TB, Sarcoidosis, and Lung Cancer
1/121
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
122 Terms
What is tuberculosis?
- chronic infectious disease caused by mycobacterium tuberculosis
- consumption or wasting
What diseases are associated with an increased risk for developing TB?
- HIV/immunosuppression
- DM
- contact with an infected person
- Cancer
What are risk factors for developing TB?
- immigrants
- dense populations
- health care workers
- IV drug users
What medication is associated with an increased risk for developing TB?
TNF-a-inhibitors
What are the two stages of the pathophysiology of TB?
1. primary infection
2. secondary
What are the primary stage of TB?
- active: non-contained bacteria replicate and cause contagious symptoms (cavitary lesions)
- latent: macrophage contained bacteria that does not replicate and no contagious symptoms (caseated GHON LESIONS)
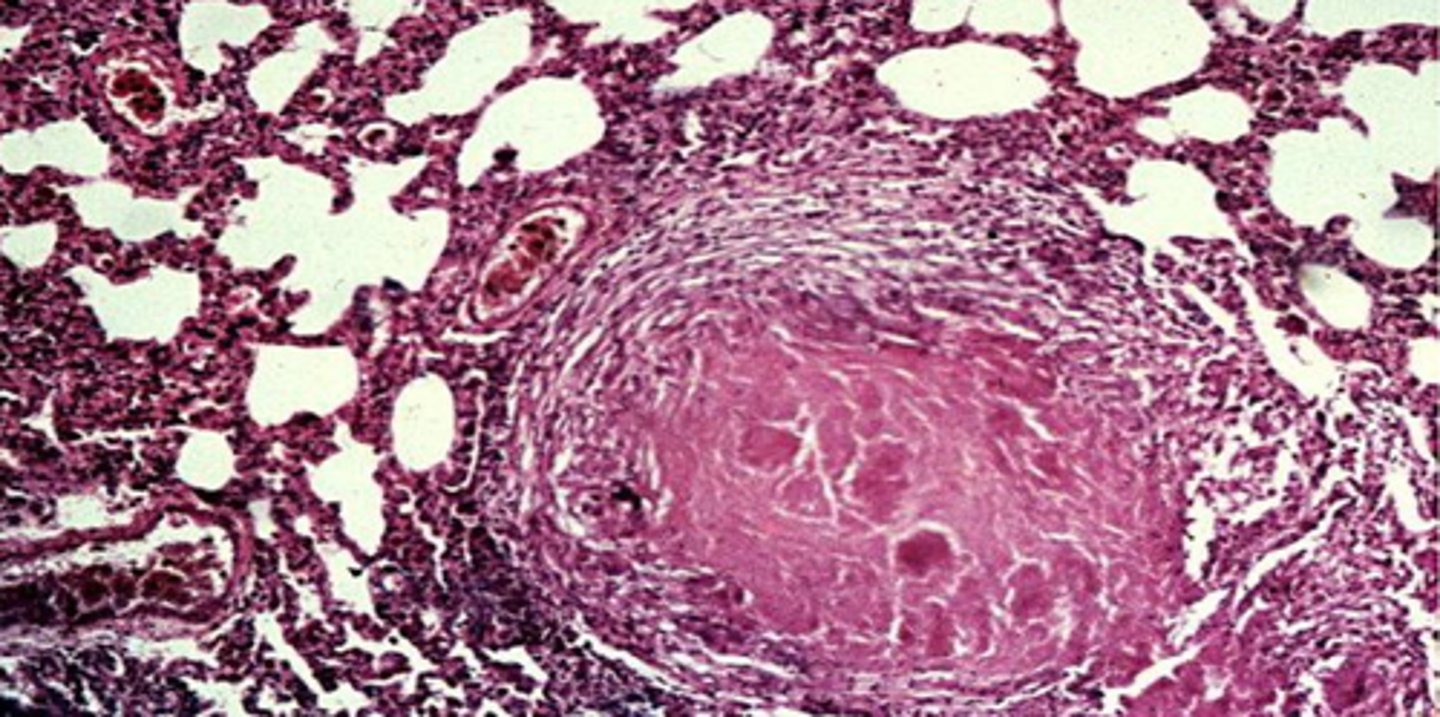
What is a caseating granuloma?
