Irritable Bowel Syndrome and Chronic Constipation
1/27
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
28 Terms
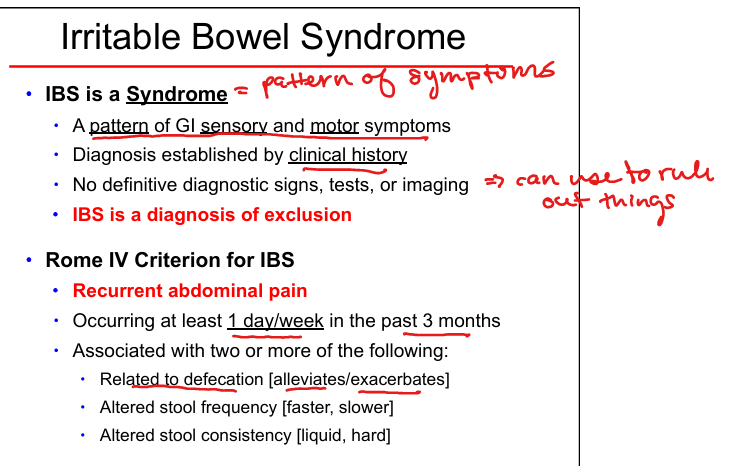
Irritable Bowel Syndrome definition
Syndrome of GI sensory + motor dysfunction; diagnosis of exclusion.
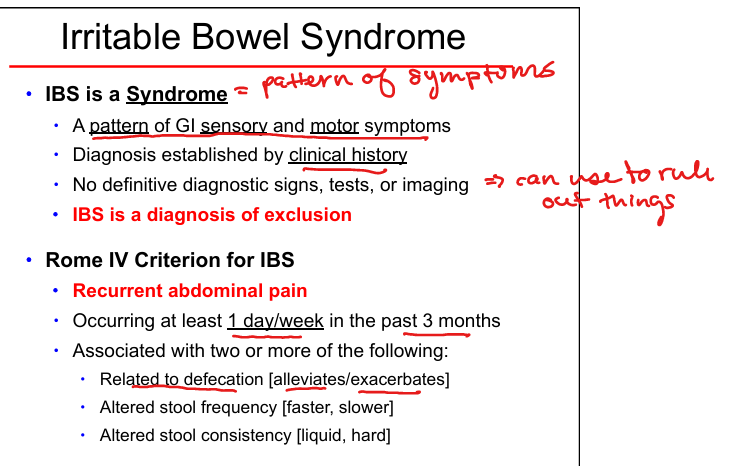
Rome IV criteria for IBS
Recurrent abdominal pain ≥1 day/week for 3 months + 2 of: related to defecation, altered stool frequency, altered stool form.
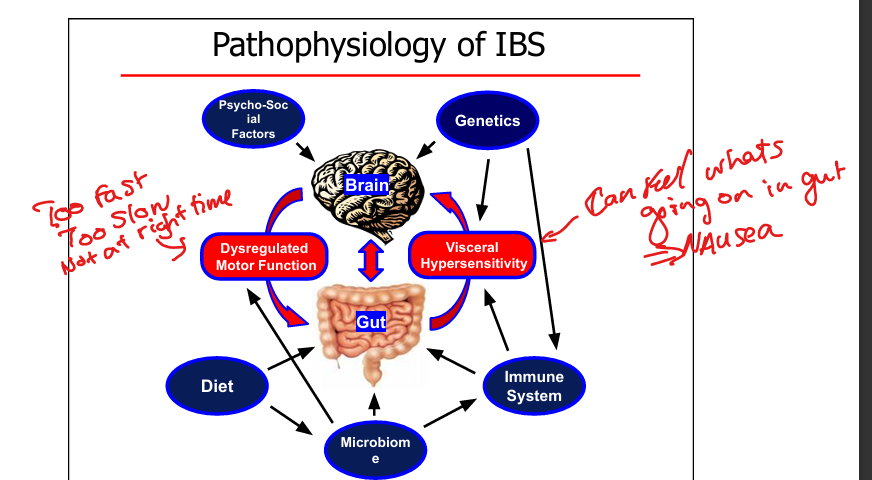
IBS pathophysiology
Visceral hypersensitivity + dysregulated motility + brain–gut axis dysfunction + microbiome + psychosocial factors.
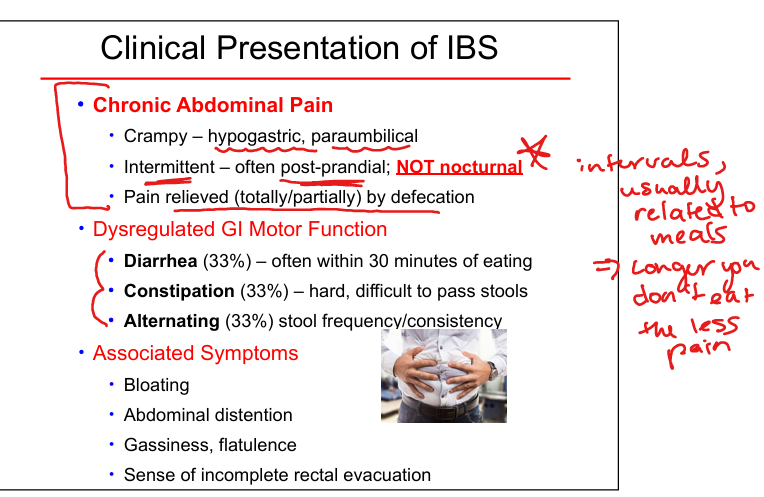
IBS pain features
Crampy, hypogastric/paraumbilical, post‑prandial, NOT nocturnal, relieved by defecation.
