Families final review
1/82
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
83 Terms
Role of the placenta
organ that transports oxygen and nutrients to the fetus from the mother while removing waste from the fetus as well.
Risk factors for an abnormal placenta
high blood pressure
maternal age >40
premature rupture of membranes (PROM)
blood clotting disorders
a twin or multiple pregnancies
previous uterine surgery or previous placental complications
substance use, including tobacco and drugs, especially cocaine use
abdominal trauma such as a fall or motor vehicle accident
what is placenta previa
when the placenta extends too low in the uterus covering some or all of the vaginal opening.
Risk factors for placenta previa
previous placenta previa
previous cesarean section
multiple pregnancies
smoking
cocaine use
prior dilation and curettage
assisted reproductive technology
how is placenta previa diagnosed
ultrasound
what precautions do we want to take in a patient with placental previa
-Never perform a vaginal exam
-no heavy lifting
-no intercourse
Why does placenta previa increase the risk of hemorrhage?
Because the placenta sits over the cervix, any dilation or contractions can tear placental vessels, causing antepartum or postpartum hemorrhage.
Is actively bleeding placenta previa an emergency?
Yes — it is an obstetric emergency requiring stabilization, monitoring, and possible blood transfusion.
Does the first episode of bleeding always require immediate delivery?
No — if the woman stabilizes, she may not need to deliver immediately.
What is the recommended mode of delivery for uncomplicated placenta previa?
c-section
Maternal risks associated with placenta previa?
Postpartum hemorrhage
Blood transfusion
Hysterectomy
ICU care after delivery
Fetal risks associated with placenta previa?
Preterm birth
Low birth weight
Low APGAR scores
Respiratory distress syndrome
what is placental abruption
is complete or partial detachment of the placenta after 20 weeks gestation but before delivery of the fetus.
The. main findings of placental abruption are
-bleeding
-abdominal pain
-hypertonic uterine contractions
-uterine tenderness
-abnormal fetal heart tracing
The risk factors for a placental abruption
· Previous abruption not caused by trauma
· Hypertension
· Cocaine use during pregnancy
· Smoking
· Polyhydramnios
· Multiple gestation pregnancy
· Preeclampsia
· Sudden uterine decompression
· Age > 35
· Trauma (ex. abdominal trauma)
What is the major maternal risk of placental abruption?
Maternal hemorrhage, which can progress to DIC, shock, and maternal death.
What fetal complications are associated with placental abruption?
Preterm delivery
Fetal growth restriction
Low birth weight
Hypoxemia & asphyxia
What fetal heart rate pattern suggests uteroplacental insufficiency in abruption?
Absent variability
Category III tracing
(Category I is normal; anything abnormal must be reported and intervened on.)
priority actions for placenta previa
• Notify provider
• Ultrasound (possible placenta previa)
• O2 (uteroplacental insufficiency)
• Prepare for blood transfusion
• Blood type & screen
• Large-gauge IV
Why give oxygen to a placental previa patient?
To improve uteroplacental oxygenation during fetal distress or insufficiency.
Why prepare for a blood transfusion?
both abruption and previa can cause severe maternal hemorrhage.
what are all of the nursing actions for a placental previa patient
Continuous monitoring (EFM)
• Ultrasound (omit vaginal exam)
• IV
• Left lateral positioning
• O2
• Prepare for blood transfusion
• Prepare for emergency c-section (OR, NPO)
• Give RhoGAM if needed
• If pre-term labor, give Terbutaline and Betamethasone (promote lung
development of baby)
• Narcan on standby
what are clinical findings most concerning for a patient with gestational diabetes
-maternal age (over 35)
-history of large birthweight babies
-BMI (above 30)
Which clinical findings put a 26‑week pregnant client at risk for gestational diabetes?
(Select all that apply)
Options:
• Fetal heart rate
• Multigravida status
• Pre‑pregnancy BMI
• Level of physical activity based on occupation
• Weight gain 2 lbs since last visit
• Previous children >9 lb (4 kg)
• Maternal age
pre pregnancy BMI
level of physical activity based on occupation
previous children birthweight more than 9lb
maternal age
what is the highest priority care for. a client with gestational diabetes
stabilizing blood glucose levels
what is the strongest evidence that the client may have gestational diabetes that requires further testing
1 hr glucose tolerance test
The client takes the 3 hour glucose tolerance test and receives the diagnosis of gestational diabetes. The nurse begins to develop the plan of care.