It is a cheese-like necrosis, typically a feature of a granuloma of TB seen in latent infections
(ghon lesion with soft tissue)
Describe the secondary stage of TB?
- reactivation of latent TB when macrophages release dormant mycobacterium
- patient is contagious
What is extrapulmonary TB (miliary/disseminated TB)?
hematologic spread of TB from initial pulmonary infection to another organ
What is extrapulmonary TB of the spine?
Pott's Disease
What is extrapulmonary TB of the lymphatic system?
Scrofula
What is scrofula and how does it present?
- extrapulmonary TB disease in children
- presents with cervical lymphadenitis

What is the TB symptom triad?
1. fever
2. chronic cough
3. night sweats
What is seen on PE of latent TB?
normal
What is seen on PE of active TB?
- wasting appearance
- fever
- apical post-tussive rales
- distant breath sounds
What is the gold standard/best test for diagnosis for TB?
- Culture and Sensitivity
- deep lung cough sputum sample in early morning to assess an acid-fast bacillus
What are other diagnostics for TB?
- PCR/NAAT (identifies specific DNA)
- AFB smear
What is screening methods for TB?
- PPD (skin test)
- QuantiFERON-TB
In what situations would a >/5 mm PPD warrant a (+) PPD?
- HIV (+)
- close contacts
- abnormal CXR
In what situations would a >/10 mm PPD warrant a (+) PPD?
- recent immigration
- group living (nursing home patient or prisoner)
- medical worker
- high-risk population
In what situations would a >/15 mm PPD warrant a (+) PPD?
all other patients
What vaccine could cause a false (+) with PPD?
BCG vaccine
What could cause false (-) with PPD?
- incorrect PPD placement
- immunocompromised
- chronic illness/infection pt
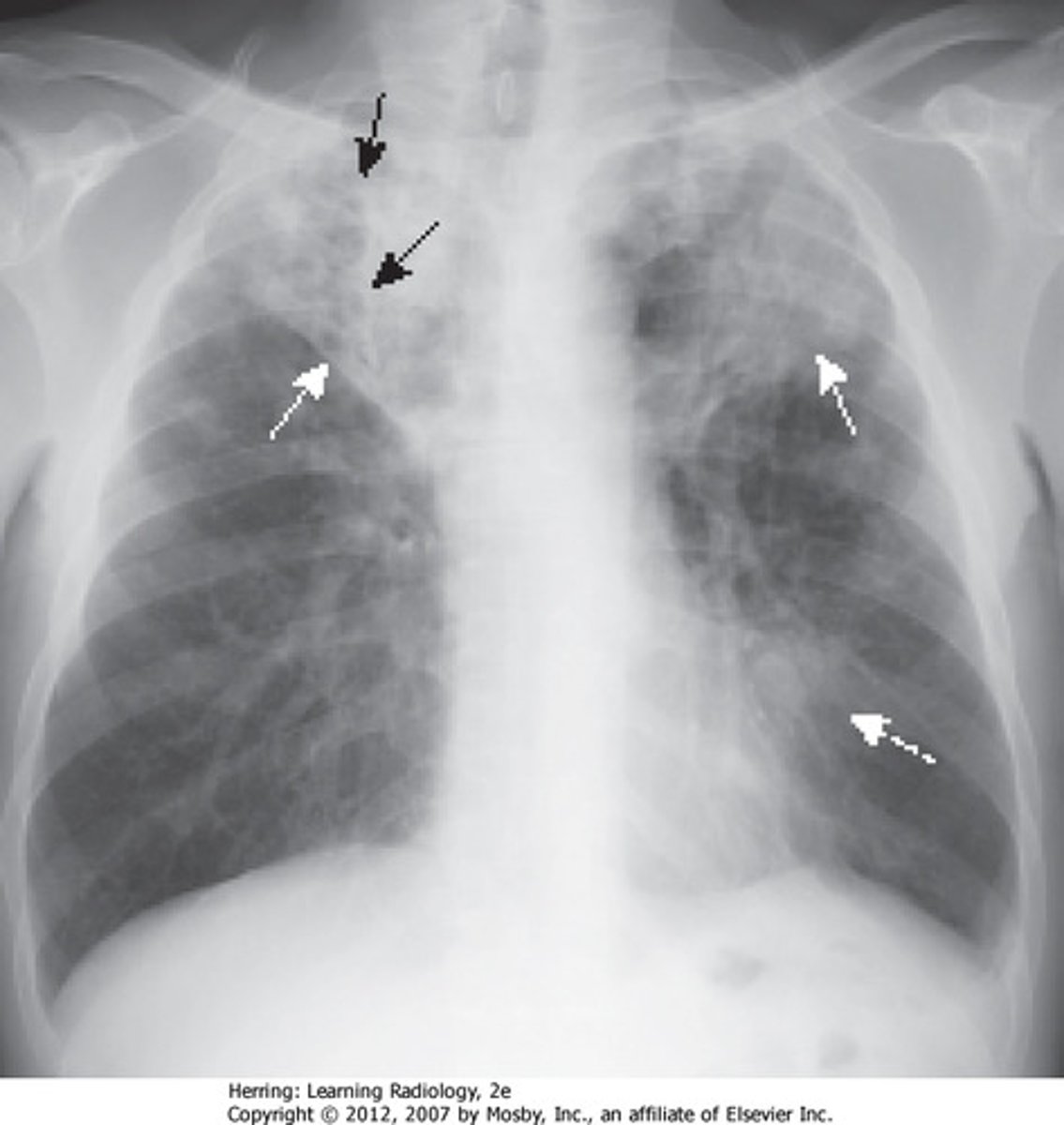
What is seen of CXR with TB?
- unilateral apical infiltrates
- caseating granulomas
- cavitations
- Ghon complexes
- pleural effusion
When is it appropriate to test for TB?
- active symptoms of TB
- immunocompromised
- medications (TNF-a)
- contact of infected individuals
- immigrants
- nursing home patients, hospitalized patients, or prisoners
- health care workers
Is TB a reportable disease?