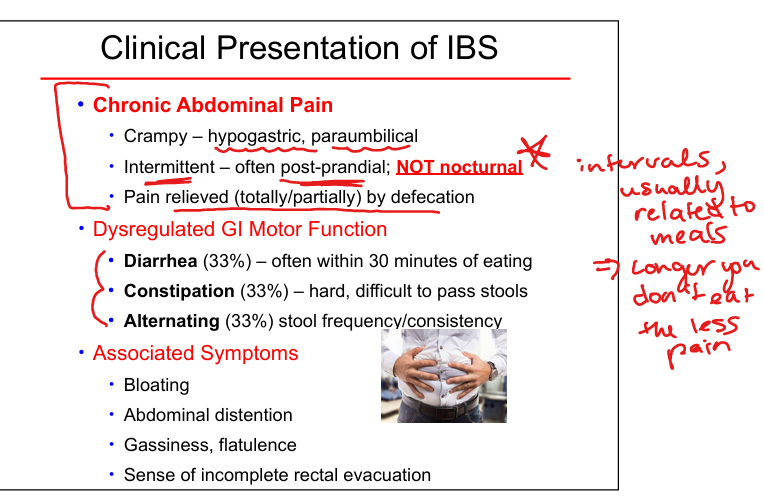
IBS associated symptoms
Bloating, distention, gas, incomplete evacuation.
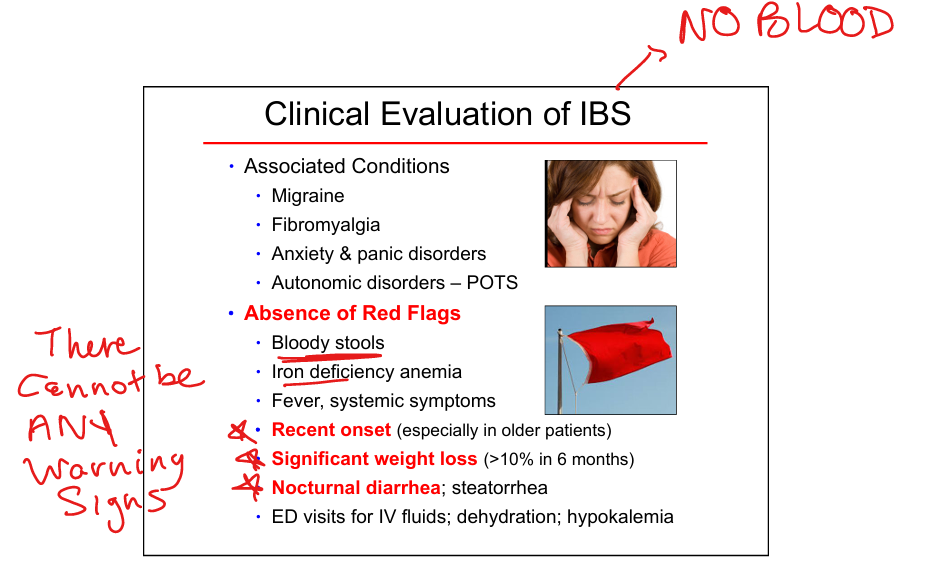
IBS red flags (meaning it isn’t IBS)
Blood in stool, iron deficiency anemia, nocturnal symptoms, weight loss, fever, recent onset in older adults.
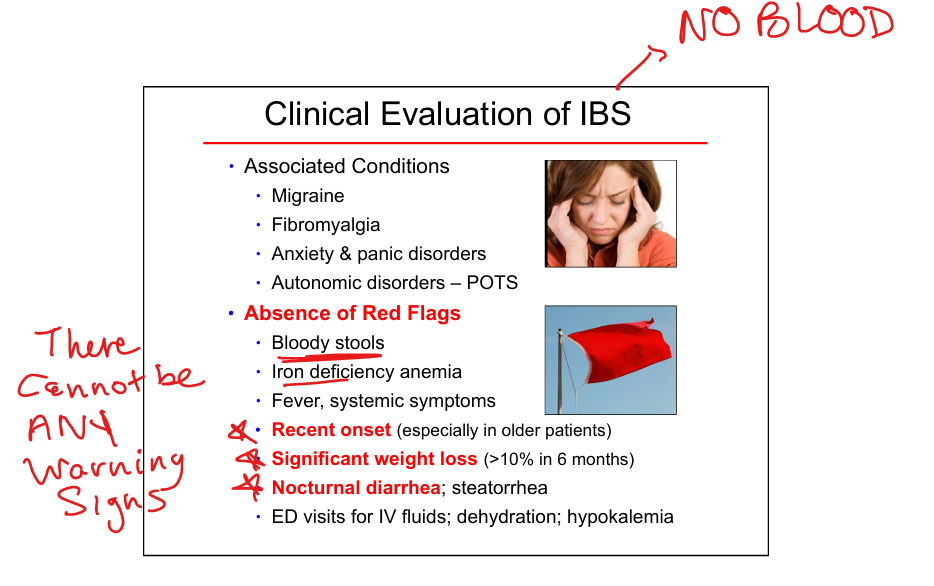
IBS associated conditions
Migraine, fibromyalgia, anxiety/panic disorders, POTS.
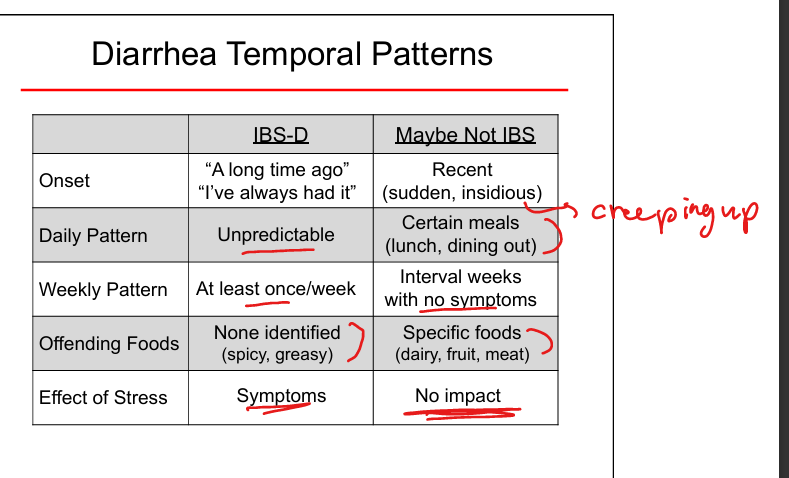
IBS‑D vs non‑IBS diarrhea onset
IBS‑D: long‑standing; non‑IBS: recent/sudden.
