EXS 320 - Unit 4 Exam
1/151
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
152 Terms
Skeletal muscle is composed of
individual muscle fibers containing myofibrils
myofibrils contain
contractile proteins called actin and myosin
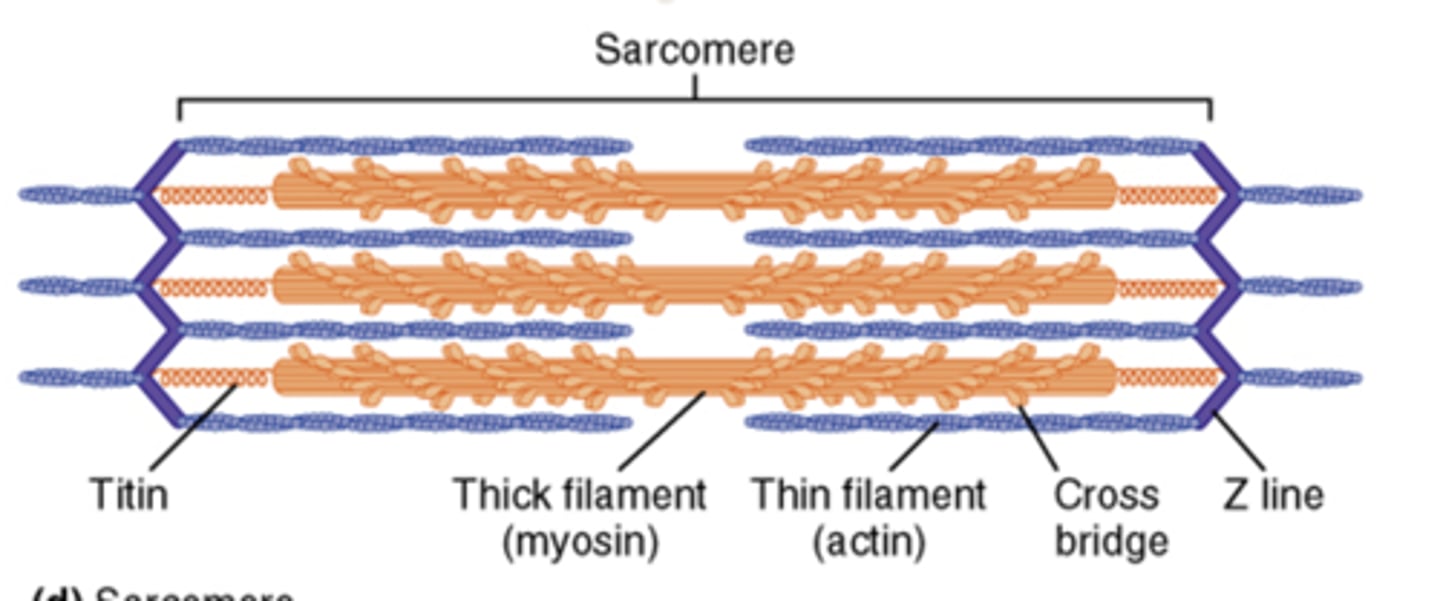
sarcomere
functional unit of skeletal muscle contraction, primary composed of actin and myosin
Structure of skeletal muscle
fascicle, muscle fiber (w/nucleus), sarcolemma, myofibril, protein filaments
actin =
thin filaments
myosin =
thick filaments
Actin & myosin function
Actin molecules form double-helical actin strands, each actin has myosin-binding site, covered by tropomyosin, myosin can only bind to actin after troponin complex removes tropomyosin from actin
myosin structure
has tail and head
- at top of head, a actin-bind site,
-just below binding site is ATPase site
- two myosin molecules bind at their tail ends
sliding filament model
tails of myosin bind to myosin binding sites on actin and pull, allows for sarcomere shortening (muscle contraction)
ATPase =
enzyme that splits ATP releasing energy that goes into the myosin heads
sarcomeres
the functional unit, have Z-lines at each end of myosin heads attached to actin and allow pulling of actin in
Muscle Contraction
1 - following depolarization of sarcolemma, calcium is released from Sarcoplasmic reticulum & attaches to troponin;
2 - tropomyosin moves on actin and uncovers myosin binding sites;
3 - actin-binding sites on myosin heads attach
4 - In presence of ATP, myosin heads "ratchet" and pull actin to the middle of the sarcomere (crossbridge cycle )
Relaxed actin =
when tropomyosin covers binding sites,
contracting actin =
myosin binding site exposed with activation of troponin complex by calcium
When ATP is hydrolyzed to ADP,
creates a high energy configuration of myosin, and attaches to actin releasing phosphate group
Power stroke =
actin gets pulled toward middle of sarcomere
Excitation-contraction coupling
ACH = the NT that binds to Nicotinic cholonergic receptors
- causes channels to open and close allowing sodium and potassium to depolarize & create an action potential in the muscle fibers.