Yes, it is mandatory
TB (+) patients no longer need isolated when?
sputum spears are (-) x 3
What is the treatment regimen for latent TB?
Isoniazid + Rifapentine (weekly) x 3 months
What is the treatment regimen for active TB (adults and children 12+)?
- Rifapentine + Isonizide + Moxifloxacin + Pyrazinamide (daily) x 8 weeks (RIMP)
- Rifapentine + Isonizide + Moxifloxacin (daily) x 9 weeks
What is the treatment regimen for active TB (<12)?
- rifampin + isoniazid + pyrazinamide + ethambutol x 2 months
- rifampin + isoniazid x 4 months
What is the treatment regimen for active TB in pregnant patients?
- Rifampin + Isonizide + Ethambutol (daily) x 2 months
- Isonizide + Rifampin x 7 months
What are the treatment complications for Rifampin/Rifapentine?
- Thrombocytopenia
- Red/orange discoloration of body fluids
- Hepatotoxicity
What are the treatment complications for Isoniazid?
- hepatotoxicity
- neuropathy
What are the treatment complications for pyrazinamid?
- hepatotoxicity
- hyperuricemia
What are the treatment complications for ethambutol?
Optic neuritis
What are the treatment complications for streptomycin?
- Ototoxicity
- Nephrotoxicity
Which drug should be used for HIV (+) patients and pregnancy in TB (makes it different than standard tx)?
rifapentine
What is the treatment regimen of extrapulmonary TB?
- same treatment of TB of the lungs, but should be at least 9+ months
- +/- corticosteroids for pericarditis and meningitis
- +/- surgical debridement/draining of affected tissues
How is the prognosis for untreated and treated TB?
- untreated = fatal in 50-60% in 5 years
- treated = excellent
What is multi-drug resistant TB, and what is treatment?
- resistant to Isoniazid and Rifampin
- need a susceptible three-drug regimen until negative culture THEN 2 drug regimen x 12 months
What is patient education with TB?
- isolate
- hygiene
- diet counseling
- HIV screening
How is atypical mycobacterium transmitted?
environmental (water, soil, dust and farms)
What is the mycobacterium avium complex (MAC)?
- M. avium and M. intracellulare
- chronic slow progressive respiratory disease
What is the diagnosis for MAC?