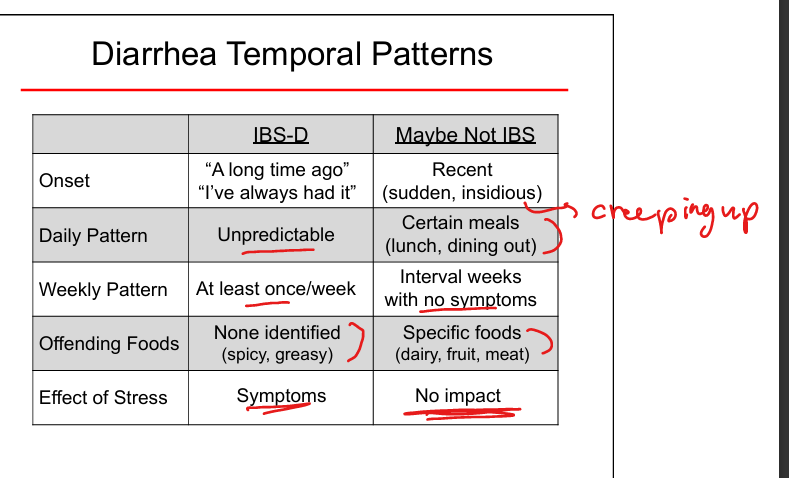
IBS‑D daily pattern vs Non-IBS
IBS: Unpredictable. Non IBS: Certain meals
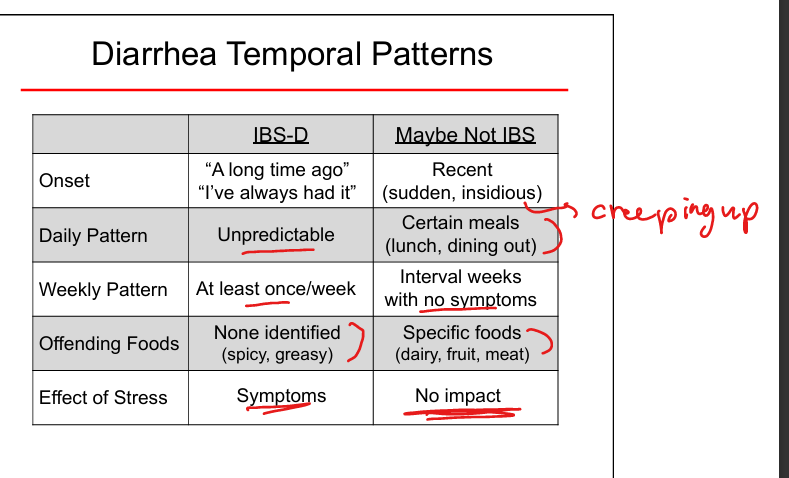
IBS vs Non‑IBS food triggers
None for IBS; Non IBS: Dairy, fruit, meat.
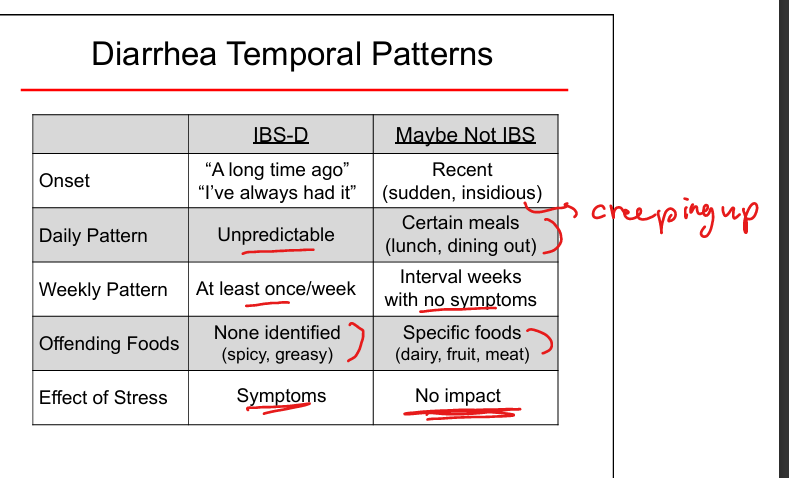
IBS‑D stress effect vs Non IBS
Worsens symptoms. Non IBS: no impact
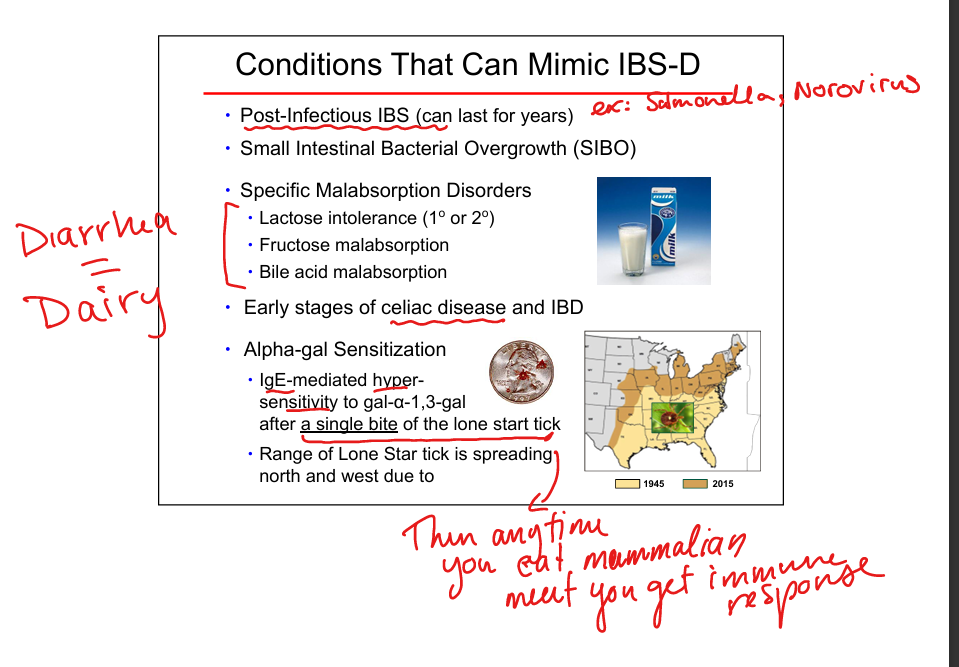
Conditions mimicking IBS‑D
Post‑infectious IBS, SIBO, lactose intolerance, fructose malabsorption, bile acid malabsorption, early celiac/IBD, alpha‑gal syndrome(tick bite now allergic to meat).
