Peds/OB 4.1: Pediatric Cardiology
1/55
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
56 Terms
Are innocent heart murmurs caused by structural heart disease? How common are they?
No, are due to turbulent blood flow; ~50% of children will have one at some point during childhood
What is a pulmonary flow murmur & how can it be characterized?
Turbulent flow through a normal pulmonary valve; systolic mid-frequency murmur heard best at the mid-upper LSB; louder when patient supine
What is a Stills murmur & how can it be characterized?
Turbulent flow in the LV outflow tract; mid-systolic musical/vibratory heard best at the lower LSB; louder supine, may disappear w/ Valsalva, softer during inspiration
What is a venous hum murmur & how can it be characterized?
Turbulent flow in jugular veins & SVC; continuous high-frequency murmur heard best w/ the diaphragm at the infra- & supraclavicular areas & base of the neck; only heard sitting or standing & can be altered w/ position changes of the head or compression of the jugular vein
How long is a patent ductus arteriosus considered to be a benign heart murmur?
Only for the first 48 hours of life - after this the ductus arteriosus should be closed & this murmur is considered pathologic!
What are the only 2 cyanotic congenital heart disorders?
Teratology of Fallot, transposition of the great arteries
What direction does blood flow in the noncyanotic congenital heart disorders? When do they tend to present?
Blood moves from left to right; tend to present in childhood or early adulthood
What direction does blood flow in the cyanotic congenital heart disorders? When do they tend to present?
Blood moves from right to left; tends to present in infancy or early childhood
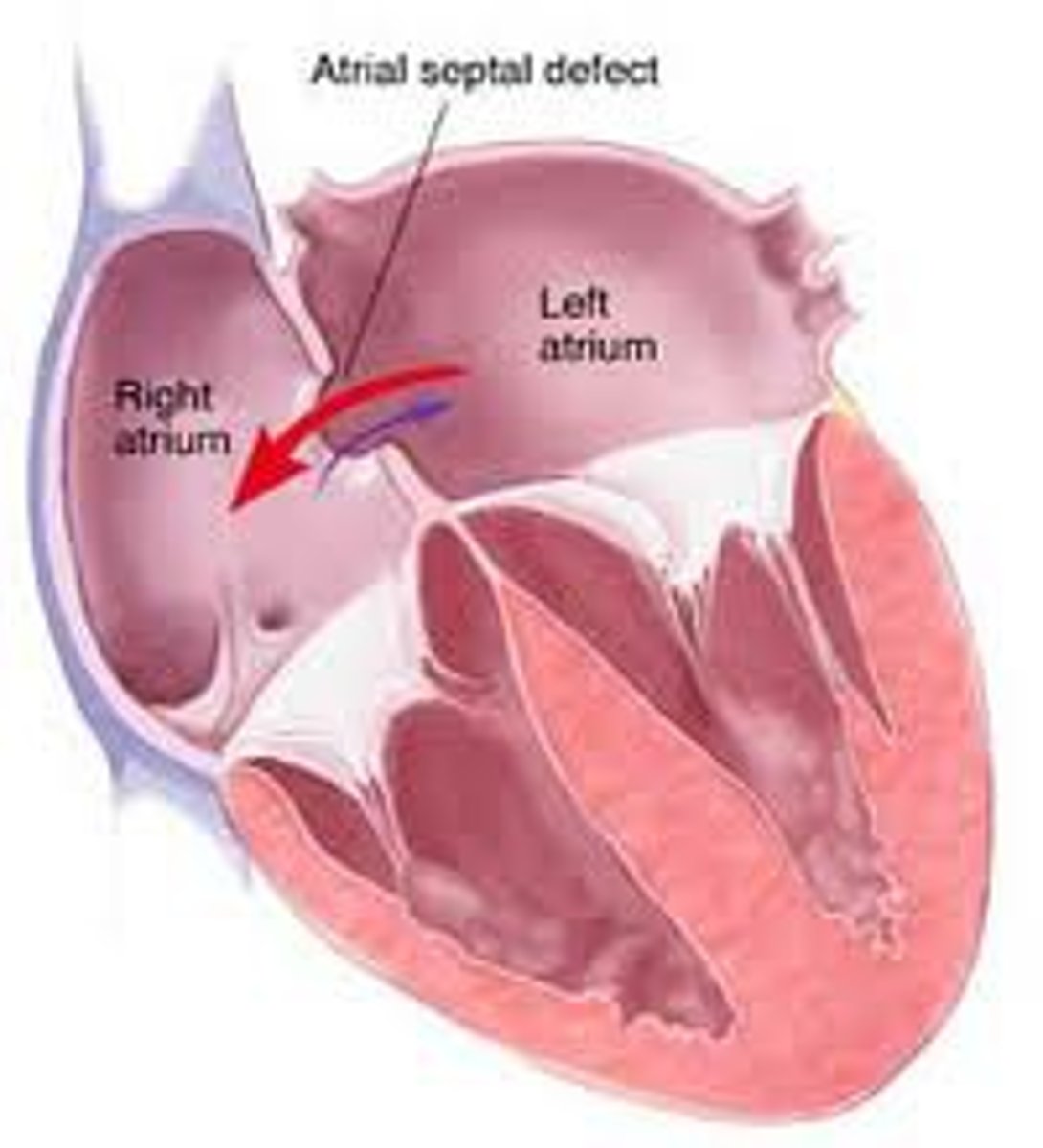
In general, what is an atrial septal defect (ASD)?
Non-cyanotic congenital heart condition where there is an abnormal defect in the wall between the two atria (L → R blood shunt)
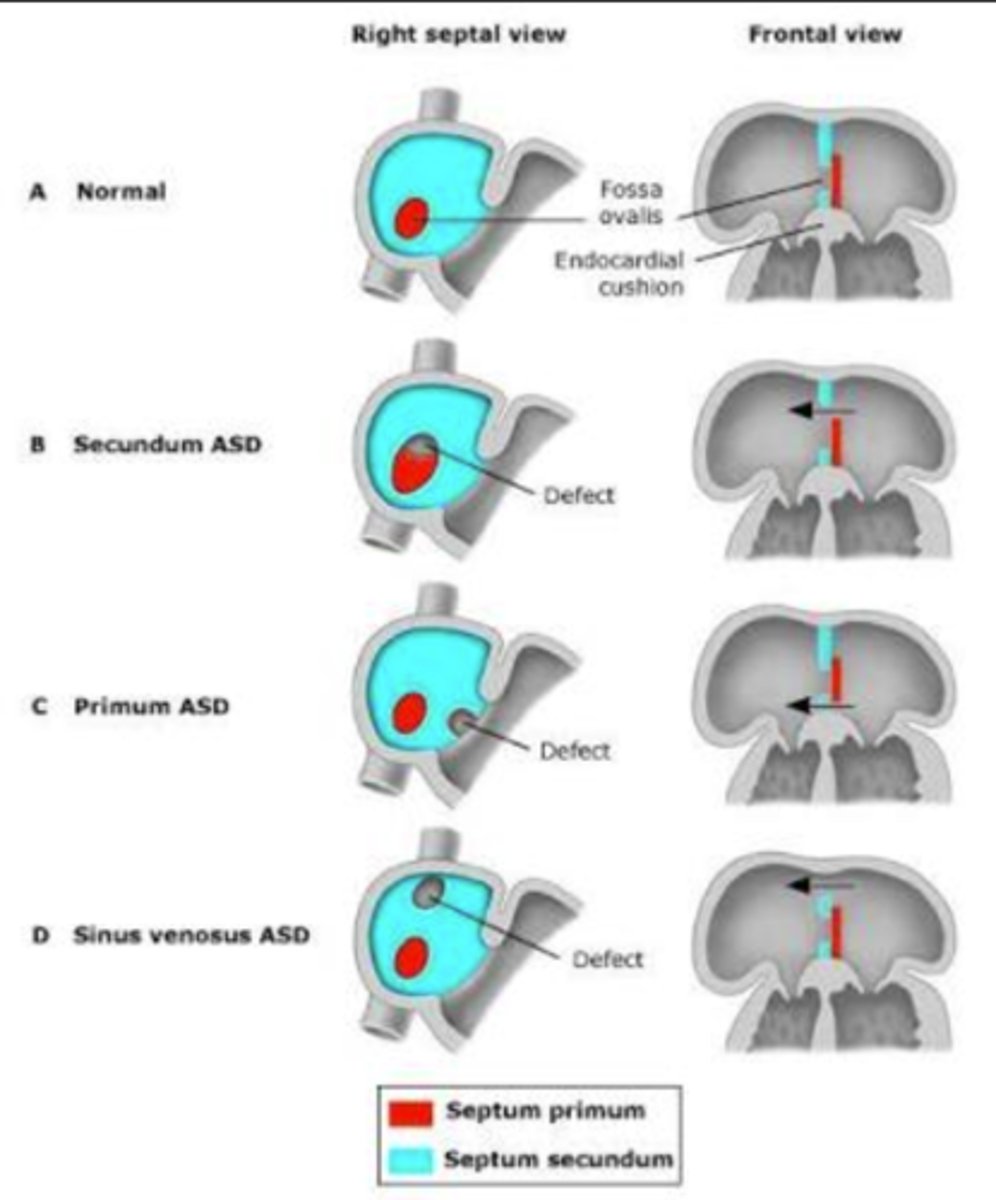
What is the difference between ostium primum, ostium secundum, & sinus venosus ASD? Which one is the most common?