- that action potential travels down T-tubule which triggers the release of Ca2+ from SR ,which allows muscle contraction
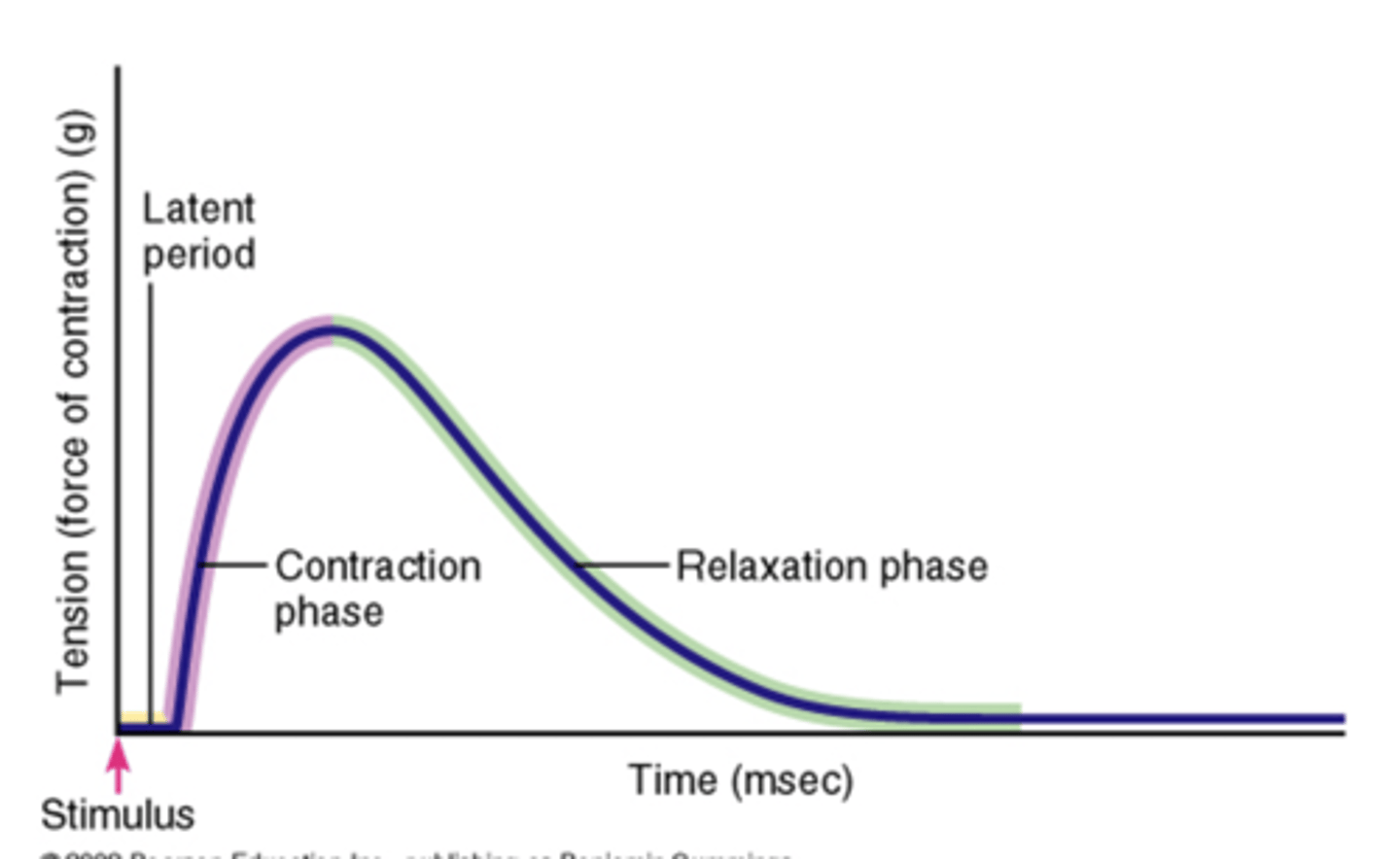
muscle twitch -
mechanical response of individual muscle fiber to a single action potential originating in the motor neuron
phases of twitch
1. latent period
2. contraction period
3. relaxation period
isotonic contraction
muscle shortens
types of muscle twitch
determined by the ability of the muscle to produce tension & amount of load
1 - isotonic
2 - isometric
isometric
muscle cannot shorten
isotonic muslce contraction
creates plateaus where the muscle shortens and the load moves
Isometric muscle contraction
happens with a load greater than the tension that the muscle can develop, no shortening occurs
Factors that effect force generation
- frequency of stimulation
- fiber diameter
- fiber length
- recruitment of fibers
- size of motor units recruited
increased frequency =
increased tension
increased fiber diameter =
increased force
maximal tension can develop if
If fiber length is at normal resting length or slightly greater , at beginning of contraction,
treppe
when muscle is stimulated at a high rate, peak tension increases with ever twitch to a higher constant level, till a plateau
Ideal length- tension curve =
between 100-115%
summation occurs