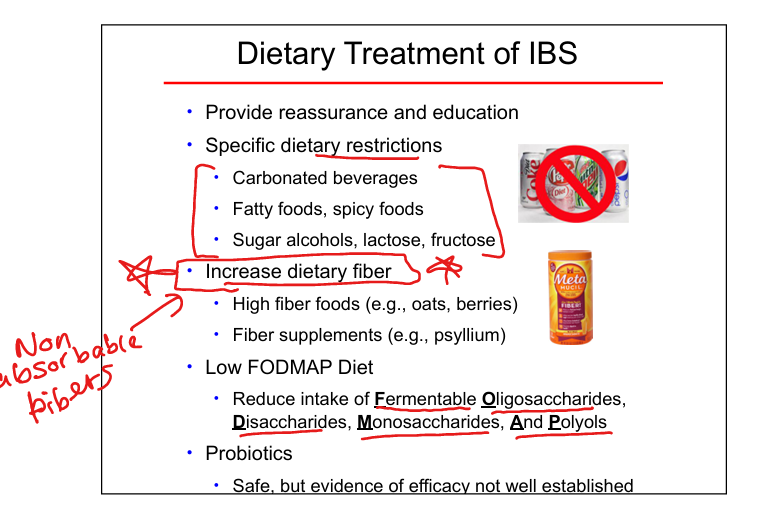
Dietary therapy for IBS
Reassurance, avoid carbonated/spicy/fatty foods, avoid sugar alcohols, lactose/fructose restriction, increase fiber, low‑FODMAP diet, probiotics.
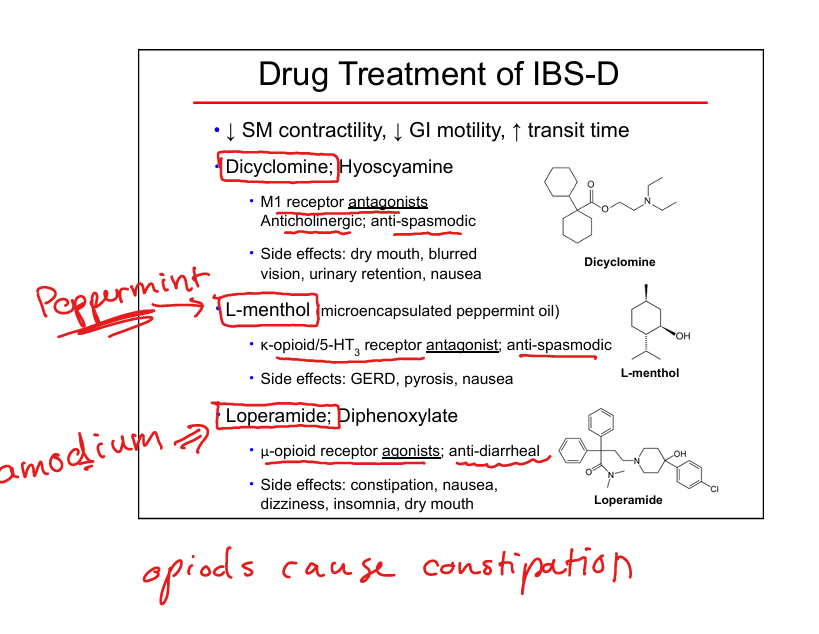
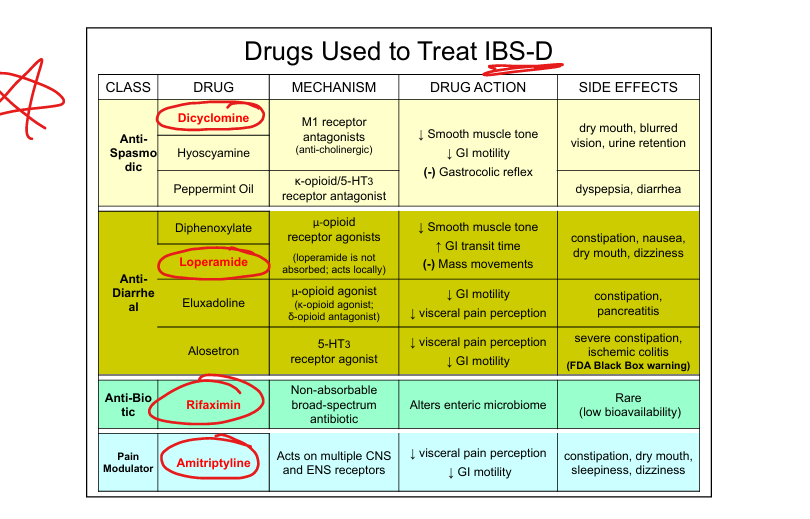
IBS‑D drug: antispasmodics
Dicyclomine, hyoscyamine; M1 antagonists; ↓ SM tone, dec GI motility; SE: dry mouth, blurry vision, urinary retention.