What additional assessment data should the nurse obtain?
Ø Select All that Apply
¨ Access to transportation
¨ 24 hour diet recall
¨ Assessment of salt intake
¨ Economic ability to purchase healthy food
¨ Access to supermarkets
¨ Location of kitchen in residence
¨ Assess intake of foods containing vitamin K
¨ Physical activity patterns
24‑hour diet recall
✔ Economic ability to purchase healthy food
✔ Access to supermarkets
✔ Physical activity patterns
The nurse implements a dietary plan to manage the client’s diabetes during pregnancy.
¨ Encourage use of low fiber food
¨ Identify carbohydrates with low glycemic index
¨ Client should increase fat based foods while pregnant
¨ Recommend consultation with a registered dietician
¨ Should consume 2 large meals and 3 small snacks/day
¨ Should consume 3 small – moderate meals and 4 snacks/day
¨ Discuss the importance of consuming high sodium diet
weight gain allowance for each BMI
how do we measure appropriate fundal height after 20 weeks
fundal height should be within 2cm plus or minus of the gestational age
what should the fundal height be after delivery
It should be at the level of umbilicus or 1cm above
1615. 27yo Gravida 2 now Para 2 delivered 3590 gram (7lb 9oz) term infant via cesarean at 1545.
Quantitative blood loss 850 mL. Client stable in PACU with oxytocin 30units/500mL LR IV @ 250mL/hr.
1645. Client states, “I feel dizzy” and appears pale. Additional blood loss 400 mL.
Fundus boggy, midline, and 3cm above umbilicus.
The client in the 4th stage of labor is most likely experiencing:
• Septic shock
• Cardiogenic shock
• Hemorrhagic shock
as most evidenced by:
• Total blood loss
• Blood pressure
• Pulse
hemorrhagic shock, total blood loss
what is the nursing actions for hemorrhage
-massage fundus
-weigh peri pads
-oxegen at 10L
laboratory values to look after in a hemorrhage patient
hgb and hit
what are the medications for a patient is hemorrhage
IV blood transfusion
Misoprostol
Ø Which 4 orders should the nurse implement first, for a hemorrhage patient? Highlight selection
¨ Hemoglobin and hematocrit |
¨ Massage fundus |
¨ Administer misoprostol |
¨ Weigh pads |
¨ Oxygen 10 L/min |
¨ Type and cross ¨ 500 mL normal saline fluid bolus |
¨ Notify surgical team |
-massage the fundus
-administer misoprostol
oxygen 10L/min
500 ml normal saline fluid bolus
0900. 4g loading dose magnesium sulfate IV started, to be run over 20 minutes. Second nurse verified pump settings. Client educated on medication side effects. Client complains of headache rated 7/10, no nausea/vomiting, no epigastric pain, no visual disturbances. Current BP 159/89. Fetal monitor shows baseline heart rate 130 bpm, moderate variability, accelerations present, decelerations absent.
0920. Magnesium sulfate loading dose complete. Magnesium rate changed to 2g/hr continuous infusions. Second nurse verified pump settings.
1100. Client noted to have cutaneous flushing and sweating. Fan brought to bedside.
1200.Absent patellar reflex,RR 11,withcomplaints of shortness of breath. Pulse oximeter 92% on RA
Which findings in a preeclamptic client on magnesium sulfate are most significant?
✔ Absent reflexes
✔ RR 11/min
✔ Urine output 20 mL/hr
✔ Shortness of breath
These indicate magnesium toxicity (CNS depression + respiratory depression + decreased renal clearance).