Primum: defect in lower portion of the atrial septum
Secundum: defect in the middle portion of the atrial septum (most common)
Sinus Venosus: defect in the high septum near the SVC
What condition is ostium primum often associated with?
Down syndrome
What are some s/sxs of an ASD? What is the murmur like?
Patient often has a hx of frequent colds & productive cough (because there's more fluid (blood) going into lungs); systolic, heard best around the mid-upper LSB w/ a widely-split S2
What is the best initial test to diagnose an ASD? Is treatment always needed?
Echocardiogram; no - often a very minor defect that rarely needs treatment
What is a potential complication of ASD that warrants surgical closure regardless of the patient's sxs?
Fluid overload & subsequent right-sided hypertrophy/right axis deviation (can progress to pulmonary HTN)
What is a serious potential complication of a patent foramen ovale (similar condition to ASD but not exactly the same)? What is a potential sign of this?
A paradoxical embolus (clot that started on the right like normal but passed through the PFO to the left) cryptogenic stroke before age 55 (cryptogenic = unknown origin)
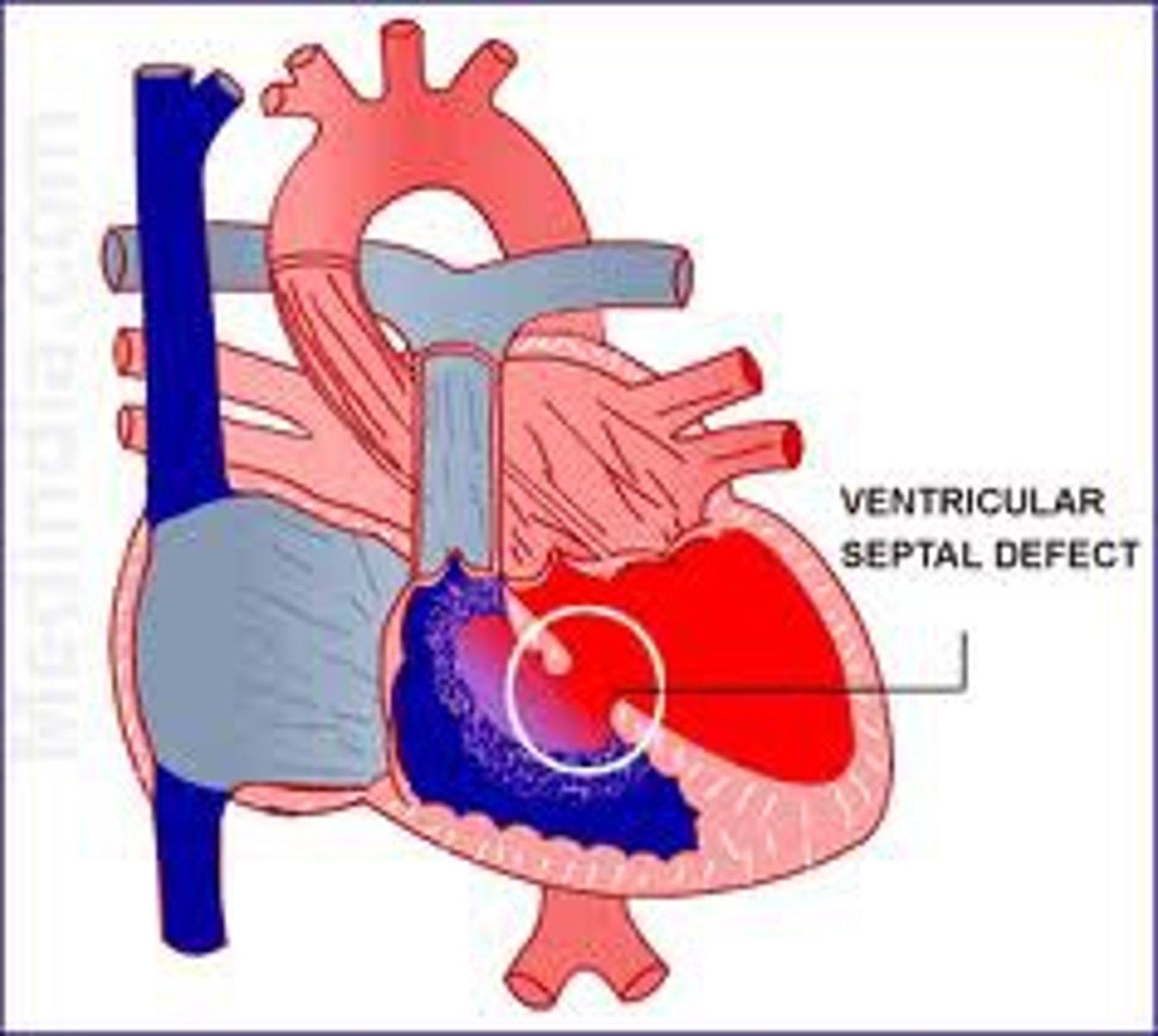
In general, what is a ventricular septal defect (VSD)? How common is it?
Non-cyanotic congenital heart defect where there is an abnormal defect in the ventricular septum (L → R blood shunt) ; most common congenital heart defect overall
What are some s/sxs of a VSD? What is the murmur like?
Non-cyanotic infant with FTT, tachypnea, & sweating (sxs worse during feeding); systolic at the upper LSB
What is the best initial test to diagnose a VSD? Does this condition require treatment?
Echocardiogram; yes - this one tends to be more significant than ASD since more blood is shunted & requires surgical closure (preferably by 3-6 mos to prevent FTT)
How does the murmur of a VSD change depending on its size?
Inverse relationship - the larger the defect, the quieter the murmur (but the more symptomatic the patient will become)
What is the most significant possible complication of untreated VSD?
Pulmonary HTN (is irreversible even after surgical closure)
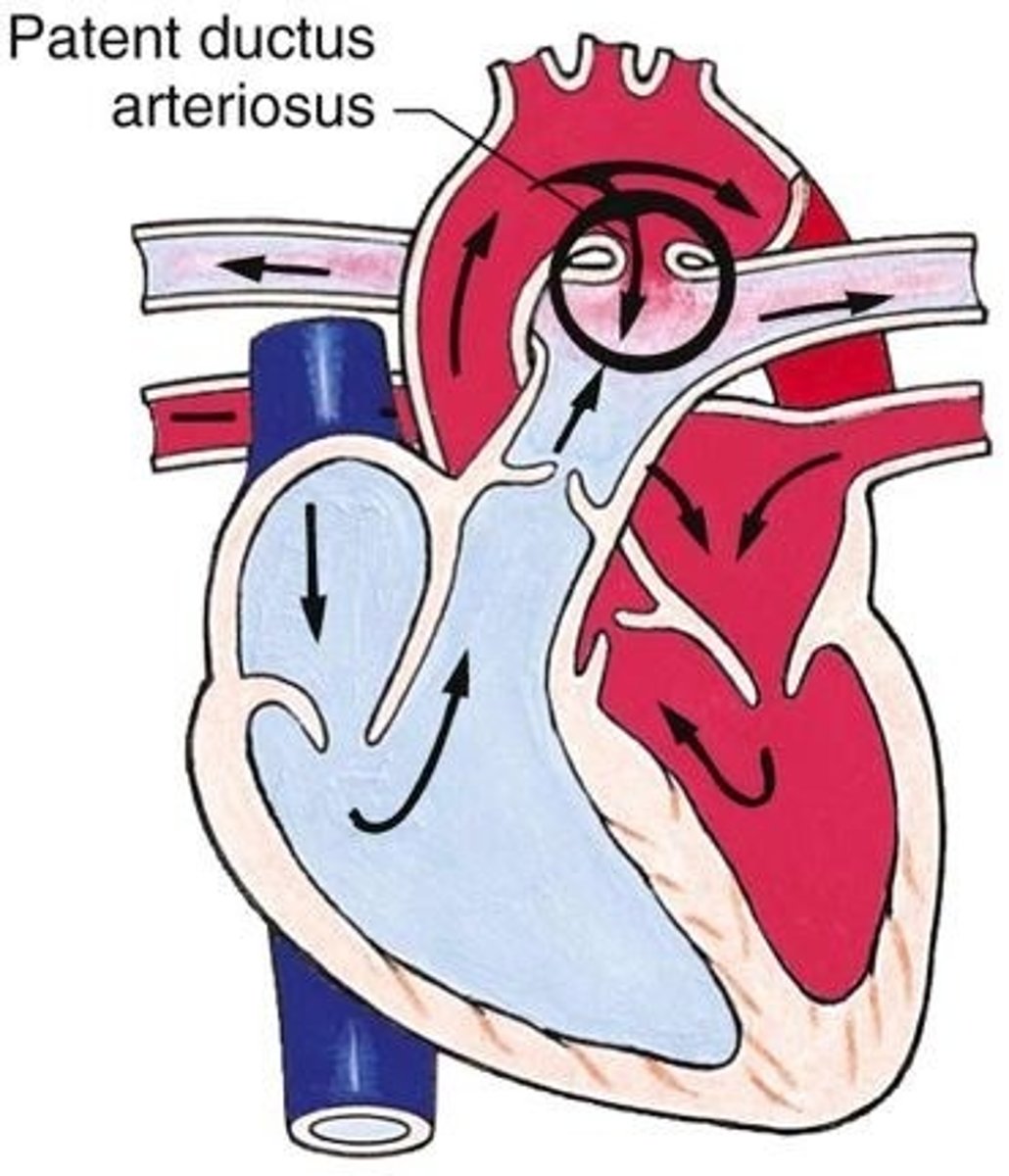
In general, what is a patent ductus arteriosus (PDA)?