when twitches occur frequently the muscle fibers cannot relax adequately and ____________ _________
then tentanus occurs
when futher increases in stimulus frequency results in increased tension past summation and
maximum tetanic contraction
any further increases past tetanus cause the muscle to generate its maximal force
decreased length of muscle
allows the crossbridges to completely overlap each other
-60-100%
increased length of muscle
not all crossbridges overlap with thin filaments
- 120-170%
Recruitment of fibers
increase in number of active motor units leads to greater # of fibers recruited = greater force generation
type of fiber recruited
Slow twitch vs. Fast twitch, affects force generation
Size of motor unit recruited
- refers to number of fibers in given motor unit
increased size = Greater force
- larger diameter motor neurons are present in motor units w/ larger muscle fibers - HARDer to activate but create greater force
- smaller neurons are activated first to allow for fine motor control
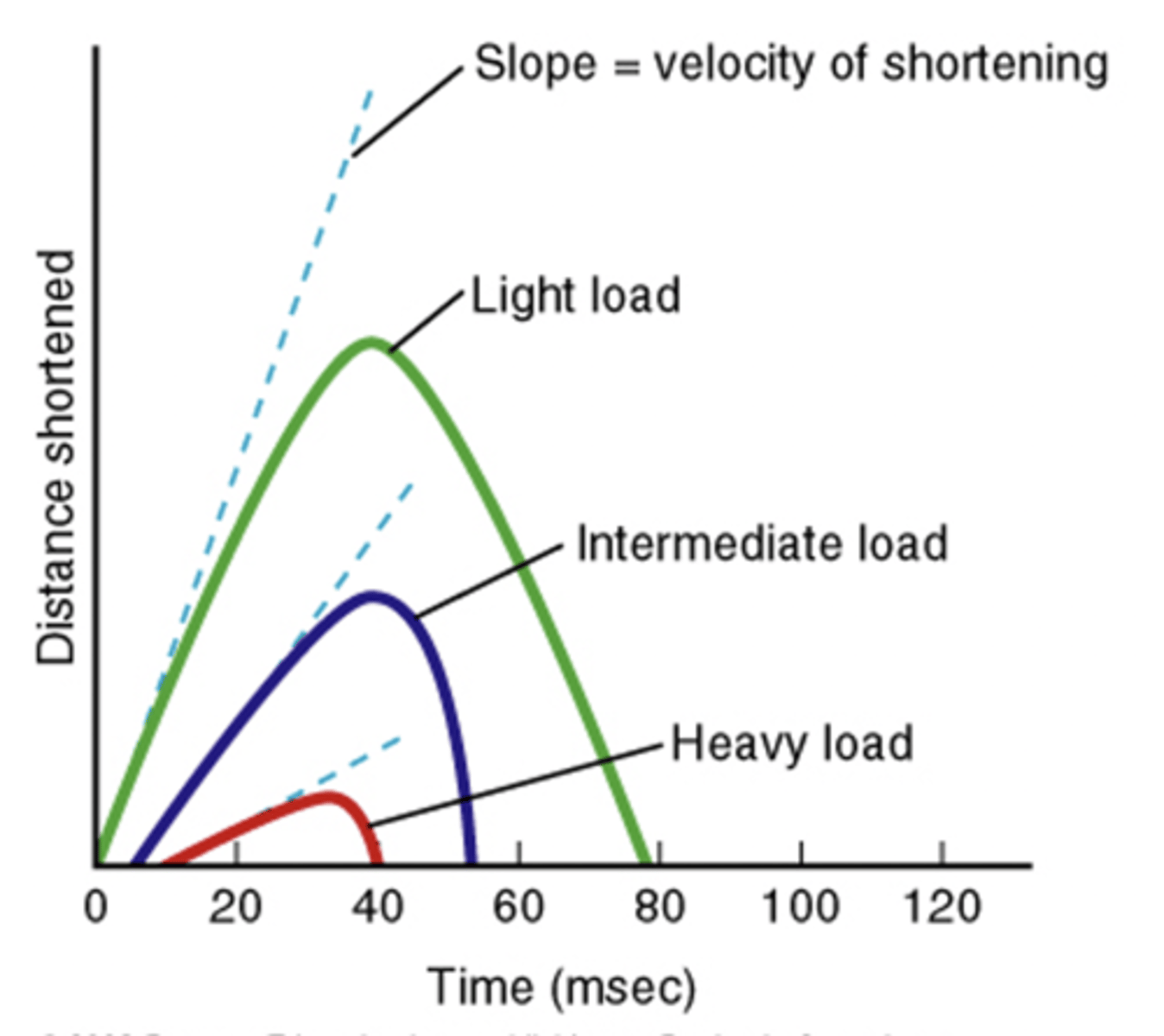
Speed of muscle fiber shortening
1 - latent period of shortening increases as load increases
2 - increasing load results in slower speed of shortening
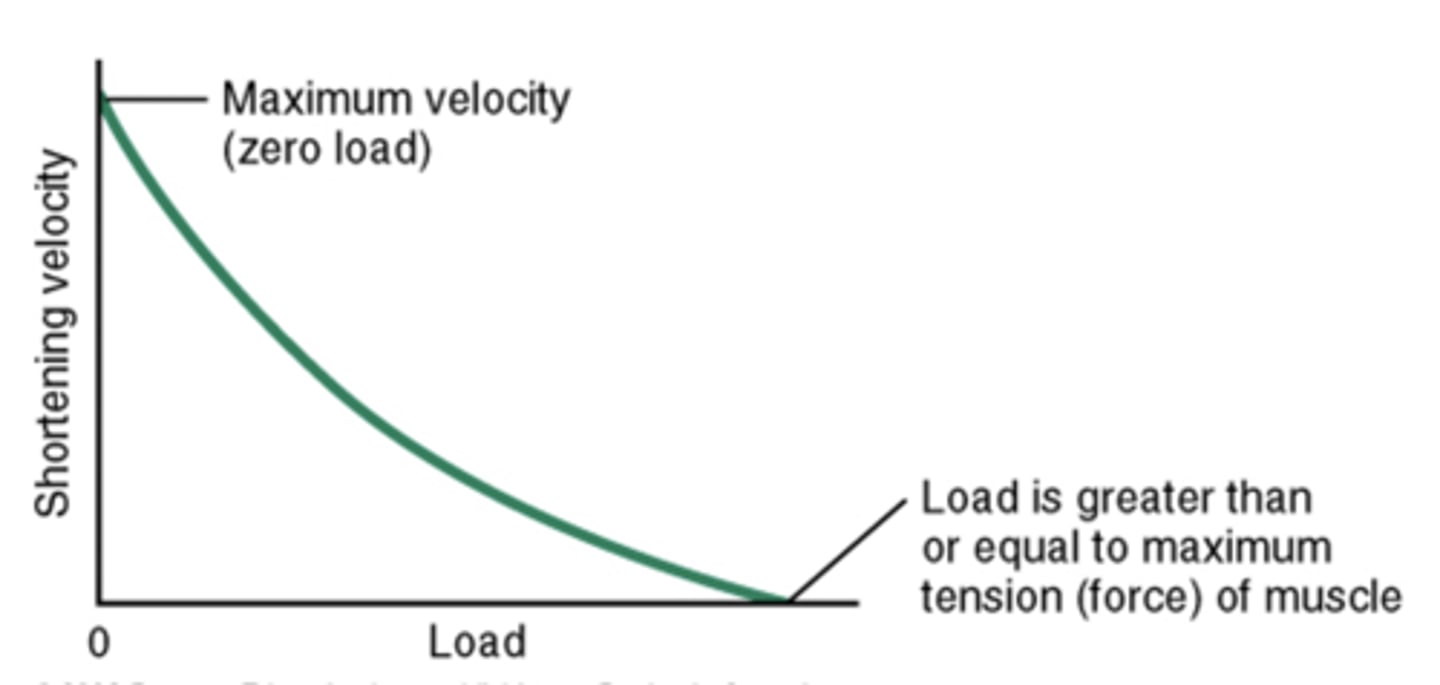
effect of load on muscle shortening
Smooth muscle
found in internal organs and blood vessels
- under autonomic control
