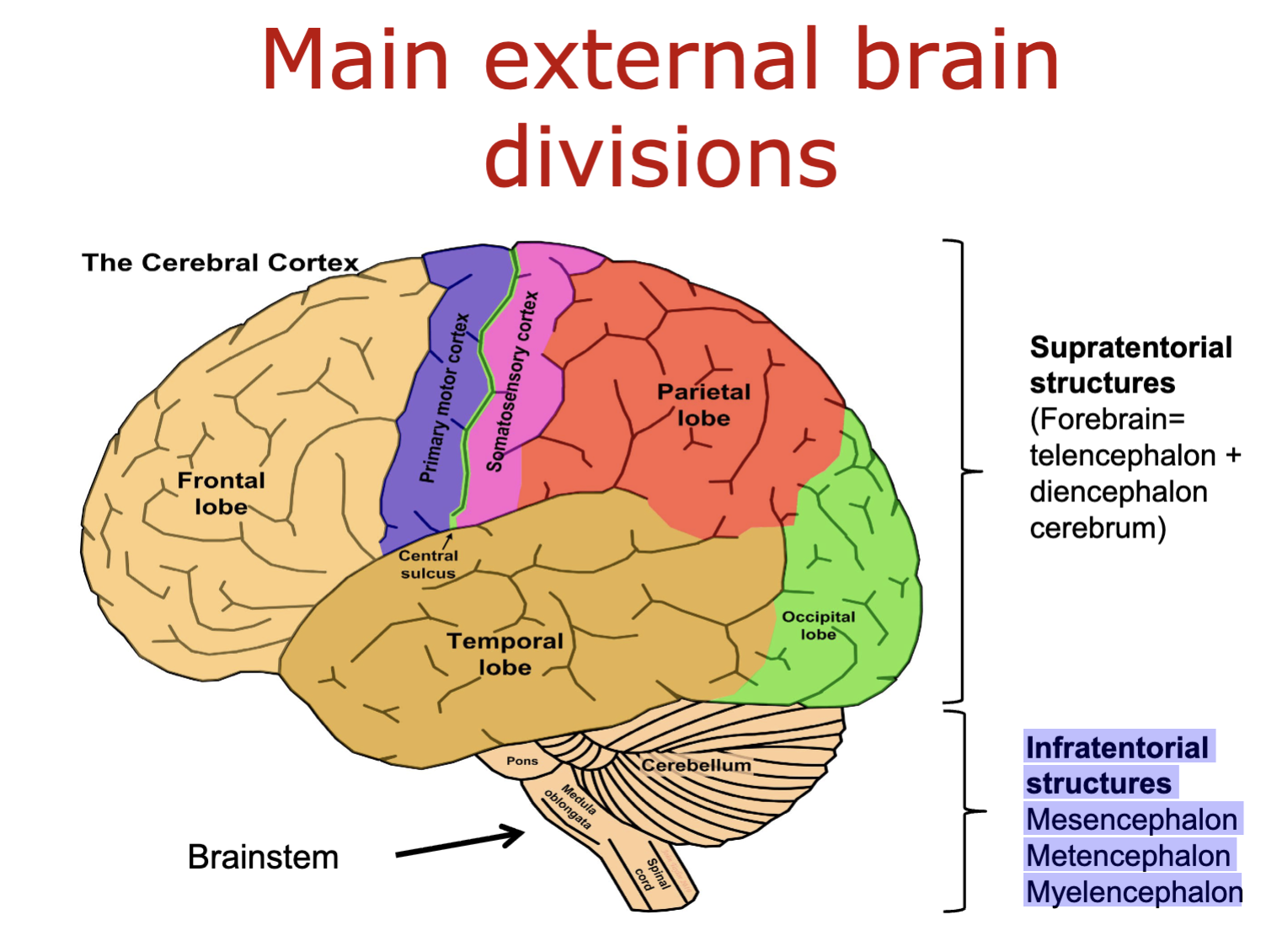
what are the infratentorial structures of the brain
Mesencephalon
Metencephalon
Myelencephalon
what are the different types of neurones in the brain
multipolar neurones
interneurones
motorneurones
sensory/bipolar neurones
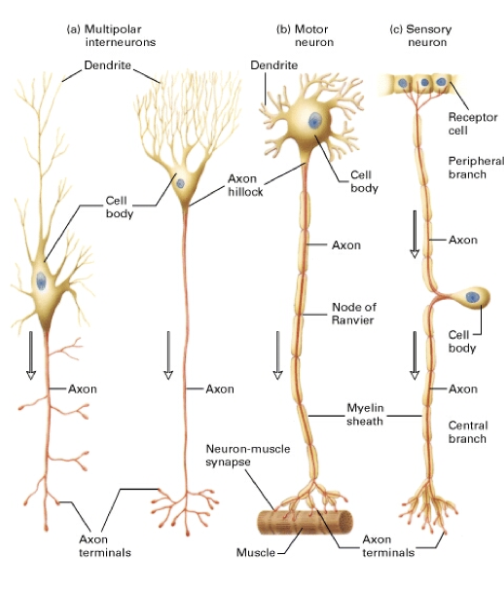
what do multipolar neurones do
Interneurones- form all the neural wiring within the CNS.
Motor Neurons- carry signals from the CNS to muscles and glands (efferent neurones).
Multipolar neurones have many processes originating from the cell body (e.g. spinal motor neurones, pyramidal neurones, Purkinje cells.)
what do sensory/bipolar neurons do
Carry messages from the body's sense receptors (eyes, ears, etc.) to the CNS (afferent neurones)
Account for 0.9% of all neurones
They have two axons (instead of an axon and a dendrite). One axon communicates with the sense organ; the other axon communicates with the CNS (e.g. dorsal root ganglion cells in the spinal cord).
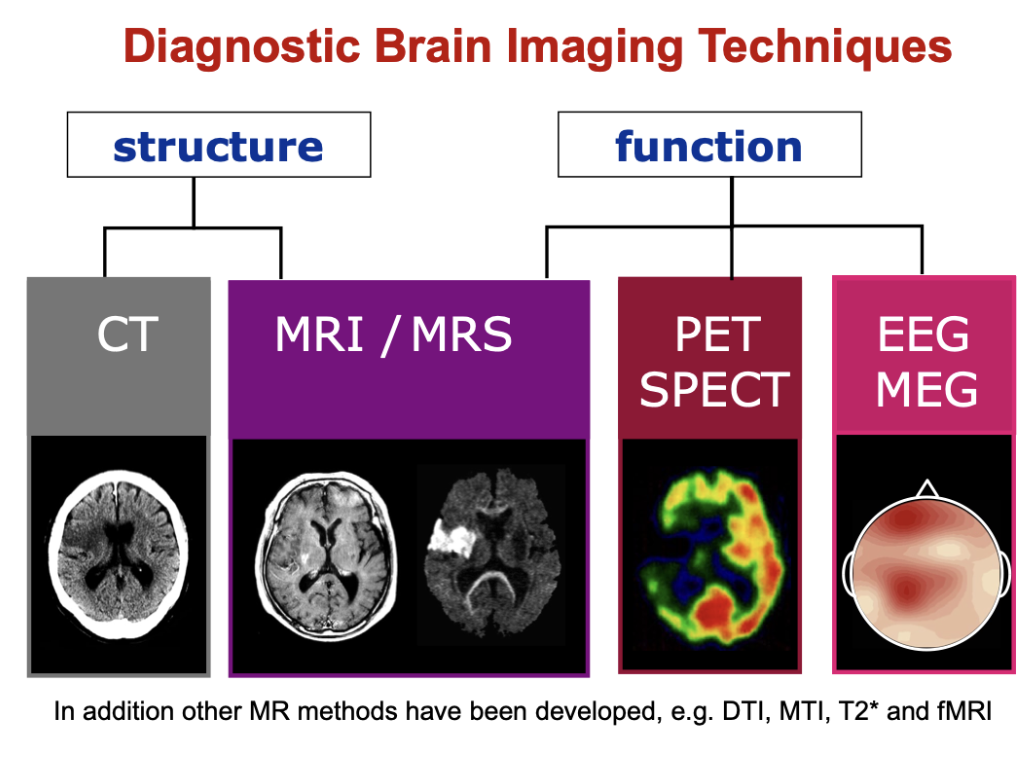
what are the 2 forms of diagnostic brain imaging techniques
structure- CT and MRI/MRS
function- PECT/SPECT and EEG/MEG
