T5 - IE1 - Pulmonology - Ostrom + Munjy - Integrated Pathophysiology of Asthma
1/75
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
76 Terms
Intermittent asthma symptoms
≤ 2 days / week
Mild persistent asthma symptoms
> 2 days / week but not daily
Moderate persistent asthma symptoms
daily
with REDUCED 5% FEV/FVC
For asthma go with __________ treatment for symptoms and ________ _______
- highest (treatment for symptoms)
- step down
i.e., start with step 5 and go down
Severe persistent asthma symptoms
Throughout the day
> 1x week night time awakening
Asthma
paroxysmal dyspnea accompanied by wheezing caused by a spasm of the bronchial tubes or by swelling of their mucous membrane
Paroxysmal dyspnea
sudden, recurring episode of difficulty breathing
seen with chest tightening, wheezing, coughing
Asthma is mild in ____% of population; ____% need regular medication
- 10(%)
- 2(%)
Asthma mortality is _______
- (is) rare
increasing over past 3 decades
Asthma is a $______ ______________ market industry
- ($)56 billion
For > 50% of patients, costs for asthma are __ ___% of family income
- > 18(% of family income)
Asthma triggers
environmental exposure
occupational exposure
drugs
foods
additives
diseases (e.g., infectious disease and toxins associated with ID)
cold air
Two phases of an asthma attack
early
- bronchospasm
inflammation
- late
Early phase of an asthma attack
bronchospasm
Late phase of an asthma attack
inflammation
Pathologic cascade of asthma figure
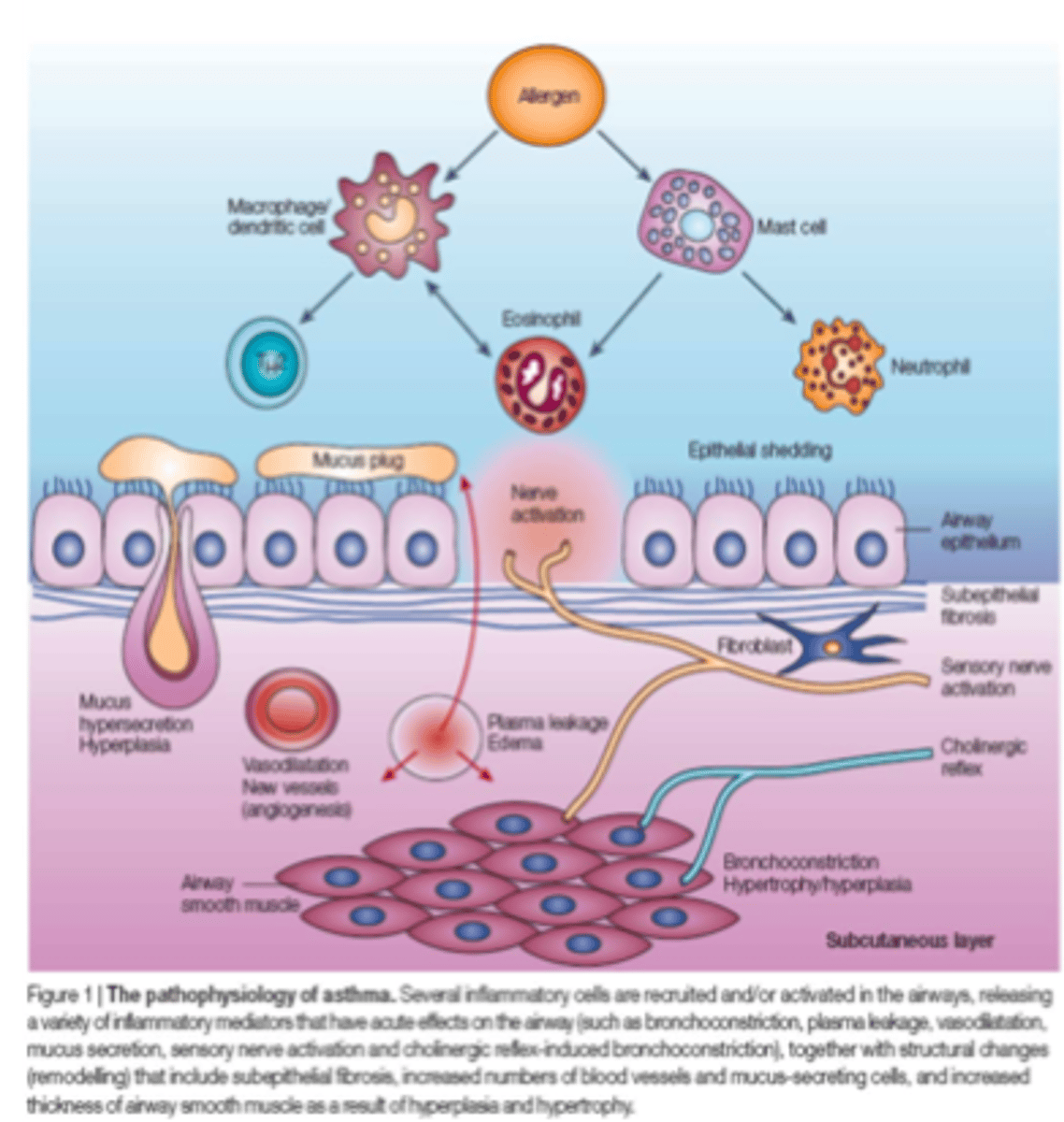
Pathologic cascade of asthma steps
1. allergen-induced bronchoconstriction
2. activation of immune cells
3. remodeling of airway tissue
4. hypercontractile status (due to hyperplasia / hypertrophy)