Non-cyanotic congenital heart defect in which the ductus arteriosus fails to close completely resulting in blood shunting from the descending aorta to the pulmonary artery
How can the murmur of a PDA be characterized?
Continuous "machinery-like" heard best at the upper LSB
What is the best initial test to diagnose a PDA? What is the preferred initial treatment?
Echocardiogram; indomethacin (an NSAID that facilitates its closure - this is why we normally avoid these in pregnancy); surgery is done if indomethacin is ineffective
In general, what is coarctation of the aorta? Although this is more common in males, what condition is this often associated with in female patients?
Non-cyanotic congenital heart defect characterized by narrowing of the aortic arch usually in the proximal descending aorta; Turner syndrome (45, XO)
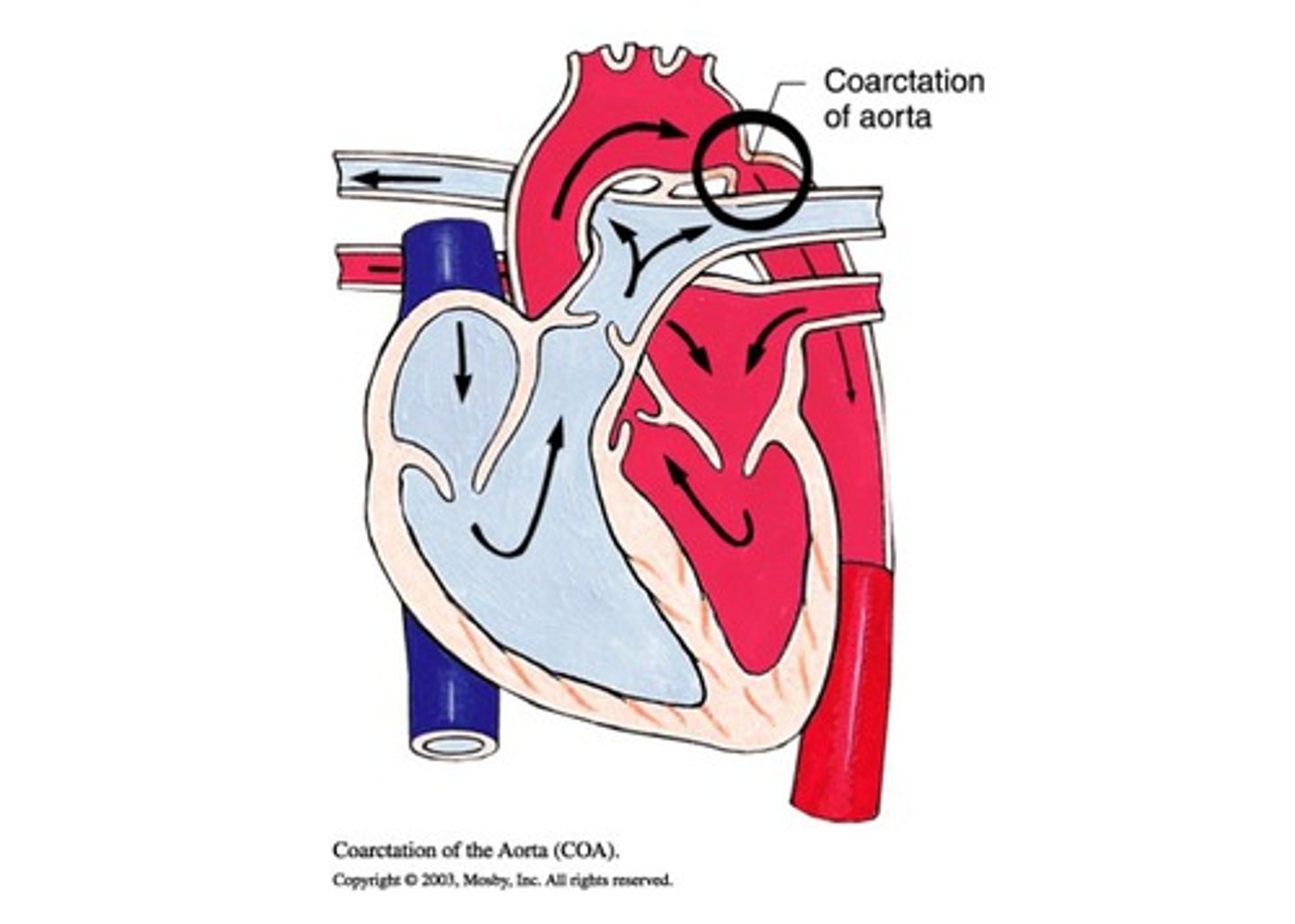
What are some s/sxs of coarctation of the aorta? What is the murmur like?
Cardiogenic shock & LA if in infants or HTN, claudication, & FTT if in childhood, decreased femoral pulses & BP gradient between the arms & legs; blowing systolic murmur in the left upper back or axilla
What is the best initial treatment for coarctation of the aorta? How is it treated?
Echocardiogram (CXR also often done); IV prostaglandin E (exact opposite effect of indomethacin: keeps ductus arteriosus open), inotropic meds to stabilize, & corrective surgery
JUST KNOW: when giving prostaglandin E in coarctation of the aorta, the patient will also require respiratory support because prostaglandins can cause apnea
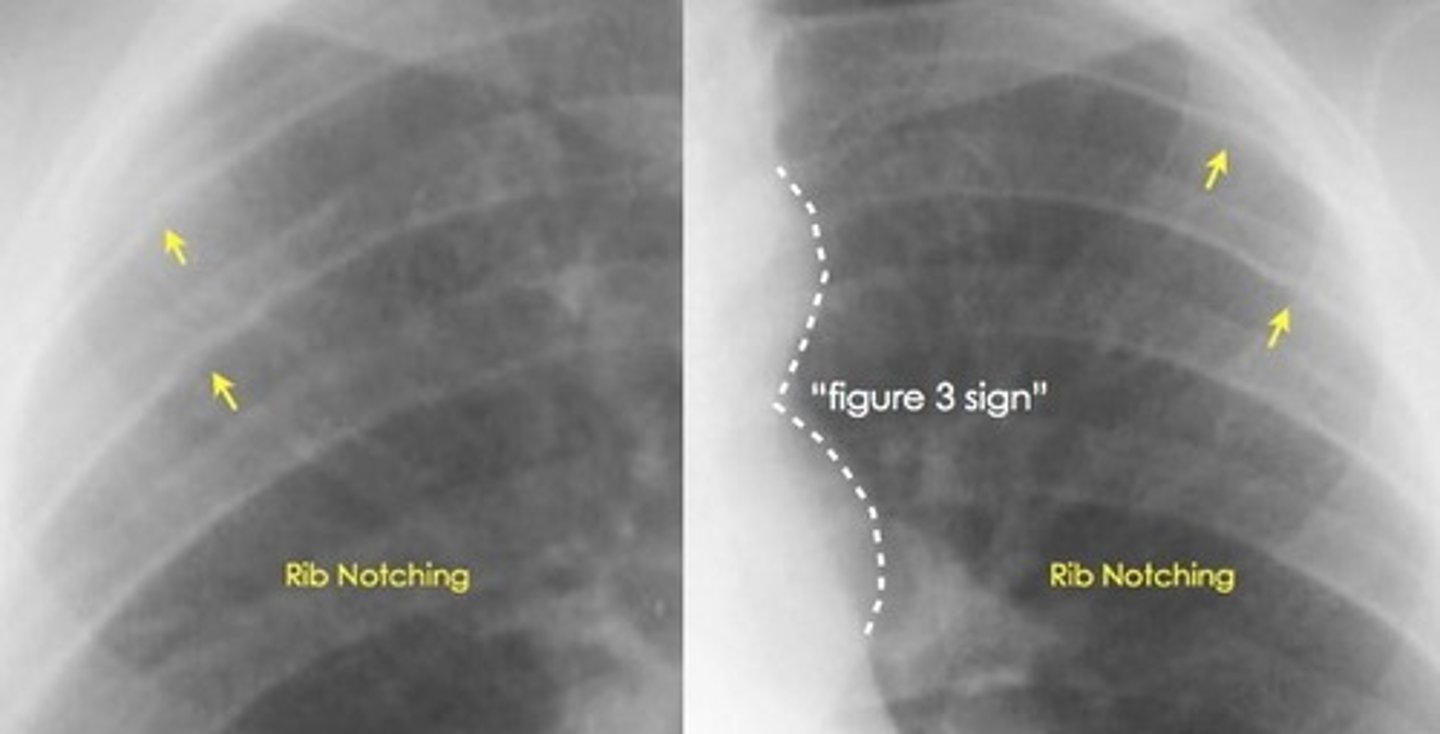
What are 2 characteristic CXR signs of coarctation of the aorta?
