Lecture 4: Breathing Systems, Scavenging, and Intubation Supplies
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
36 Terms
Where are common areas to find a leak in the breathing system?
neck of reservoir bag
breathing circuit hoses
any hose connection
inlet/outlet to vaporizer
one-way valves
CO2 absorbent canister
flow meter
What are the important safety concerns of the breathing machine?
pressure check (aka leak test) any breathing system (and machine) prior to use
pollution to environment and personnel
patient may wake up because not getting enough anesthetic
patient may become hypoxemic if not getting enough O2
What is the function of the breathing systems and what are the 2 main types?
deliver gases and eliminate exhaled CO2
2 main types: rebreathing, non-rebreathing
True or false: rebreathing system (aka circle system), lower O2 flows than nonrebreathing system.
true
What are the components of the rebreathing system?
fresh gas source
unidirectional valves
breathing hoses
breathing system pressure gauge
CO2 absorber
APL valve
reservoir bag
What is the pathway of gas in a rebreathing system?
gases flow in a one-way circular pattern → into patient via inspiratory hose → out of patient through expiratory hose
What prevents rebreathing of CO2 in a rebreathing system?
chemical absorption (sodasorb)
What are the advantages and disadvantages of rebreathing systems?
advantages: can use lower O2 flow rates; easy to set up and use
disadvantages: increased resistance for smaller patient; more components to work with
What are the recommended oxygen flow rates for a closed circle system, low-flow circle system, and a semi-closed circle system?
closed circle system: 4-11 mL/kg/min - oxygen flow approximates patient’s oxygen consumption, which varies with metabolic rate
low-flow circle system: 10-22 ml/kg/min - oxygen flow rate > than patient’s oxygen consumption
semi-closed circle system: 22-44 ml/kg/min - fresh gas inflow exceeds the uptake of oxygen by patient
What are the advantages and disadvantages of close circle systems?
Advantages: more economical, retain more heat and humidity, and less likely to cause OR pollution
Disadvantages: vaporizer accuracy compromised, depends on your assessment of O2, and CO2 absorption completely dependent on chemical absorbant
What are the advantages and disadvantages of low-flow circle systems?
Advantages: economical, some heat and humidity retained, and reduced waste gas
Disadvantages: slow to change anesthetic depth
What are the advantages and disadvantages of semi-closed circle systems?
Advantages: N2 accumulation insignificant, rapid changes in inspired anesthetic concentration, CO2 partially eliminated via pop-off valve
Disadvantages: less economical, more heat and humidity lost
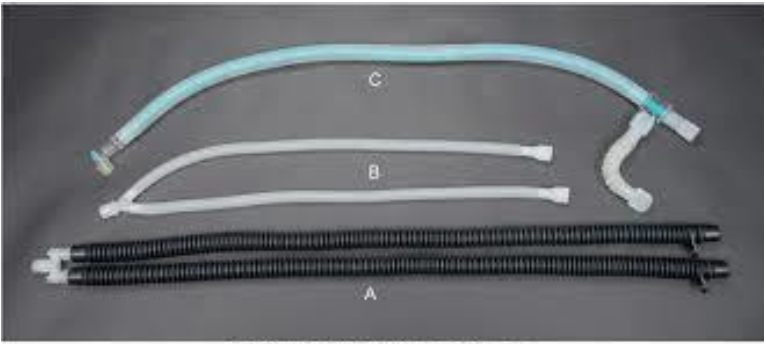
What are these three rebreathing (circle) system hoses?
A. adult hose for patients 7-150 kg
B. pediatric hose for patients <7 kg
C. universal-F hose comes in adult and pediatric sizes
How does a pressure gauge on a breathing system differ from oxygen cylinder pressure gauge?
measure in mmHg where as oxygen cylinder pressure read in psi
What can occur when CO2 absorption canister is exhausted?
CO2 will accumulate in circuit → rebreathing of CO2 → respiratory acidosis
What are the methods/tools to determine when to change soda lime?
capnography (increased inspired CO2 and ETCO2)
color change (useful, but not reliable)
lack of heat in canister
hardness of granules
clinical signs in patient
What are the components of a non-breathing system?
fresh gas source
expiratory limb or coaxial breathing hose
open/close valve
reservoir bag
What is the typical O2 flow rate?
150-300 ml/kg/min
Which patient should use a non-rebreathing system?
if < 3kg → always
if > 3kg → optional unless very large (not used for horses)
What are the advantages and disadvantages of a non-rebreathing system?
Advantages: less resistance to breathing for patient, little to no dead space and fewer components that can leak or malfunction
Disadvantages: higher O2 flow rates required to get rid of CO2 ➔ pollution to environment and can contribute to hypothermia; not as economical
What are the most commonly used non-rebreathing systems used in vet med?
Mapleson D (Bain circuit = modified Mapleson D)
Mapleson F (modified Jackson Rees circuit)
How can you prevent exposure to waste air gas?
engage a scavenging system
leak test the machine and breathing system prior to use
use cuffed and correctly sized endotracheal tubes
use a low-flow circle system if possible
avoid mask and chamber inductions
when disconnecting patient-turn off flow meter, vaporizer, empty gas from bag in to scavenging and occlude Y piece
perform machine and equipment maintenance periodically
adequate ventilation of areas where anesthetic gas exposure occurs
What are tips for safely filling or emptying vaporizers?
