Unit 4 PHRM 2022
1/54
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
55 Terms
Identify federal and provincial legislation and standards of practice relevant to the preparation of compounded sterile products.
Federal:Health Canada
• Policy on “Manufacturing and Compounding Drug Products in Canada”
• Outlines the factors that determine if a product falls under compounding or
manufacturing
Manufacturing:
▪ Preparation of product for sale to pharmacies for dispensing to their
patients
▪ Defined and governed by the Food and Drug Act and Regulations
▪ Mostly done by pharmaceutical companies
Compounding:
▪ Preparation of product for use by a specific patient based on a
prescription within an established pharmacist-patient-prescriber
relationship
▪ Governed provincially
▪ Mostly done by pharmacy personnel
ACCORDING TO NAPRA: In situations involving requests to compound preparations outside of a prescriber–patient–pharmacist relationship,
in the absence of a patient-specific prescription, the preparation activities fall under the federal legislative framework.
For example, the bulk preparation of compounded preparations in the absence of a prescriber–patient–pharmacist
relationship would fall under the federal legislative framework.
ACCORDING TO NAPRA: Health Canada is the federal department responsible for the Food and Drugs Act and the Controlled Drugs and Substances
Act and their associated regulations. In January 2009, Health Canada developed its “Policy on Manufacturing and
Compounding Drug Products in Canada”7
. At the time these Model Standards were prepared, Health Canada was
examining this policy with a view to creating new standards for situations not covered within the practice of pharmacy
or under the current federal licensing framework, such as commercial compounding manufacturing.
Provincial: NAPRA
Introduction: The new NAPRA Model Standards for Pharmacy Compounding of Non-hazardous Sterile Preparations have been
adapted from standards originally developed by the Ordre des pharmaciens du Quebec, which are in turn based on
General Chapter <797> of the United States Pharmacopeia – National Formulary (USP–NF) in effect in the United
States since 2004. Their preparation was led by the NAPRA ad hoc Committee on Pharmacy Compounding and involved
extensive consultation with experts and stakeholders.
Objective: To provide pharmacists and pharmacy techs who compound non hazardous sterile preparations with the standards necessary to evaluate their practice, develop service-related procedures and
implement appropriate quality controls for both patients and compounding personnel, with a view to guaranteeing the
overall quality and safety of sterile preparations. The Model Standards will come into effect in each province/territory
once they have been adopted by the respective provincial/territorial pharmacy regulatory authorities. THE MINIMUM requirements to be applied in compounding sterile preparations, but should aim to exceed these standards.
NAPRA’s professional competencies for Canadian pharmacists and pharmacy technicians at entry to practice provide
guidance for developing an ethical, legal and professional practice. One of these competencies specifies that a pharmacist
or pharmacy technician must seek guidance when uncertain about his or her own knowledge, skills, abilities or scope of
practice. Therefore, individuals who do not have the knowledge, training, expertise, facilities or equipment required to
compound sterile products must refer patients to a colleague who does have the competencies and facilities required to
do so or, where permitted by provincial/territorial legislation, ask another pharmacy to compound the product for them
• In 2016, the Alberta College of Pharmacy approved the Model Standards of Non-hazardous Sterile Preparations for the province. These standards are based on 797 standards.
Regulatory Framework:
Compounded sterile preparations are prepared by many health care professionals, including nurses, physicians,
pharmacists and pharmacy technicians. However, the majority of sterile compounding is performed by pharmacy
personnel under the supervision of pharmacists.
Pharmacy Compounding must always be carried out within a prescriber, patient, and pharmacist relationship.
Provincial/territorial pharmacy regulatory authorities are responsible for regulating a pharmacy’s compounding services
in these situations.
Pursuant to model standards, sterility is also required for the reconstitution and certain manipulations (according to manufactureres instructions) of sterile products approved by Health Canada and for repackaging of approved sterile products, regardless of the route of administration.
Compounded Sterile Preparations Include these medications:
• nasal inhalation solutions
• respiratory therapy solutions
• solutions for live organ and tissue or graft baths
• injections (e.g., intramuscular, intravenous, intrathecal, intradermal, subcutaneous)
• irrigation solutions for wounds and body cavities (e.g., thoracic, spinal, abdominal, pelvic)
• ophthalmic drops and ointments
• otic drops for intratympanic administration
• parenteral nutrition
• dialysis solutions
allergen extracts
• topical preparations (where sterility is essential to the therapy, e.g., for patients with burns)
• radiopharmaceuticals
USP <797>
• The United States Pharmacopeia (USP) is an official publication used by both
pharmacists and pharmacy technicians in their practices. It is the official
standard authority for all prescription and over-the-counter medications in
the United States.