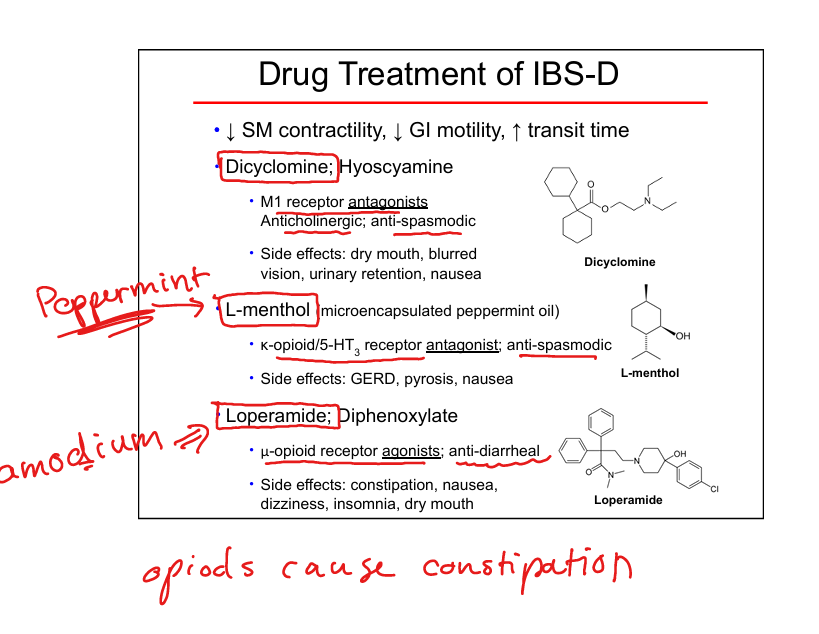
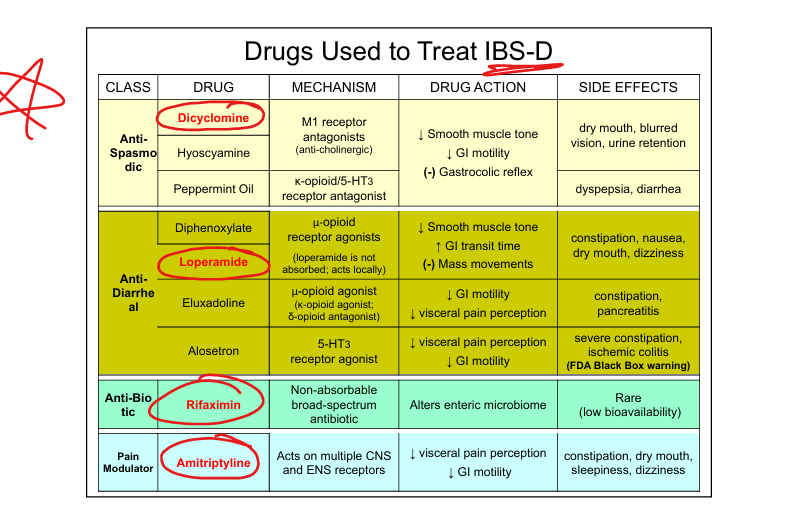
IBS‑D drug: peppermint oil (L-menthol)
K‑opioid/5‑HT3 antagonist; antispasmotic SE: GERD, reflux, nausea.

IBS‑D drug: loperamide(Imodium)
μ‑opioid agonist; slows transit; antidiarrheal SE: constipation.
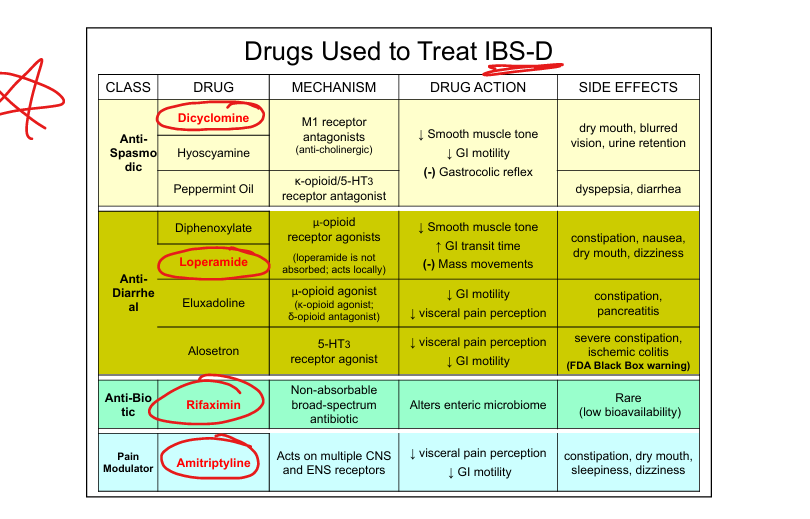
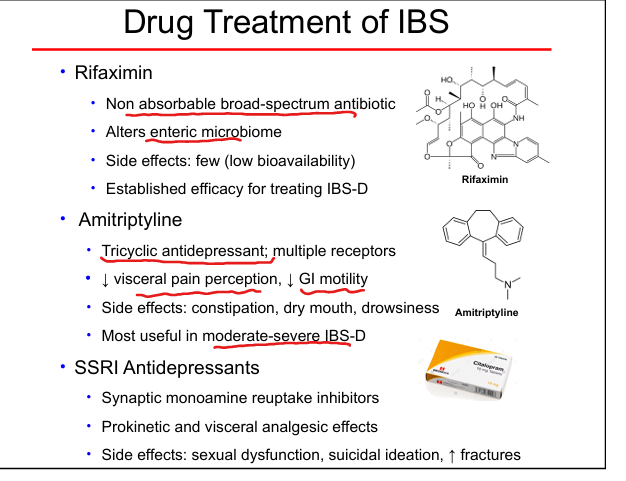
IBS‑D drug: rifaximin
Non‑absorbable antibiotic; alters microbiome; few SE. (Min like minimum like micro like microbiome antibiotic)
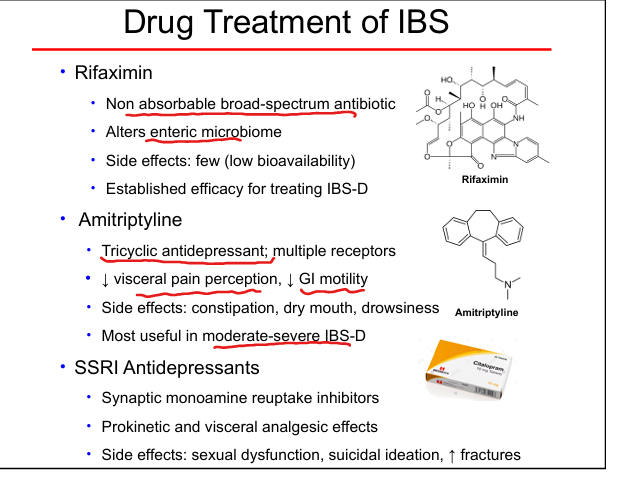