Pathologic cascade of asthma step 1: __________-induced ____________
- allergen(-induced)
- bronchoconstriction
Step 2. Activation of immune cells
Pathologic cascade of asthma step 1: allergen-induced bronchoconstriction
step 2. activation of ____________ ______
- (activation of) immune cells
Step 3. remodeling of airway tissue
Pathologic cascade of asthma
step 2. activation of immune cells
step 3. ___________________ of airway tissue
- remodeling (of airway tissue)
step 4. hypercontractile status
Pathologic cascade of asthma
step 3. remodeling of airway tissue
step 4. _____________ status
- hypercontractile (status)
Structural changes in the asthmatic pathway
Asthmatic airways have:
1. Increased number of goblet cells
(mucus production)
2. Thickened basement membrane
(myofibroblasts, extracellular matrix)
3. Increased number of smooth muscle
cells (hyperplasia)
4. Increased size of smooth muscle
cells (hypertrophy)
Structural changes in the asthmatic pathway - asthmatic airways have: increased number of ____________ _______, which _______ mucus production
- (increased number of) goblet cells
- increase (mucus production)
Structural changes in the asthmatic pathway - asthmatic airways have: thickened _____________ ________
- basement membrane
Myofibroblasts, extracellular matrix
Structural changes in the asthmatic pathway - asthmatic airways have: increased number of _________ _________ cells (__________)
- smooth muscle (cells)
- hyperplasia
i.e., increased amount of smooth muscle cells
Structural changes in the asthmatic pathway - asthmatic airways have: increased size of smooth muscle cells (_________)
- hypertrophy
i.e., strengthening of these smooth muscles
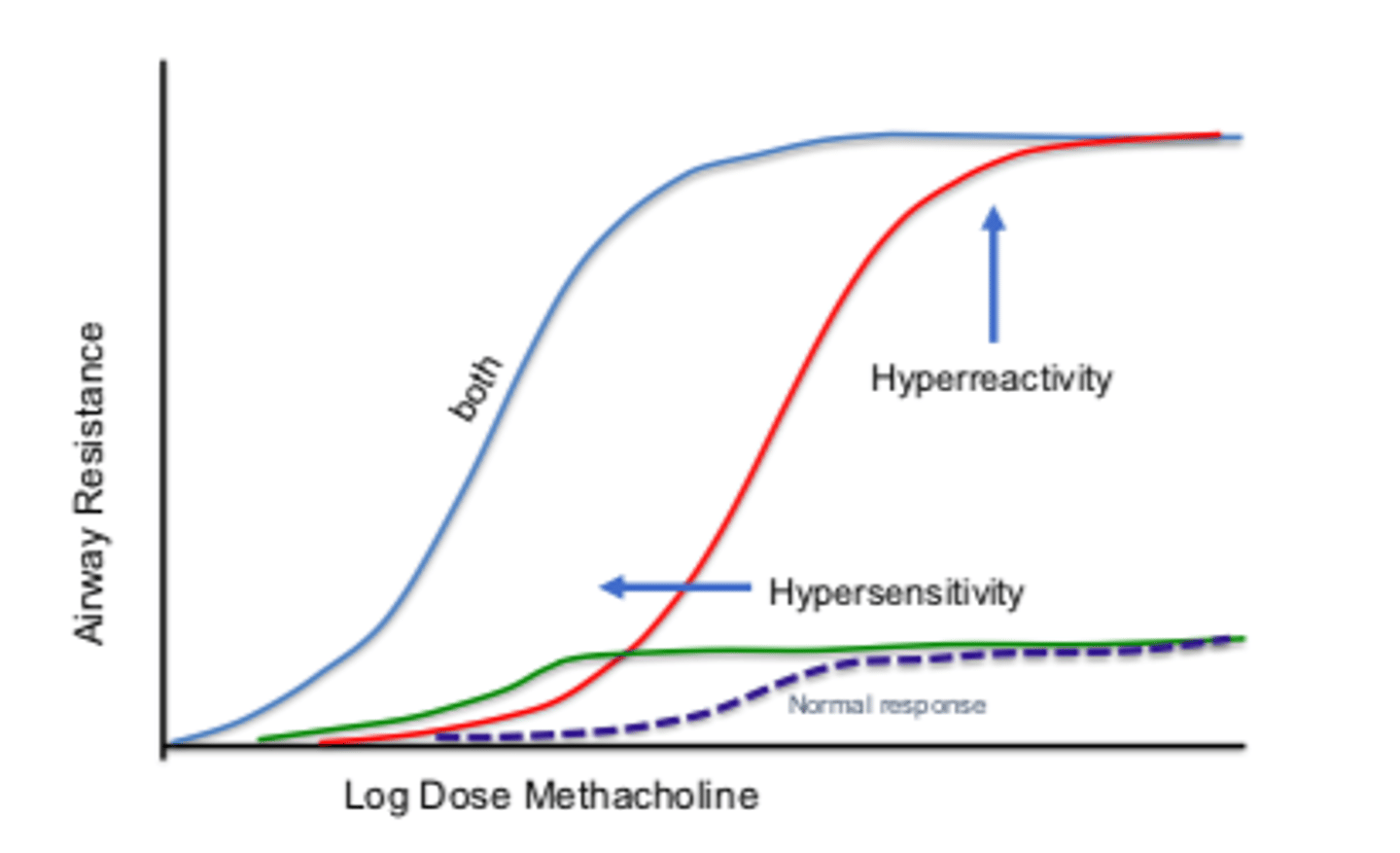
