PSYC 188 - Midterm #2
1/49
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
50 Terms
Conduct problems
Related to antisocial (goes against society) behavior
Age-inappropriate actions & attitudes that violate family expectations, societal norms & the personal or property rights of others
Asocial = not feeling social
Key features of antisocial behaviors
Some behaviors decrease w/ age (e.g., disobeying at home), talking about small children
Must consider developmental factors in order to prevent clinical bias because some behaviors can be normal as a child develops
Some behaviors increase with age and opportunity (e.g. hanging around kids who get into trouble)
More common in boys during childhood
When is it a disorder?
Psychological Dimensions of Conduct Problems
Destructive x covert
Destroying things, but covert, kind of undercover, not involving other ppl directly
E.g. property violations
Nondestructive x covert
No destruction on property, people, or animals, but destruction to self?
E.g. Substance abuse, swearing, rule breaking
Overt x destructive
Overaggression
E.g. physical assault, fighting, cruelty to animals/people
Overt x nondestructive
Being annoying, defiant, angry
Reactive aggression
Engaging in physical violence in response to a threat, frustrating event, or provocation
Impulsivity/automaticity
No consideration of alternative responses
Mostly seen in younger kids and those with ADHD
Proactive aggression
Deliberately engaging in an aggressive act to obtain a desired goal
Learned through modeling and reinforcement
When positively reinforced…
E.g. pushing a kid in line to get lunch money
When negatively reinforced…
E.g. school suspension to get out of school
E.g. mom tells child to clean board game they threw off table, they get in mom’s face and she says “fine, i’ll put it away”, this is negative reinforcement
Relational Aggression
Purposefully leaving a child out of an activity
Getting mad at someone and excluding him/her from the peer group
Telling lies about a person so others won’t like him/her
Telling others you will not like them unless they do what you say
There’s a stereotype that girls are more likely to do this, but this isn’t backed up by evidence
Oppositional Defiant Disorder
A pattern of angry/irritable mood, argumentative/defiant behavior or vindictiveness lasting at least 6 months as evidenced by at least 4 symptoms from any of the following categories & exhibited during interaction with at least individual who is not a sibling
Why is it important to be 6 months?
Demonstrating that it’s not just them having a tough time at school or not sleeping well, but it’s how they present themselves most of the time
Emphasis on not being like this towards a sibling
ODD Severity
Mild - Symptoms are confined to only setting (e.g., at home, at school, at work, with peers)
Moderate - Some symptoms are present in at least two settings
Severe - Some symptoms are present in three or more settings
ODD: Associated Characteristics
Typically do not regard themselves as angry, oppositional, or defiant
View their behavior as a justified response to unreasonable demands or circumstances
May have a history of hostile parenting; hard to know which came first
ODD: Prevalence, Course, and Comorbidities
3-5%
More prevalent in males (prior to adolescence)
First symptoms usually appear in preschool and rarely later than early adolescence
Often (but not always) precedes the development of conduct disorder
Comorbid with anxiety disorders, major depressive disorder, substance use
Conduct Disorders
A repetitive & persistent pattern of behavior in which the basic rights of others or major age-appropriate societal norms or rules are violated, as manifested by the presence of at least 3 of the following 15 criteria in the past 12 mos. from any of the categories below, with at least one criterion present in the past 6 mos
CD: Childhood-onset type
Individuals show at least one symptom characteristic of conduct disorder prior to age 10 years
CD: Adolescent-onset type
Individuals show no symptoms characteristic of conduct disorder prior to age 10 years
CD: Unspecified onset
Criteria for a diagnosis of conduct disorder are met, but there’s not enough information available to determine whether the onset of the first symptom was before or after age 10 years
CD Severity
Mild: Few if any conduct problems in excess of those required to make the diagnosis are present, & conduct problems cause relatively minor harm to others
Moderate: The number of conduct problems & the effect on others are intermediate between those specified in “mild” & those in “severe”
Severe: Many conduct problems in excess of those required to make the diagnosis are present, or conduct problems cause considerable harm to others
CD: Age of Onset Subtypes
Why limited prosocial emotions (LPE) specifiers?