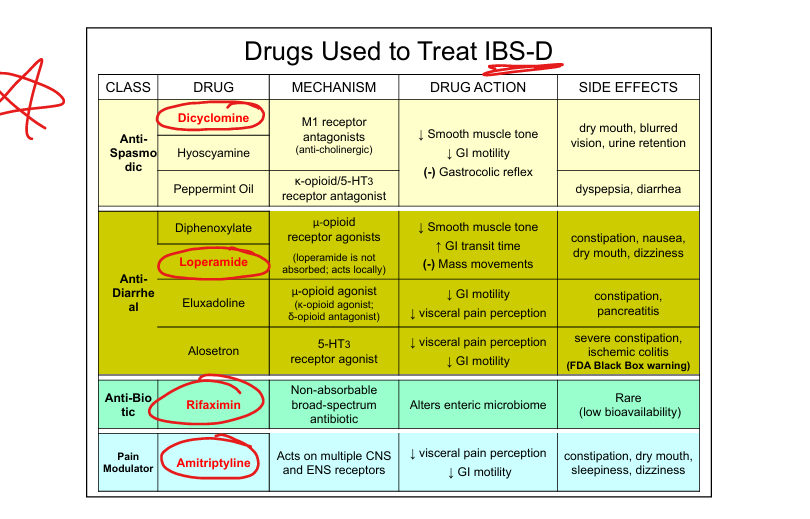
IBS‑D drug: amitriptyline
↓ visceral pain, ↓ motility; SE: constipation, dry mouth, sedation.
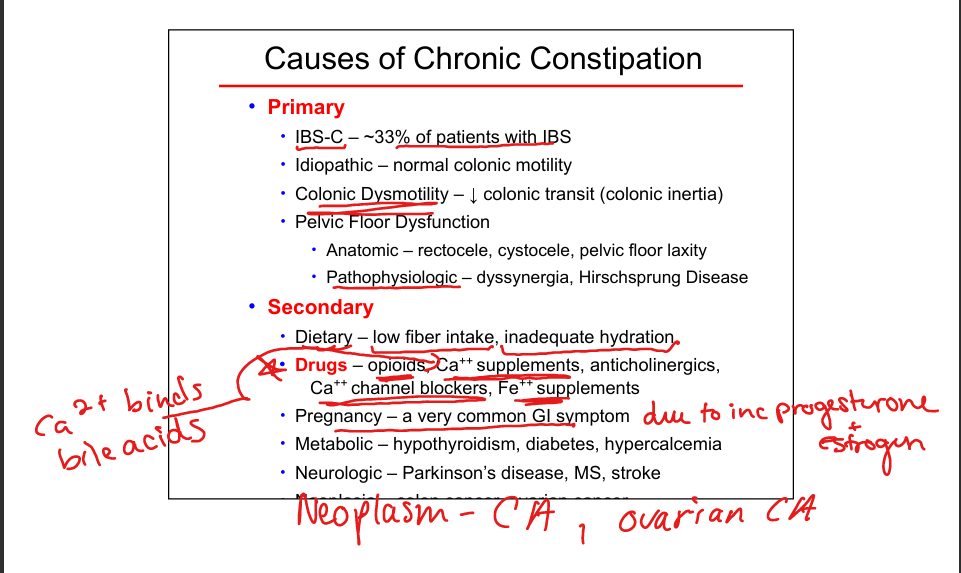
Primary constipation types
IBS‑C, normal transit, slow transit (colonic inertia), pelvic floor dysfunction.
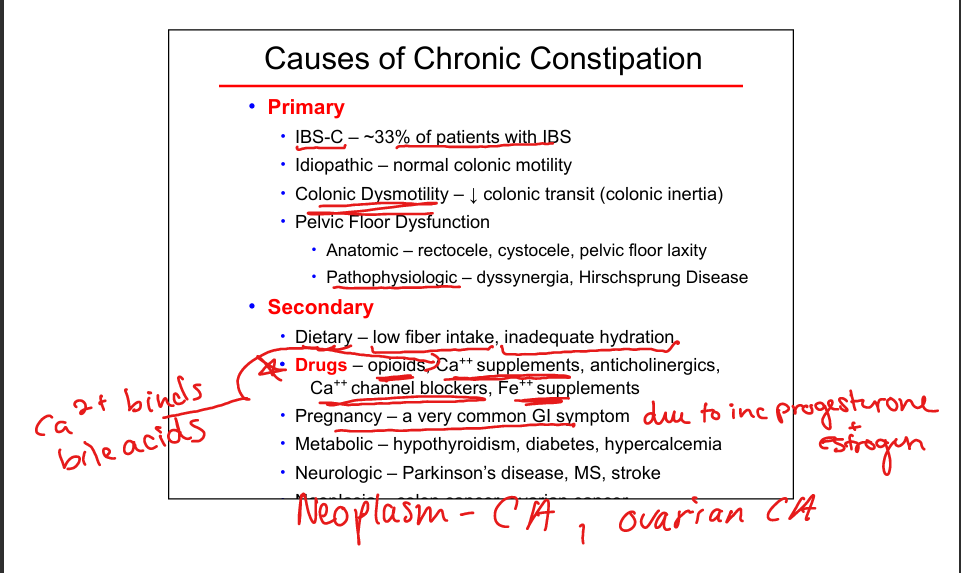
Secondary constipation causes
Low fiber, dehydration, opioids, anticholinergics, CCBs, iron, pregnancy, hypothyroid, diabetes, hypercalcemia, Parkinson’s, MS, stroke, malignancy.