- AFB smear/culture
- PCR
- CXR
What is the treatment for MAC?
macrolide (clarithromycin or azithromycin) PLUS rifampin and ethambutol x 12-18 months after negative culture
What is non-tuberculosis mycobacterium transmission and presentation (NTM)?
- usually from freshwater sources
- can cause skin infection with nodules and ulcerations
What are the types of NTM?
- M. marinum: salt and fresh water
- M. fortuitum: pedicure bath water
- M. abscessus/M. fortuitum: surgical procedures
What is the diagnosis of NTM?
- tissue biopsy
- AFB smear/culture
- PCR/NAAT
What is the treatment of NTM?
macrolide + rifampin + ethambutol for 4-6 weeks after resolution of skin lesions
What is sarcoidosis, and what is it characterized by?
- a chronic multisystem inflammatory disorder
- accumulation of noncaseating granulomas in multiple organs
What is seen on CXR with sarcoidosis?
non-caseating granulomas in multiple organs
What is the location of 90% of granulomas with sarcoidosis?
- lungs
- lymph nodes in hilar regions
What is the etiology of sarcoidosis?
unknown
What is the pathophysiology of sarcoidosis?
-T and B cell hyper-reactivity = excess immune reaction = inflammation
- TNF elevation causes inflammation
- granuloma secrete ACE and 1-25D
What are the top organ systems affected by sarcoidosis?
- lungs
- lymphatics
- skin
What are the symptoms of sarcoidosis?
- cough
- dyspnea
- chest pain
- hemoptysis
- myalgias/arthralgia
What are the PE findings of sarcoidosis?
- pulmonary HTN
- lupus pernio and erythema nodosum
- hilar LAD
What is lupus pernio?
- violaceous, raised discoloration of nose/ear/cheek/chin
- resembles frostbite
- pathognomonic for sarcoidosis

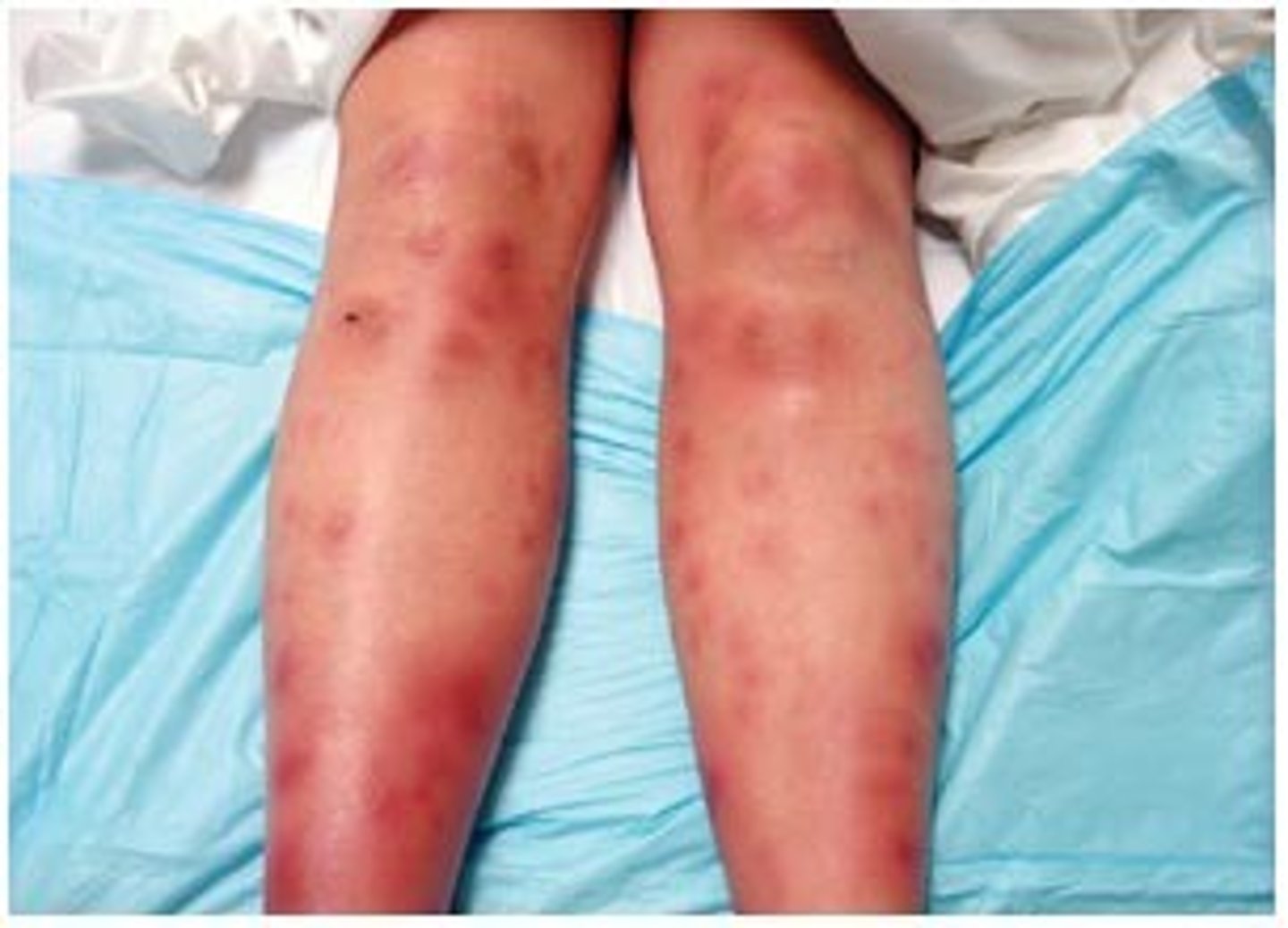
What is erythema nodosum?
- tender red nodules that are usually found on the shins
- associated with sarcoidosis
What are complications fo sarcoidosis?
- Nephritis/renal failure
- cranial or peripheral nerve palsy
- CHF, arrhythmias/heart block, cardiomyopathy
- granuloma formation
- Lofgren's syndrome
Why does nephritis occur with sarcoidosis?
hypercalcemia associated with sarcoidosis (granuloma secrete Vit D = more Ca2+ absorption)