primary focus of giving magnesium
prevents seizures by depressing the central nervous system
what is a side effect of magnesium effecting the vital signs
lowers blood pressure
Assessment findings for magnesium sulfate toxicity
less urine output
lethargic
respiratory depression
0900. 4g loading dose magnesium sulfate IV started, to be run over 20 minutes. Second nurse verified pump settings. Client educated on medication side effects. Client complains of headache rated 7/10, no nausea/vomiting, no epigastric pain, no visual disturbances. Current BP 159/89. Fetal monitor shows baseline heart rate 130 bpm, moderate variability, accelerations present, decelerations absent. 0920. Magnesium sulfate loading dose complete. Magnesium rate changed to 2g/hr continuous infusions. Second nurse verified pump settings. 1100. Client noted to have cutaneous flushing and sweating. Fan brought to bedside. 1200. Absent patellar reflex, RR 11, with complaints of shortness of breath. Pulse oximeter 92% on RA. What additional assessments should the nurse obtain STA ¨ Fetal status ¨ Breath sounds ¨ Pupils ¨ Level of consciousness ¨ Sensation ¨ Capillary refill
|
fetal status
breath sounds
level of consciousness
Action |
Stop magnesium infusion |
Administer calcium gluconate |
Place client in supine position |
Activate rapid response |
Provide oxygen |
Monitor fetus |
Administer anti-seizure medication |
Draw serum magnesium level |
Check for medication error |
Elevate extremities STA the actions that are indicated for a patient with magnesium deficiency |
stop the magnesium infusion
administer calcium gluconate
activate rapid response
provide oxygen
monitor fetus
draw magesium level
check for medication error
Which 3 actions should the nurse take FIRST for magnesium toxicity? Options: stop mag, monitor fetus, check med error, oxygen, calcium gluconate, draw mag level, rapid response
✔ Stop magnesium infusion
✔ Provide oxygen
✔ Administer calcium gluconate
if the magnesium toxicity is unchanged then
request an additional dose of calcium gluconate
For magnesium toxicity what 2 parameters should the nurse monitor and what actions should be taken.
monitor respiratory status and deep tendon reflexes
stop the infusion and administer calcium gluconate.
how to evaluate for compartment syndrome
-assess 6 p’s: pain, pallor, pressure, pulselessness, paresthesia, pain with passive stretch
-see if pain is unrelieved by medication
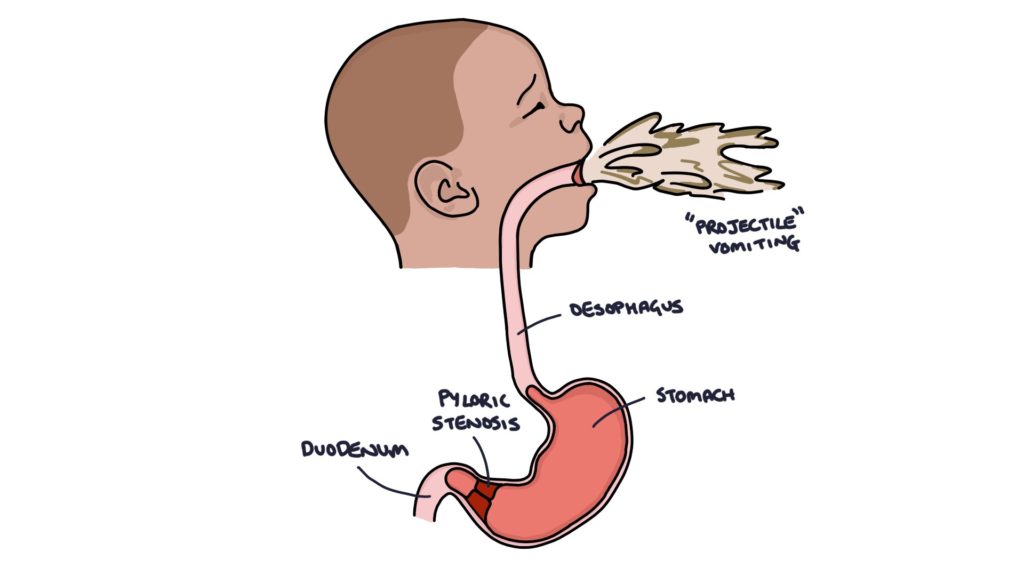
Manifestations of pyloric stenosis
-projectile vomiting
-olive shaped mass

manifestations of intersusseption
-sausage shaped abdominal mass
-sudden episodic abdominal pain
-bilious emesis
-red “current” stools
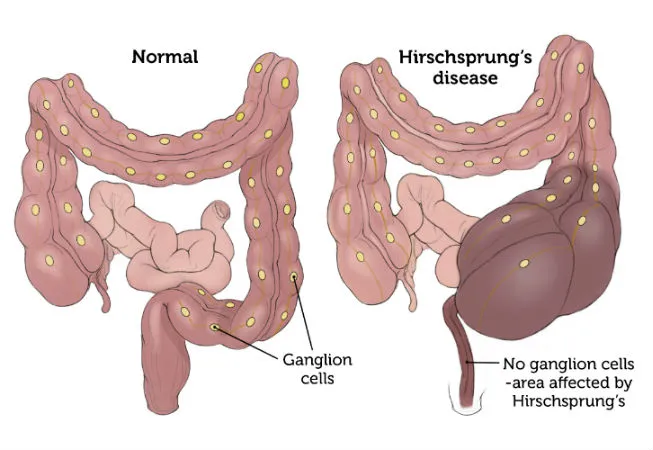
Manifestations of Hirschsprung’s disease
-ribbon like stools
-failure to pass meconium in 48 hours
A nurse is preparing to care for a child with watery diarrhea, what are the nursing actions
-oral rehydration therapy
How do we position a patient with epistaxis
sit up and lean forward
Diagnostic for sickle cell anemia
hemoglobin electrophoresis