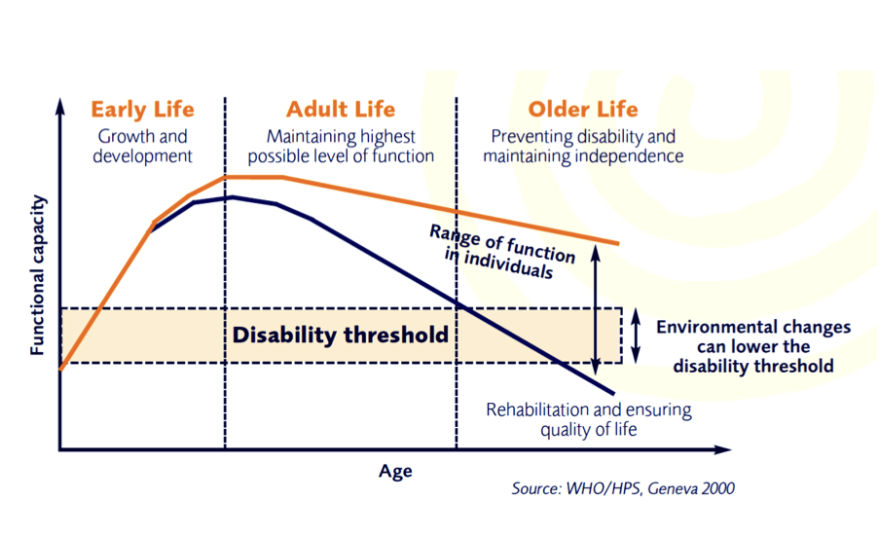
how does the functional capacity of the brain change throughout life
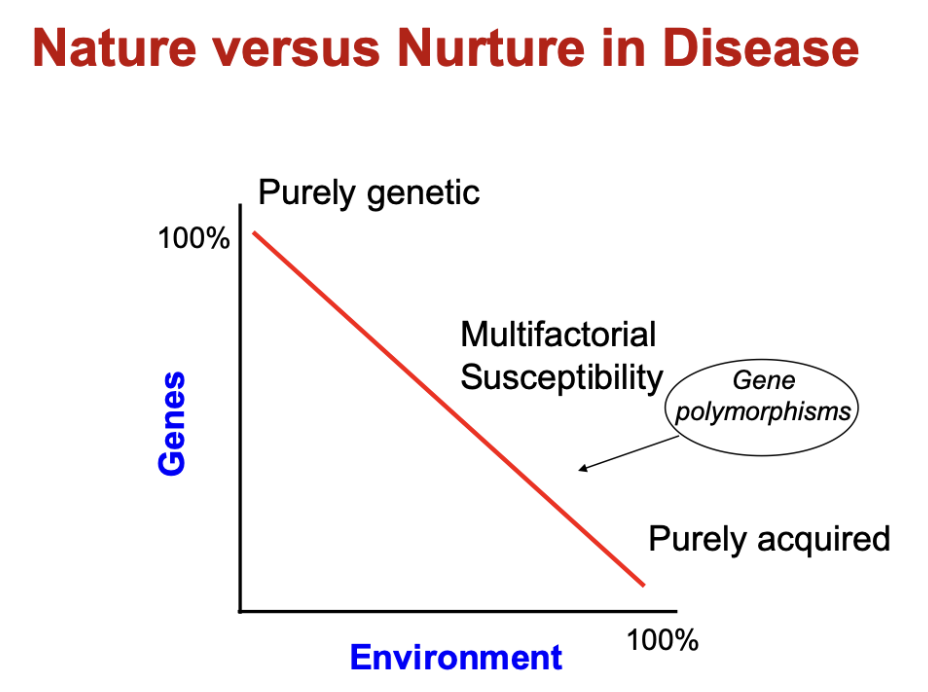
what is meant by multifactorial susceptibility
a mix of genetic and acquired causes
how does ageing and brain function relate
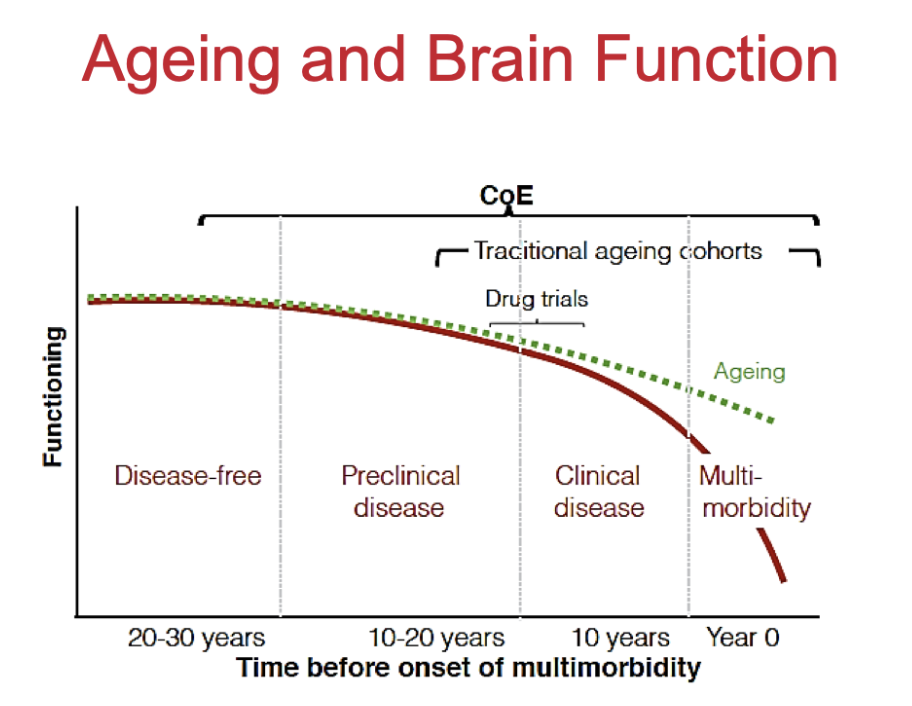
what happens to the brain as we age
ventricles enlarge
cortex gets thinner- lose about 0.5% per year
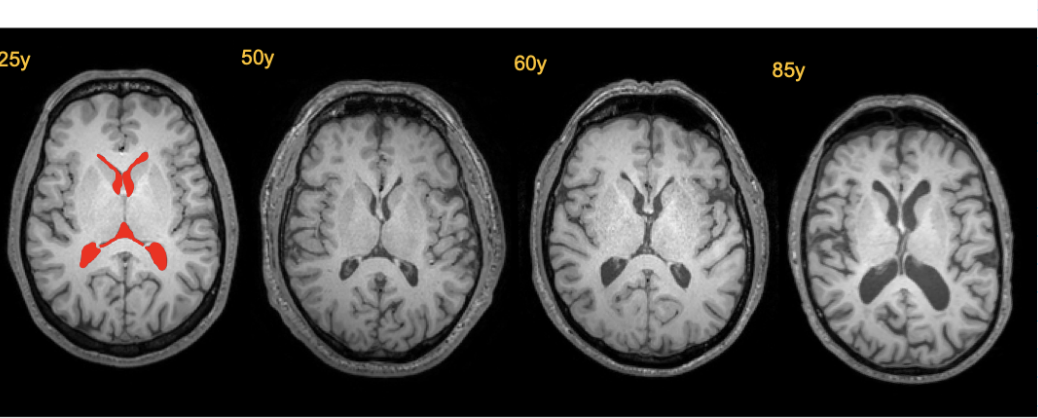
what happens to brain atrophy during ageing
Reduced brain volume (atrophy)
Widened sulci (more space between gyri)
Enlarged ventricles
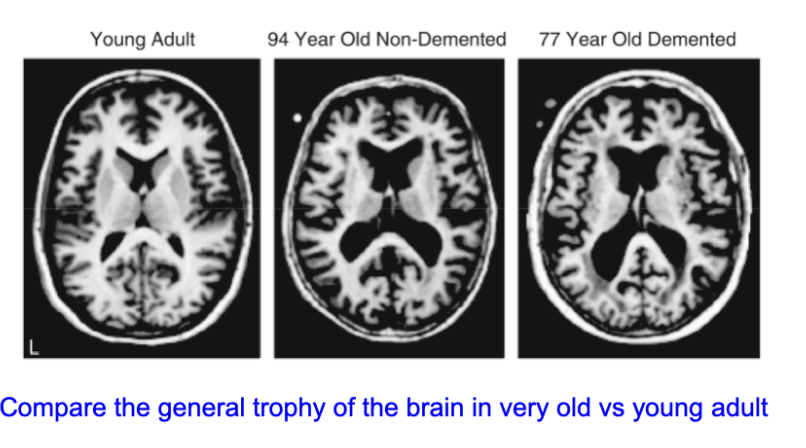
In dementia:
Changes are more pronounced
Greater loss of cortical and subcortical tissue
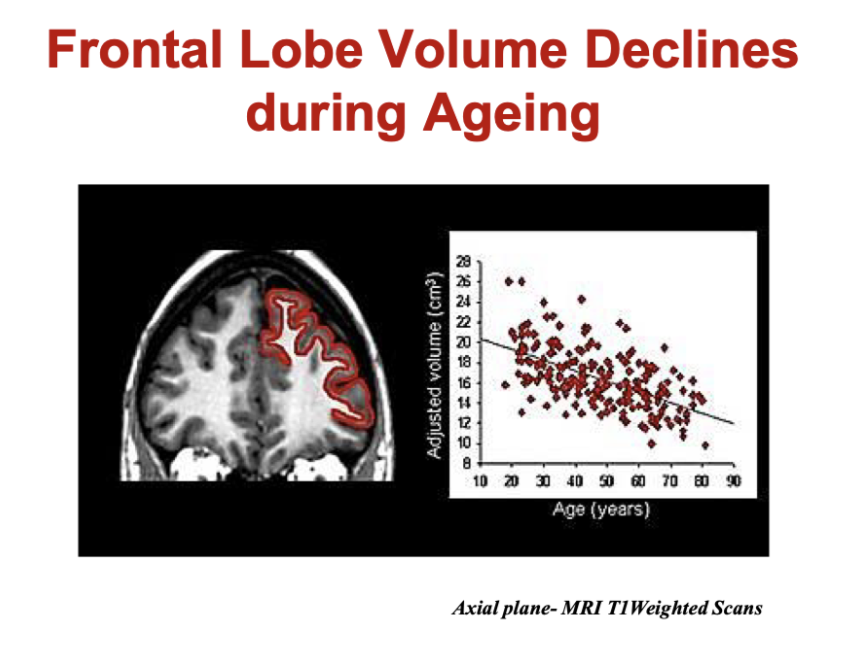
what happens to the frontal lobe during ageing
frontal lobe volume declines during ageing
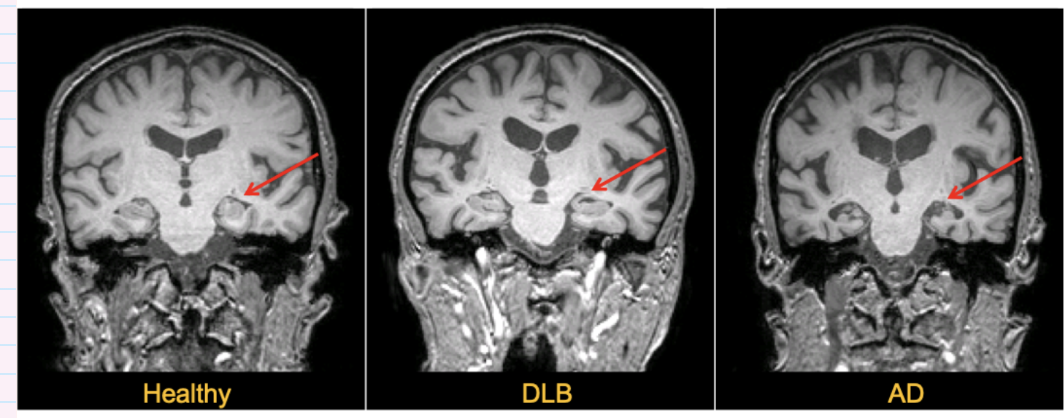
what happens to brain structure in dementia
atrophy is greater in alzheimer’s diseases (AD) than in dementia with lewy bodies (DLB)
atrophy of medial temporal lobes structures most likely in AD
Which brain regions show early volume loss in Alzheimer’s disease?