What CN palsy occurs with sarcoidosis?
Bell's palsy
What cardiac issues occurs with sarcoidosis?
-CHF, arrythmia, cardiomyopathy
What bone issues occur with sarcoidosis?
granuloma formation
What is Lofgren's syndrome triad?
- erythema nodosum
- bilateral hilar LAD
- polyarthralgia + fever
What is the best initial assessment for sarcoidosis?
CXR
What is seen on CXR with sarcoidosis, and what is stage I/ IV?
- I: hilar lymphadenopathy
- IV: overt pulmonary fibrosis

What is best for getting a true diagnosis and histology (identifying non-caseating granulomas) with sarcoidosis?
bronchoscopy with biopsy
What is seen on CT with sarcoidosis?
cluster of black pearl signs

What is ratio of CD4/CD8 on bronchoalveolar lavage for sarcoidosis?
> 3.5
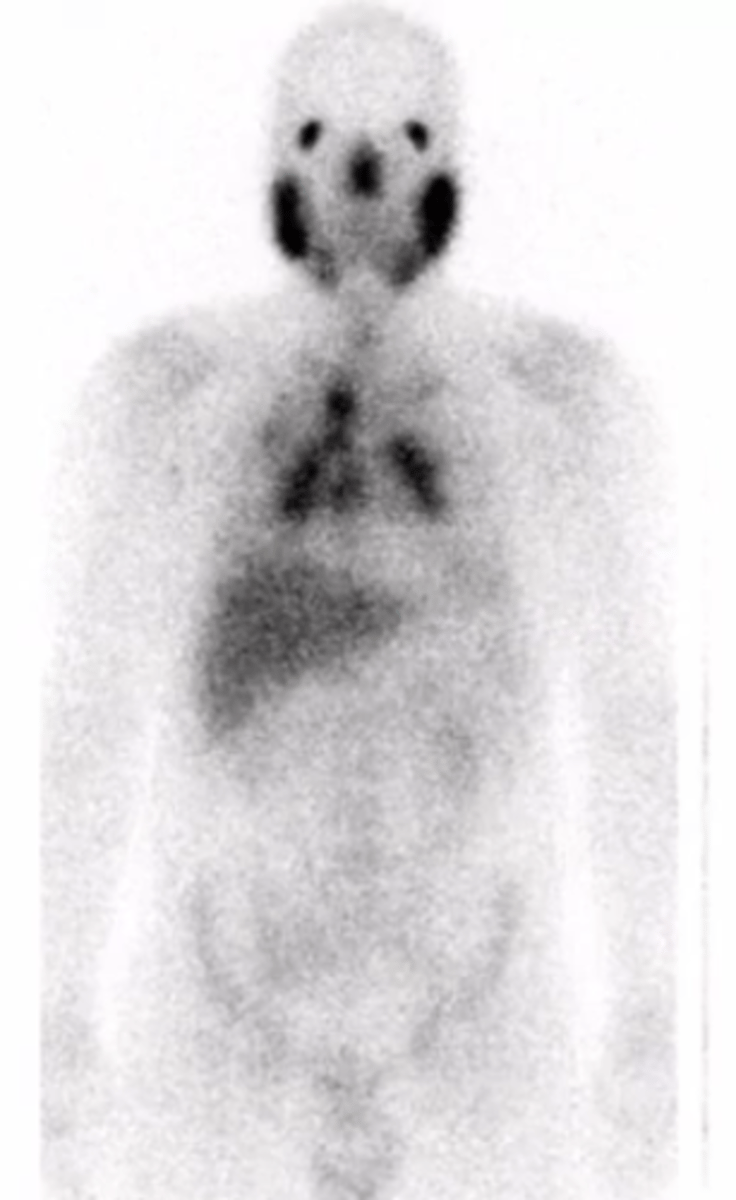
What does a PET scan show with sarcoidosis?
gallium uptake of the parotids or other regions for involvement
What is the "panda sign" in sarcoidosis?
uptake in the parotids
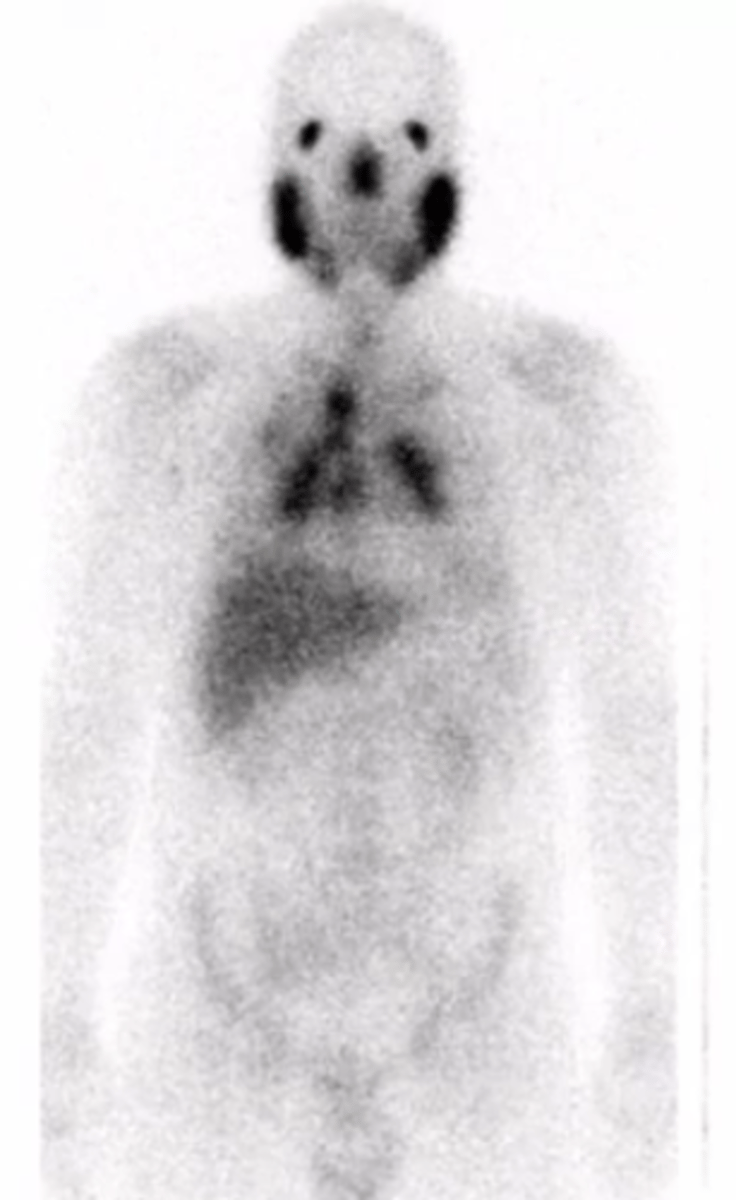
What is the "lambda sign" in sarcoidosis?