Suspected findings for rheumatic fever
Discrete pink-red maculopapular rash on face, then trunk, then
extremities
fever
joint pain
for a patient with cystic fibrosis we give pancreatic enzymes with
snacks
Acute exacerbation of asthma
expiratory wheeze, chest tightness, and cough
we use quick relief inhalers like albuterol
Impetigo
-can be caused by staph or strep
-ages 2-5 years old
-spread through direct contact
-honey crusted lesions
-nurisng interventions: oil, antibiotics, and infection control
why would a newborn with upper respiratory infection not want to eat
newborns are obligate nose breathers
ICP interventions
-elevate head of the bed 30 degrees
-administer mannitol
hypothyroidism symptoms
lethargic, slow, jaundiced
medication for thyrotoxicosis
what is the priority assessment for regular wellness of a 6 month year old
update on vaccination status
9 month fine motor skill milestones
-pincer grasp
-grabbing a rattle
12 month year old physical milestones
-birth weight doubled
-anterior fontanelle is closed
Anticipatory guidance for toddlers
-bedtime fears are normal
-prevent giving food with caries
-negatism and ritualism is normal
-decrease in appetite is normal
method to promote sleep in children with bedtime fears
-keep a dim light in the room
Findings of nephrotic syndrome
urine dipstick of 2+ protein
ankle edema
hyperlipidemia
NOT polyuria
anorexia?
primary cause of hypertension in pediatrics
renal dysfunction
Meningocele interventions
-keep dressing moist and use sterile technique
a failure to thrive patient will likely have
developmental delays
what so we not do for assessment of epiglottis
-use tongue depressor to inspect oral mucosa
-throat culture
what should we do for epiglottis patient
-vitals
-past medical hx
-auscultaion of the chest
-observe patient’s ability to swallow
with an acyanotic defect what finding would be reported to provider
dyspnea as it is a sign of heart failure
What is a sign of slipped capital epiphysis
-pain in a PUBERTAL child
chemotherapy patient with neutropenic precautions should not be
pulled around
vaccines due ages 4-6
1. DTaP (Diphtheria, Tetanus, Pertussis)
5th dose (final booster)
Completes protection against diphtheria, tetanus, and whooping cough
2. IPV (Inactivated Polio Vaccine)
4th dose (final dose)
Completes polio immunity series
3. MMR (Measles, Mumps, Rubella)
If not already given earlier:
2nd dose is completed by age 4–6
4. Varicella (Chickenpox)
2nd dose (final dose) by age 4–6
5. Annual Flu vaccine
Recommended every year for all children 6 months and older
a 5 year old should be up to date on
By age 5, most children should also already be up to date on:
Hepatitis B series
Hepatitis A series
Hib (Haemophilus influenzae type b) series
Pneumococcal (PCV) series
Rotavirus (completed in infancy)
normal temperatures in pediatrics
Normal range: 97* – 100.4*F
• Axillary: 97.6*F
• Oral or tympanic: 98.6*F
• Rectal: 99.6*F
HR range for an infant
100-160
HR range for toddler
90-140
HR for school aged
75-120
normal RR for an infant
30-60
normal RR for toddler
24-40
normal RR school aged
18-30