Figure 3 sign; inferior notching of the ribs
In general, what is aortic stenosis?
Non-cyanotic congenital heart defect characterized by narrowing of the aortic valve
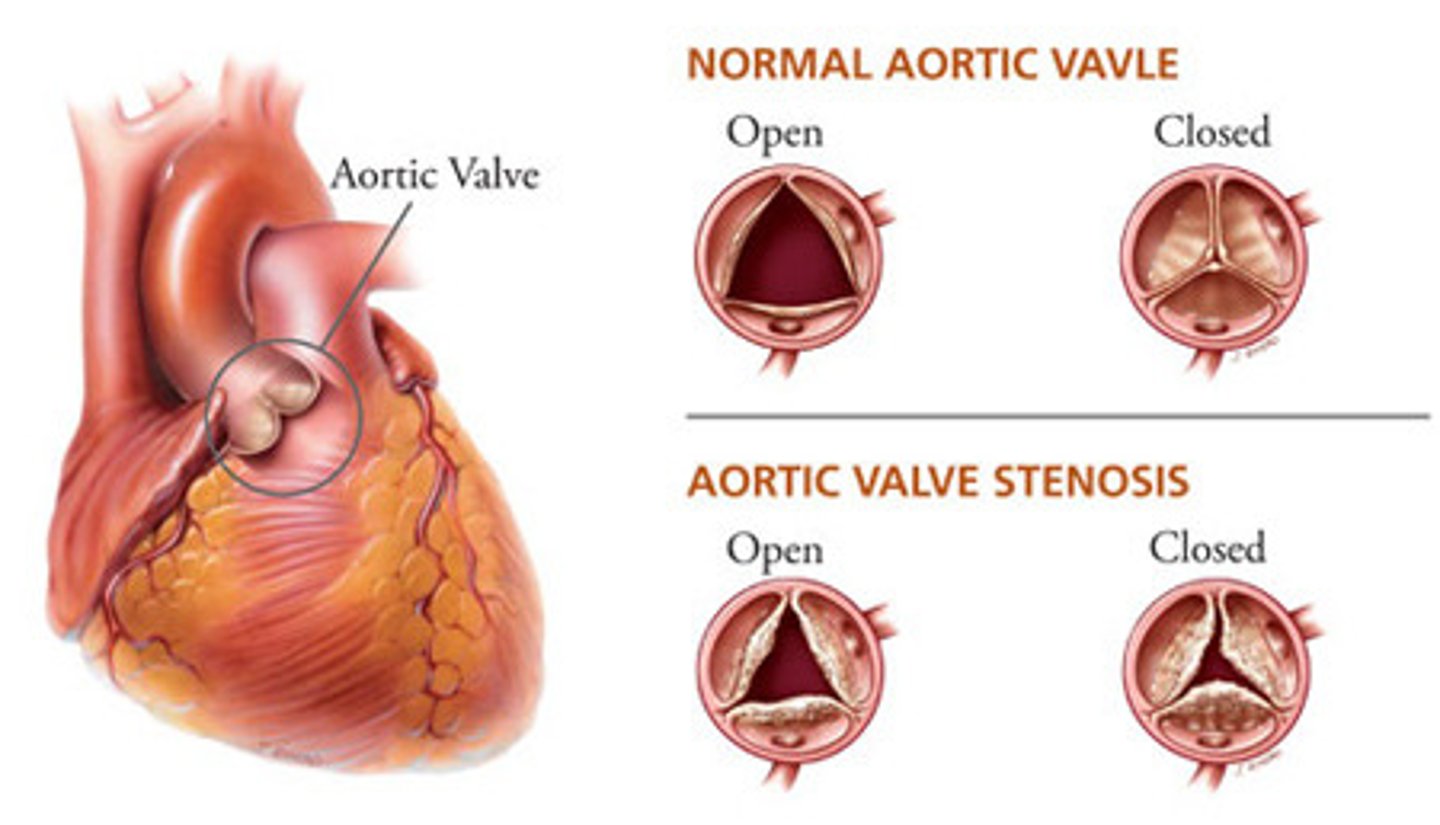
How does aortic stenosis usually present? What is the murmur like?
Usually as a neonate w/ CHF within the first 12-24 hrs of life; harsh systolic ejection murmur heard best at the upper RSB w/ radiation to the neck
What is the best initial test to diagnose aortic stenosis? How is this treated?
Echocardiogram; prostaglandin E until surgery can be done, balloon valvuloplasty is gold-standard
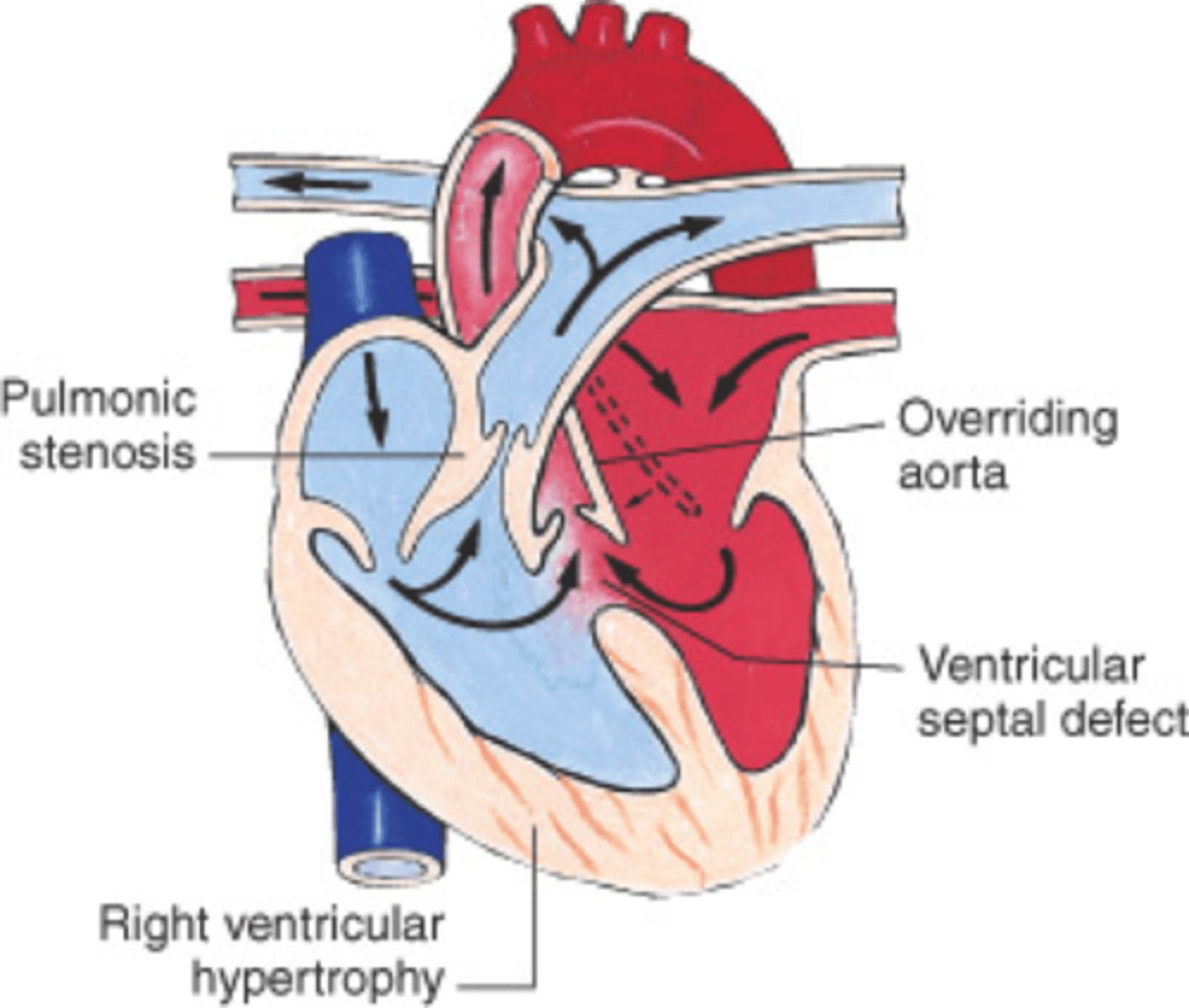
In general, what is Tetralogy of Fallot?