Early atrophy occurs in:
Hippocampus
Entorhinal cortex
Compared to healthy ageing:
AD shows greater and earlier volume loss in these regions
Key idea:
These areas are critical for memory → explains early memory symptoms in AD
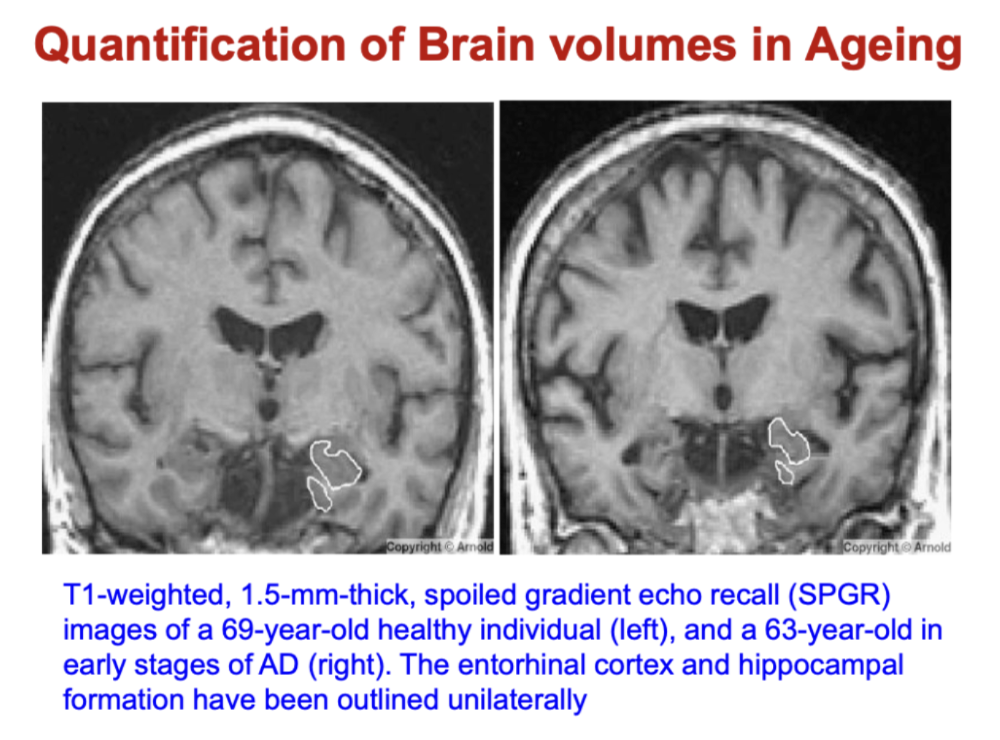
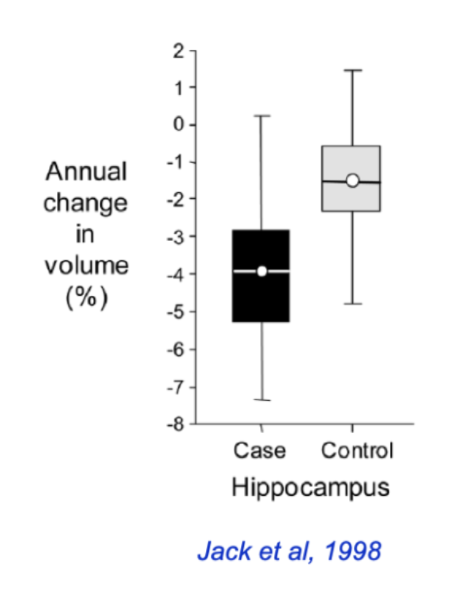
How does hippocampal atrophy differ between normal ageing and Alzheimer’s disease?
Normal ageing:
~1.6% volume loss per year
Alzheimer’s disease (AD):
~4.0% volume loss per year
≈ 2× faster atrophy than controls
Key idea:
Ageing → gradual hippocampal loss
AD → accelerated medial temporal lobe atrophy
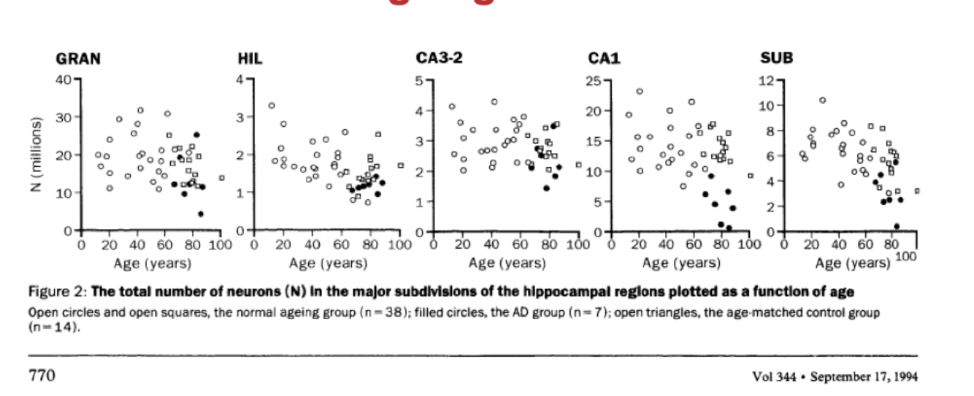
what are the patterns of hippocampal neuronal loss in ageing and AD
most distinctive AD related neuron loss was seen in the CA1 region (hippocampus subfield)- in normal ageing pr MCI almost no neuron loss
- neurodegenerative processes associated with AD qualitatively different- AD is not accelerated by ageing but a distinct pathological process
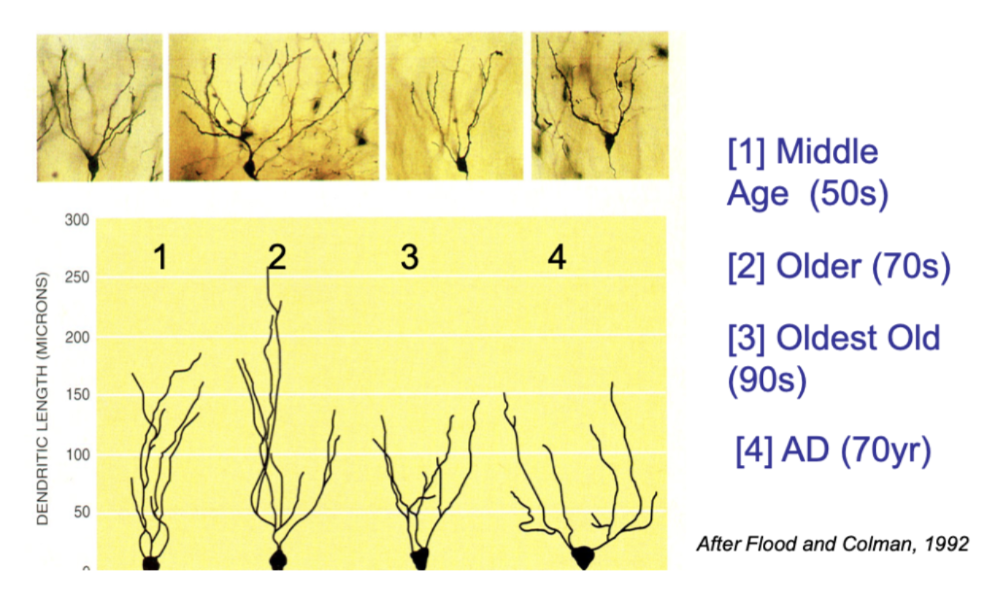
how does the appearance of hippocampal neurones change during ageing
With ageing:
Reduced dendritic length and branching
Simpler neuronal structure (less connectivity)
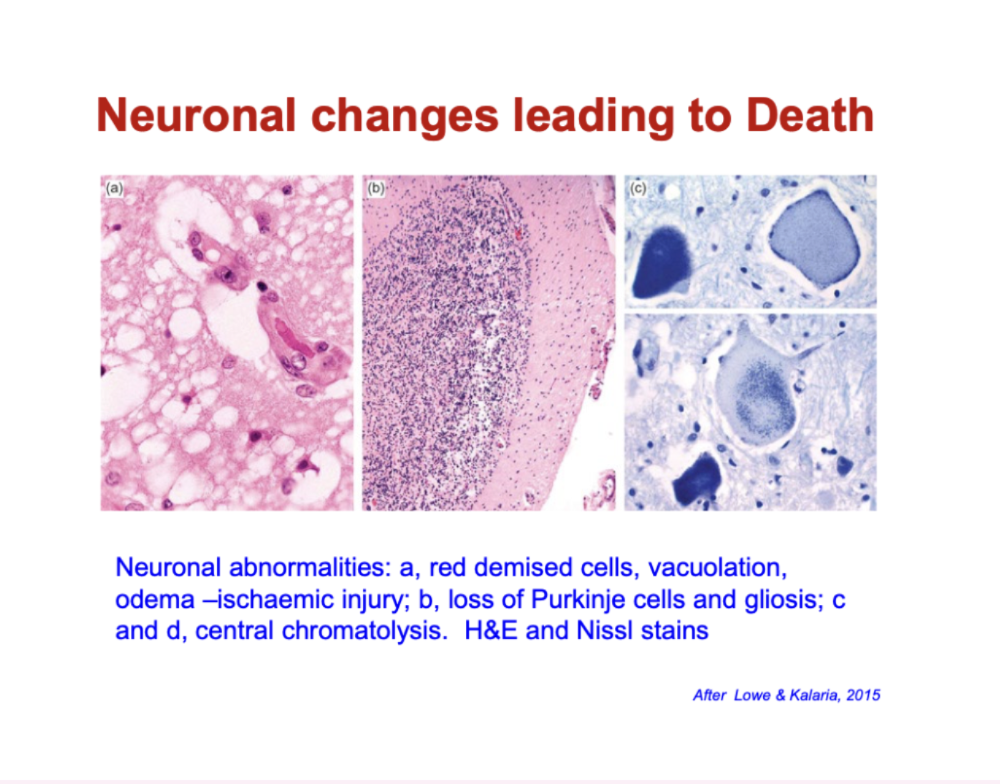
What histological changes indicate neuronal injury and death?