- lack sarcomeres
- actin & myosin are present in parallel configuration but run together in oblique fashion
Smooth Muscle Excitation-Contraction Coupling
utilizes calcium-calmodulin interaction that activates myosin kinase enzyme
Myosin (light-chain) kinase (MLCK)
phosphorylates myosin heads allowing for binding to actin and cross-bridge activity
smooth muscle contraction
contraction squeezes when thick and thin filament overlap past rest
Cardiac muscle
- has striations/sarcomeres
- utilizes calcium-troponin- tropomyosin mechanism for contraction
two areas of cardiac muscle cells
sinoatrial node & AV node
- have "pacemaker" properties
- can contract w/o outside stimulation
via gap junctions
Cardiac cells communicate _____
- allow coordinated contractions of heart
autonomic input
cardiac muscle controlled by
- influences rate and forcefulness of contractions
excitation-contraction coupling in Cardiac muscle
1 - current (AP) spreads through gap junctions to contractile cell
2 - action potentials travel along plasma membrane & T tubules
3 - Ca2+ channels open in plasma membrane & SR
4 - Ca2+ induces release from SR
5 - Ca2+ binds to troponin, exposing myosin binding sites
6 - crossbridge cycle begins
7 - Ca2+ is actively transported back into the SR and ECF
8 - tropomyosin blocks myosin-binding sites (muscle fiber relaxes )