Cyanotic congenital heart defect characterized by 4 main defects: a VSD, overriding aorta, RV hypertrophy, & pulmonary stenosis
What are some s/sxs of Tetralogy of Fallot? Why is this condition significant?
Signs of chronic cyanosis (ex. clubbing of fingers), FTT, "Tet spells" (patient becomes cyanotic & dizzy while walking, relieved by squatting); it is the most common cause of central cyanosis
What is the best initial test to diagnose Tetralogy of Fallot? How is it treated?
Echocardiogram (CXR also often done); prompt surgical repair
How does Tetralogy of Fallot appear on CXR?
As a "boot-shaped deformity"

What are some things that exacerbate sxs of Tetralogy of Fallot? What are some things that relieve it?
Exacerbate: ↑ RVOT, ↓ SVR (exercise, vasodilation, volume depletion, etc.)
Relieve: ↓ RVOT, ↑ SVR (crying, vasoconstriction, tachycardia, etc.)
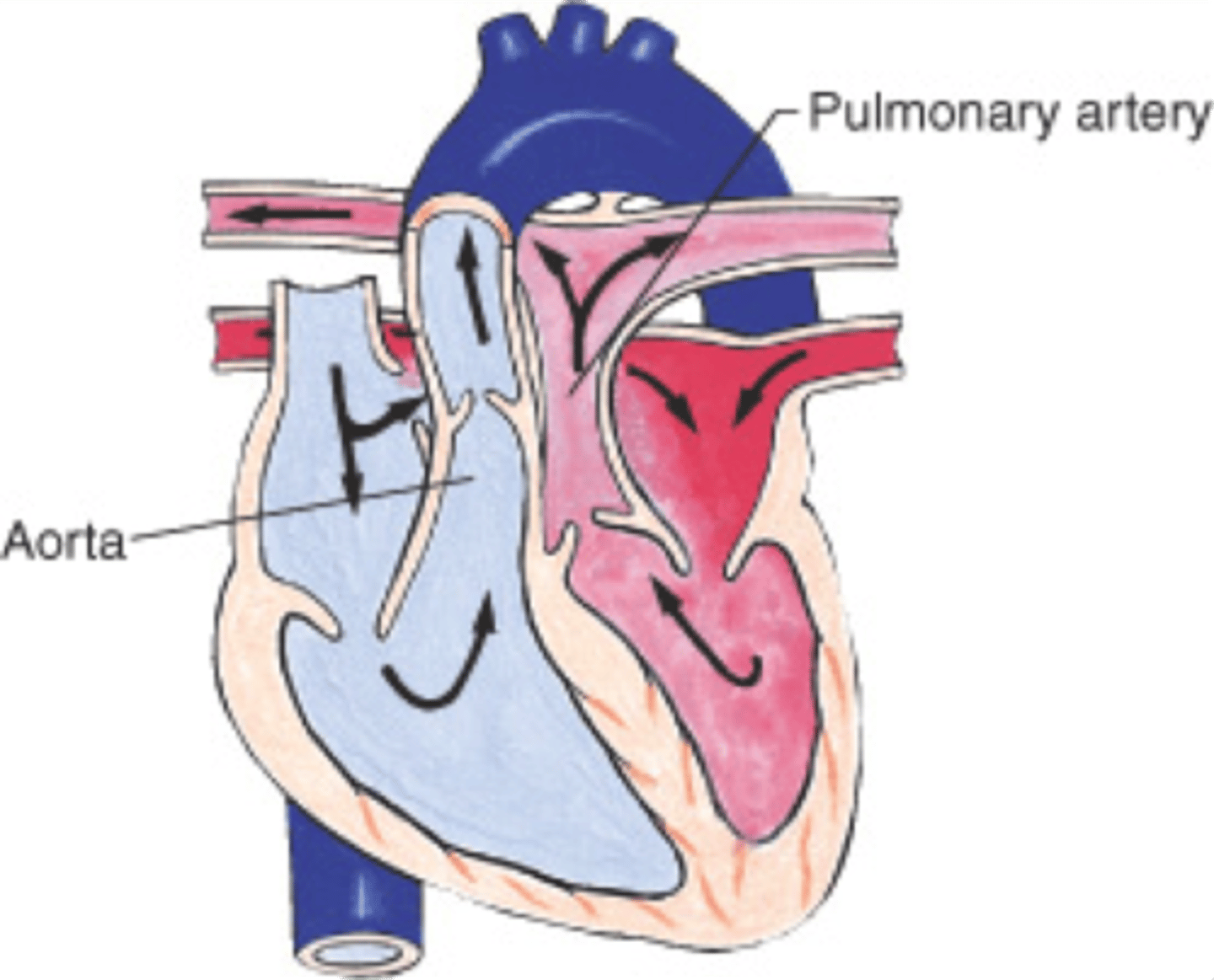
In general, what is transposition of the great arteries (TGA)? Why is this condition significant?
Cyanotic congenital heart defect where the aorta communicates w/ the RV, while the pulmonary trunk communicates w/ the LV; it is incompatible with life!!
What are some s/sxs of TGA?
Progressively-worsening cyanosis, pallor, pulmonary edema, tachypnea, tachycardia, & a loud S2 within the first 48 hrs of life - these babies will be extremely sick & very cyanotic
What is the best initial test to diagnose TGA? How is this treated?
Echocardiogram; best initial is prostaglandin E1 (praying they have a PDA open to get some oxygenated blood to the periphery, & this med will keep it open if they do) followed by corrective surgery ASAP
In general, what is hypoplastic left heart syndrome (HPLS)? What valvular abnormalities are often seen with it?
Underdevelopment of the LV & left-sided heart structures; stenosis/atresia of the mitral & aortic valves
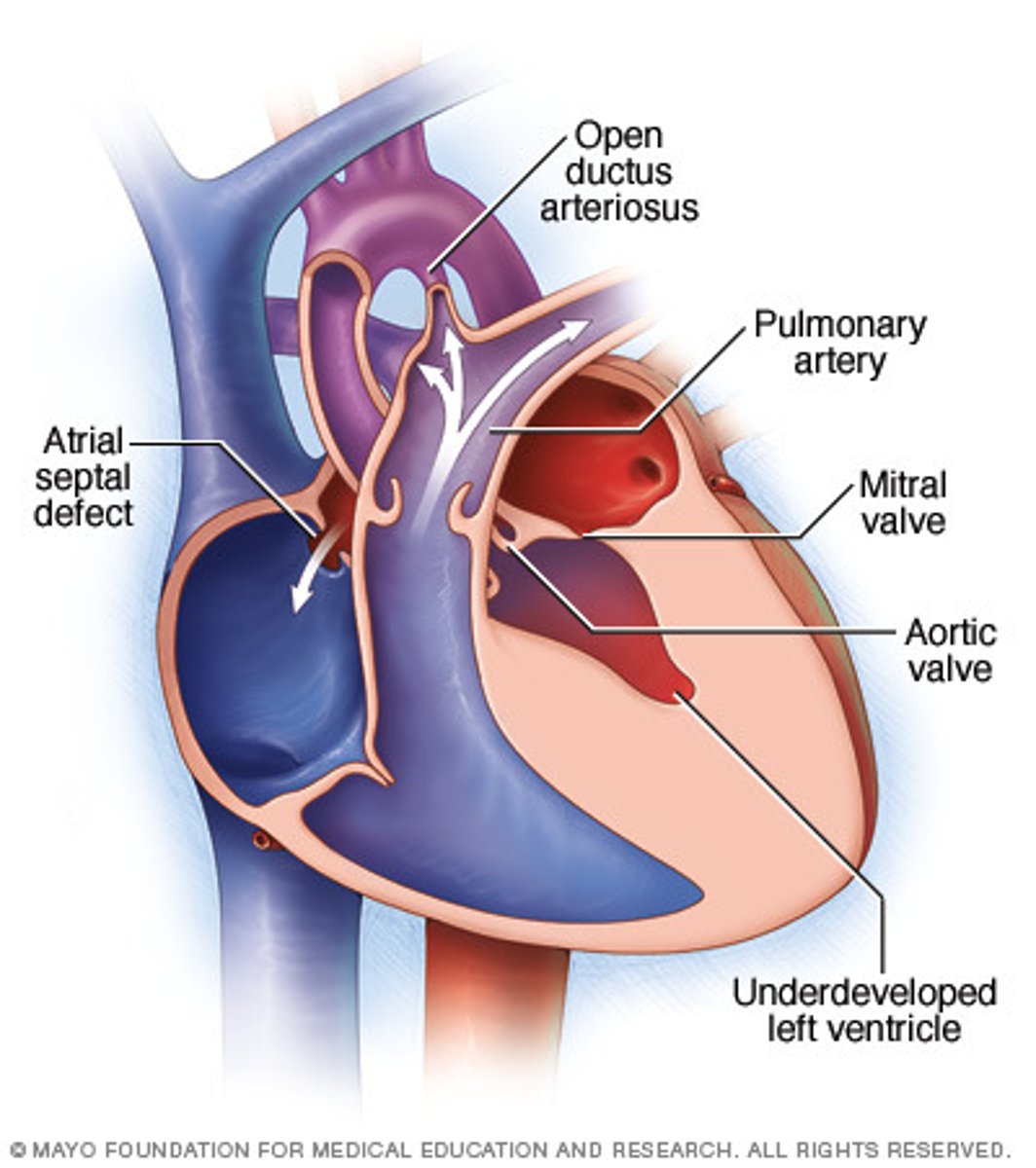
How does HLHS often present?