Bronchoconstriction is a ___________ physiologic response
- normal (physiologic response)
Non-asthmatics: low-level response to stimulus that produces mild, if any, bronchonstriction at normal to high doses (normal response)
Asthmatics are ALWAYs hyper-responsive airways
Bronchoconstriction normal physiological response: non-asthmatics
low-level response to stimulus that produces mild, if any, bronchoconstriction at normal to high doses
see figure 1a
Bronchoconstriction normal physiological response: Asthmatics ALWAYs have _______-_________ airways
- hyper-responsive (airways)
hypersensitivity: normal response to abnormally low stimulus dose (leftward shift)
hyperreactivity: exaggerated response to normal-high stimulus dose (upward shift)
see figure 1a
Insults
events in the brain such as trauma, infection, or chemical imbalance
Bronchoconstriction figure 1a
Non-asthmatics:
low-level response to stimulus that produces mild, if any, bronchonstriction at normal to high doses (normal response)
Asthmatics: hypersensitivity: normal response to abnormally low stimulus dose (leftward shift)
hyperreactivity: exaggerated response to normal-high stimulus dose (upward shift)
Methacholine challenge diagnosis: inhale _____________ concentrations of methacholine aerosols with ________ before and after each dose
- (inhale) increasing (concentrations of methacholine)
- spirometry
Results recorded as percent decrease in FEV1 from baseline for each step of the protocol & concentration applied
Methacholine challenge diagnosis: Results recorded as __________ decrease in ______ from baseline for each step of the protocol & concentration applied
- percent (decrease)
- FEV1
Positive reaction = 20% fall in FEV1
Methacholine challenge diagnosis: positive reaction = ___% fall in FEV1