Cardiovascular system
heart, blood vessels, blood
heart
right and left atria, right and left ventricles
blood vessels
arteries, arterioles, capillaries, venules, veins
blood
plasma, erythrocytes, leukocytes, platelets
cardiovascular system functions
- transport of oxygen and nutrients to cells
- transport of metabolic waste products to organs for excretion
- temperature regulation
path of blood flow
- oxygenated blood goes from lungs to pulmonary veins, into left atrium, through left ventricle, into aorta, oxygen levels blood into systemic capillary beds
- deoxygenated blood goes from systemic circuit into venae cavae into right atrium through right ventricle and into pulmonary arteries to pulmonary circuit , where O2 moves into blood and CO2 leaves
primary function of heart
create a "pressure head" for the entire circulatory system
right atrium is
responsible for collecting blood from body (minus lungs), via inferior and superior vena cavae, sending it to the right ventricle pushing it to the lungs for exchange of gases b/w blood and lung air
left atrium is
responsible for collecting blood from lungs and sending to left ventricle which pushes it out to the whole body (except lungs)
left ventricle must
contract with greatest force to be able to distribute blood to such a large area, thus, it has the greatest mass of muscle tissue
atrioventricular (AV) valves
valves b/w the atria and ventricles
- open when atrial pressures exceed ventricular pressures allowing blood to flow from the atria to the ventricles
tricuspid valve
right AV valve
bicuspid valve
left AV valve
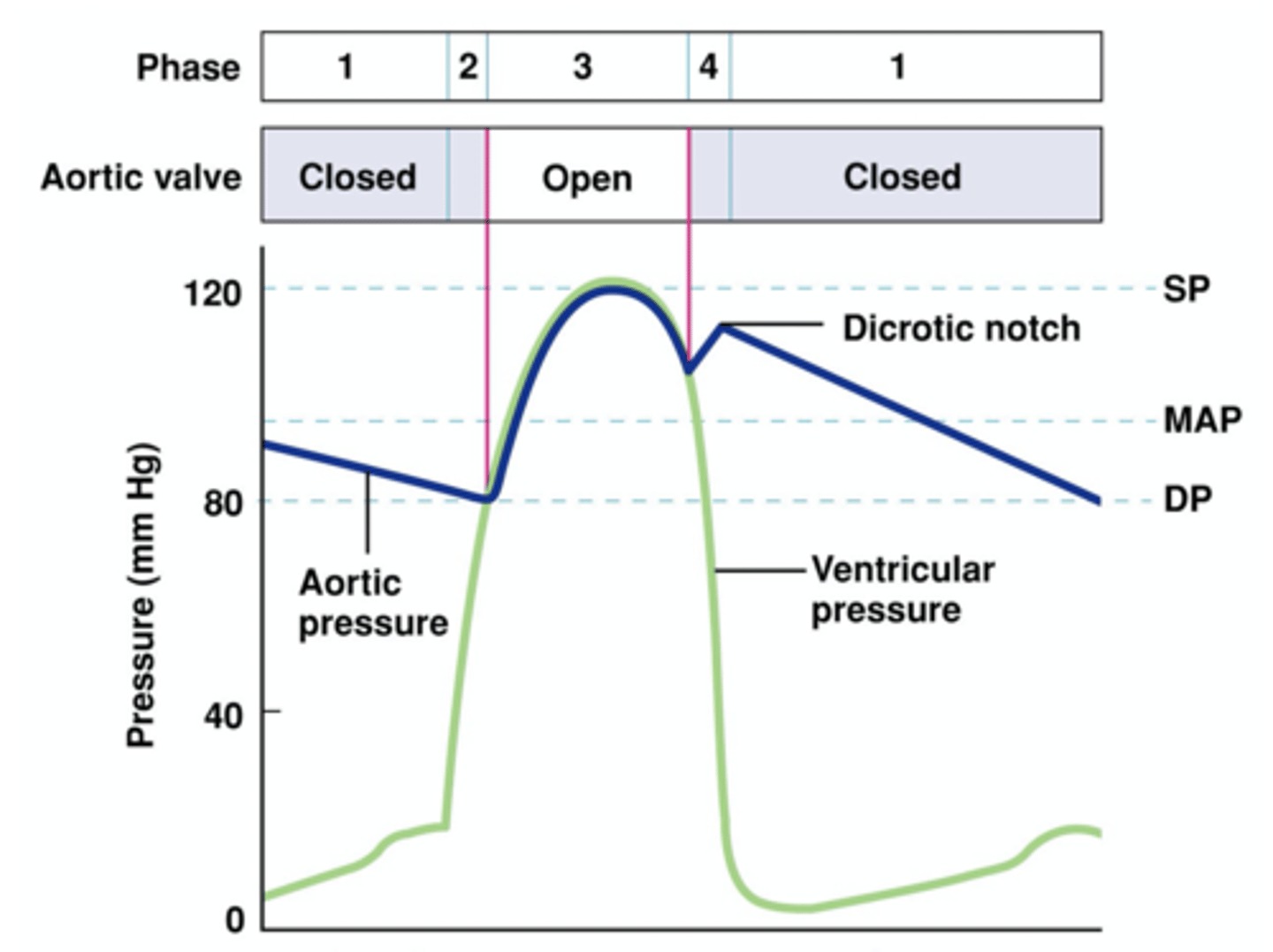
pulmonary and aortic semilunar valves
valves b/w ventricles and main blood vessels leaving the heart
- open when pressure inside the ventricles exceeds the pressure in the pulmonary trunk and aorta
valve cusps
serve to seal the heart valves when ventricles relax, and open when ventricles contract, allowing blood to flow into aorta and arteries
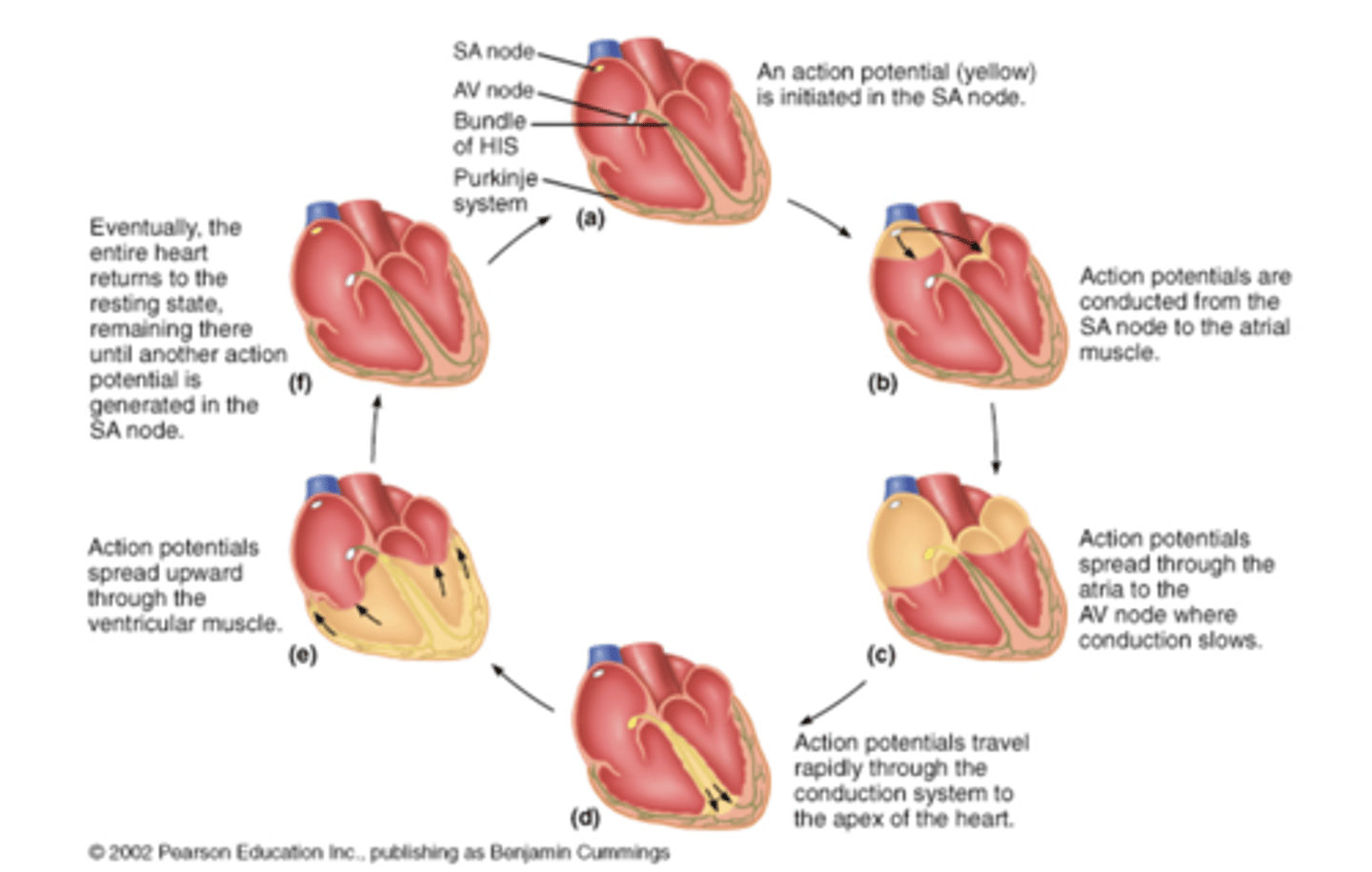
electrical conduction in the heart
starts at SA node, spreads through atria, to AV node
- at AV node, slight delay before conduction spreads down the septum through AV bundle, the right/left bundle branches and then up the walls of the ventricles via Purkinje fibers
intercalated disks
where cardiac muscle cells are connected
Within the intercalated disk
- gap junctions allow ions to pass b/w adjacent cells and thus allows current to flow from cell to cell
- desmosomes keep cells from tearing apart during contraction
pacemaker cells
in SA and AV node spontaneously generate action potentials
- SA node cells control overall pace of HR (70 bpm) , if SA node does NOT depolarize, AV node will spontaneously depolarize at rate of 50 bpm