Those with LPE more likely to have childhood-onset, severe, violent and chronic CD
LPE traits are relatively stable from late childhood to early adolescence
Behavior therapy alone is less effective for those with LPE traits (stimulant medication + behavioral therapy seems to help)
The problems of those with LPE traits are more strongly related to dysfunctional parenting practices
Those with LPE traits show deficits in processing fear and distress signals in others (amygdala hyporeactivity)
LPE traits tend to be more heritable
Reductions in emotional, though not cognitive empathy
CD: Prevalence
5-10% for boys, 2-4% for girls
Prevalence rates rise from childhood to adolescence
More common in boys than in girls
Girls less likely to use physical aggression
Few children with CD receive treatment
Differentially diagnosed in Black and Latino children?
Antisocial Behavior Causes: Neurobiology
Decreased NTs:
Serotonin
Dopamine
Increased hormones
Testosterone
Low levels of autonomic arousal
Under arousal of HPA axis
May explain lack of empathy and emotional reactivity to others
Limited ability to feel fear and guilt
Insensitivity to punishment
Less able to experience pleasure, excitement, and exhilaration
Conduct Problems Causes: Temperamental & Psychosocial
Difficult temperament
High emotion reactivity
Don’t learn effective regulation skills
Parents may have trouble responding sensitively & appropriately
Can compromise parent-child interaction quality
Children may rely on impulsive decision-making
Peer rejection, selective affiliation with deviant peers, deviancy training
Thrill-seeking & recklessness (with CD)
Parents may alternate between overly permissive & hostile & angry disciplinary tactics
One of the best predictors of CD
One of the best predictors of ODD → CD
Parents may feel powerless
Low parental monitoring
Maternal depression, paternal substance abuse
High crime neighborhoods
Antisocial Behavior Causes: Cognitive Behavioral
Rewards for aggression
Hostile attribution bias
See world in scarier lens so that they are ready to defend themselves, quiicker to anger
May perceive and label their own arousal as anger
Focus on positive aspects of aggression and lack of responsiveness to emotional stimuli
Social learning
Modeling new aggressive behaviors, disinhibition of aggression
Reinforcement trap
Giving in to a child’s tantrum
Mother reinforces child’s behavior and reinforces her own behavior
Antisocial behavior treatment: Parent Management Training (PMT)
Teach parents the causes of disruptive behavior problems
Show parents how to attend to and praise appropriate behavior
Parent-child interaction therapy (PCIT)
Parents and children attend therapy together
Parents developing skills: Praising, Reflecting, Imitating, Describing (kind of like narrating what the child is doing), Enthusiasm
Parents create more realistic expectations for children’s behavior
Give effective
Antisocial behavior treatment: Multisystemic treatment (MST)
Targets family, school, and peers
Therapists work in teams of 3-5 and are available to child and family 24/7
Usually lasts 3 months
Family
Help parents effectively interact with and monitor kids
Remove obstacles that interfere
School
Increase parental involvement in education
Remove obstacles to academic achievement
Peers
Limit opportunities for interactions with deviant peers
Increase interactions with prosocial youths/new peer networks
Lowers probability of future offenses and arrests
Only available to ~1% of adolescents with serious conduct problems
Costly, but not as much as incarceration
Intermittent Explosive Disorder
Criterion A. Recurrent (doesn’t have to be everyday, but there is a pattern) behavioral outburst representing a failure to control aggressive impulses as manifested by either of the following:
Verbal aggression or physical aggression occurring twice weekly, on average, for a period of 3 months. Does not result in property damage or physical injury
Three behavioral outbursts involving property damage or physical injury within a 12-month period
Criterion B. Aggressiveness grossly out of (way out of) proportion to the situation
E.g. child with this can lose a game of monopoly and flip over board and start breaking things with it, start to hurt family members (unlike in ODD)
Criterion C. The recurrent aggressive outbursts are not premeditated (i.e., they are impulsive and/or anger-based) and are not committed to achieve some tangible objective (e.g., money, power, intimidation)
People who are pretty easy going and nice to be around a lot of the time, may even be sweet, but if something sets them off, it’s an intense response that is not well-regulated
Diagnostic Criteria – IED
Criterion D. Outbursts cause distress in individual, or impairment in occupational or interpersonal functioning, or are associated with financial or legal consequences
Other people bothered by it, but person is bothered by it as well
Criterion E. Chronological age is at least 6 years (or equivalent developmental level)
Criterion F. The recurrent aggressive outbursts are not better explained by another mental disorder, medical condition, or substance use
IED is …
Rare condition
Characterized by frequent aggressive outbursts
Leads to injury and/or destruction of property
Few controlled treatment studies
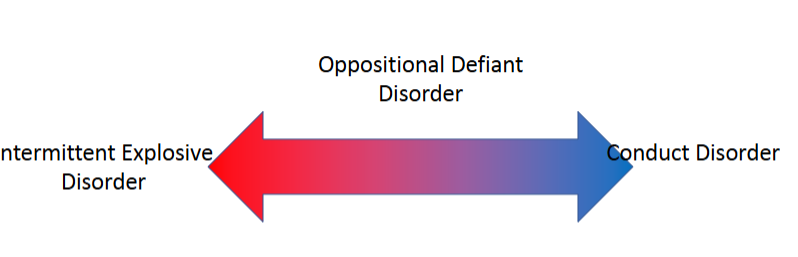
Difference between IED, ODD, & CD
IED is most consistent with emotional dysregulation
Conduct disorder is most consistent with behavioral dysregulation
ODD is somewhere in the middle
IED Assessment
Keep in mind any other comorbidities: multiple psychiatric diagnoses
Conduct disorders (ODD/IED/CD) often cluster together with:
ADHD
Mood disorders
Anxiety
SUDs
Comorbid diagnoses tend to predict poorer outcomes
Unfortunately, it’s rarely “one thing” – can make diagnosis and treatment planning rather complicated
Distinguishing between conduct disorders
ODD does involve…
Emotion regulation problems (ODD, IED)
Conflict with authority (ODD, CD)
More likely in CD than ODD
Significant physical aggression
Significant destruction of property
Pattern of theft and deceit
More likely IED than ODD
Serious aggression
Pyromania - Background
Terminology
Fire-setting: behavior of setting a fire
Arson: criminal act of intentional fire-setting
Pyromania: a psychiatric disorder of which intentional-fire setting is a symptom but no sufficient for diagnosis
Pyromania - History
Has been described in medical reports for at least 200 years
Name derives from greek fire (pyr) & madness (mania)
Validity has been debated over time, but it remains scarcely researched
First appeared in DSM in 1952 as a supplemental item, then re-emerged in DSM-III in 1980 as an impulse-control disorder
Pyromania’s Diagnosis
Deliberate and purposeful fire setting on more than one occasion
Tension or affective (emotional) arousal before the act
Fascination with, interest in, curiosity about, or attraction to fire and its situational contexts (e.g., paraphernalia, uses, consequences)
Pleasure, gratification, or relief when setting fires or when witnessing or participating in their aftermath
The fire setting is not done for monetary gain, as an expression of sociopolitical ideology, to conceal criminal activity, to express anger or vengeance, to improve one’s living circumstances, in response to a delusion or hallucination, or as a result of impaired judgement (e.g., in major neurocognitive disorder, intellectual disability [intellectual developmental disorder], substance intoxication)
The fire setting is not better explained by conduct disorder, a manic episode, or antisocial personality disorder
Diagnosis: Pyromaniac fire-setting as an aesthetic behavior?