Early injury (e.g. ischaemia):
“Red neurons” (shrunken, intensely stained)
Vacuolation & oedema (cell swelling/damage)
Progression:
Loss of neurons (e.g. Purkinje cells)
Gliosis (increase in supporting glial cells after injury)
Cellular breakdown:
Chromatolysis (loss/disruption of Nissl substance → impaired protein synthesis)
what are the changes in mechanisms of neurodegeneration during ageing
↑ Oxidative stress mechanisms
↑ Neuroinflammatory responses
↑ Abnormal Protein-Protein Interactions
↓The Ubiquitin-Proteasome system
↑ The autophagy-lysosome system (autophagy)
↑ Apoptosis and delayed cell death
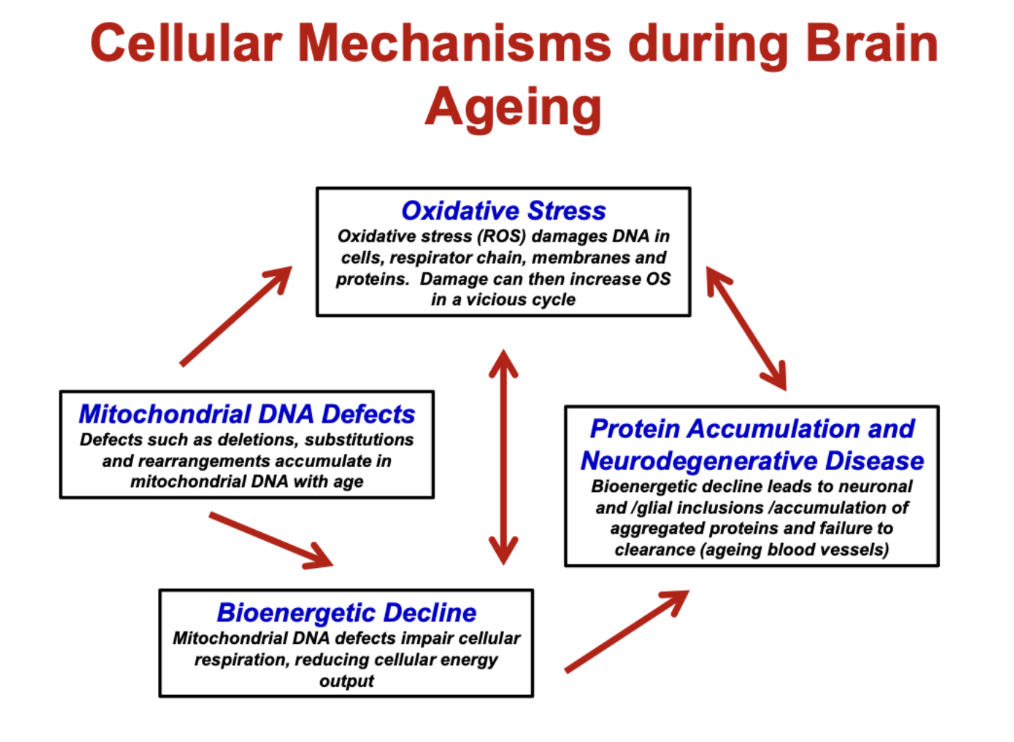
What are the key cellular mechanisms driving brain ageing?
Oxidative stress (ROS):
Damages DNA, proteins, membranes
Creates a vicious cycle of further damage
Mitochondrial DNA defects:
Accumulate with age
Impair mitochondrial function
Bioenergetic decline:
↓ cellular respiration → ↓ energy (ATP)
Protein accumulation:
Misfolded/aggregated proteins build up
Impaired clearance → neurodegeneration
Key idea:
These processes are interconnected and amplify each other → neuronal dysfunction and disease
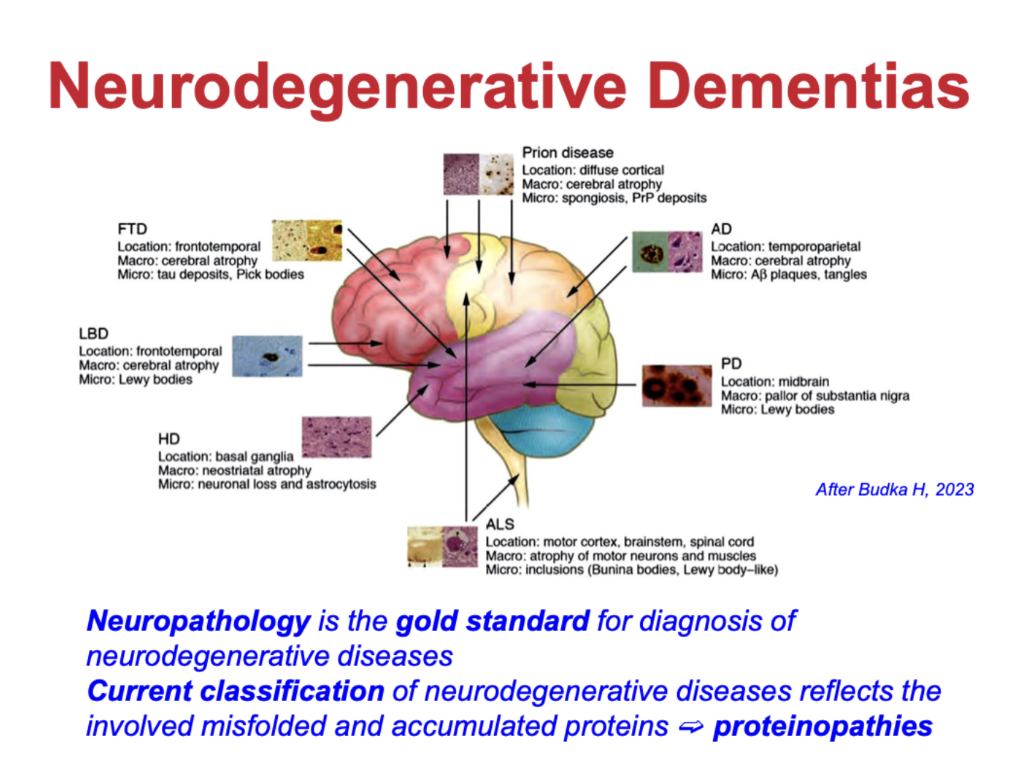
How are neurodegenerative dementias classified?
Classified by misfolded/accumulated proteins → “proteinopathies”
Examples:
Alzheimer’s disease (AD): Aβ plaques, tau tangles
Parkinson’s disease (PD) / Lewy body dementia: α-synuclein (Lewy bodies)
Frontotemporal dementia (FTD): tau or TDP-43
Prion diseases: misfolded prion protein
Huntington’s disease (HD): mutant huntingtin
ALS: protein inclusions (e.g. TDP-43)
Neuropathology = gold standard for diagnosis
Disease type depends on which protein accumulates and where in the brain
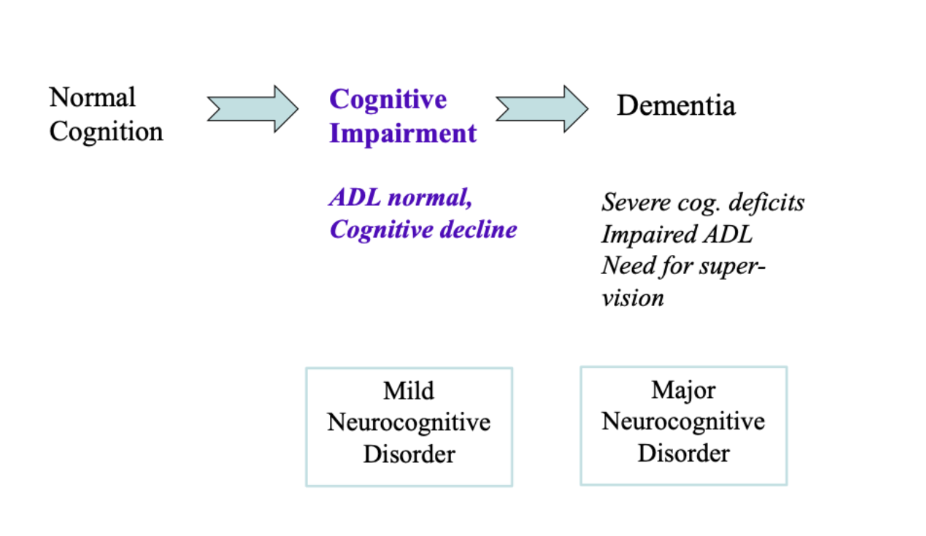
how do we define dementia
impairment in any of
memory
language
visual processing and orientation
mood, personality and social skills
frontal executive function, including planning and problem solving
causes inability to function independently
how does normal cognitive state change over time
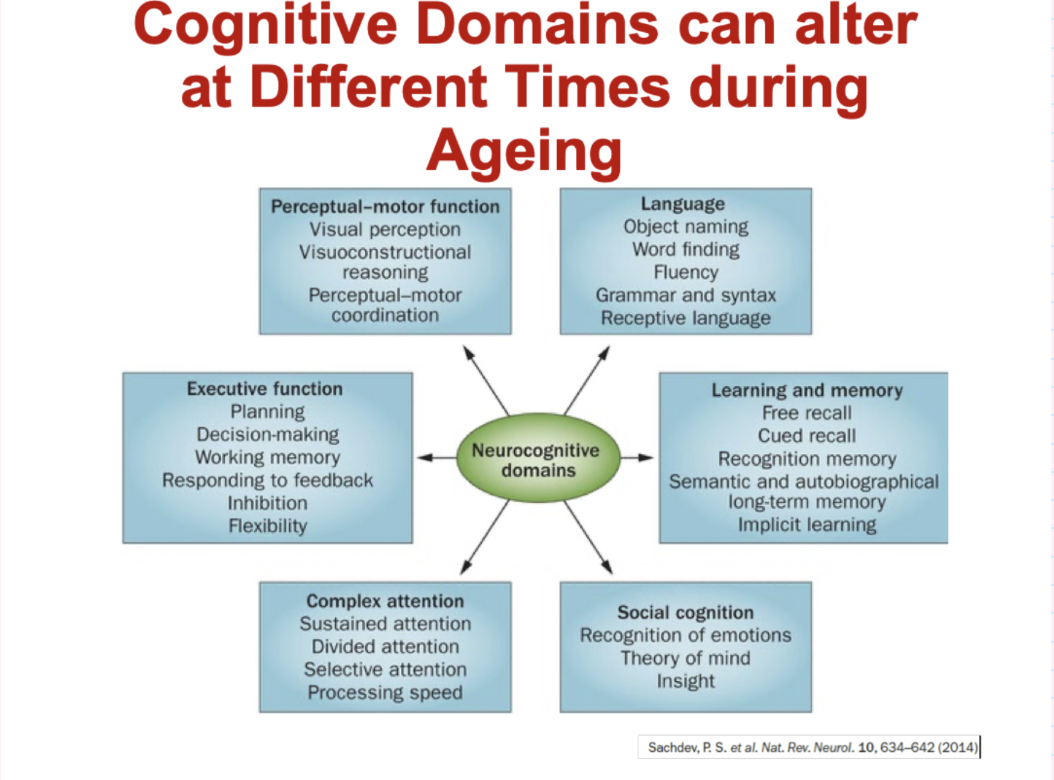
Which cognitive domains are affected during ageing?