- 20(% fall in FEV1)
If FEV1 does not fall by at least 20% the test is negative
Methacholine challenge diagnosis: negative reaction; does ______ fall by at __________ ___%
- NOT (fall)
- (at) least 20(%)
Methacholine challenge diagnosis: ____________ methacholine concentration varies by institution
- maximum (methacholine concentration)
Early asthma attack: bronchospasm - allergen attaches to _______ ________ and immunoglobulin-____ releases __________
- mast cell
- (immunoglobulin-)E
- (releases) histamine
Which causes the bronchospasm of the smooth muscle airway
Allergen also alerts the T-lymphocyte
Early asthma attack: allergen also alerts the ____-___________ which leads to the release of many __________
- T-lymphocytes
- (many) cytokines
IL-4, IL-5, GM-CSF, TNF, TGF
Cytokines released by t-lymphocytes after exposure to allergen induced asthma
IL-4
IL-5
GM-CSF
TNF
TGF
Cytokines from the t-lympocytes lead to late stage ___________
- (late stage) inflammation
Eosinophil releases ECP + MBP; Neutrophils release proteases + PAF
ECP
eosinophil cationic protein
MBP
major basic protein
Eosinophils release _____ and _____ during asthma
- ECF
- MBP
Neutrophils release _______ and _____ during asthma
- proteases
- PAF
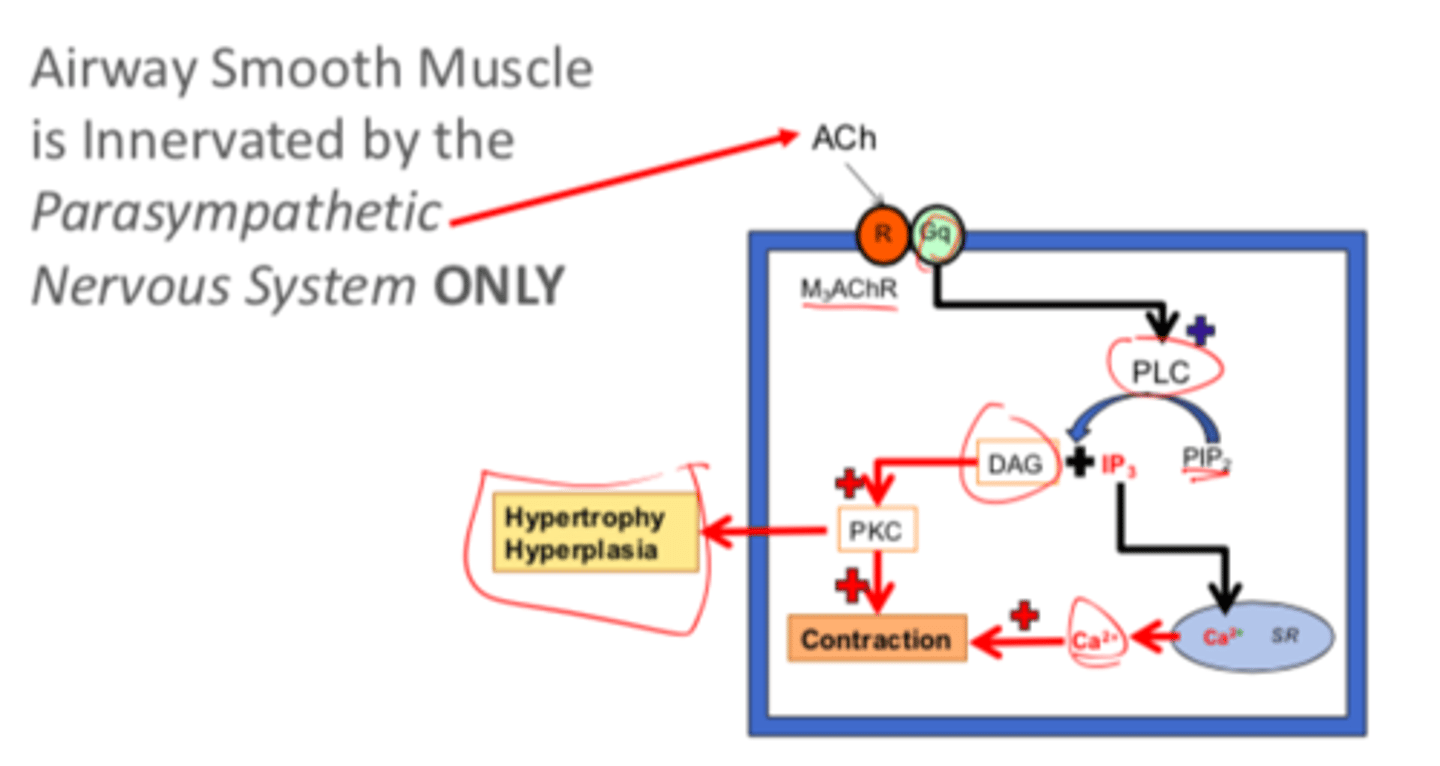
Airway smooth muscle is innervated by the ______________ nervous system ONLY
- parasympathetic (nervous system ONLY)
Airway smooth muscle contraction pathway
Ach -> M3AchR activates Phospholipase C -> PIP2 -> IP3 +DAG
DAG pathway
PKC (protein kinase C) -> contraction
IP3 pathway
IP3 increase of Ca in the seroplasmic reticulum, increased Ca2+ -> contraction
Airway smooth muscle contraction pathway: IP3 pathway