Neonate initially stable due to PDA but declines rapidly once it closes (death common in 1st WOL); pulses may be absent, single S2 of increasing intensity, gray/pale skin, development of shock
What is the best initial test to diagnose HLHS? How is this treated?
Echocardiogram (often found during prenatal fetal echo); initiate prostaglandin E1 (keep PDA open), avoid O2 supplementation, & perform 3-step surgery
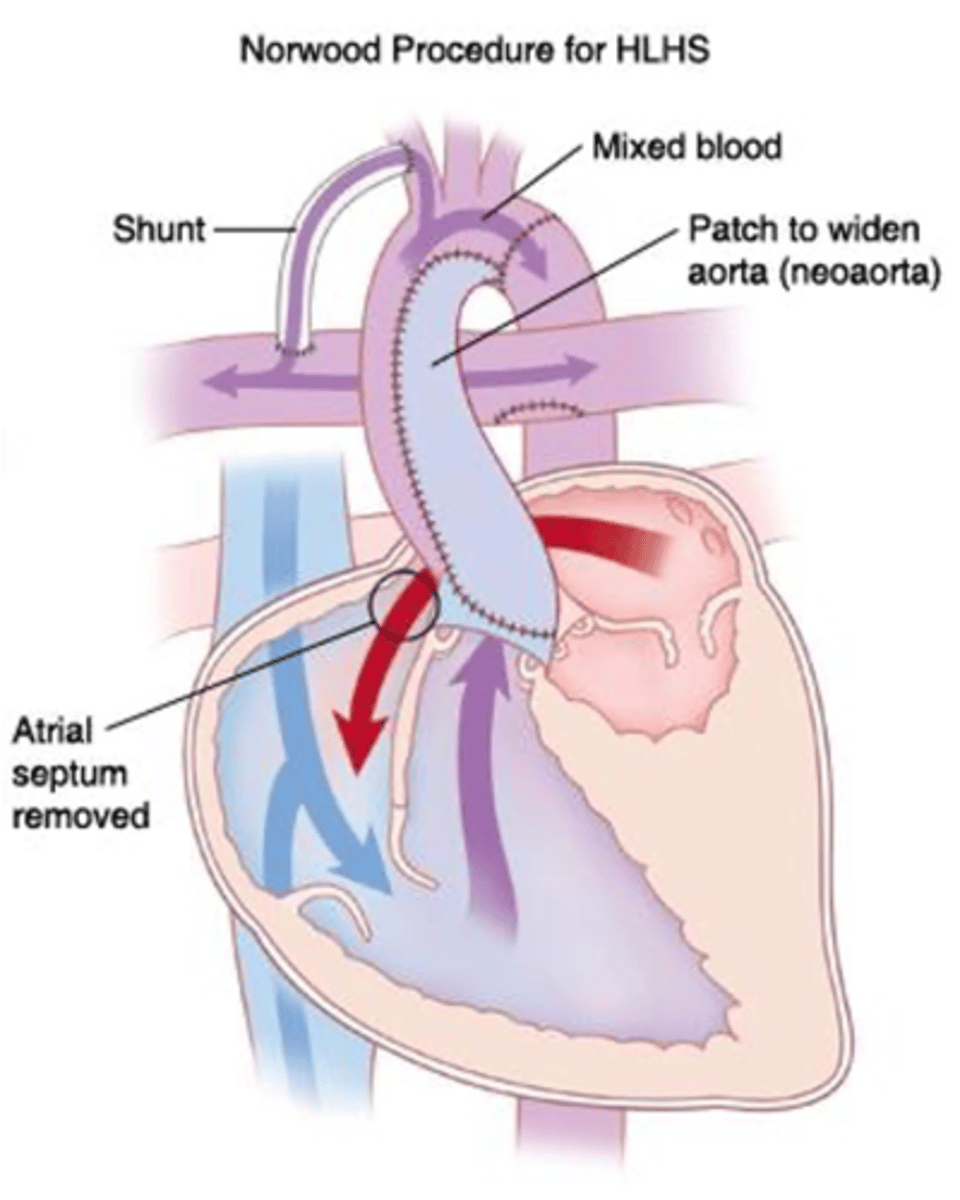
What is the Norwood procedure, & what happens in it?
1st stage of HLHS correction; pulmonary trunk is cut & used to thicken the aorta & attach it to the RV. This provides blood flow to the body but leaves the pulmonary arteries "floating in space." This is fixed by placing a shunt from the subclavian artery to the pulmonary arteries, restoring blood flow to the lungs
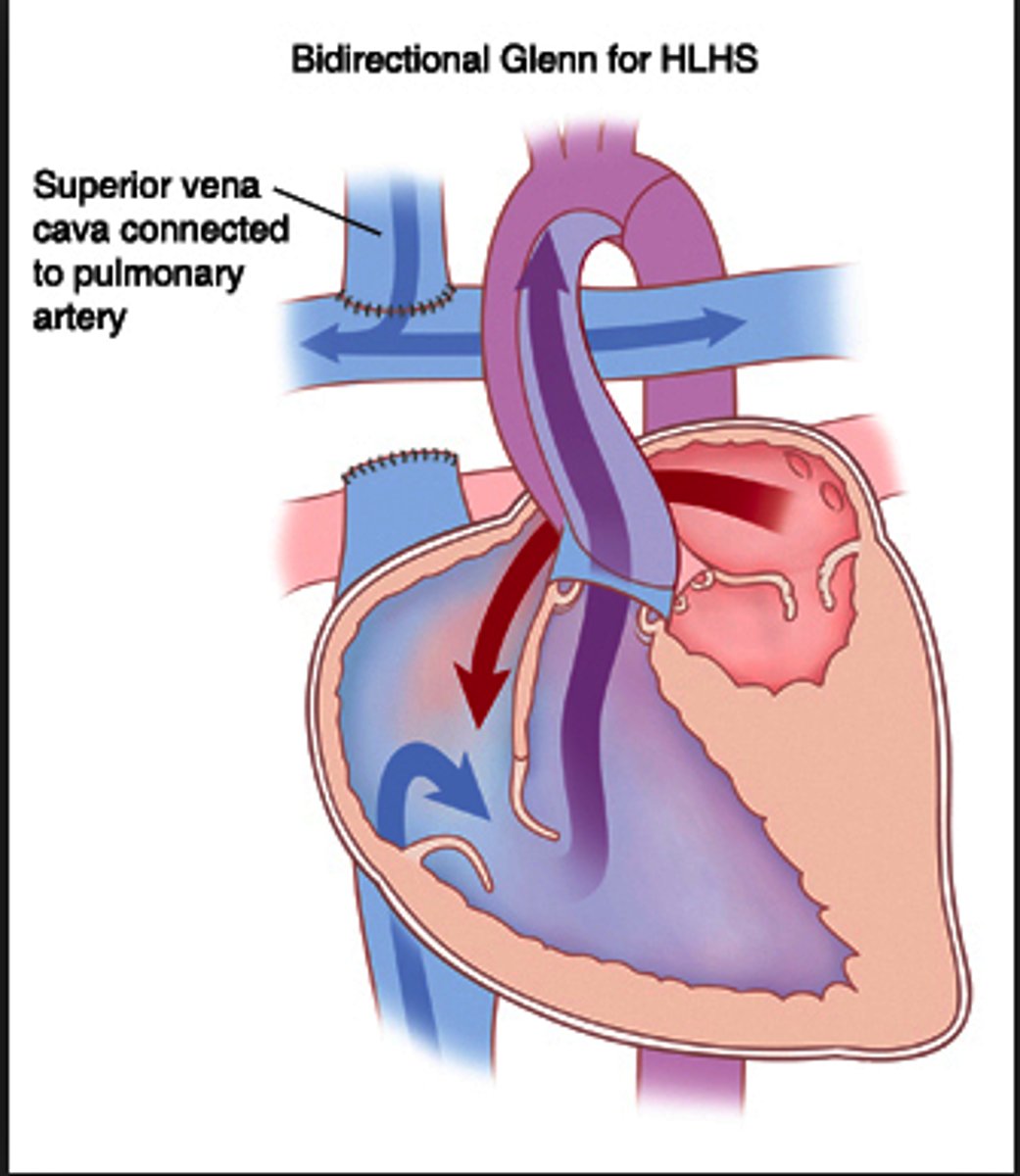
What is the Glenn procedure, & what happens in it?