After depolarizing, AV node
will be in refractory state at the SA node rate and will not be able to depolarize at its own intrinsic rate
conduction fibers
associated w/ pacemaker cells and spread AP throughout heart
Conduction moves
in "waves" starting on outside of atria and moving through ventricles in "inside-out" fashion
spread of action potentials through heart
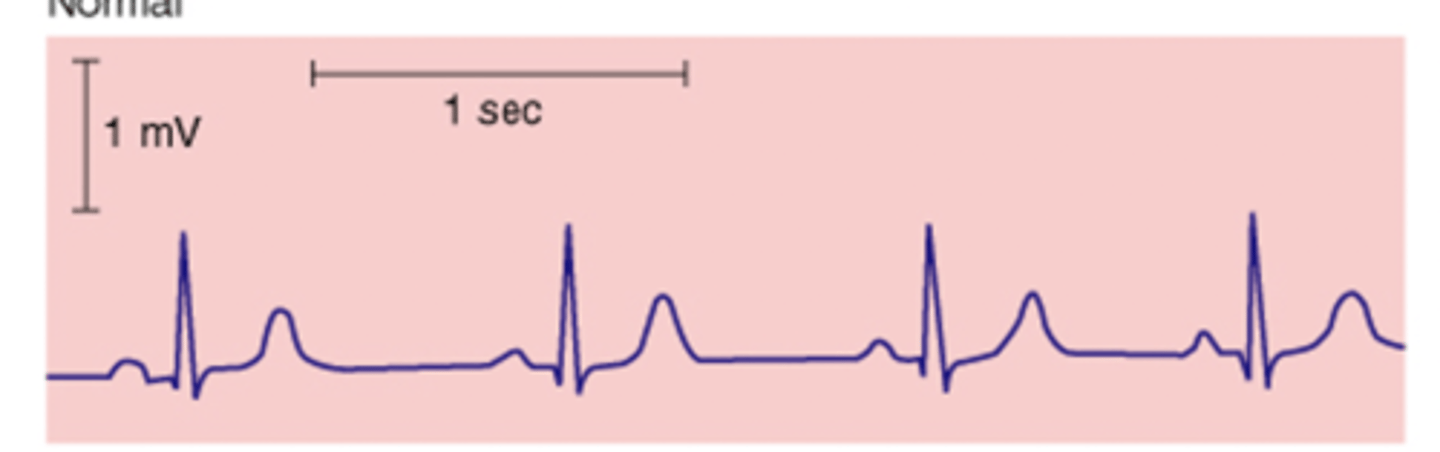
EKG (ECG)
the wave of depolarization through cardiac tissue can be detected and creates 5 waves (P,Q,R,S,T)
P wave
represents atrial depolarization
QRS waves
make QRS complex & represents ventricular depolarization
T wave
represents ventricular repolarization
Normal ECG reading
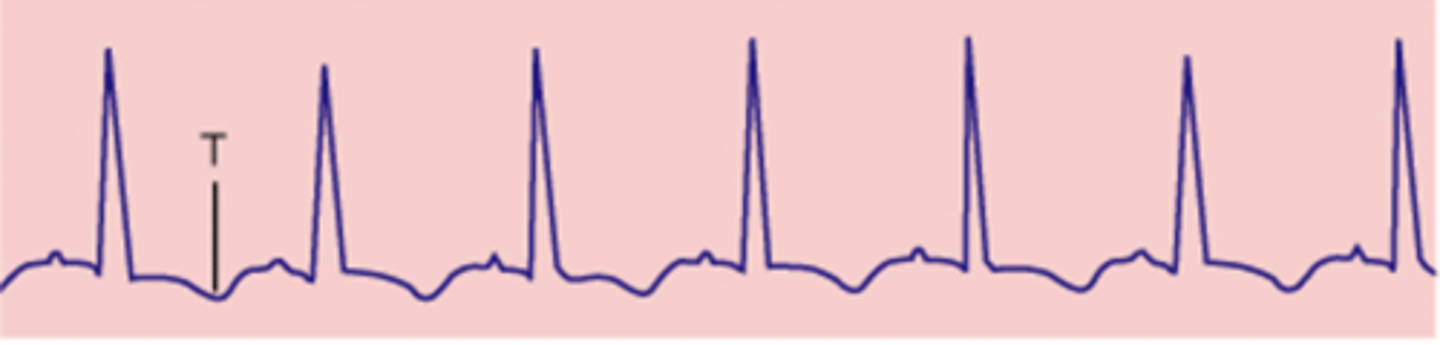
sinus tachycardia
inverted T wave
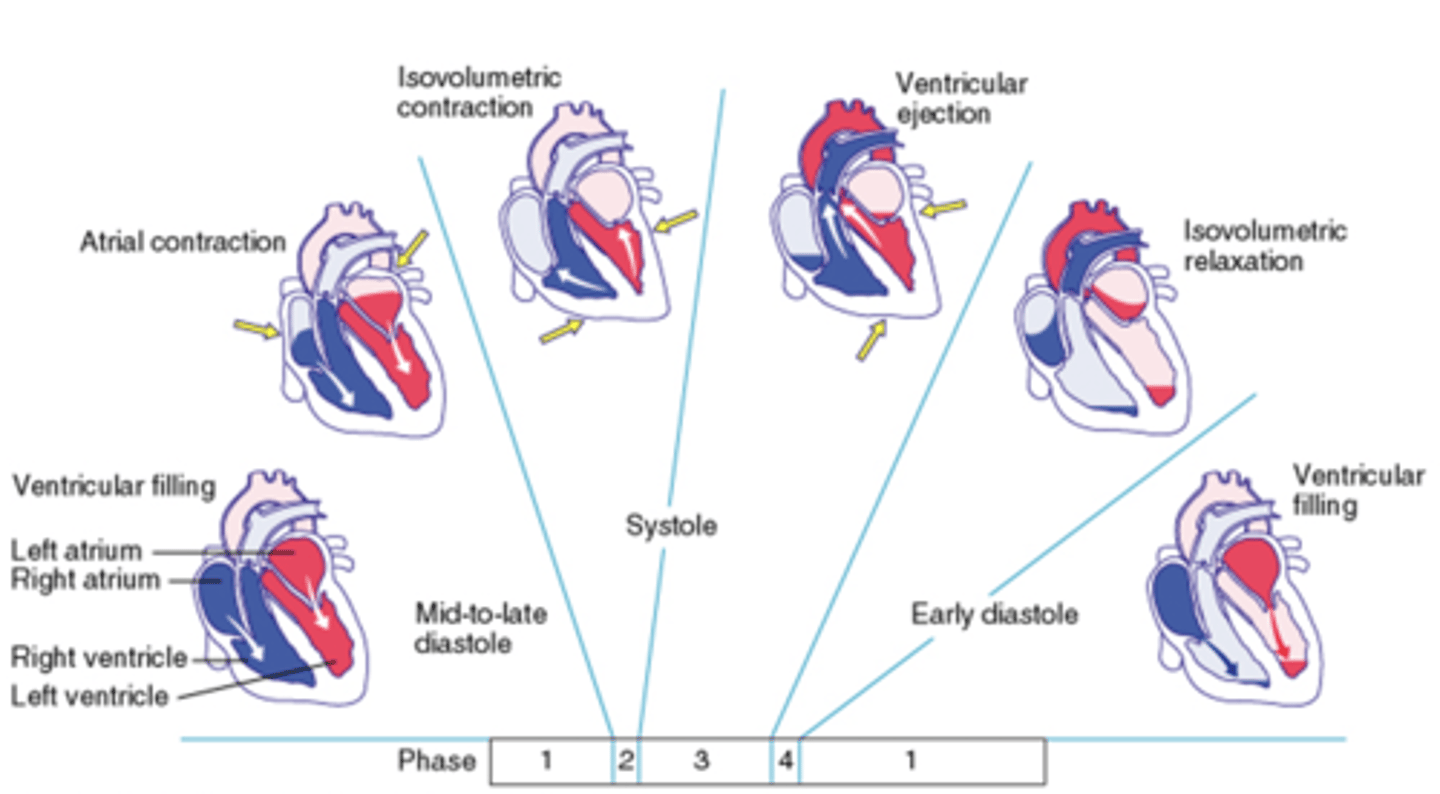
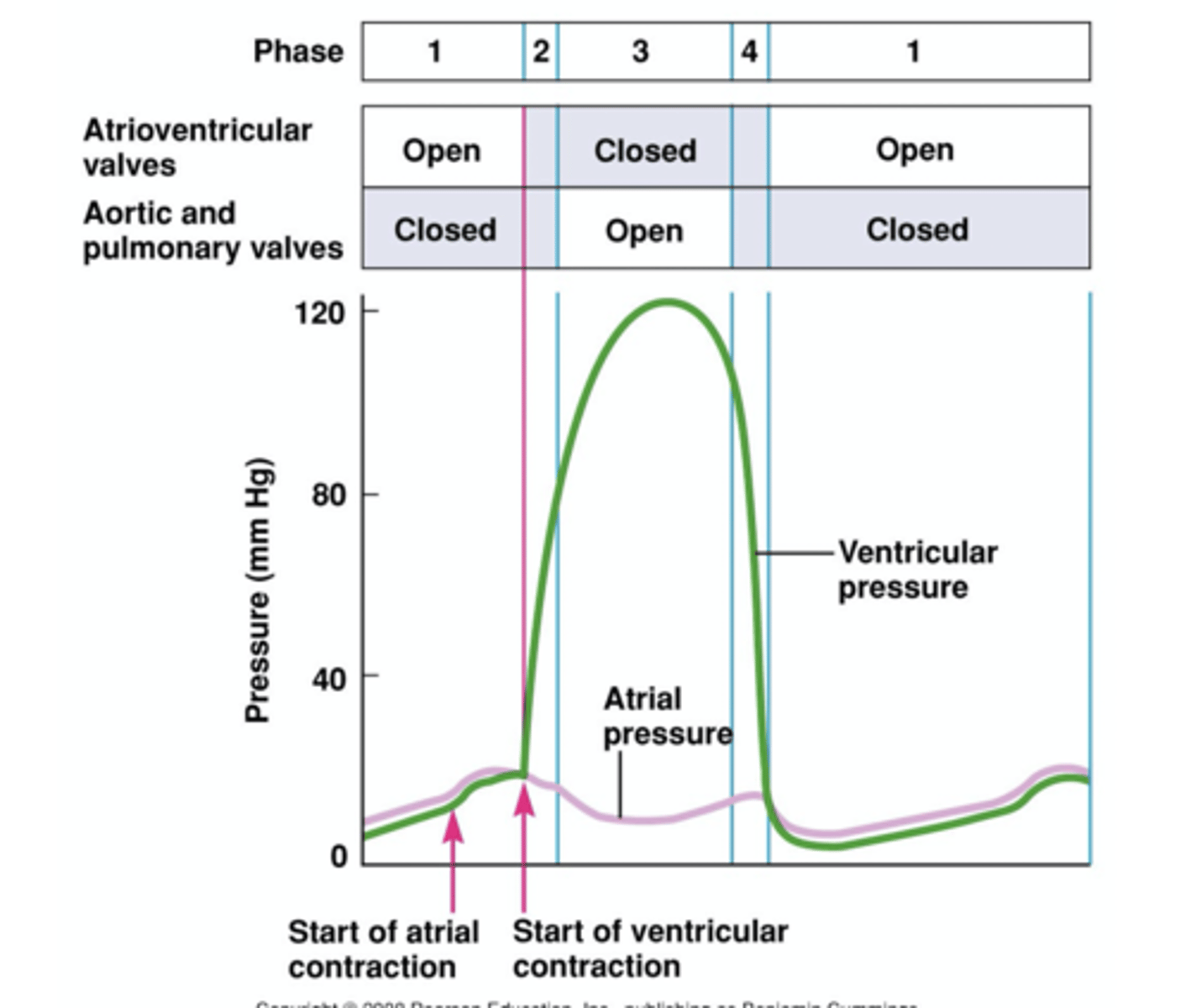
cardiac cycle
refers to events that relate to the flow of blood through heart during one complete heartbeat
cardiac cycle includes
- pumping phases (pump cycle )
- valve opening/closing
- pressure changes in atria, ventricle, & aorta
- volume changes in ventricles
- heart sounds associated w valve opening/closing
Phases of cardiac cycle
1. Ventricular filling: mid-to-late diastole
2. isovolulmetric contaction, systole
3. ventricular ejection, systole