Aesthetic behavior
Behavior that has no clear extrinsic reward but is intrinsically rewarding to perform
Fire as an aesthetic stimulus
People with pyromania in a study said the fire was like an “amalgam of elements, some of which interact synergetically”
Fire destroys and cleanses, it humanizes but also demonizes
Fire interacts and transforms elements in its environment
Personal speculative theory:
A person with pyromania has an unusually increased aesthetic response to fire?
Pyromania’s Diagnosis – Associated characteristics
May make considerable advance preparations for starting a fire
It’s their plan for the day to cause fire and experience the fire
Population prevalence of pyromania is unknown, but lifetime prevalence of fire setting is 1/13%
Diagnoses in just 3% of arsonists
Little etiological and treatment research
Pyromania’s Diagnosis - Development & Course
Limited info
Although 40% of arson arrests are in those younger than 18yo, pyromania in childhood appears to be rare
Juvenile fire-setting is usually associated with conduct disorder, ADHD, or an adjustment disorder
Pyromania’s Differential Diagnosis
Must rule out other causes
Rule out other gain related to fire-setting
Fire-setting behavior in the context of other disorders
Must consider other common comorbidities
Substance use disorders
Gambling disorders
Depressive disorders
Bipolar disorders
Other disruptive, impulse-control, & conduct-disorders
Treatment - Tarasoff warning
“…a psychotherapist has a duty to protect or warn a third party only if the therapist actually believed or predicted that the patient posed a serious risk of inflicting serious bodily injury upon a reasonably identifiable victim.”
Tarasoff v. Regents of the University of California
A patient confided to his therapist of direct intent to kill an identifiable victim (Tatianna Tarasoff)
Therapist alerted campus police of the patient’s intent, but not the victim
The patient murdered the victim after being released from police custody
Treatment - Medication & CBT
Some medication have shown promise in case studies
CBT may reduce behavior as urge increases
Kleptomania
DSM diagnosis (since DSM-3)
Failure to resist urge to steal unnecessary items
Seems rare, but it is not well studied
Highly comorbid with mood disorders
Als0 co-occurs with substance-related problems
Kleptomania: DSM-5 Criteria
Recurrent failure to resist impulses to steal objects that are not needed for personal use or for their monetary value
Increasing sense of tension immediately before committing the theft
Pleasure, gratification, or relief at the time of committing the theft
The stealing is not committed to express anger or vengeance & is not in response to a delusion or a hallucination
The stealing is not better explained by conduct disorder, a manic episode, or antisocial personality disorder
Kleptomania: Associated Characteristics
Estimates are difficulty to establish, but seems very rare
Ration of females to males is estimated as 3:1 (White upper -and upper-middle class women, more specifically)
Onset most commonly in adolescence
Can be episodic in course but occur across long periods
Kleptomania: Risk & Prognostic Factors
May be associated with family history of OCD, & Alcohol Use Disorder
Neurotransmitter pathways associated with behavioral addictions, appear to play a role in kleptomania
May affect legal, family, career in negative way
Assessment of Kleptomania: Differential Diagnosis
Differential Diagnostic Considerations:
Nor “ordinary” theft or shoplifting
Malingering
Antisocial Personality Disorder
Manic episodes, psychotic episodes, and major neurocognitive disorder
Comorbidities
Compulsive buying
Depressive and bipolar disorders
Anxiety disorders
Eating disorders (especially bulimia nervosa)
Personality disorders
SUDs (especially alcohol)
Other disruptive, impulse-control, & conduct disorders
Cognitive-Behavioral Treatment of Kleptomania
Kleptomania can be conceptualized as a set of unwanted behaviors which are the result of operant and respondent conditioning, shaping, behavioral chaining, distorted cognitions & impoverished coping skills
Functional assessment of stealing behavior
Cognitions related to shame can be addressed
Comorbid psychiatric conditions can be treated with CBT, as well