Executive function: planning, decision-making, working memory, flexibility
Memory & learning: recall (free/cued), recognition, long-term memory
Language: word finding, fluency, grammar, comprehension
Attention: sustained, divided, selective attention, processing speed
Perceptual-motor: visual perception, coordination, visuospatial skills
Social cognition: emotion recognition, theory of mind, insight
Different domains decline at different rates and times during ageing
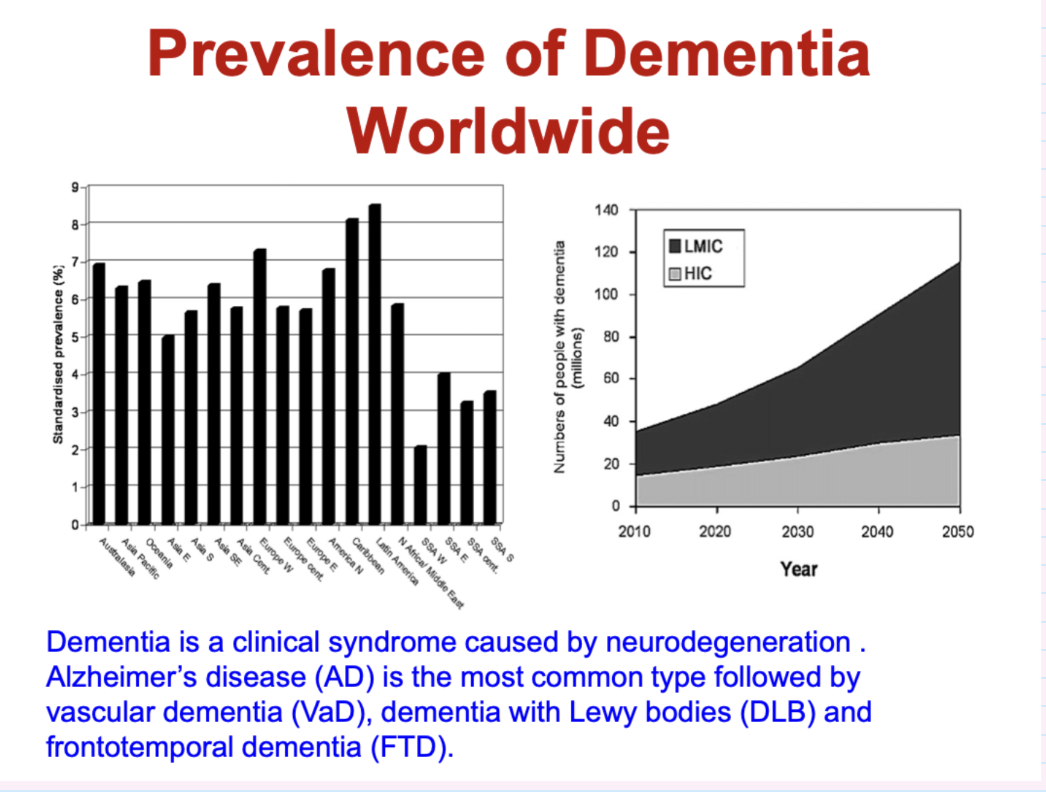
describe the prevelence if dementia worldwide
Dementia is a clinical syndrome caused by neurodegeneration . Alzheimer’s disease (AD) is the most common type followed by vascular dementia (VaD), dementia with Lewy bodies (DLB) and frontotemporal dementia (FTD).
what are the most common causes of degenerative dementias
Alzheimer’s disease: ~55–70% (most common)
Vascular dementia: ~15–25%
Other dementias (10–30%):
Lewy body dementia
Parkinson’s disease dementia
Frontotemporal dementia
whatt are the 4 types of dementia
alzheimer’s (50-75%)
vascular (20-30%)
lewy body (10-25%)
frontotemporal (10-15%)
give 6 common ageing related brain disorders and dementias
Alzheimer’s Disease
Parkinson’s Disease
Dementia with Lewy Bodies
Frontotemporal Dementia
Prion Diseases
Vascular Dementia
what is alzheimer’s disease
a progressive degenerative brain disorder and the most common cause of dementia
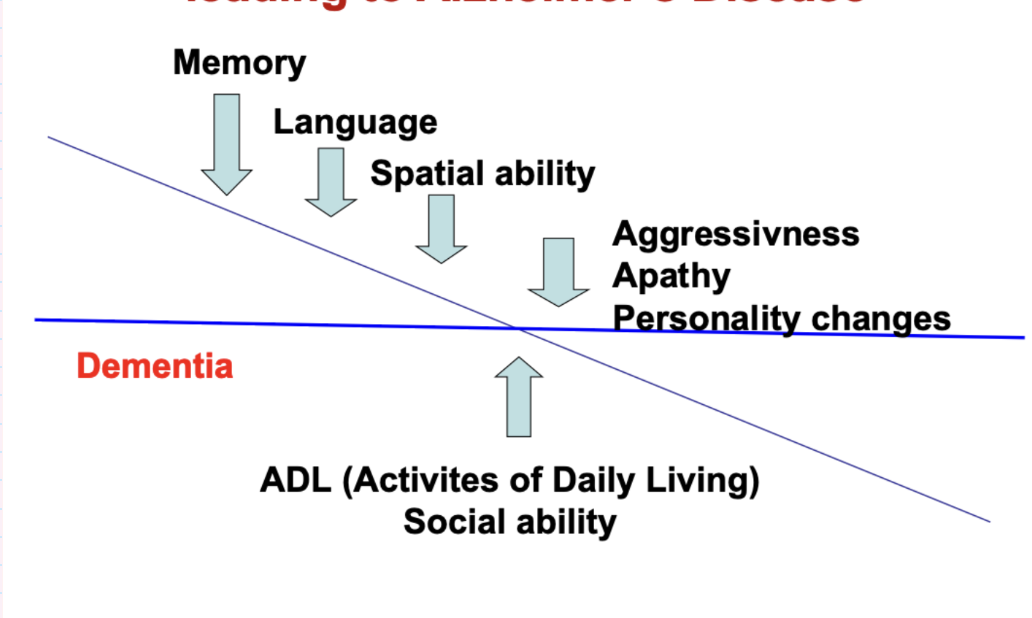
how do cognitive ageing related thresholds lead to alzheimer’s disease
once decline affects ADL (activities of daily living) and social ability- considered dementia
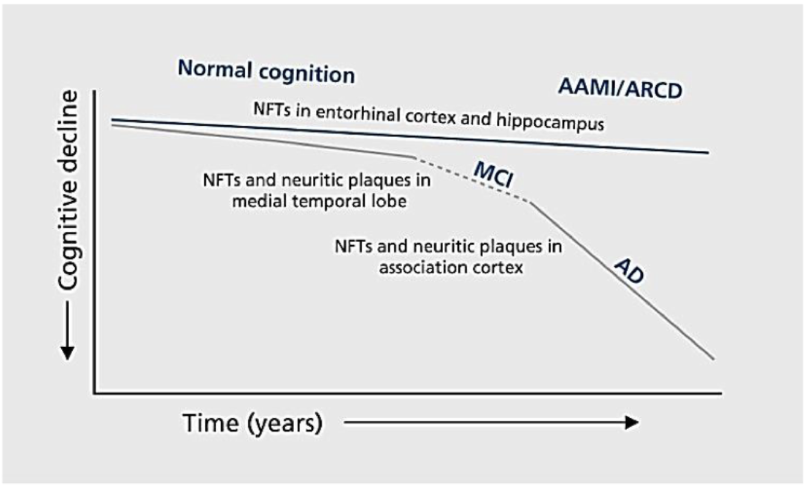
how does cognition and brain pathology cange during ageing
progressive accumulation of brain pathology increases damage and decreases cognitive functions
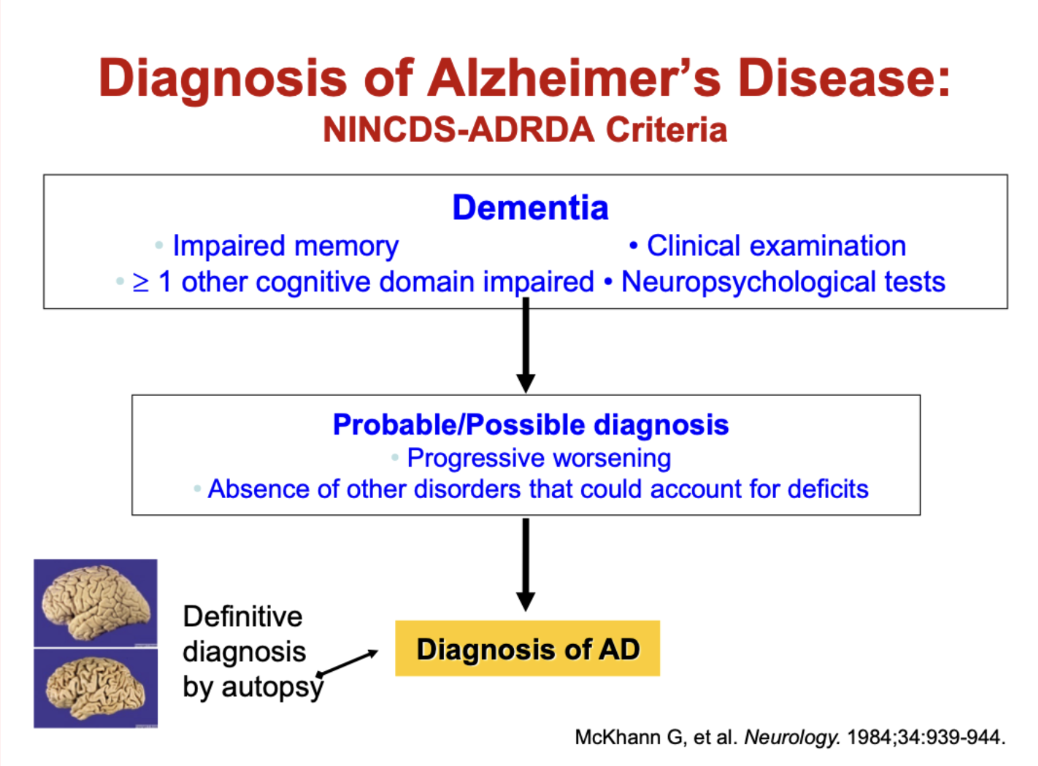
How is Alzheimer’s disease diagnosed (NINCDS-ADRDA criteria)?