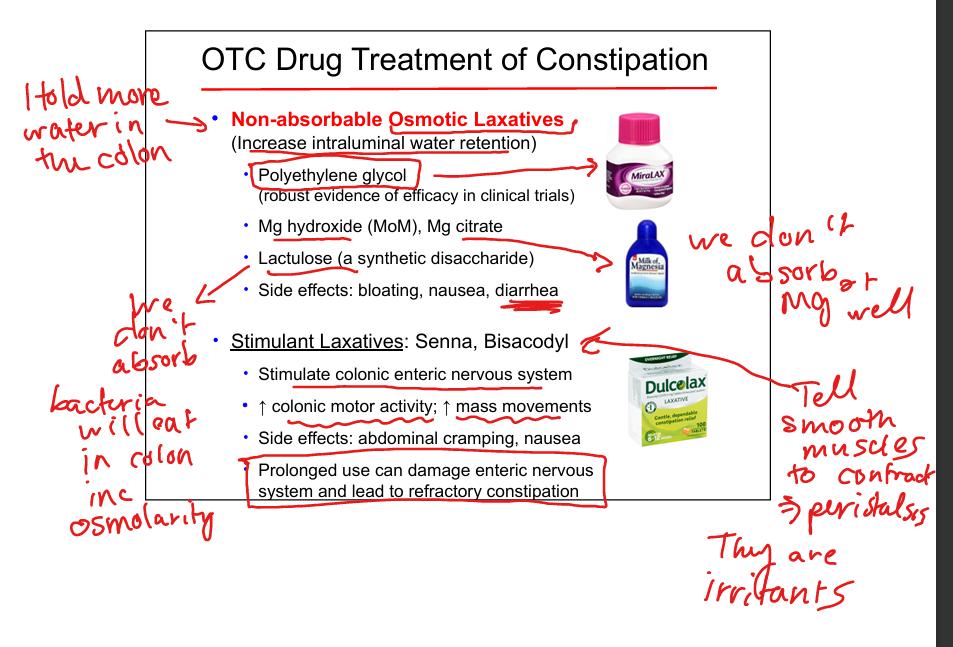
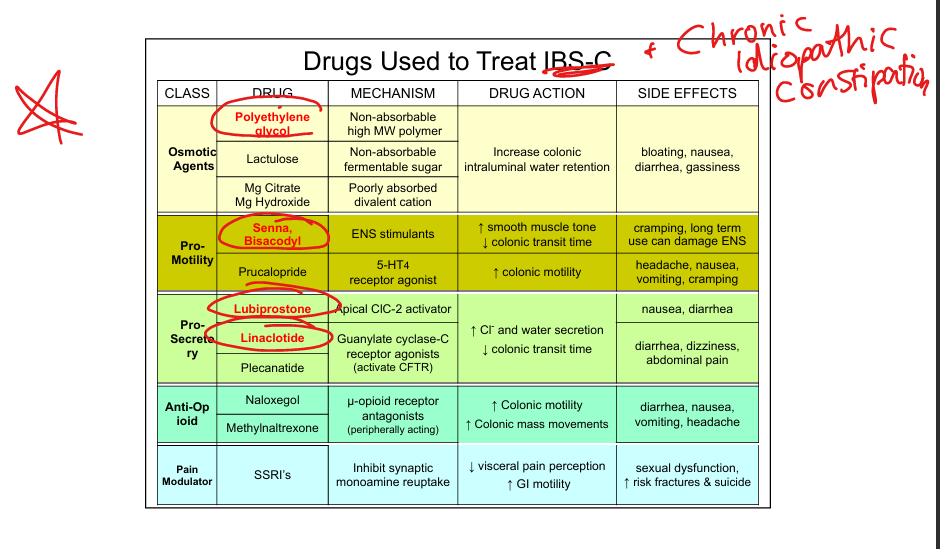
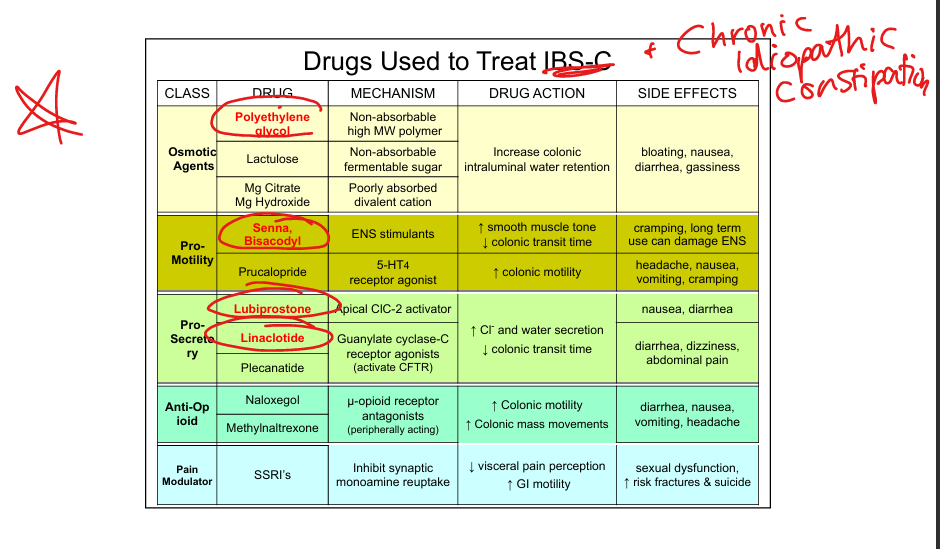
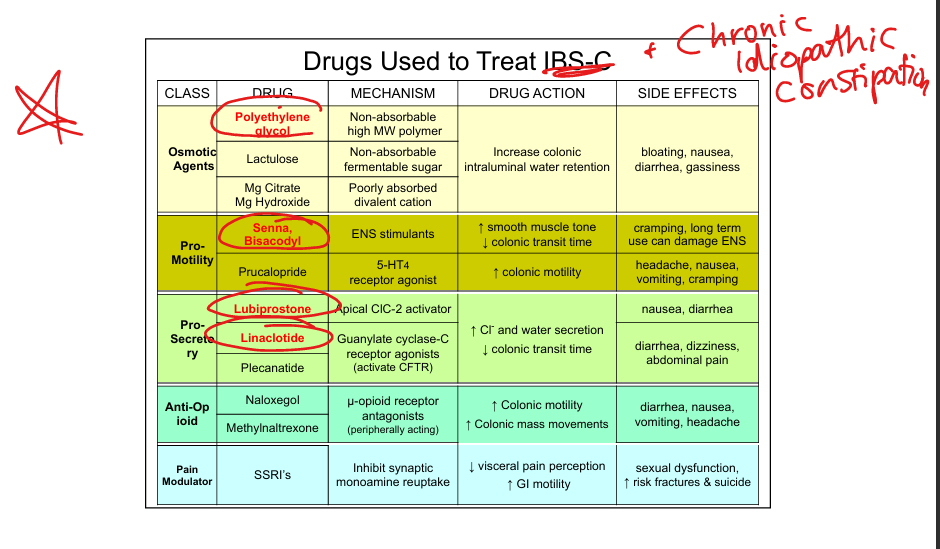
Constipation OTC: osmotic agents
Polyethylene glycol (best evidence), lactulose, Mg citrate/hydroxide; Thet increase intraluminal water retention softening stool SE: bloating, diarrhea.