• In 2004, USP Chapter 797 became official in the U.S., and has been used in
sterile compounding environments since, improving the concepts and
standards of compounded sterile preparations (CSP’s).
• USP 797 pertains to all personnel involved in preparation, storage, and
transportation of CSPs prior to administration.
CSHP – Canadian Society of Hospital Pharmacists
• CSHP Compounding: Guidelines for Pharmacies 2014
• Created a set of compounding guidelines for pharmacies to use as a
complement to any legislative provincial/federal practice requirements. The
guidelines cover sterile and non-sterile compounding, as well as
radiopharmaceuticals and hazardous preparations, in pharmacies where such
preparations are intended for human use, regardless of route of
administration.
ASHP – American Society of Health-System Pharmacists
• Strives to improve medication use and enhance patient safety
• Developed the “ASHP Guidelines on Compounding Sterile Preparations”
CETA (Controlled Environment Testing Association)
• Provides certification of secondary engineering controls. The controls include
equipment such as cleanrooms, laminar flow hoods, fume hoods, biological
safety cabinets, isolation rooms, and other controlled environments.
• More information, Appendix 5 in the NAPRA Model Standards outlines the
Minimum Indicators for Certification of Controlled Areas and Primary
Engineering Controls
Alberta College of Pharmacy (ACP)
• Activities are governed by the Health Professions Act
• Pharmacies must meet guidelines and standards that ensure quality and
safety of the pharmaceuticals they compound
• Standards of Practice for Pharmacists and Pharmacy Technicians
National Institute for Occupational Safety and Health (NIOSH)
• The NIOSH list can be used to determine whether a particular product is
hazardous
• Compiles and reviews drugs that can pose an occupational hazard to
healthcare workers
• The drugs outlined in NIOSH are organized into three tables, depending on the
potential handling risks
• Provides recommended standard precautions that should be taken when
handling hazardous drugs, such as engineering controls and personal
protective equipment (PPE)
USP <800>
• Describes practice and quality standards for handling hazardous drugs in
health care settings and help promote patient safety, worker safety, and
environmental protection
• Standards were written to protect all workers, patients, and the general
public who may be accessing facilities where hazardous drugs are prepared.
2. Identify potential sources of contamination in sterile compounding.
Touch Contamination: People (skin, exposure poor technique), products (exterior packaging, product itself), Faculty (walls, ceiling, floor, furniture)
Air Contamination: Viable and non viable contaminants found in air (facilities are designed to reduce contamination by 99.9% so if this is not working properly ((Laminar flow hood fails to work properly) CONTAMINATION occurs
Water Contamination: Sneezing, coughing
Shadowing: obstruction of airflow
Non-Viable Contaminants:
is a particle that does not contain a living
microorganism but acts as transportation for viable particles.
VIable Contaminants:
Viable
contaminants contain one or more living microorganisms. Bioburden is defined
as the number of bacteria living on a surface that has not been sterilized.
Factors that Affect Contamination Include:
Duration of Contact
Surface Texture: porous or rough textures are harder to clean and more likely to contain contaminiants than smoother surfaces
Surface Area : risk of contamination increases with larger surface area.
Examine infection control in institutions in terms of the following: a. Germ theory of disease (microorganisms and disease)
Originated with the french scientist Louis Pasteur and further studied by german physician Robert Koch
Theory: “Microorganisms (pathogens / germs) can lead to disease, expecially if they permitted to multiply without limitation and overwhelm the body’s immune system.
Contaminant: particulate matter or microbial orgamisun (Ex. bacteria (structural transformer), fungi, virus..,)
Microorgamisms normally reside in a particular body site are called resident / normal flora (microbiome).
Microorganisms that colonize a person for hours to weeks but do not stay permanently = transient flora.
Examine infection control in institutions in terms of the following: b. Asepsis and types of sterilization
Asepsis:
Sterilization: Process which renders substance, surface or area sterile by the elimination or destruction of microorganisms and their spores. The Types Include: Moist Heat, dry heat, radiation, mechanical, chemical.
Tyopes of Sterilization:
1. Moist Heat:
a. Tyndallisation: otherwise known as fractional sterilization, is the
repeated heating to boiling and application of steam over a number of
sessions.
b. Autoclaving: heating under pressure in a sealed chamber.
Page 13 of 140 NorQuest College – PHRM 2022: Learner Guide
2. Dry heat:
a. Directly by flame
b. Indirectly by convection, the circulation of heated air within a sealed
chamber, either:
i. Passively by gravity: heated air is less dense than cool air and thus
rises, or
ii. Actively by mechanical means: a fan or blower directs heated air
onto or into the materials, substances or surfaces being sterilized.