4 - isovolumetric relaxation, early diastole
ventricular pressure during cardiac cycle
aortic pressure during cardiac cycle
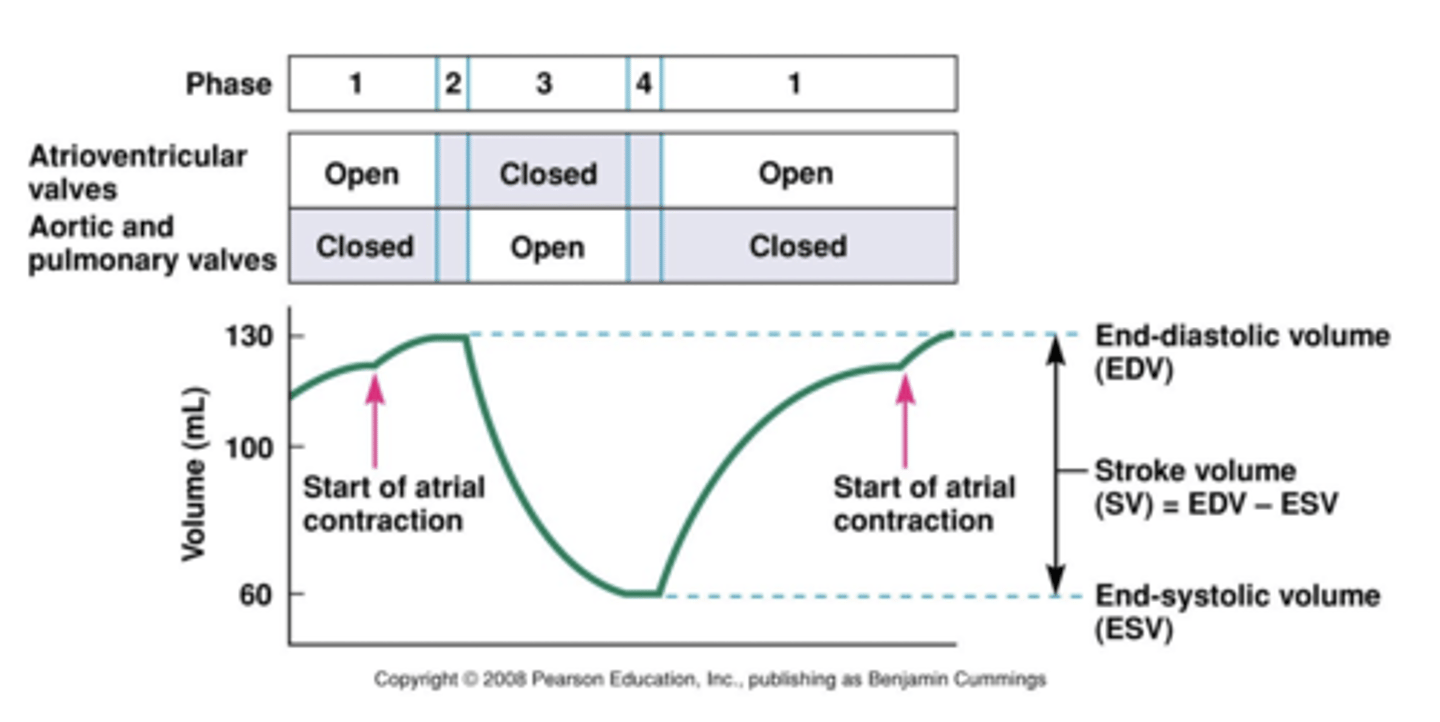
ventricular volume during cardiac cycle
heart sounds
heard during phase 2 and 4 of cardiac cycle
cardiac output =
heart rate (HR) x stroke volume (SV)
stroke volume =
end diastolic volume (EDV) - end systolic volume (ESV)
Ejection Fraction (EF) =
Stroke volume (SV) / End-diastolic volume (EDV) x 100%
venous return
flow of blood back to the right atrium
preload
amount of stretch of the ventricular wall myocardium
- related to end-diastolic volume (EDV)
afterload
combined load of EDV and arterial resistance during ventricular contraction
- increased afterload = decreased stroke volume (SV)
sympathetic fibers project
to the SA node, AV node, and ventricular myocardium
increases heart rate
stimulation of heart by sympathetic fibers____ ___ ___
Parasympathetic fibers project
to SA node and AV node
decreases HR
stimulation by parasympathetic fibers ____ ___
will increase CO
increased Heart rate ____ ____ __
increases force of contraction (contractility)
sympathetic fibers projecting ventricular myocardium
Epinephrine can
increase contractility & HR
increased contractility
decreases ESV resulting in greater SV
venous return
Stroke volume can be regulated by