2nd stage of HLHS correction; the SVC is cut and attached directly to the pulmonary arteries and the shunt is removed. This results in the pulmonary arteries receiving deoxygenated blood directly from the SVC
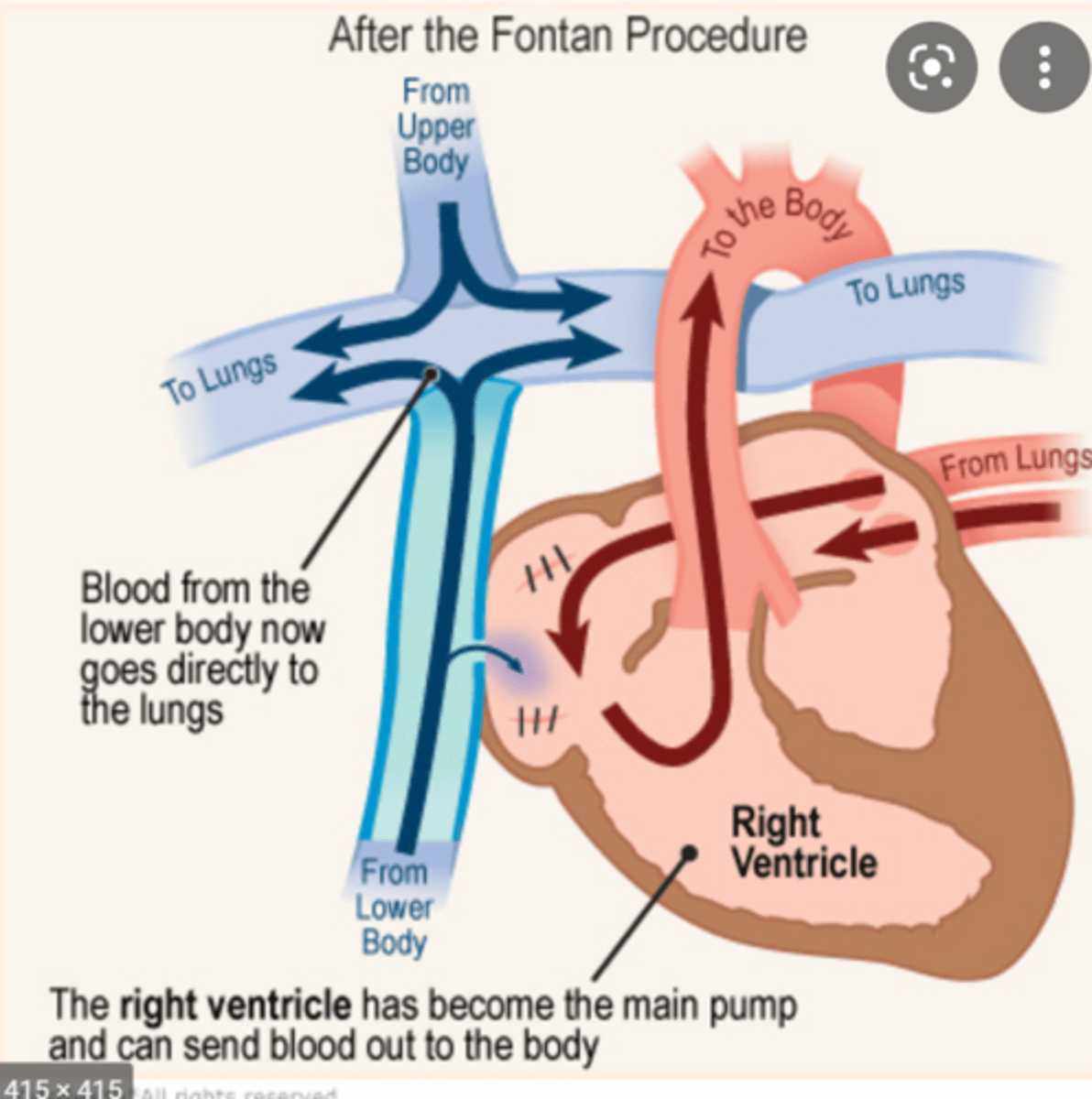
What is the Fontan procedure, & what happens in it?
3rd stage of HLHS correction; the IVC is connected to the pulmonary arteries. This closes the circuit & results in only deoxygenated blood travelling to the lungs & only oxygenated blood travelling to the body
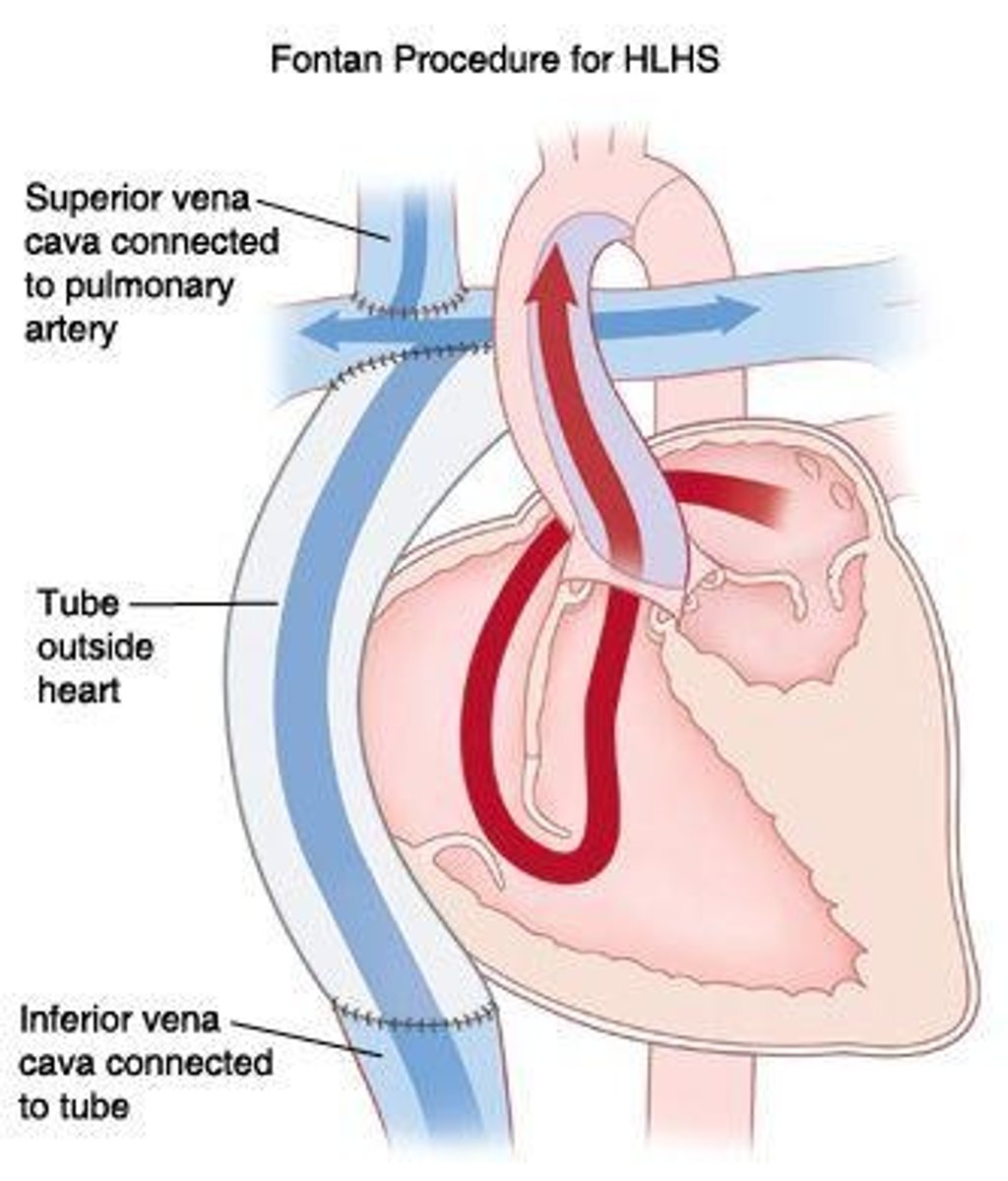
JUST KNOW: the Norwood-Glenn-Fontan procedure to correct HLHS relies on an ASD being open to allow blood returning from the the lungs via the pulmonary veins to the LA to cross over the septum back to the right side of the heart
In general, what is Kawasaki disease? Who is it most common in and why is it clinically-significant?