uptake in the chest
What is seen in labs with sarcoidosis?
- LFT: high alk phos
- CBC: leukopenia
- Serum/urine calcium: high
- ACE levels: high
- ESR: elevated
What is the mainstay of therapy for sarcoidosis?
oral corticosteroids
What are the second line agents for sarcoidosis?
methotrexate, hydroxychloroquine, or azathioprine
What are other options for sarcoidosis?
- monoclonal ABs (mab's)
- TNF-a- blockers
What may be indicated in severe cases of sarcoidosis?
lung transplant
What is the #1 risk factor for lung cancer?
tobacco use (smoking)
What are 4 other RFs for the development of lung cancer?
- age
- scarring disease (COPD)
- environmental exposure
- genetics
What is the pathophysiology of lung cancer?
- Activation of dominant oncogenes
- Inactivation of tumor-suppressor genes
What are the 2 classifications of lung cancer?
1. small-cell (SCLC)
2. Non-small cell lung cancer (NSCLC)
What are the 3 types of NSCLC?
1. Adenocarcinoma
2. Squamous cell carcinoma
3. Large cell carcinoma
What is small-cell lung cancer?
- 98% of the time related to a smoking history
- 13% of all lung malignancy
What is the pathophysiology of SCLC, and does it present as central or peripheral?
- neuroendocrine tumor
- arises central peribronchial location
- rapid growth and metastasis
- high association with paraneoplastic syndromes
What is adenocarcinoma lung cancer?
- most common type of all lung malignancies
- seen more in non-smokers, women, and young adults
What is the pathophysiology of adenocarcinoma lung cancer, and does it present as central or peripheral?
- usually presents as a peripheral tumor
- somewhat rapid growth
What is adenocarcinoma in situ?
- spreads along alveolar structures without invasion
- less chance of mets --> pretty good and curable
What is squamous cell lung carcinoma?
- second most common subtype with hemoptysis for presentation
- strong associated with smoking
What is the pathophysiology of squamous cell lung cancer, and does it present as central or peripheral?
- central tumor with cavitary lesions
- tends to grow slowly
- highly associated with hypercalcemia/pancoast syndrome
What is large cell carcinoma?
rarer form of cancer (2-5%)
What is the pathophysiology of large cell carcinoma, and does it present as central or peripheral?
- peripheral tumors
- rapid growth/aggressive
What are the symptoms of central lung tumors?
- cough
- hemoptysis
- wheezing
- Dysnpnea
- chest pain
- weight loss
What are the symptoms of a peripheral lung tumor?
- voice changes
- pain in vertebra/ribs
- atelectasis
- PE
- neurologic sx
- weight loss
What 4 places can lung cancer metastasize to?
- bone
- liver
- adrenal
- brain
What is Pancoast syndrome?
tumor at apex that infiltrates the branchial plexus causing arm pain, numbness and weakness
What is Horner Syndrome?
tumor of the eye's sympathetic nerve supply causing ptosis, mitosis and anhidrosis
What is SVC syndrome, and is it more associated with NSCLC or SCLC?
- blockage of SVC from tumor causing R sided facial, neck and arm swelling
- NSCLC
What are paraneoplastic symptoms?
- hormone substances secreted by tumors causing endocrine disturbance
- examples: hypoglycemia, SIADH, hypercalcemia, hypertrophic pulmonary osteoarthritis, cushing syndrome, or lambert-eaton myasthenic syndrome
What is Lambert-Eaton Myasthenia Syndrome?
- impaired Ach release at NMJ
- causes ocular and proximal muscle weakness and decreased DTRs