IP3 increase of Ca in the seroplasmic reticulum -> increased intracellular Ca2+ -> contraction
Airway smooth muscle contraction pathway: DAG pathway
DAG -> PKC (protein kinase C) -> contraction
Airway smooth muscle contraction pathway: early pathway in order to get DAG + IP3
Ach -> M3AchR activates Phospholipase C -> PIP2 -> IP3 +DAG
Muscarinic receptors in lung - submucosal glands
M1 and M3
Bronchial secretions
Muscarinic receptors in lung - airway smooth muscle
M3 and M2
bronchoconstriction
Muscarinic receptors in the lung - autoreceptors
M2
M2 are the auto receptors that signal the stop to the M1 and M3 in the submucosal glands and the M2 and M3 in the airway smooth muscle
autoreceptors
signal the presynaptic neuron to stop releasing the neurotransmitter
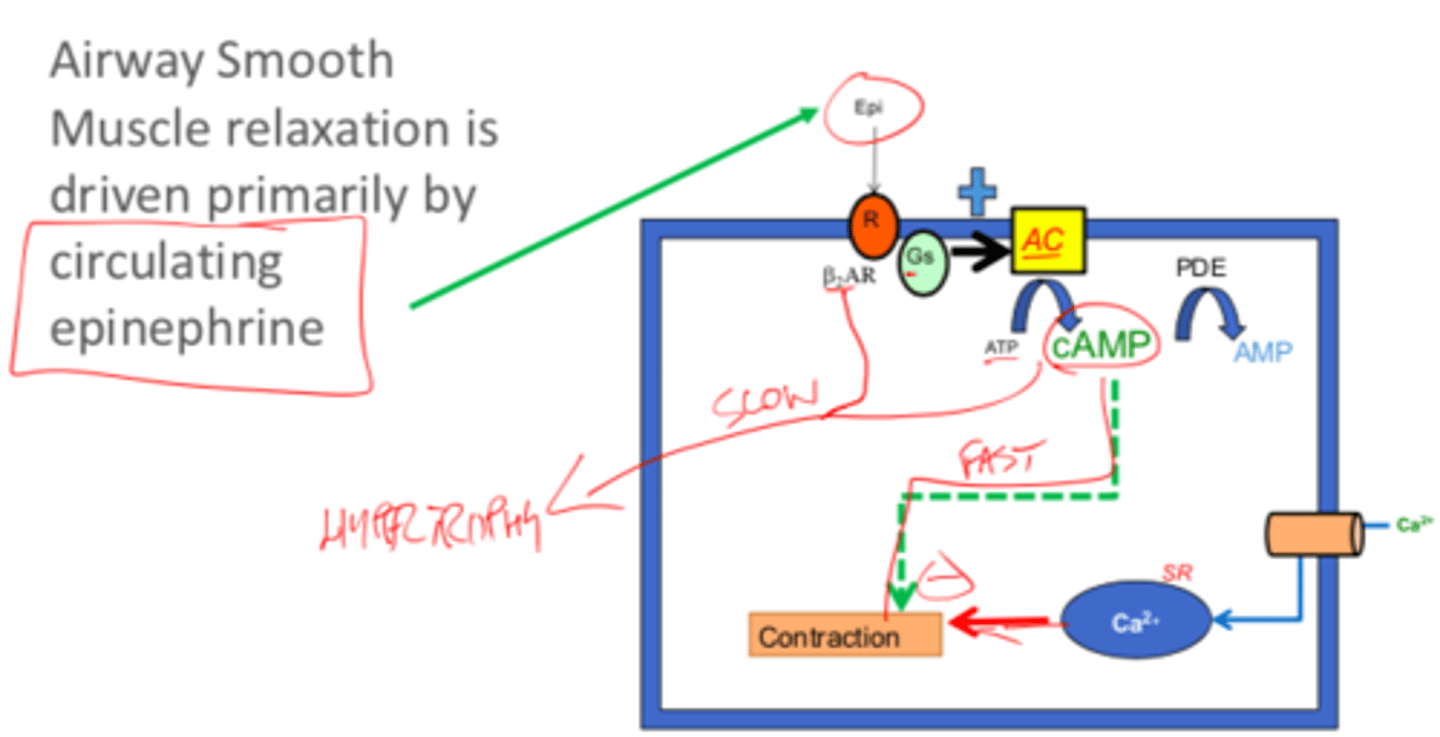
Airway smooth muscle relaxation is primarily driven by _______________ ___________
- circulating epinephrine
Airway smooth muscle innervation (parasympathetic) figure
Airway smooth muscle relaxation figure
Phosphokinase C from DAG in airway smooth muscle innervation / contraction leads to ______________ and __________
- hypertrophy
- (and) hyperplasia
Airway smooth muscle relaxation pathway
Epi -> β2AR -> GS -> adenylate cyclase -> ATP to cAMP -> inhibits contraction (fast response)
Epi -> β2AR -> hypertrophy (slow response); thus the use of β2-agonists long-term still causes hypertrophy despite use of rescue of asthma (not good in the long-run)
Airway smooth muscle relaxation pathway: fast response
Epi -> β2AR -> Gs -> adenylate cyclase -> ATP to cAMP -> inhibits contraction
cAMP via PDE -> AMP
Thus relaxation
Airway smooth muscle relaxation pathway: slow response
Epi -> β2AR -> hypertrophy (slow response)