Dementia required:
Impaired memory
≥1 other cognitive domain impaired
Assessed by clinical exam + neuropsychological testing
Probable/Possible AD:
Progressive worsening over time
No other disorder explaining symptoms
Definitive diagnosis:
Confirmed by autopsy
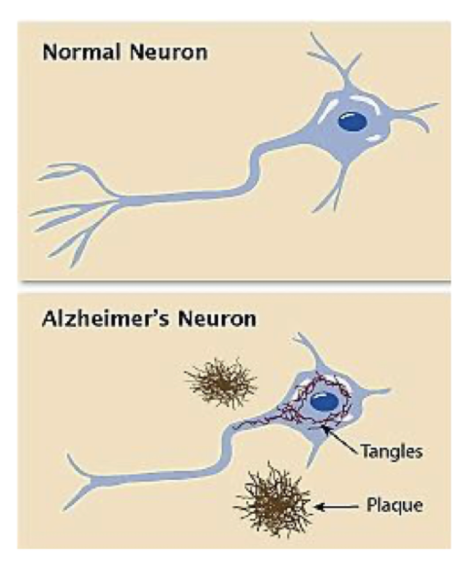
what are the key pathological hallmarks od AD
accumulation of brain pathology with age
amyloid or neuritic plaques (NP)
neurofibrillary tangles (NFT)
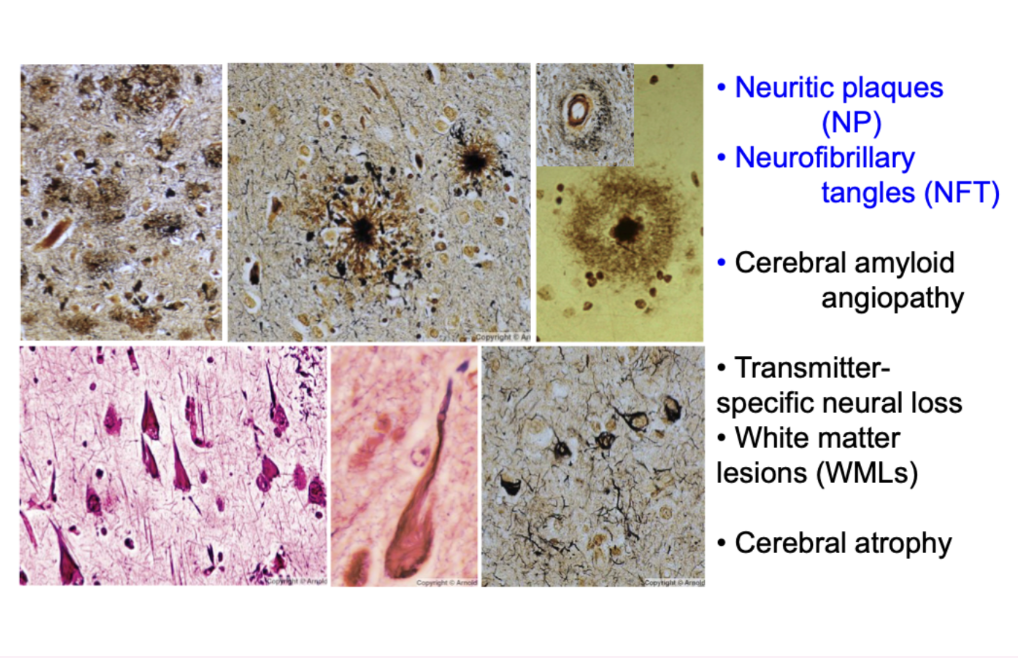
what are he pathological features of AD
neuritic plaques (NP)
neurofibrillary tangles (NFT)
cerebral amyloid angiopathy
transmitter-specific neural liss
white matter lesions (WML)
cerebral atrophy
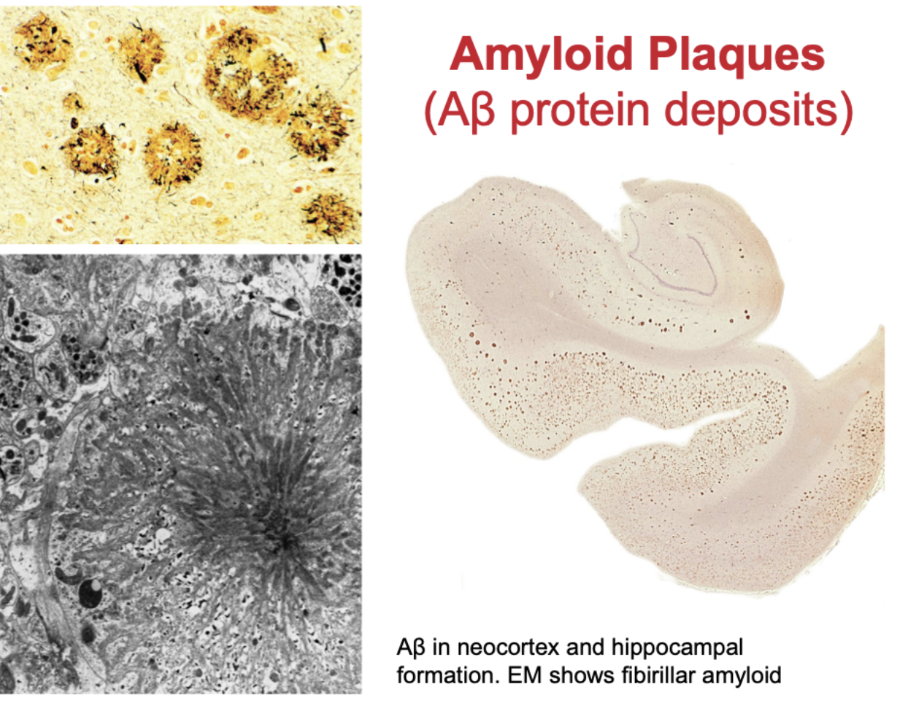
describe the change in brain amyloid plaques with ageing
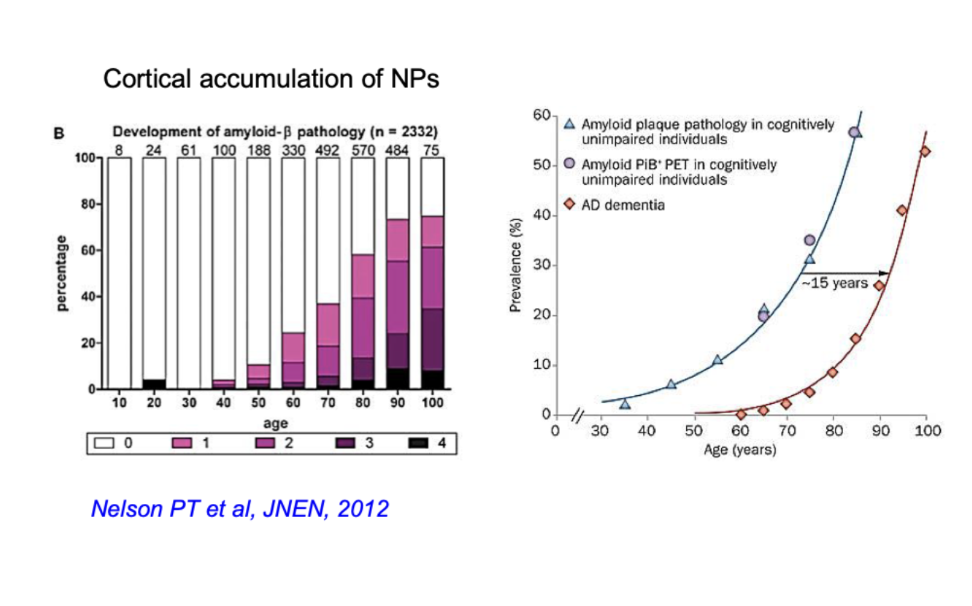
what are amyloid plaques
Aβ protein deposits
Aβ in neocortex and hippocampal formation- EM shows fibrillae amyloid
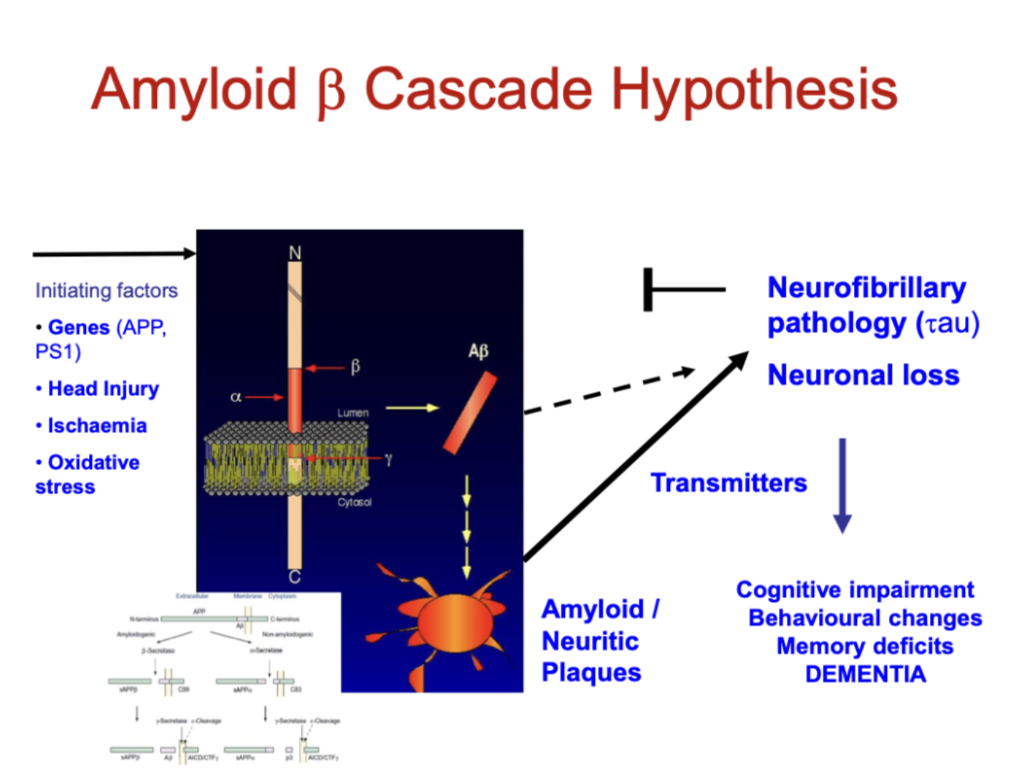
What initiates the amyloid β cascade in Alzheimer’s disease?