Acute febrile vasculitis of unknown origin; 80% of patients are < 5 y/o & male (3:2); it is the most common cause of acquired heart disease
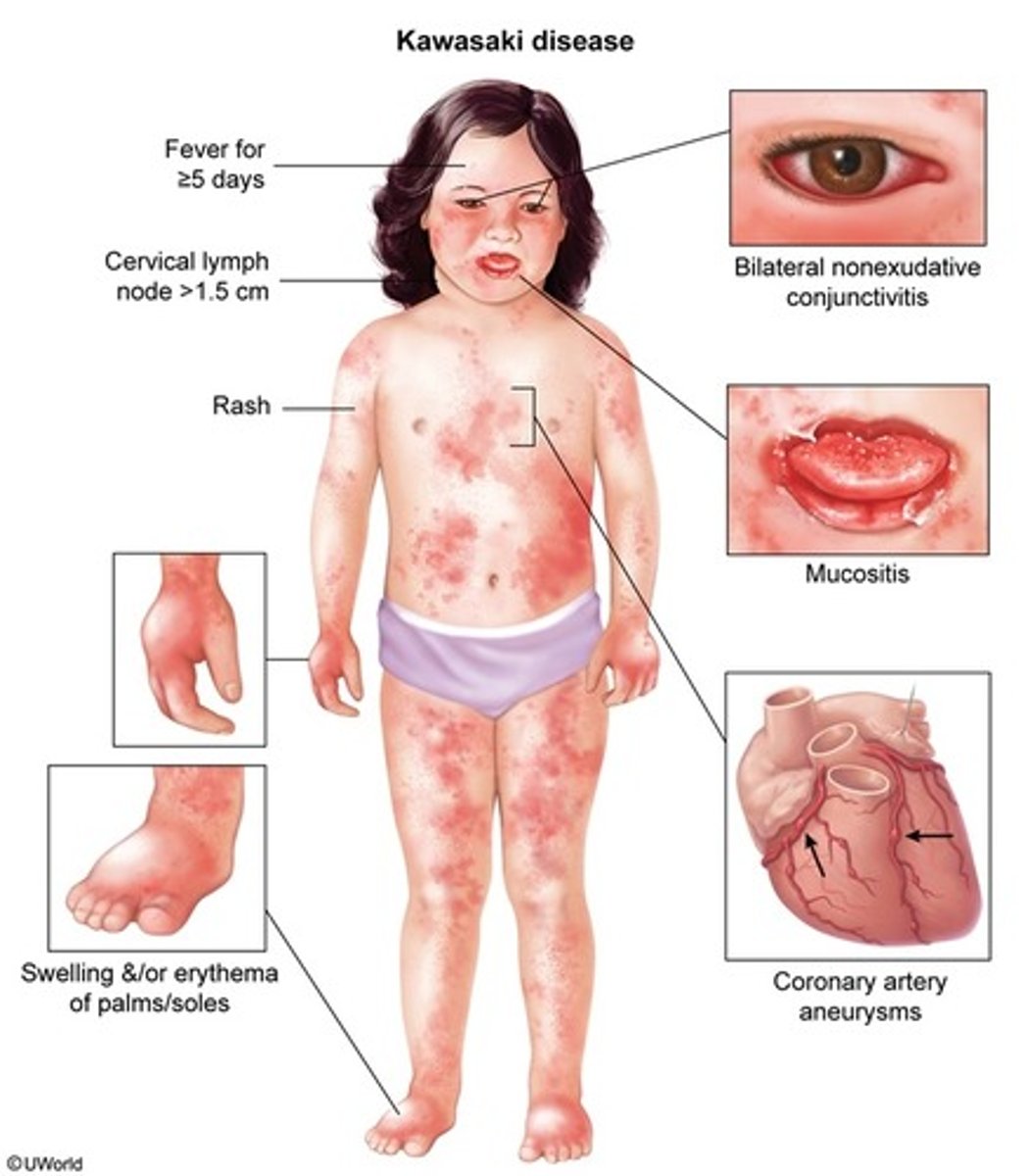
What is the diagnostic criteria for Kawasaki disease?
Fever (> 102F) for > 5 days PLUS 4/5 criteria:
- b/l, painless, nonexudative conjunctivitis
- oropharyngeal changes (red cracked swollen lips, strawberry tongue)
- unilateral cervical LAD > 1.5 cm
- rash
- extremity changes (hand/foot erythema, swelling, etc.)
What is the "Crash & Burn" mnemonic used for?
Can help identify the criteria of Kawasaki disease:
C: conjunctivitis
R: rash
A: adenopathy
S: strawberry tongue
H: hand/foot changes
Burn: high fever
What is the most significant possible complication of Kawasaki disease?
Coronary artery aneurysms
How is Kawasaki disease diagnosed? How is it treated?
Diagnosis: labs such as ESR, CRP, platelets, etc.; based on clinical diagnostic criteria & exclusion of all other conditions
Treatment: evaluate for CAD via echocardiogram, anti-inflammatory therapy (IVIg, ASA)
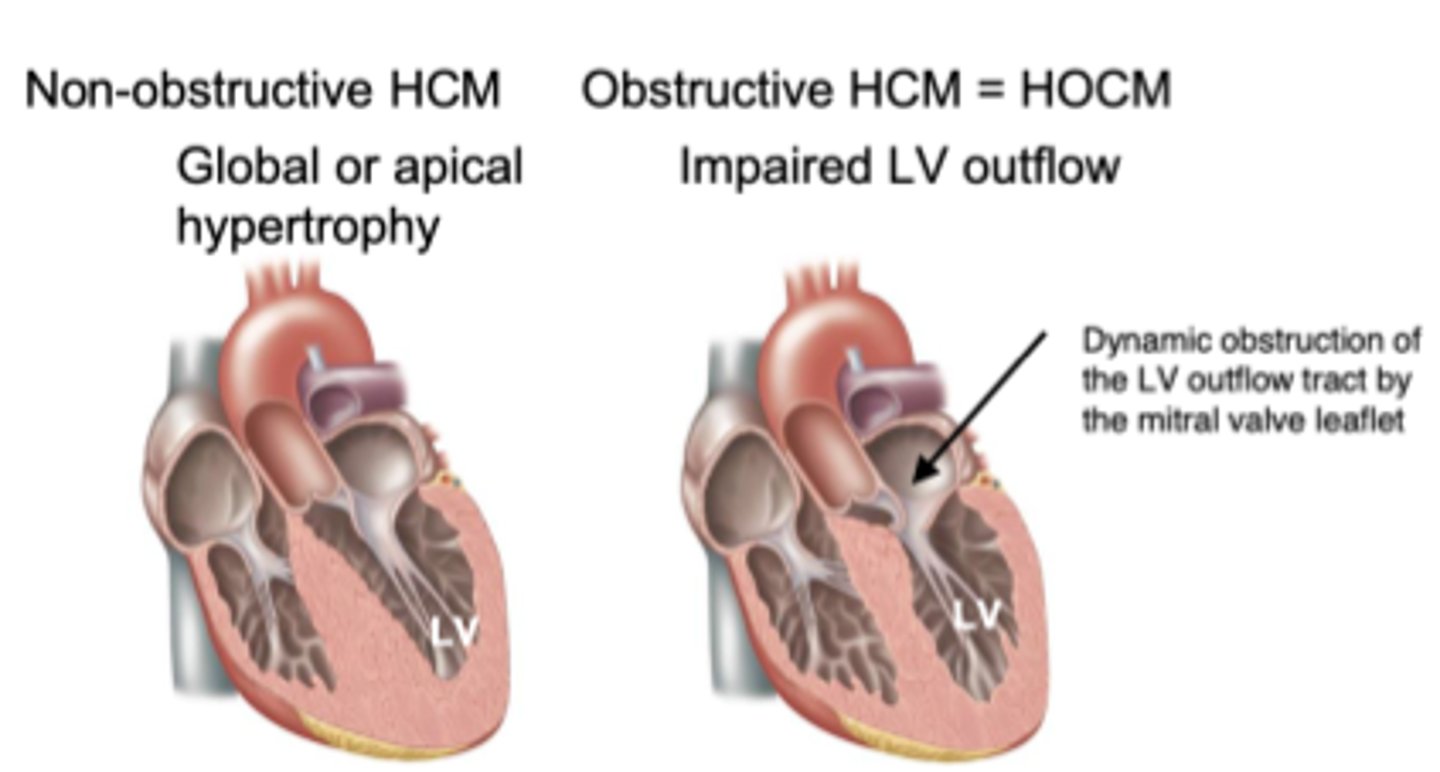
In general, what is hypertrophic obstructive cardiomyopathy (HOCM)? How does it usually present?
Similar to hypertrophic cardiomyopathy, but in this case there is a blockage of the LV outflow tract leading to ↓ peripheral perfusion; often as syncope, but may present as chest pain or sudden death as well
What is the murmur of HOCM like?
Presents similar to aortic stenosis (systolic crescendo-decrescendo at upper RSB) but worsens with anything that reduces LV volume
What are some things that decrease LV volume (& subsequently worsen HOCM)?
Preload reduction (hypovolemia, tachycardia, Valsalva, arrhythmias), afterload reduction (positive inotropes, beta agonists, nitrates, ACEi)
How is HOCM diagnosed? How is it treated?
Diagnosis: echocardiogram (asymmetric wall thickness)
Treatment: beta-blockers mainstay, CCBs, negative inotropes, antiarrhythmics, hydration, avoid strenuous activity, surgery if refractory)
If a patient requires surgery on a congenital heart defect (regardless of the type), what is something we ALWAYS need to give them before the procedure?
Prophylactic ABX (prevents infective endocarditis)