The use of β2-agonists long-term still causes hypertrophy despite use of rescue of asthma (not good in the long-run)
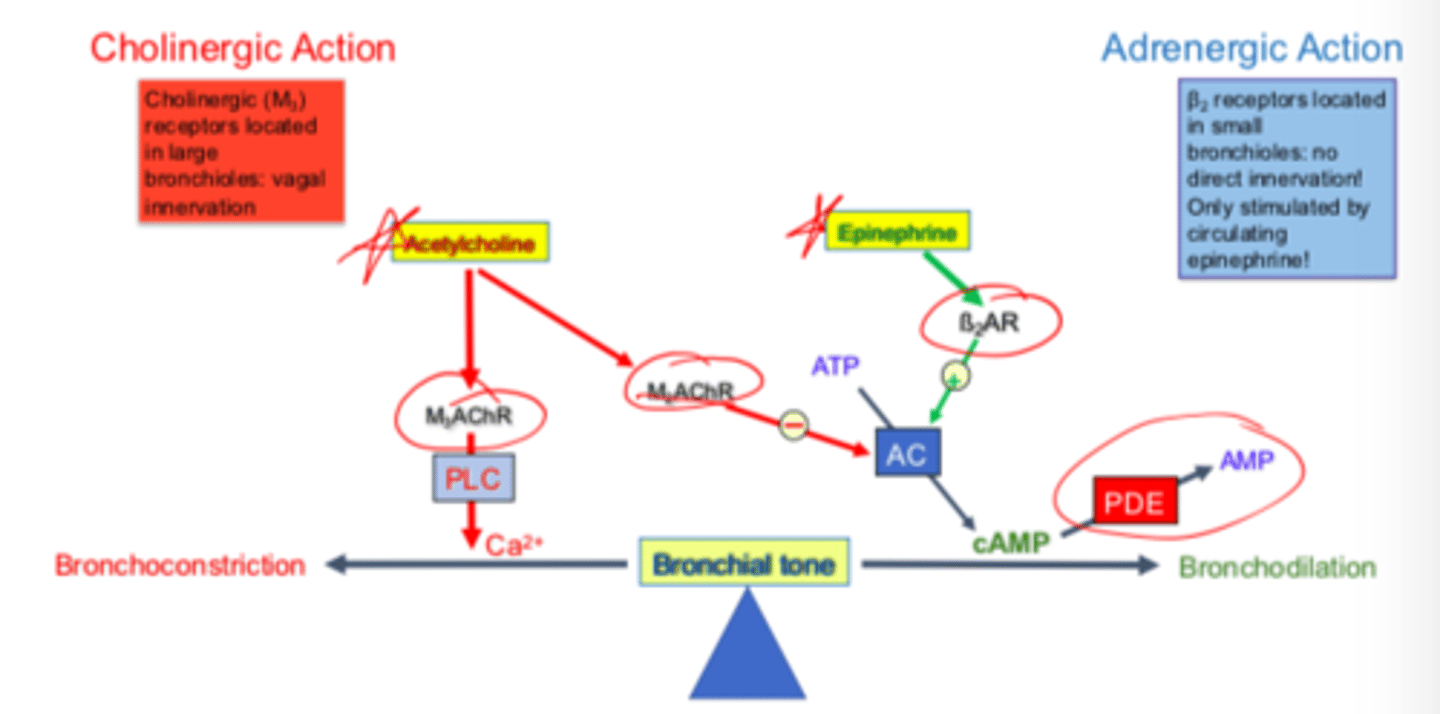
Yin/Yang control of bronchial tone - cholinergic action: cholinergic (_____) receptors located in large bronchioles due to _________ innervation.
This causes ___________
- M3
- vagal (innervation)
- bronchoconstriction
Yin/Yang control of bronchial tone - cholinergic action: acetylcholine innervates M2 receptors and ________________ adenylate cyclase (AC) to ___________ bronchodilation
- inhibits (adenylate cyclase)
- prevent (bronchodilator)
i.e., M3 causes bronchoconstrction; M2 prevents bronchodilation
Yin/Yang control of bronchial tone - adrenergic action: β2 receptors located in _________ bronchioles: ___ ________ innervation; only stimulated by __________ epinephrine
- small (bronchioles)
- no direct (innervation)
- circulating (epinephrine)
Regularly follow-up asthmatic patients every ____ __________
- (every) 3 months
Yin/Yang Control of Bronchial Tone Figure
Asthmatics lose the ____________ between the bronchial tone
- (lose the) balance
Bronchoconstriction is more sensitive
Asthma mechanisms: _____ and ________ _________; Mast cell _______ in exacerbations
- IgE
- mast cells
- mediates (in exacerbations)
Asthma mechanisms: Th2 Inflammatory cytokines in asthma
IL-4
IL-5
IL-13
Asthma mechanisms: basophil
FceRI
FceRI
receptor present in the surface of mast cells, basophils, and activated eosinophils that binds free IgE with very high affinity. When antigen binds to IgE and cross-links FcERI, it causes cellular activation and degranulation
Environment and gene involvement in asthma: _____________ _________ slightly after birth, which may lead to ________ _____________ and _________ development