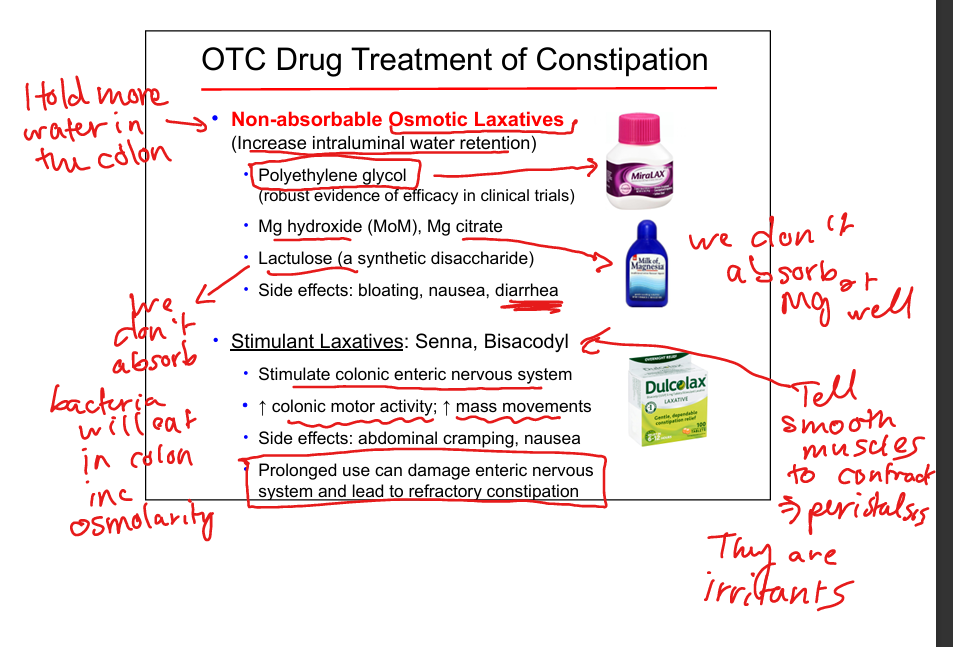
Constipation OTC: stimulant agents
Senna, bisacodyl; ↑ ENS activity + colonic motor movement; SE: cramping; long‑term use may damage ENS.
Constipation Rx: lubiprostone
CIC‑2 activator → ↑ Cl⁻ + water secretion; SE: nausea, diarrhea.
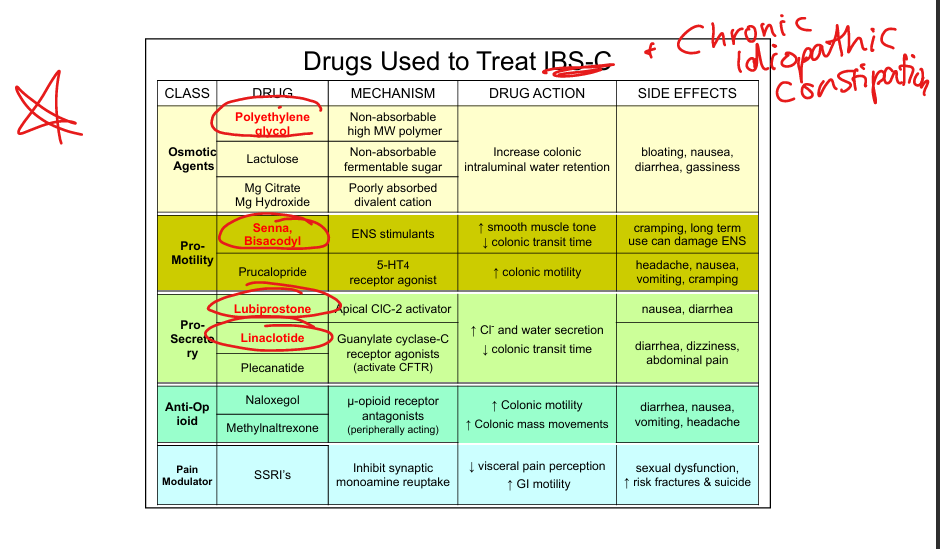
Constipation Rx: linaclotide
GC‑C agonists → ↑ cGMP → activate CFTR, ↑ Cl⁻ + water secretion; SE: diarrhea, dizziness. (A touch of cholera!)
Polyethylene glycol
Treats constripation; non absorbable high molecular weight polymer; increases colonic intraluminal water retention to soften stool; AE: bloating, nausea, diarrhea, gassiness
Senna or Bisacodyl
Treats constipation; ENS stimulant that increases smooth muscle tone and colonic motility; AE: cramping, long term use can damage ENS
IBS summary
Chronic abdominal pain + altered bowel habits without red flags; diagnosis of exclusion.
CIC summary
Chronic constipation due to motility or pelvic floor dysfunction; treated with diet, meds, biofeedback.