3. Radiation: The use of photons with either non-ionizing radiation (UV light)
or ionizing radiation (gamma rays or X-rays.)
4. Mechanical: Passage of a fluid through a screen-like material with small
pores that block microorganisms
a. 0.22-micron pore size removes bacteria
b. 0.01 microns removes viruses
5. Chemical: Few chemicals produce complete sterility, but may reduce
microbial numbers to safe levels
a. Liquid: Applying a reactive substance in a liquid state on to a surface,
area, or material. Examples include formaldehyde or hydrogen
peroxide. This is also referred to as cold sterilization.
b. Gas: Passing a reactive substance in a gaseous state on, through, or
over a surface, area, or material. Examples include ethylene oxide,
nitrogen dioxide, or ozone.
Differentiate between asepsis and sterilization.
Asepsis: State of absense of disease causing microorganisms. Antiseptics are agents that are used to kill miccroorganisms on living skin and mucous membranes. Germicidal agents are used to kill pathogenic microorganisms such as viruses, bacteria, spores, molds, and fungi. Sporicidal agents = kills spores.
Sterilization: is any process which renders a substance, surface, or area sterile by the elimination or destruction of microorganisms and their spores. Sterile refers to the state of absence of ANYYY microorganisms, not just the disease causing ones.
1. Describe the types of primary engineering controls (PECS) and how they work.: PECS
Primary Engineering Controls (PECS) highly specialized pieces of equipment of specialized rooms used for preparing sterile compounds.
PECs include laminar
airflow workbenches (LAFW) and compounding aseptic isolators (CAI). LAFWs
are also referred to as Laminar Airflow Hoods (LAFH).
Describe the types of primary engineering controls (PECS) and how they work.: CPECS:
For compounding of hazardous sterile preparations, a containment primary
engineering control (C-PEC), such as a biological safety cabinet (BSC) or
compounding aseptic containment isolator (CACI), must be used. They are
designed to protect personnel from any undesirable exposure to airborne
medicinal products during compounding and the transfer of hazardous
material during preparation.
Describe the types of primary engineering controls and how they work: Secondary Engineering Controls
controlled areas in which the
PECs are placed. In general, the engineering controls in sterile compounding
facilities are designed to reduce circulating airborne contamination. Primary
and secondary engineering controls work together to create a particle free
environment.
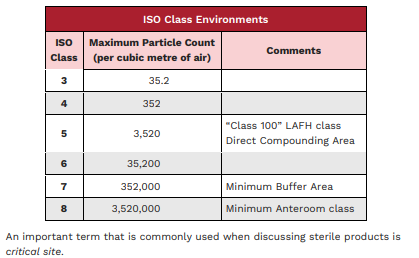
Describe the types of primary engineering controls and how they work: International Orgamization of Standards (ISO)
The International Organization of Standards (ISO) environmental class of
spaces within facilities is determined by the count of particles of a specific
size per cubic metre of air (see table below). A Primary Engineering Control
(PEC) is a device or room that provides an ISO Class 5 environment.
2. Explain the principles for working in a primary engineering control using aseptic technique.
Sterile compounding involves the use of aseptic technique. This technique
involves processes and physical preparation methods used by personnel who
prepare sterile compounds. It is meant to prevent the introduction of
pathogenic organisms or other contaminants into a sterile environment or
preparation. Sterile compounding can range from aseptic manipulation of
commercially available products to patient-specific ones or batching for
products which are not commercially available. Batching is making several,
sometimes dozens, of the same product in one sitting.
To ensure these aseptic practices are followed, sterile compounding personnel
must be orientated, trained, and evaluated consistently. These steps assist in
preventing medication errors, contamination of the final products, and allows
compounding personnel to achieve the highest standards of quality control.
ISO CLASSES
3. Examine infection control in institutions in terms of sterile compounding facilities including the anteroom and clean room.
1. Determine the conditions required for aseptic drug product preparation.
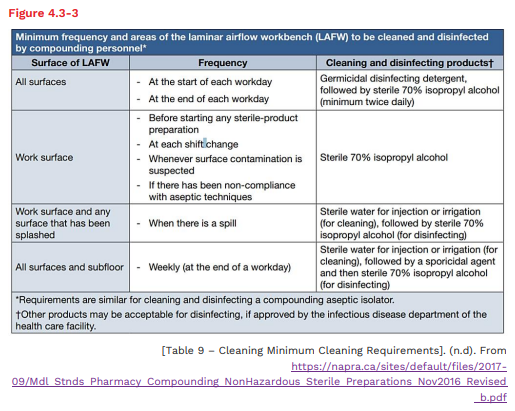
2. Describe the procedure and importance of routine cleaning of PECs.
The methods and procedures for cleaning the PEC
will vary depending on the policies in place at each institution. Refer to the
charts below for more information. Figure 4.3-3 outlines the minimum
frequency and areas to be cleaned and disinfected, as per NAPRA.