Ideally wear a charcoal mask
Always announce that you are filling a vaporizer if it must occur when other personnel are in the room
Best to select a time late in the day (or first thing Monday morning) to refill vaporizers to minimize unnecessary exposure
Replace cap on bottle when done
Switch to key-fill vaporizers if possible
Always turn vaporizer dial OFF before filling!
What are the 2 types of scavenging systems?
passive: charcoal absorption, to outside wall or window
active: central vacuum collection
What are the advantages and disadvantages of charcoal absorption?
advantages:
absorbs halogenated anesthetic gases
mobile; initial cost is low; easy to set up
disadvantages:
does NOT absorb CO2 or N2O
must be replace dafter gaining 50g of weight (8-12hrs of use)
use limited to lower oxygen flow rates
adds resistance
Generally, you want to use the largest size of endotracheal tube that will fit without causing trauma to the _______.
larynx
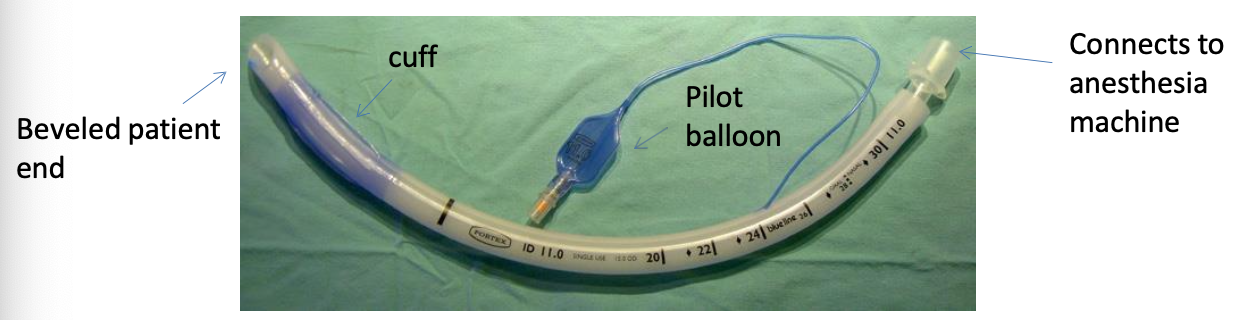
What is the most common type of ETT?
murphy
What is the term that describes the portions of the breathing passages that contain air, but there is no gas exchange (mouth, nasal passages, pharynx, trachea, end of ET tube/Y-piece)?
dead space
What is a murphy type ETT?
“Murphy’s Eye” design - an oval hole positioned on the bevel facing the opening of the tube
if distal end of tube becomes occluded, there is still air flow
What is the difference between a cuffed ETT under a low volume high pressure system vs high volume low pressure system?
low volume high pressure: take a small amount of air, but put a high amount of localized pressure on the tracheal mucosa
high volume low pressure: larger amount of air, but low pressure on the trachea and widely distributed
What are cole ETTs?
uncuffed
characterized by a “shoulder” near the distal end (laryngotracheal portion)
designed to create a seal by using a smaller end to fit in the arytenoid carilages
smaller portion goes in trachea

What are guarded or armored ETTs?
made of silicone rubber
have steel wire or nylon coil embedded in the wall
resists kinking (good for awkward cases with poor visibility or significant neck bending)
more expensive

How does a laryngoscope work and what are the benefits?
Allows for visualization
Light source (allows for quick detection of abnormal anatomy)
Easier accessibility to airway
Apply light pressure to base of tongue, just underneath epiglottis.
Tilts larynx ventrally and opens glottis, frees up the epiglottis if still tucked underneath soft palate
What are the steps for correct endotracheal intubation?
preoxygenate patient 3-5 mins
at least 3 sizes ETT checked and ready + other supplies
assistant holds head, opens mouth, pulls tongue → person intubating grasps laryngoscope in one hand and ETT in other (pos. application of 0.2-0.5ml regular 2% lidocaine to arytenoids)
airway assessed for size ETT → ETT lubricated and passed between arytenoids, slight twisting motion may be needed
distal tip ETT should not extend past thoracic inlet
attach ETT adaptor to breathing circuit with oxygen turned on and capnograph attached → assess capnograph waveform to confirm placement and secure ETT In place
cuff inflation technique should occur next
confirm strong heartbeat and turn inhalant to predetermined value, assist w ventilation, instrument patient with monitors, and begin anesthetic record
What are some methods to confirm ETT placement?
direct observation of ETT going into trachea
capnograph reading from ETT registers high enough CO2 value
feel breath from end of ET tube on hand
auscultation of breath sounds bilaterally when breath give
absence of two “tubes” palpated because ETT is inside the trachea
feel the ETT sliding past tracheal rings, also use to guid depth of placement
What is the cuff inflation technique (aka minimal occlusion volume technique)?
should be no escape of gas from ETT cuff when delivering a positive pressure ventilation (manual breath) and bag is squeezed to 20 cmH2O
by ~25 cmH2O air should be able to escape around tube, if not some air should be removed from pilot balloon to prevent over inflation of the cuff
recheck after patient asleep 10-15 min