Triggers:
Genetic mutations (APP, PS1)
Head injury
Ischaemia
Oxidative stress
Key process:
Abnormal APP processing → amyloid-β (Aβ) production
Aβ aggregates → amyloid (neuritic) plaques
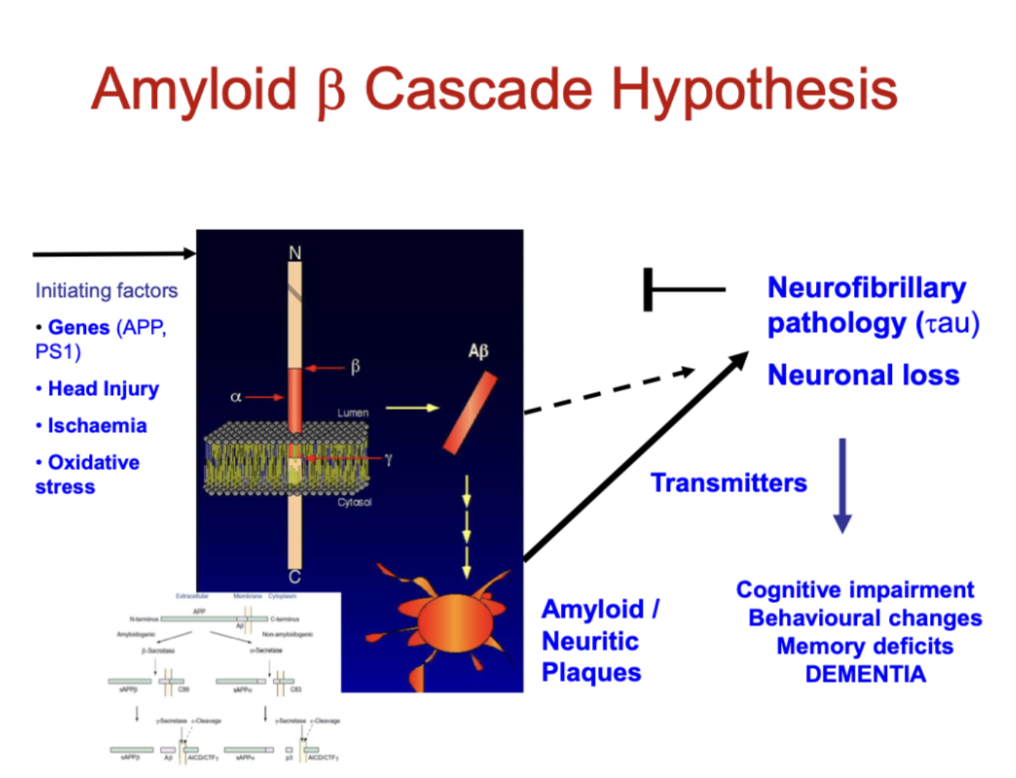
What are the downstream effects of the amyloid β cascade?
Pathological changes:
Tau pathology (neurofibrillary tangles)
Neuronal loss
Neurotransmitter deficits
Clinical outcome:
Cognitive impairment
Memory loss
Behavioural changes → Dementia
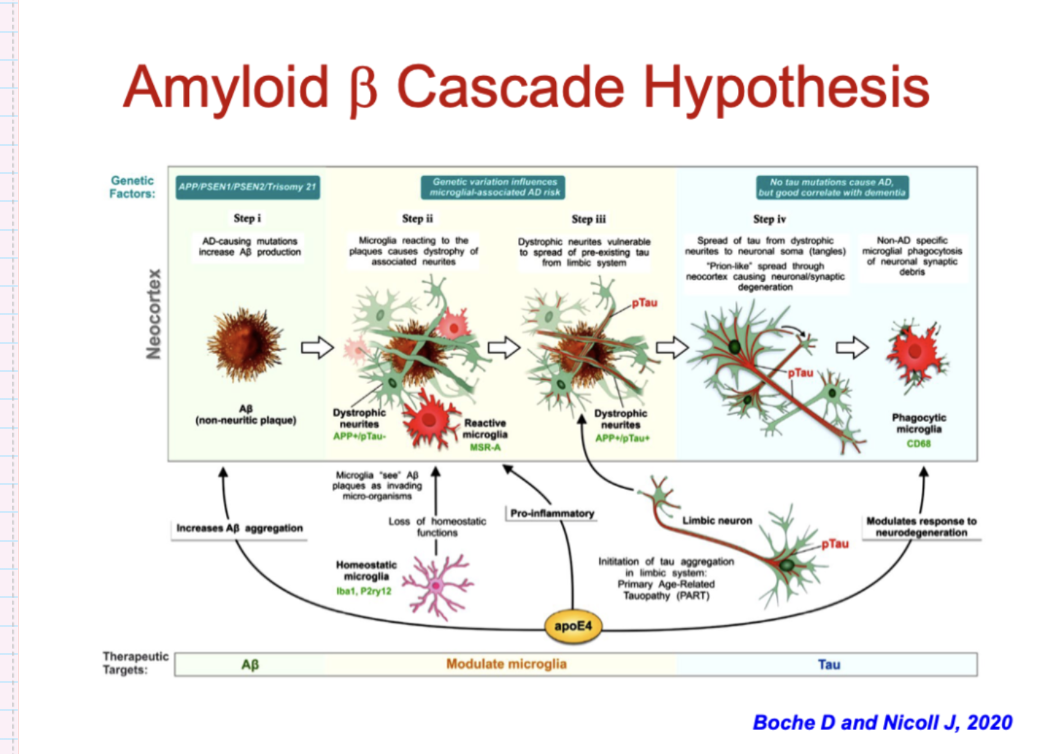
What does the updated Amyloid β cascade hypothesis explain?
Aβ accumulation (genetic risk) initiates disease
Microglia become activated → inflammation + loss of normal function
Neuronal damage develops around plaques
Tau pathology spreads through the brain (prion-like)
Leads to progressive neuronal and synaptic loss
Key idea:
Alzheimer’s is a multistep process involving Aβ, inflammation, and tau → ultimately causing dementia
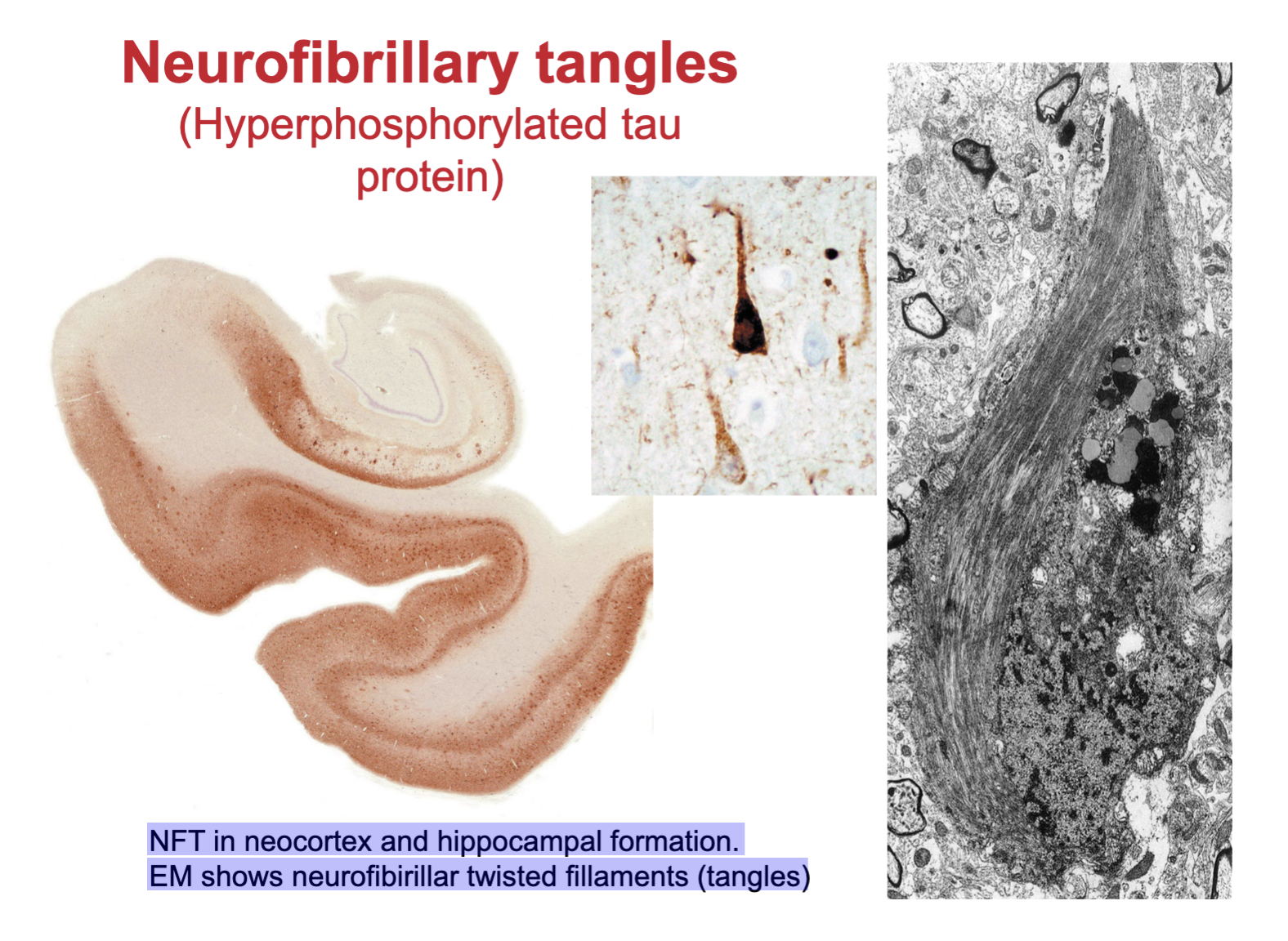
what are neurofibrillary tanges
Hyperphosphorylated tau protein
NFT in neocortex and hippocampal formation.