- maternal exposure
- lung morphogenesis
- immune (development)
KR is now 19 years old and has had a history of asthma for 3 years. She is generally well controlled but has significant flare ups during soccer season and also in the Spring when flowers are blooming. This year, she had a severe upper respiratory tract infection and her recovery time took 2 weeks due to significant wheezing and worsening of her asthma. Previously, she was able to control her asthma quite well when she avoided triggers and could go over a year without any attacks.
What are some respiratory tract changes that KR is experiencing?
Inflammation - increase inflammatory mediators
Increase mucus from the goblet cells
Hypertrophy and hyperplasia of bronchiolar smooth muscles
KR is now 19 years old and has had a history of asthma for 3 years. She is generally well controlled but has significant flare ups during soccer season and also in the Spring when flowers are blooming. This year, she had a severe upper respiratory tract infection and her recovery time took 2 weeks due to significant wheezing and worsening of her asthma. Previously, she was able to control her asthma quite well when she avoided triggers and could go over a year without any attacks.
How would these changes lead to worsening of chronic asthma?
Hypertrophy and hyperplasia occurs due to bronchoconstriction, which leads to a larger and stronger response
Bronchiolar smooth muscle hypertrophy is signaled by _____________ __________ ______
- protein kinase C
DAG
diacylglycerol
Histamine acts similar to _______________ ______ in the activation of asthma
- (similar to) acetylcholine M3
Histamine from Mast Cells triggers PKC and Ca2+ -> bronchoconstrction