Cleaning a horizontal PEC: (overlapping motion for cleaning, top to bottome cleanest to dirtiest)
❑ The ceiling of the hood; wiping
back to front, working from side
to side
❑ The filter grate
❑ The horizontal bar and hooks,
if applicable
❑ The first side panel from back
to front working from top to
bottom
❑ The second side panel from
back to front working from top
to bottom
❑ The work surface wiping back
to front, working from side to
side
❑ Ensure you wipe the front
edges of each section as well
Cleaning a Vertical PEC:
❑ Push up the view screen, if applicable
❑ The filter grate
❑ The back panel; wiping top to bottom,
working from side to side
❑ The horizontal bar and hooks, if applicable
❑ The first side panel from back to front
working from top to bottom
❑ The second side panel from back to front
working from top to bottom
❑ The work surface wiping back to front,
working from side to side
❑ If applicable, lower the glass front panel
and wipe the inside of the glass in one
sweeping motion from top to bottom. Then
wipe the outside of the glass
❑ Ensure you wipe the front edges of each
section as well
sweeping motion includes: Examples include
Cleaning of side panels starts at the
interior upper back corner (x) close to
the HEPA filter. It proceeds in
overlapping motions that move towards
the outer edge of a horizontal PEC
Figure 4.3-5
Cleaning of the work surface starts at
the interior back corner (x) close to the
HEPA filter. It proceeds in overlapping
motions that move towards the outer
edge of a horizontal PEC
3. Explain the purpose of hand hygiene and protective equipment in sterile
product preparation.
4. Describe the procedure for applying and removing protective apparel:
a. Hair covers
b. Masks
c. Shoe covers
d. Gowns
e. Gloves
f. Goggles
5. Examine infection control in institutions in terms of the following:
a. Hand hygiene
b. Protective equipment/apparel
1. Identify the documentation requirements related to sterile products
preparation.
2. Determine information to be included on the label for a sterile product.
3. Explain the storage requirements for sterile products.
4. Apply your knowledge of drug stability, instability, and incompatibility to sterile products.
5. Navigate resources to compile stability and sterility data.
6. Identify the information found in a parenteral drug manual
1. Identify and describe supplies required for the compounding of sterile
products for each of the following:
a. Needles
b. Syringes
c. IV bags
d. Venting devices
e. Filters
2. Differentiate among small-volume parenteral (SVP), IV piggyback, and
large-volume parenteral (LVP) preparations.
3. Describe the different types of intravenous solutions and their uses.
4. Describe the proper arrangement of supplies in the different types of
Primary Engineering Controls.
5. Explain the various techniques required to manipulate the following
products:
a. Vials
b. Vials requiring reconstitution
c. Ampoules
d. IV bags
6. Describe the steps involved in finishing a sterile product.
7. Explain how waste generated in the production of sterile products is safely handled and discarded in the pharmacy.
1. Describe and explain the significance of the following in relation to
parenteral products:
a. Osmolality
b. Osmolarity
c. pH
d. Tonicity
2. Describe total parenteral nutrition (TPN) and apply your knowledge of
pharmaceutical calculation to its preparation.
. Identify the conditions for which TPN is used.
4. Explain the advantages and disadvantages of TPN.
5. Identify the different components/ingredients of TPN preparations.
6. Describe the steps involved in preparing TPN product.
7. Explain the safety considerations to be followed in the preparation and
administration of TPN.
8. Differentiate between central administration and peripheral intravenous
administration of TPN.
1. Identify and describe routes of parenteral drug administration.
2. Describe the characteristics of intravenous (IV) products.
3. Describe intravenous infusion devices and methods.
4. Calculate the concentration of IV infusions and rates of infusion
1. Describe quality management to ensure the accurate compounding and integrity of a sterile product
1. Identify and describe supplies required for the compounding of sterile
products for each of the following:
a. Needles
b. Syringes
c. IV bags
d. Venting devices
e. Filters
syringes can be used 5 times, but only for the same drug. ?, make sure that
2. Differentiate among small-volume parenteral (SVP), IV piggyback, and
large-volume parenteral (LVP) preparations.
3. Describe the different types of intravenous solutions and their uses.
4. Describe the proper arrangement of supplies in the different types of
Primary Engineering Controls.
5. Explain the various techniques required to manipulate the following
products:
a. Vials
b. Vials requiring reconstitution
c. Ampoules
d. IV bags
6. Describe the steps involved in finishing a sterile product.
Explain how waste generated in the production of sterile products is safely handled and discarded in the pharmacy.