EM shows neurofibrillary twisted filaments (tangles)
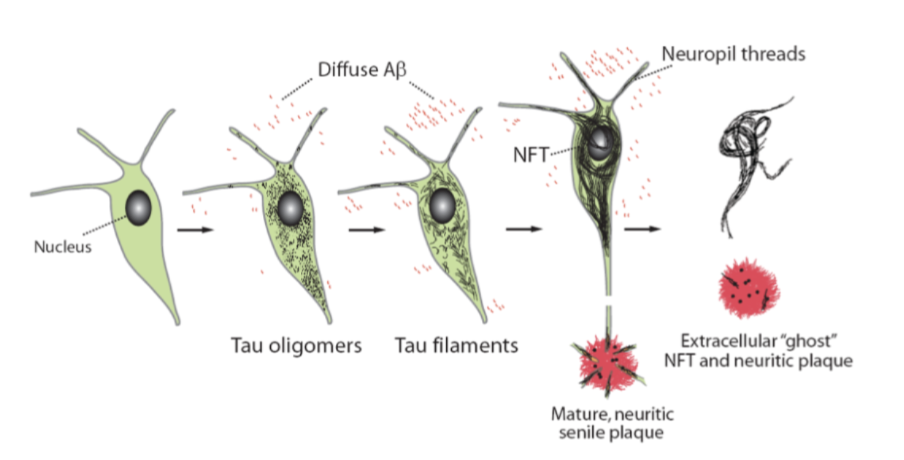
describe the progression of tau positive neurofbrillary pathology
Tau changes from normal → oligomers → filaments → neurofibrillary tangles (NFTs)
NFTs accumulate inside neurons → disrupt function
Neurons degenerate → release tau → extracellular “ghost” tangles
Associated with neuritic plaques and neuropil threads
Key idea:
Tau pathology progressively damages neurons and spreads, driving neurodegeneration
What are the main molecular classes of neurodegenerative dementias?
Alzheimer’s disease (Aβ + tau)
Synucleinopathies:
Dementia with Lewy bodies (DLB)
Parkinson’s disease dementia (PDD)
Tauopathies:
Frontotemporal dementia (FTD), PSP, CBD, Pick’s disease
What other disorders can cause neurodegenerative dementia?
Frontotemporal dementias (non-tau):
TDP-43, ubiquitin, progranulin
Prion diseases:
Creutzfeldt-Jakob disease, etc.
Trinucleotide repeat disorders:
Huntington’s disease, spinocerebellar ataxias
Motor neuron diseases:
ALS, PLS, SMA (with dementia)
Key idea:
Dementias are classified by underlying protein pathology
What protein accumulations are associated with major neurodegenerative diseases?
Alzheimer’s disease: Aβ plaques, tau
Parkinson’s / DLB: α-synuclein (Lewy bodies)
Tauopathies (FTD, PSP, CBD, Pick’s): tau (3R/4R)
FTD (non-tau): TDP-43, ubiquitin, progranulin
Prion diseases: PrP plaques
What is the key pathological mechanism in neurodegenerative proteinopathies?
Diseases involve misfolded proteins that:
Form intracellular inclusions or extracellular deposits
Are insoluble and aggregate
Spread via “seeding” mechanism (prion-like propagation)
Examples:
Synuclein (Parkinson’s, MSA)
Tau (FTD, AD)
Polyglutamine (Huntington’s)
Key idea:
Neurodegeneration is driven by toxic protein accumulation and spread
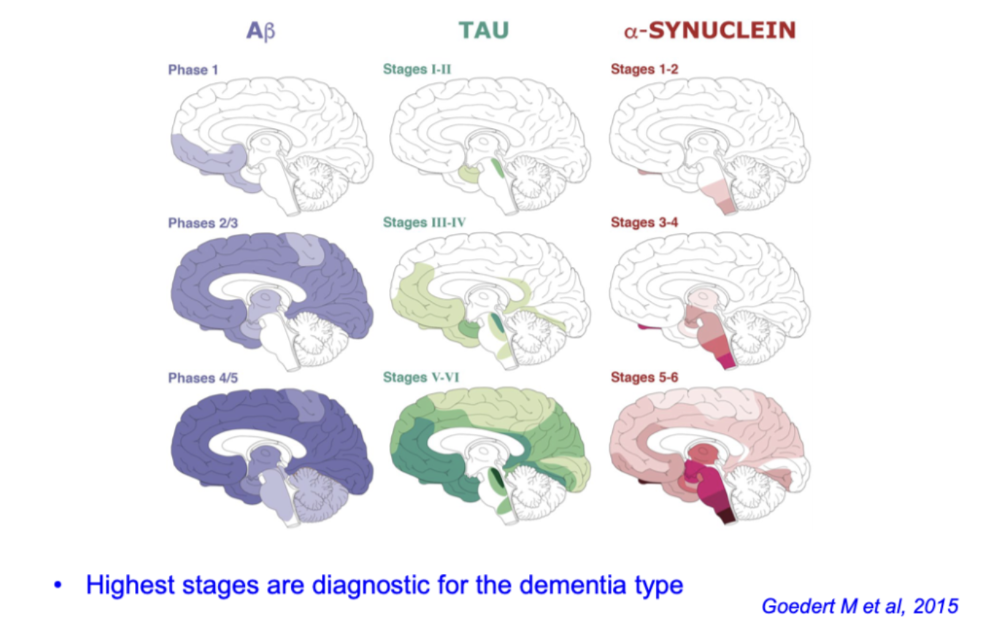
How do Aβ, tau, and α-synuclein spread in dementias?
Spread progressively in stages across the brain
Aβ: cortex early
Tau: limbic → cortex
α-synuclein: brainstem → cortex
Higher stage = more severe disease / diagnostic pattern
what is programmed cell death (PCD) and apoptosis- mechanisms of degeneration
PCD, a process where cell plays an active role in its own demise
Critical role in the development of NS and in its response to insult
Both anti-PCD and pro-PCD modulators play prominent roles, e.g. ischaemic (stroke) injury
Non-apoptotic forms of PCD e.g. autophagy
PCDs that do not fit the criteria for either apoptosis or autophagy – suggest other pathways?
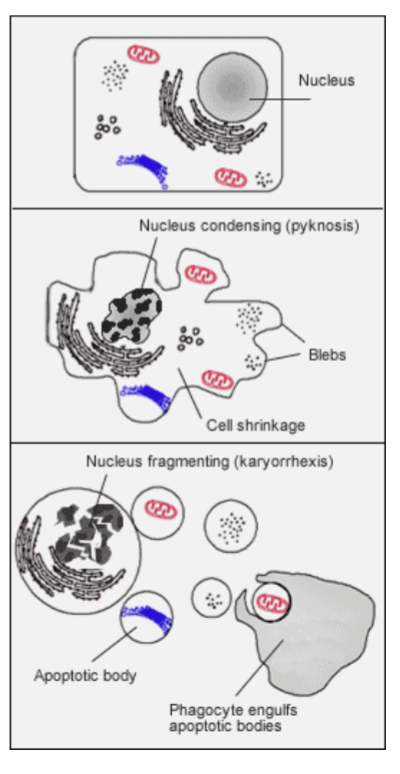
what is necrosis vs apoptosis- mechanisms of neurodegeneration
Apoptosis is distinguished from necrosis; mechanism that allows cells to self- destruct when stimulated by the appropriate trigger
Initiated if cell is no longer needed or becomes a threat to health
Aberrant inhibition or initiation of apoptosis contributes to many disease processes
Process of programmed cell death (PCD) has had broader recognition since 1972
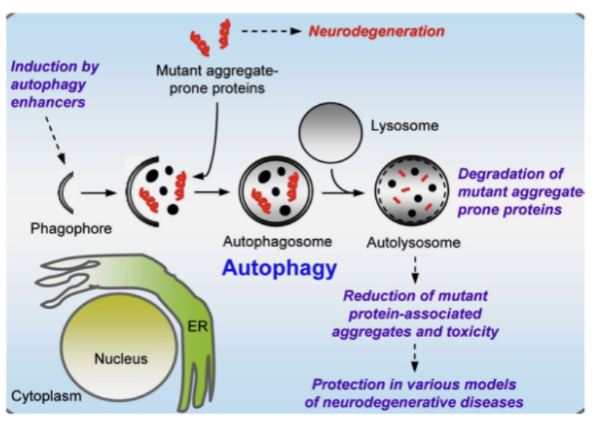
what is autophagy in neurodegeneration
Autophagy clears misfolded/aggregate-prone proteins
Process: phagophore → autophagosome → lysosome → degradation
Protective role:
Reduces toxic protein aggregates
Limits neuronal damage
Key idea:
Impaired autophagy → protein accumulation → neurodegeneration
what are the processes influencing neuron health
genetically determined disease process
ageing related decline
environmental risk factors/comorbidity
neuron stress and repair mechanisms
additional opportunities for interventions